- Phencyclidine
-
Phencyclidine 
Systematic (IUPAC) name 1-(1-phenylcyclohexyl)piperidine Clinical data AHFS/Drugs.com entry Pregnancy cat. ? Legal status Schedule I (CA) ? (UK) Schedule II (US) Routes Smoked, Insufflated, Oral Pharmacokinetic data Half-life 7–46 hours Identifiers CAS number 77-10-1 
ATC code None PubChem CID 6468 DrugBank DB03575 ChemSpider 6224 UNII J1DOI7UV76 KEGG C07575 ChEMBL CHEMBL275528 Chemical data Formula C17H25N Mol. mass 243.387 g/mol SMILES eMolecules & PubChem - InChI=1S/C17H25N/c1-4-10-16(11-5-1)17(12-6-2-7-13-17)18-14-8-3-9-15-18/h1,4-5,10-11H,2-3,6-9,12-15H2
Key:JTJMJGYZQZDUJJ-UHFFFAOYSA-N
 (what is this?) (verify)
(what is this?) (verify)Phencyclidine (a complex clip of the chemical name 1-(1-phenylcyclohexyl)piperidine), commonly initialized as PCP and known colloquially as angel dust, is a recreational dissociative drug. Formerly used as an anesthetic agent, PCP exhibits both hallucinogenic and neurotoxic effects.[1]
First synthesized in 1926,[2] it was eventually patented in 1952 by the Parke-Davis pharmaceutical company and marketed under the brand name Sernyl. In chemical structure, PCP is an arylcyclohexylamine derivative, and, in pharmacology, it is a member of the family of dissociative anesthetics. PCP works primarily as an NMDA receptor antagonist, which blocks the activity of the NMDA receptor and, like most antiglutamatergic hallucinogens, is significantly more dangerous than other categories of hallucinogens.[3][4] Other NMDA receptor antagonists include ketamine, tiletamine, dextromethorphan and nitrous oxide. Although the primary psychoactive effects of PCP last for a few hours, its total elimination rate from the body typically extends eight days or longer.
As a recreational drug, PCP may be ingested, smoked, or snorted.[5]
Contents
Biochemistry and pharmacology
Pharmacodynamics
PCP is well known for its primary action on ionotropic glutamate receptors, such as the NMDA receptor in rats and in rat brain homogenate.[6][7] As such, PCP is an NMDA receptor antagonist. NMDA receptors mediate excitation,[8] however, studies have shown that PCP unexpectedly produces substantial cortical activation in humans[9] and rodents.[10]
Research also indicates that PCP inhibits nicotinic acetylcholine (nACh) receptors. Analogues of PCP exhibit varying potency at nACh receptors[citation needed] and NMDA receptors.[11] In some brain regions, these effects are believed to act synergistically by inhibiting excitatory activity.[citation needed]
PCP, like ketamine, also acts as a D2 receptor partial agonist in rat brain homogenate.[7] This activity may be associated with some of the more psychotic features of PCP intoxication, which is evidenced by the successful use of D2 receptor antagonists (such as haloperidol) in the treatment of PCP psychosis.[12]
The relative immunity to pain is likely produced by indirect interaction with the endogenous endorphin and enkephalin system, as has been suggested by studies involving rats.[13][clarification needed]
PCP may also work as a dopamine reuptake inhibitor.[14]
Pharmacokinetics
PCP is metabolized into PCHP, PPC and PCAA.
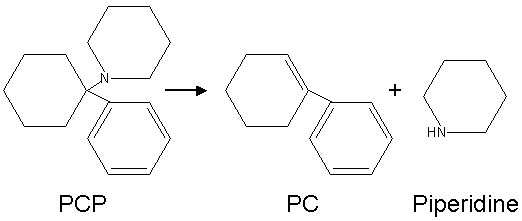
When smoked, some of it is broken down by heat into 1-phenyl-1-cyclohexene (PC) and piperidine.
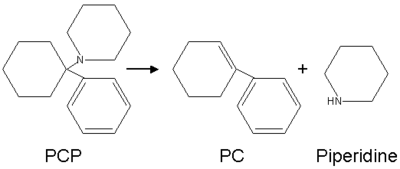 Conversion of PCP into PC and piperidine by heat. (Image in the PD)
Conversion of PCP into PC and piperidine by heat. (Image in the PD)
Structural analogues
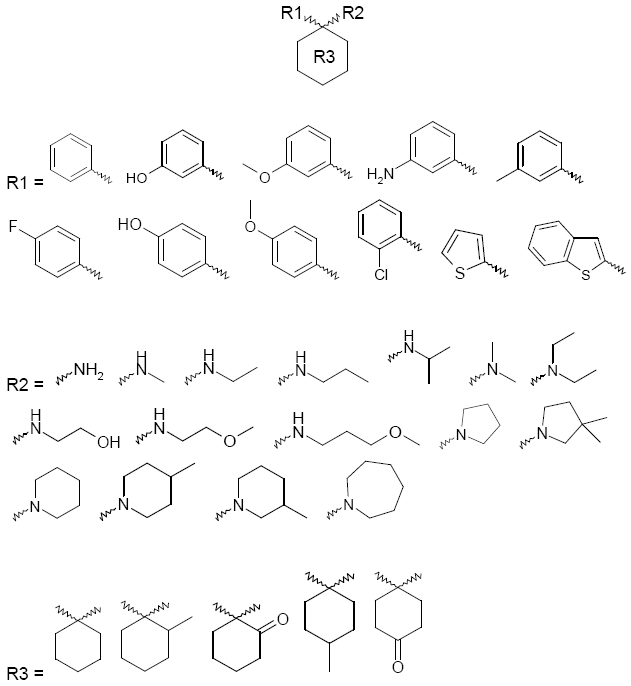
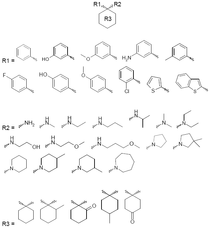 Possible Analogues of PCP
Possible Analogues of PCPMore than 30 different analogues of PCP were reported as being used on the street during the 1970s and 1980s, mainly in the USA. The best known of these are PCPy (rolicyclidine, 1-(1-phenylcyclohexyl)pyrrolidine); PCE (eticyclidine, N-ethyl-1-phenylcyclohexylamine); and TCP (tenocyclidine, 1-(1-(2-Thienyl)cyclohexyl)piperidine). These compounds were never widely-used and did not seem to be as well-accepted by users as PCP itself, however they were all added onto Schedule I of the Controlled Substance Act because of their putative similar effects.[15][citation needed]
The generalized structural motif required for PCP-like activity is derived from structure-activity relationship studies of PCP analogues, and summarized below. All of these analogues would have somewhat similar effects to PCP itself, although, with a range of potencies and varying mixtures of anesthetic, dissociative and stimulant effects depending on the particular substituents used. In some countries such as the USA, Australia, and New Zealand, all of these compounds would be considered controlled substance analogues of PCP, and are hence illegal drugs, even though many of them have never been made or tested.[16][17][clarification needed]
Brain effects
Some studies found that, like other NMDA receptor antagonists, phencyclidine can cause a certain kind of brain damage called Olney's lesions in rats.[18][19] Studies conducted on rats showed that high doses of the NMDA receptor antagonist MK-801 caused reversible vacuoles to form in certain regions of the rats' brains. All studies of Olney's lesions have only been performed on animals and may not apply to humans. The research into the relationship between rat brain metabolism and the creation of Olney's Lesions has been discredited and may[weasel words] not apply to humans, as has been shown with ketamine.[20][21]
Phencyclidine has also been shown to cause schizophrenia-like changes in N-acetylaspartate and N-acetylaspartylglutamate in the rat brain, which are detectable both in living rats and upon necropsy examination of brain tissue.[22] It also induces symptoms in humans that mimic schizophrenia.[23]
The full extent of the pharmacology of this compound in the human CNS is not fully understood; it binds to many different receptor sites. The primary interactions are as a non-competitive antagonist at the 3A-subunit [epsilon subunit] of the NMDA receptor.[citation needed] Phencyclidine is known[by whom?] to bind, with relatively high affinity, to the D1 subunit of the human DAT (Dopamine Transporter)[citation needed], in addition to displaying a positive antagonistic effect at the α7-subunit of the Nicotinic Acetylcholine Receptor (nAChR).[citation needed] It also binds to the mu-opioid receptor[citation needed], which seems[weasel words] to be a central part of the mechanism of action of drugs in this class.[citation needed] (For example, Dizocilpine [MK-801] shows little appreciable[weasel words] analgesic effect despite having a high specificity for the NMDA-3A and NMDA-3B subunits – this may well[weasel words] be mediated by the lack of related efficacy at the mu-opioid receptor, though the NMDAR may[weasel words] play a role in transmission of pain signals).[citation needed]
History and medicinal use
PCP was first synthesized in 1926 and later tested after World War II as a surgical anesthetic. Because of its adverse side effects, such as hallucinations, mania, delirium, and disorientation, it was shelved until the 1950s. In 1953, it was patented by Parke-Davis and named Sernyl (referring to serenity),[24] but was only used in humans for a few years because of side-effects. In 1967, it was given the trade name Sernylan and marketed as a veterinary anesthetic, but was again discontinued. Its side effects and long half-life in the human body made it unsuitable for medical applications.
Recreational use
 Illicit PCP seized by the DEA in several forms.
Illicit PCP seized by the DEA in several forms.PCP began to emerge as a recreational drug in major cities in the United States in 1967.[25] In 1978, People magazine and Mike Wallace of 60 Minutes called PCP the country's "number one" drug problem. Although recreational use of the drug had always been relatively low, it began declining significantly in the 1980s. In surveys, the number of high school students admitting to trying PCP at least once fell from 13% in 1979 to less than 3% in 1990.[26]
PCP comes in both powder and liquid forms (PCP base is dissolved most often in ether), but typically it is sprayed onto leafy material such as cannabis, mint, oregano, parsley, or ginger leaves, then smoked.
PCP is a Schedule II substance in the United States, a Schedule I drug by the Controlled Drugs and Substances act in Canada, a List I drug of the Opium Law in the Netherlands and a Class A substance in the United Kingdom.
Methods of administration
In its pure (free base) form, PCP is a yellow oil (usually dissolved in petroleum, diethyl ether, or tetrahydrofuran). Upon treatment with hydrogen chloride gas, or isopropyl alcohol saturated with hydrochloric acid, this oil precipitates into white-tan crystals or powder (PCP hydrochloride). In this, the salt form, PCP can be insufflated, depending upon the purity. However, most PCP on the illicit market often contains a number of contaminants as a result of makeshift manufacturing, causing the color to range from tan to brown, and the consistency to range from powder to a gummy mass.[citation needed] These contaminants can range from unreacted piperidine and other precursors, to carcinogens like benzene and cyanide-like compounds such as PCC (piperidinocyclohexyl carbonitrile).[citation needed]
The term "embalming fluid" is often used to refer to the liquid PCP in which a cigarette is dipped, to be ingested through smoking, commonly known as "boat" or "water." The name most likely originated from the somatic "numbing" effect and feelings of dissociation induced by PCP, and has led to the widespread and mistaken belief that the liquid is made up of or contains real embalming fluid. Occasionally, however, some users and dealers could have, believing this myth, used real embalming fluid mixed with, or in place of, PCP.[27][28] Smoking PCP is known as "getting wet", and a cigarette or joint which has been dipped in PCP may be referred to on the street as a "fry stick," "sherm," "amp," "lovely," "KJ (an abbreviation for 'Killer Joint')," "toe tag", "dipper", "happy stick," or "wet stick." "Getting wet" may have once been a popular method of using PCP, especially in the western United States where it may have been sold for about $10 to $25 per cigarette.[citation needed]
Effects
Behavioral effects can vary by dosage. Low doses produce a numbness in the extremities and intoxication, characterized by staggering, unsteady gait, slurred speech, bloodshot eyes, and loss of balance. Moderate doses (5–10 mg intranasal, or 0.01–0.02 mg/kg intramuscular or intravenous) will produce analgesia and anesthesia. High doses may lead to convulsions.[29] Users frequently do not know how much of the drug they are taking due to the tendency of the drug to be made illegally in uncontrolled conditions.[30]
Psychological effects include severe changes in body image, loss of ego boundaries, paranoia and depersonalization. Hallucinations, euphoria, suicidal impulses and aggressive behavior are reported.[29][31] The drug has been known to alter mood states in an unpredictable fashion, causing some individuals to become detached, and others to become animated. Intoxicated individuals may act in an unpredictable fashion, possibly driven by their delusions and hallucinations. PCP may induce feelings of strength, power, and invulnerability as well as a numbing effect on the mind.[5] Occasionally, this leads to bizarre acts of violence.[32] However, studies by the Drug Abuse Warning Network in the 1970s show that media reports of PCP-induced violence are greatly exaggerated and that incidents of violence were unusual and often (but not always) limited to individuals with reputations for aggression regardless of drug use.[33] The reports in question often dealt with a supposed increase in strength imparted by the drug; this could partially be explained by the anaesthetic effects of the drug. The most commonly-cited types of incidents included self-mutilation of various types, breaking handcuffs (a feat reportedly requiring about 550 lbf (2.4 kN) of force), inflicting remarkable property damage, and pulling one's own teeth.[33][34][35]
Included in the portfolio of behavioral disturbances are acts of self-injury including suicide, and attacks on others or destruction of property. The analgesic properties of the drug can cause users to feel less pain, and persist in violent or injurious acts as a result. Recreational doses of the drug can also induce a psychotic state that resembles schizophrenic episodes which can last for months at a time with toxic doses.[36] Users generally report they feel detached from reality, or that one's consciousness seems somewhat disconnected from reality.[37]
Symptoms are summarized by the mnemonic device RED DANES: rage, erythema (redness of skin), dilated pupils, delusions, amnesia, nystagmus (oscillation of the eyeball when moving laterally), excitation, and skin dryness.[38]
Management of intoxication
Management of phencyclidine intoxication mostly consists of supportive care — controlling breathing, circulation, and body temperature — and, in the early stages, treating psychiatric symptoms.[39][40][41] Benzodiazepines, such as lorazepam, are the drugs of choice to control agitation and seizures (when present). Typical antipsychotics such as phenothiazines and haloperidol have been used to control psychotic symptoms, but may produce many undesirable side effects — such as dystonia — and their use is therefore no longer preferred; phenothiazines are particularly risky, as they may lower the seizure threshold, worsen hyperthermia, and boost the anticholinergic effects of PCP.[39][40] If an antipsychotic is given, intramuscular haloperidol has been recommended.[41][42][43]
Forced acid diuresis (with ammonium chloride or, more safely, ascorbic acid) may increase clearance of PCP from the body, and was somewhat controversially recommended in the past as a decontamination measure.[39][40][41] However, it is now known that only around 10% of a dose of PCP is removed by the kidneys, which would make increased urinary clearance of little consequence; furthermore, urinary acidification is dangerous, as it may induce acidosis and worsen rhabdomyolysis (muscle breakdown), which is not an unusual manifestation of PCP toxicity.[39][40]
See also
References
- ^ Maisto, Stephen A.; Mark Galizio, Gerard Joseph Connors (2004). Drug Use and Abuse. Thompson Wadsworth. ISBN 0-15-508517-4.
- ^ Development of PCP, 2006 ,CESAR (Center for Substance Abuse Research)
- ^ Drugs and Behavior, 4th Edition, McKim, William A., ISBN 0-13-083146-8
- ^ Kapur, S. and P. Seeman. "NMDA receptor antagonists ketamine and PCP have direct effects on the dopamine D2 and serotonin 5-HT2receptorsimplications for models of schizophrenia(2002)
- ^ a b "NIDA InfoFacts: Hallucinogens - LSD, Peyote, Psilocybin, and PCP". DrugAbuse.gov. National Institute on Drug Abuse. http://drugabuse.gov/infofacts/hallucinogens.html. Retrieved 2011-01-26.
- ^ Large, CH; Bison, S (2011). "The Efficacy of Sodium Channel Blockers to Prevent Phencyclidine-Induced Cognitive Dysfunction in the Rat: Potential for Novel Treatments for Schizophrenia". Journal of pharmacology and experimental therapeutics 338 (1): 100–113 =. http://jpet.aspetjournals.org/content/338/1/100.abstract. Retrieved July 2011.
- ^ a b Seeman P, Guan HC, Hirbec H (August 2009). "Dopamine D2High receptors stimulated by phencyclidines, lysergic acid diethylamide, salvinorin A, and modafinil". Synapse 63 (8): 698–704. doi:10.1002/syn.20647. PMID 19391150.
- ^ Hirsch, JC; Crepel, F (1991). "Blockage of NMDA receptors unmasks a long-term depression in synaptic efficacy in rat profrontal neurons in vitro". Exp Brain Res 85 (3): 621–624. PMID 1680738.
- ^ Breier, AK; Malhotra, DA (1997). "Association of ketamine-induced psychosis with focal activation of the prefrontal cortex in healthy volunteers". Am J Psychiatry 154: 805–811.
- ^ Suzuki, Y; Jodo, E (2002). "Acute administration of phencyclidine induces tonic activation of medial prefrontal cortex neurons in freely moving rats". Neuroscience 114 (3): 769–779.
- ^ Zarantonello, P; Bettini, E (2011). "Novel Analogues of ketamine and phencyclidine as NMDA receptor antagonists". Bioorganic and medicinal chemistry letters 21 (7): 2059–2063. http://www.ncbi.nlm.nih.gov/pubmed/21334205. Retrieved July 2011.
- ^ Giannini AJ, Nageotte C, Loiselle RH, Malone DA, Price WA (1984). "Comparison of chlorpromazine, haloperidol and pimozide in the treatment of phencyclidine psychosis: DA-2 receptor specificity". Journal of Toxicology. Clinical Toxicology 22 (6): 573–579. doi:10.3109/15563658408992586. PMID 6535849.
- ^ Castellani S, Giannini AJ, Adams PM (1982). "Effects of naloxone, metenkephalin, and morphine on phencyclidine-induced behavior in the rat". Psychopharmacology 78 (1): 76–80. doi:10.1007/BF00470593. PMID 6815700.
- ^ AJ Giannini,S Kalavsky,RH Loiselle, MC Giannini, WA Price. Possible role of the DA-2 receptor in phencyclidine psychosis. Neuroscience Abstracts. 9:33, 1983,
- ^ PCP synthesis and effects: table of contents
- ^ Itzhak Y, Kalir A, Weissman BA, Cohen S. New analgesic drugs derived from phencyclidine. Journal of Medicinal Chemistry. 1981; 24(5):496–499
- ^ Chaudieu I, Vignon J, Chicheportiche M, Kamenka JM, Trouiller G, Chicheportiche R. Role of the aromatic group in the inhibition of phencyclidine binding and dopamine uptake by PCP analogs. Pharmacology Biochemistry and Behaviour. 1989 Mar;32(3):699–705.
- ^ Olney J, Labruyere J, Price M (1989). "Pathological changes induced in cerebrocortical neurons by phencyclidine and related drugs". Science 244 (4910): 1360–1362. doi:10.1126/science.2660263. PMID 2660263.
- ^ Hargreaves R, Hill R, Iversen L (1994). "Neuroprotective NMDA antagonists: the controversy over their potential for adverse effects on cortical neuronal morphology". Acta Neurochir Suppl (Wien) 60: 15–9. PMID 7976530.
- ^ Jansen, Karl. Ketamine: Dreams and Realities. MAPS, 2004. ISBN 0-9660019-7-4
- ^ Erowid DXM Vault : Response to "The Bad News Isn't In": Please Pass The Crow, by William E. White
- ^ Reynolds, Lindsay M.; Susan M. Cochran, Brian J. Morris, Judith A. Pratt and Gavin P. Reynolds (March 1, 2005). "Chronic phencyclidine administration induces schizophrenia-like changes in N-acetylaspartate and N-acetylaspartylglutamate in rat brain". Schizophrenia Research 73 (2-3): 147–152. doi:10.1016/j.schres.2004.02.003. PMID 15653257.
- ^ Murray JB (May 2002). "Phencyclidine (PCP): a dangerous drug, but useful in schizophrenia research". J Psychol 136 (3): 319–327. doi:10.1080/00223980209604159. PMID 12206280.
- ^ Zukin, Stephen R; Sloboda, Zili; Javitt, Daniel C (2005). "Phencyclidine (PCP)". In Lowinson, Joyce H. Substance Abuse: A Comprehensive Textbook (4th ed.). Philadelphia: Lippincott Williams & Wilkins. ISBN 0-7817-3474-6. http://books.google.com/books?id=HtGb2wNsgn4C&pg=PA324&dq=Phencyclidine+history&hl=en&ei=lVH3TLLzJYrWvQOW-PCdDg&sa=X&oi=book_result&ct=result&resnum=7&ved=0CEIQ6AEwBg#v=onepage&q=Phencyclidine%20history&f=false. Retrieved 2 December 2010
- ^ Inciardi 1992, p. 46.
- ^ Inciardi 1992, pp. 46–49.
- ^ Kids Use Embalming Fluid as Drug, By Joann Loviglio, July 27, ????, ABC News
- ^ Illegal drug users dip into embalming fluid, By Douglass Dowty, August 03, 2009, The Post-Standard
- ^ a b Diaz, Jaime. How Drugs Influence Behavior. Englewood Cliffs: Prentice Hall, 1996.
- ^ Chudler, Eric H.. "Neuroscience for Kids - PCP". Neuroscience for Kids. http://faculty.washington.edu/chudler/pcp.html. Retrieved 2011-01-26.
- ^ Inciardi 1992, p. 48–49.
- ^ Does PCP turn people into cannibals? The Straight Dope, 2005
- ^ a b Inciardi 1992, p. 48.
- ^ Gahlinger, 2001
- ^ Does PCP turn people into cannibals? The Straight Dope, 2005
- ^ Luisada PV. The phencyclidine psychosis: phenomenology and treatment. In Petersen Rc, Stillman RC (eds). Phencyclidine (PCP) abuse: an appraisal. National Institute on Drug Abuse: Rockville, Maryland, 1978.
- ^ Pender JW (1972). "Dissociative anesthesia". Calif Med 117: 46–47. PMC 1518731. PMID 18730832. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1518731.
- ^ A James Giannini (1997). Drugs of Abuse (Second ed.). Los Angeles: Practice Management Information Corp. p. 126. ISBN 1-57066-053-0.
- ^ a b c d Helman RS, Habal R (October 6, 2008). "Phencyclidine Toxicity". eMedicine. http://www.emedicine.com/med/TOPIC1813.HTM. Retrieved on November 3, 2008.
- ^ a b c d Olmedo R (2002). "Chapter 69: Phencyclidine and ketamine". In Goldfrank LR, Flomenbaum NE, Lewin NA, Howland MA, Hoffman RS, Nelson LS (eds.). Goldfrank's Toxicologic Emergencies. New York: McGraw-Hill. pp. 1034–1041. ISBN 0-07-136001-8. http://books.google.com/?id=HVYyRsuUEc0C&pg=PA1041. Retrieved on November 3, 2008 through Google Book Search.
- ^ a b c Milhorn HT (April 1991). "Diagnosis and management of phencyclidine intoxication". American Family Physician 43 (4): 1293–1302. PMID 2008817.
- ^ Giannini AJ. Price WA. PCP: Management of acute intoxication. Medical Times. 1985;113(9):43–49
- ^ Giannini AJ, Eighan MS, Loiselle RH, Giannini MC (April 1984). "Comparison of haloperidol and chlorpromazine in the treatment of phencyclidine psychosis". Journal of Clinical Pharmacology 24 (4): 202–204. PMID 6725621. http://jcp.sagepub.com/cgi/pmidlookup?view=long&pmid=6725621.
- Notes
- Inciardi, James A. (1992). The War on Drugs II. Mayfield Publishing Company. ISBN 1-55934-016-9.
External links
- Erowid.org – PCP Information
- National Institute of Drug Abuse InfoFacts: PCP (Phencyclidine)
- Drugs and Human Performance Fact Sheets on Phencyclidine
- A site with information on PCP, Partnership for a Drug-Free America
- Phencyclidine and Ketamine: A View From the Street-1981 article on the use and effects of PCP
- ChemSub Online: Phencyclidine
Analgesics (N02A, N02B) Opioids
See also: Opioids templateOpium & alkaloids thereofSemi-synthetic opium
derivativesSynthetic opioidsAlphaprodine • Anileridine • Butorphanol • Dextromoramide • Dextropropoxyphene • Dezocine • Fentanyl • Ketobemidone • Levorphanol • Methadone • Meptazinol • Nalbuphine • Pentazocine • Propoxyphene • Propiram • Pethidine • Phenazocine • Piminodine • Piritramide • Tapentadol • Tilidine • Tramadol
Pyrazolones Cannabinoids Anilides Non-steroidal
anti-inflammatories
See also: NSAIDs templatePropionic acid classFenoprofen • Flurbiprofen • Ibuprofen# • Ketoprofen • Naproxen • Oxaprozin
Oxicam classAcetic acid classDiclofenac • Indometacin • Ketorolac • Nabumetone • Sulindac • Tolmetin
Celecoxib • Rofecoxib • Valdecoxib • Parecoxib • Lumiracoxib
Anthranilic acid
(fenamate) classMeclofenamate • Mefenamic acid
SalicylatesAspirin (Acetylsalicylic acid)# • Benorylate • Diflunisal • Ethenzamide • Magnesium salicylate • Salicin • Salicylamide • Salsalate • Trisalate • Wintergreen (Methyl salicylate)
Atypical, adjuvant and potentiators,
Metabolic agents and miscellaneousAmitryptiline • Befiradol • Bicifadine • Carisoprodol • Camphor • Cimetidine • Clonidine • Chlorzoxazone • Cyclobenzaprine • Duloxetine • Esreboxetine • Flupirtine • Gabapentin • Glafenine • Hydroxyzine • Ketamine • Menthol • Mephenoxalone • Methocarbamol • Nefopam • Orphenadrine • Pregabalin • Proglumide • Scopolamine • Tebanicline • Trazodone • Gabapentin enacarbil • ZiconotideDepressants Antihistamines
H1R inverse agonistsOthersAntipsychotics
Mixed MOATypicalsChlorpromazine • Haloperidol ...AtypicalsChannel Blockers Dissociatives
NMDAR Antagonists3-MeO-PCP • Esketamine • Dieticyclidine • Eticyclidine • Gacyclidine • Ketamine • Phencyclidine • PCPr • Rolicyclidine • Tenocyclidine • TiletamineOthersGABAergics 1,4-BD • Aceburic Acid • Gabaculine • GBL • GABA • GABOB • GHB • GHV • GVL • Isovaleramide • Isovaleric Acid • Phenibut • Picamilon • Tiagabine • Valeric Acid • Valerenic Acid • Valnoctamide • Valproic Acid (Sodium Valproate / Valproate Semisodium) • Valpromide • VigabatrinGlutethimide ...Methaqualone ...OthersBaclofen • Clomethiazole • Diethyl Ether • Ethanol (Alcohol) • Etomidate • Gaboxadol • Muscimol • Stiripentol • Theanine • Kavalactones (Kava Kava) • Valerenic Acid (Valerian)Glycinergics Alanine • Cycloserine • Dimethylglycine • Glycine • Hypotaurine • Methylglycine / Sarcosine • Serine • Taurine • Trimethylglycine / BetaineNarcotics
MOR AgonistsAlfentanil • Buprenorphine • Butorphanol • Carfentanil • Diacetylmorphine (Heroin) • Dihydrocodeine • Ethylmorphine • Etorphine • Fentanyl • Hydrocodone • Hydromorphone • Ketobemidone • Levacetylmethadol • Levorphanol • Meperidine / Pethidine • Methadone • Nalbuphine • Oxycodone • Oxymorphone • Pentazocine • Phenazocine • Propoxyphene • Remifentanil • Tapentadol • Tramadol • SufentanilSympatholytics
α/β-AR ModulatorsPropranolol ...OthersClonidine ...Miscellaneous Hallucinogens Psychedelics
5-HT2AR agonists- Lysergamides: AL-LAD
- ALD-52
- BU-LAD
- CYP-LAD
- DAM-57
- Diallyllysergamide
- Ergometrine (Ergonovine, Ergobasine)
- ETH-LAD
- LAE-32
- LSA (Ergine, Lysergamide)
- LSD
- LSH
- LPD-824
- LSM-775
- Lysergic Acid 2-Butyl Amide
- Lysergic Acid 2,4-Dimethylazetidide
- Lysergic Acid 3-Pentyl Amide
- Methylergometrine
- Methylisopropyllysergamide
- Methysergide
- MLD-41
- PARGY-LAD
- PRO-LAD;
- Phenethylamines: Aleph
- 2C-B
- 2C-B-Dragonfly
- 2C-B-FLY
- 2C-C-FLY
- 2C-D-FLY
- 2C-E-FLY
- 2C-I-FLY
- 2CBFly-NBOMe
- 2C-T-7-FLY
- 2C-C
- 2C-C-NBOMe
- 2C-CN-NBOMe
- 2C-D
- 2CD-5EtO
- 2C-D-NBOMe
- 2C-E
- 2C-EF
- 2C-E-NBOMe
- 2C-F
- 2C-F-NBOMe
- 2C-G
- 2C-G-NBOMe
- 2C-H-NBOMe
- 2C-I
- 2C-N
- 2C-N-NBOMe
- 2C-O
- 2C-O-4
- 2C-P
- 2C-T
- 2C-T-2
- 2C-T-4
- 2C-T-4-NBOMe
- 2C-T-7
- 2C-T-7-NBOH
- 2C-T-8
- 2C-T-9
- 2C-T-13
- 2C-T-15
- 2C-T-17
- 2C-T-21
- 2C-TFM
- 2C-TFM-NBOMe
- 2C-YN
- 2CBCB-NBOMe
- 25B-NBOMe
- 25I-NBMD
- 25I-NBOH
- 25I-NBOMe
- 3C-E
- 3C-P
- 5-APB
- 5-APDB
- 6-APB
- 6-APDB
- Br-DFLY
- DESOXY
- DMMDA
- DMMDA-2
- DOB
- DOB-FLY
- DOM-FLY
- DOC
- DOEF
- DOET
- DOF
- DOI
- DOM
- DON
- DOPR
- DOTFM
- Escaline
- Ganesha
- HOT-2
- HOT-7
- HOT-17
- IAP
- Isoproscaline
- Jimscaline
- Lophophine
- MDA
- MDEA
- MDMA
- MMA
- MMDA
- MMDA-2
- MMDA-3a
- MMDMA
- Macromerine
- Mescaline
- Methallylescaline
- NBOMe-mescaline
- Proscaline
- TCB-2
- TFMFly
- TMA;
- Piperazines: pFPP
- TMFPP;
- Tryptamines: 1-Methyl-5-methoxy-diisopropyltryptamine
- 2,N,N-TMT
- 4-HO-5-MeO-DMT
- 4-Acetoxy-DET
- 4-Acetoxy-DIPT
- 4-Acetoxy-DMT
- 4-Acetoxy-DPT
- 4-Acetoxy-MiPT
- 4-HO-DPT
- 4-HO-MET
- 4-Propionyloxy-DMT
- 4-HO-MPMI
- 5-Me-MIPT
- 5-N,N-TMT
- 5-AcO-DMT
- 5-MeO-2,N,N-TMT
- 5-MeO-α,N,N-TMT
- 5-MeO-α-ET
- 5-MeO-α-MT
- 5-MeO-DALT
- 5-MeO-DET
- 5-MeO-DIPT
- 5-MeO-DMT
- 5-MeO-DPT
- 5-MeO-EiPT
- 5-MeO-MET
- 5-MeO-MIPT
- 5-MeO-MPMI
- 7,N,N-TMT
- α,N,N-TMT
- α-ET
- α-MT
- AL-37350A
- Baeocystin
- Bufotenin
- DALT
- DBT
- DCPT
- DET
- DIPT
- DMT
- DPT
- EiPT
- Ethocin
- Ethocybin
- Iprocin
- MET
- Miprocin
- MIPT
- Norbaeocystin
- PiPT
- Psilocin
- Psilocybin;
- Others: AL-38022A
- Ibogaine
- Noribogaine
- Voacangine
Dissociatives
NMDAR antagonists- Arylcyclohexylamines: 3-MeO-PCP
- 4-MeO-PCP
- Dieticyclidine
- Esketamine
- Eticyclidine
- Gacyclidine
- Ketamine
- Methoxetamine
- Neramexane
- Phencyclidine
- PCPr
- Rolicyclidine
- Tenocyclidine
- Tiletamine;
- Morphinans: Dextrallorphan
- Dextromethorphan
- Dextrorphan
- Methorphan (Racemethorphan)
- Racemorphan;
- Others: 2-MDP
- 8A-PDHQ
- Aptiganel
- Dexoxadrol
- Dizocilpine (MK-801)
- Etoxadrol
- Ibogaine
- Midafotel
- NEFA
- Nitrous Oxide
- Noribogaine
- Perzinfotel
- Remacemide
- Selfotel
- Xenon
Deliriants
mAChR antagonists- 3-Quinuclidinyl benzilate
- Atropine
- Benactyzine
- Benzatropine
- Benzydamine
- Biperiden
- Brompheniramine
- CAR-226,086
- CAR-301,060
- CAR-302,196
- CAR-302,282
- CAR-302,368
- CAR-302,537
- CAR-302,668
- Chlorpheniramine
- Chloropyramine
- Clemastine
- CS-27349
- Cyclizine
- Cyproheptadine
- Dicyclomine (Dicycloverine)
- Dimenhydrinate
- Diphenhydramine
- Ditran
- Doxylamine
- EA-3167
- EA-3443
- EA-3580
- EA-3834
- Elemicin
- Flavoxate
- Hydroxyzine
- Hyoscyamine
- Meclizine
- Myristicin
- N-Ethyl-3-piperidyl benzilate
- N-Methyl-3-piperidyl benzilate
- Pyrilamine
- Orphenadrine
- Oxybutynin
- Pheniramine
- Phenyltoloxamine
- Procyclidine
- Promethazine
- Scopolamine (Hyoscine)
- Tolterodine
- Trihexyphenidyl
- Tripelennamine
- Triprolidine
- WIN-2299
Miscellaneous - Apomorphine
- Bromocriptine
- Cabergoline
- Lisuride
- Memantine
- Pergolide
- Piribedil
- Pramipexole
- Ropinirole
- Rotigotine
- Butane
- Chloroform
- Diethyl Ether (Ether)
- Enflurane
- Freon
- Gasoline (Petrol)
- Kerosene (Paraffin)
- Propane
- Toluene
κOR agonists- 2-EMSB
- 2-MMSB
- Alazocine
- Bremazocine
- Butorphanol
- Cyclazocine
- Cyprenorphine
- Dextrallorphan
- Dezocine
- Enadoline
- Herkinorin
- HZ-2
- Ibogaine
- Ketazocine
- Metazocine
- Nalbuphine
- Nalorphine
- Noribogaine
- Pentazocine
- Phenazocine
- Salvinorin A
- Spiradoline
- Tifluadom
- U-50,488
- U-69,593
- Dextrallorphan
- Dextromethorphan
- Dextrorphan
- Noscapine (Narcotine)
OthersStimulants (N06B) Adamantanes Adaphenoxate • Adapromine • Amantadine • Bromantane • Chlodantane • Gludantane • Memantine • Midantane
Adenosine antagonists 8-Chlorotheophylline • 8-Cyclopentyltheophylline • 8-Phenyltheophylline • Aminophylline • Caffeine • CGS-15943 • Dimethazan • Paraxanthine • SCH-58261 • Theobromine • TheophyllineAlkylamines Arylcyclohexylamines Benocyclidine • Dieticyclidine • Esketamine • Eticyclidine • Gacyclidine • Ketamine • Phencyclamine • Phencyclidine • Rolicyclidine • Tenocyclidine • Tiletamine
Benzazepines 6-Br-APB • SKF-77434 • SKF-81297 • SKF-82958
Cholinergics A-84543 • A-366,833 • ABT-202 • ABT-418 • AR-R17779 • Altinicline • Anabasine • Arecoline • Cotinine • Cytisine • Dianicline • Epibatidine • Epiboxidine • GTS-21 • Ispronicline • Nicotine • PHA-543,613 • PNU-120,596 • PNU-282,987 • Pozanicline • Rivanicline • Sazetidine A • SIB-1553A • SSR-180,711 • TC-1698 • TC-1827 • TC-2216 • TC-5619 • Tebanicline • UB-165 • Varenicline • WAY-317,538
Convulsants Anatoxin-a • Bicuculline • DMCM • Flurothyl • Gabazine • Pentetrazol • Picrotoxin • Strychnine • Thujone
Eugeroics Adrafinil • Armodafinil • CRL-40941 • Modafinil
Oxazolines 4-Methylaminorex • Aminorex • Clominorex • Cyclazodone • Fenozolone • Fluminorex • Pemoline • Thozalinone
Phenethylamines 1-(4-Methylphenyl)-2-aminobutane • 1-Phenyl-2-(piperidin-1-yl)pentan-3-one • 1-Methylamino-1-(3,4-methylenedioxyphenyl)propane • 2-Fluoroamphetamine • 2-Fluoromethamphetamine • 2-OH-PEA • 2-Phenyl-3-aminobutane • 2-Phenyl-3-methylaminobutane • 2,3-MDA • 3-Fluoroamphetamine • 3-Fluoroethamphetamine • 3-Fluoromethcathinone • 3-Methoxyamphetamine • 3-Methylamphetamine • 3,4-DMMC • 4-BMC • 4-Ethylamphetamine • 4-FA • 4-FMA • 4-MA • 4-MMA • 4-MTA • 6-FNE • Alfetamine • α-Ethylphenethylamine • Amfecloral • Amfepentorex • Amfepramone • Amidephrine • Amphetamine (Dextroamphetamine, Levoamphetamine) • Amphetaminil • Arbutamine • β-Methylphenethylamine • β-Phenylmethamphetamine • Benfluorex • Benzedrone • Benzphetamine • BDB (J) • BOH (Hydroxy-J) • BPAP • Buphedrone • Bupropion (Amfebutamone) • Butylone • Cathine • Cathinone • Chlorphentermine • Cinnamedrine • Clenbuterol • Clobenzorex • Cloforex • Clortermine • D-Deprenyl • Denopamine • Dimethoxyamphetamine • Dimethylamphetamine • Dimethylcathinone (Dimethylpropion, Metamfepramone) • Dobutamine • DOPA (Dextrodopa, Levodopa) • Dopamine • Dopexamine • Droxidopa • EBDB (Ethyl-J) • Ephedrine • Epinephrine (Adrenaline) • Epinine (Deoxyepinephrine) • Etafedrine • Ethcathinone (Ethylpropion) • Ethylamphetamine (Etilamfetamine) • Ethylnorepinephrine (Butanefrine) • Ethylone • Etilefrine • Famprofazone • Fenbutrazate • Fencamine • Fenethylline • Fenfluramine (Dexfenfluramine) • Fenmetramide • Fenproporex • Flephedrone • Fludorex • Furfenorex • Gepefrine • HMMA • Hordenine • Ibopamine • IMP • Indanylamphetamine • Isoetarine • Isoethcathinone • Isoprenaline (Isoproterenol) • L-Deprenyl (Selegiline) • Lefetamine • Lisdexamfetamine • Lophophine (Homomyristicylamine) • Manifaxine • MBDB (Methyl-J; "Eden") • MDA (Tenamfetamine) • MDBU • MDEA ("Eve") • MDMA ("Ecstasy", "Adam") • MDMPEA (Homarylamine) • MDOH • MDPR • MDPEA (Homopiperonylamine) • Mefenorex • Mephedrone • Mephentermine • Metanephrine • Metaraminol • Methamphetamine (Desoxyephedrine, Methedrine; Dextromethamphetamine, Levomethamphetamine) • Methoxamine • Methoxyphenamine • MMA • Methcathinone (Methylpropion) • Methedrone • Methoxyphenamine • Methylone • MMDA • MMDMA • MMMA • Morazone • N-Benzyl-1-phenethylamine • N,N-Dimethylphenethylamine • Naphthylamphetamine • Nisoxetine • Norepinephrine (Noradrenaline) • Norfenefrine • Norfenfluramine • Normetanephrine • Octopamine • Orciprenaline • Ortetamine • Oxilofrine • Paredrine (Norpholedrine, Oxamphetamine, Mycadrine) • PBA • PCA • PHA • Pargyline • Pentorex (Phenpentermine) • Pentylone • Phendimetrazine • Phenmetrazine • Phenpromethamine • Phentermine • Phenylalanine • Phenylephrine (Neosynephrine) • Phenylpropanolamine • Pholedrine • PIA • PMA • PMEA • PMMA • PPAP • Prenylamine • Propylamphetamine • Pseudoephedrine • Radafaxine • Ropinirole • Salbutamol (Albuterol; Levosalbutamol) • Sibutramine • Synephrine (Oxedrine) • Theodrenaline • Tiflorex (Flutiorex) • Tranylcypromine • Tyramine • Tyrosine • Xamoterol • Xylopropamine • Zylofuramine
Piperazines Piperidines 1-Benzyl-4-(2-(diphenylmethoxy)ethyl)piperidine • 1-(3,4-Dichlorophenyl)-1-(piperidin-2-yl)butane • 2-Benzylpiperidine • 2-Methyl-3-phenylpiperidine • 3,4-Dichloromethylphenidate • 4-Benzylpiperidine • 4-Methylmethylphenidate • Desoxypipradrol • Difemetorex • Diphenylpyraline • Ethylphenidate • Methylnaphthidate • Methylphenidate (Dexmethylphenidate) • N-Methyl-3β-propyl-4β-(4-chlorophenyl)piperidine • Nocaine • Phacetoperane • Pipradrol • SCH-5472
Pyrrolidines 2-Diphenylmethylpyrrolidine • α-PPP • α-PBP • α-PVP • Diphenylprolinol • MDPPP • MDPBP • MDPV • MPBP • MPHP • MPPP • MOPPP • Naphyrone • PEP • Prolintane • Pyrovalerone
Tropanes 3-CPMT • 3'-Chloro-3α-(diphenylmethoxy)tropane • 3-Pseudotropyl-4-fluorobenzoate • 4'-Fluorococaine • AHN-1055 • Altropane (IACFT) • Brasofensine • CFT (WIN 35,428) • β-CIT (RTI-55) • Cocaethylene • Cocaine • Dichloropane (RTI-111) • Difluoropine • FE-β-CPPIT • FP-β-CPPIT • Ioflupane (123I) • Norcocaine • PIT • PTT • RTI-31 • RTI-32 • RTI-51 • RTI-105 • RTI-112 • RTI-113 • RTI-117 • RTI-120 • RTI-121 (IPCIT) • RTI-126 • RTI-150 • RTI-154 • RTI-171 • RTI-177 • RTI-183 • RTI-193 • RTI-194 • RTI-199 • RTI-202 • RTI-204 • RTI-229 • RTI-241 • RTI-336 • RTI-354 • RTI-371 • RTI-386 • Salicylmethylecgonine • Tesofensine • Troparil (β-CPT, WIN 35,065-2) • Tropoxane • WF-23 • WF-33 • WF-60
Others 1-(Thiophen-2-yl)-2-aminopropane • 2-Amino-1,2-dihydronaphthalene • 2-Aminoindane • 2-Aminotetralin • 2-MDP • 2-Phenylcyclohexylamine • 2-Phenyl-3,6-dimethylmorpholine • 3-Benzhydrylmorpholine • 3,3-Diphenylcyclobutanamine • 5-(2-Aminopropyl)indole • 5-Iodo-2-aminoindane • AL-1095 • Amfonelic acid • Amineptine • Amiphenazole • Atipamezole • Atomoxetine (Tomoxetine) • Bemegride • Benzydamine • BTQ • BTS 74,398 • Carphedon • Ciclazindol • Cilobamine • Clofenciclan • Cropropamide • Crotetamide • Cypenamine • D-161 • Diclofensine • Dimethocaine • Efaroxan • Etamivan • EXP-561 • Fencamfamine • Fenpentadiol • Feprosidnine • G-130 • Gamfexine • Gilutensin • GSK1360707F • GYKI-52895 • Hexacyclonate • Idazoxan • Indanorex • Indatraline • JNJ-7925476 • JZ-IV-10 • Lazabemide • Leptacline • Levopropylhexedrine • Lomevactone • LR-5182 • Mazindol • Meclofenoxate • Medifoxamine • Mefexamide • Mesocarb • Methastyridone • Methiopropamine • N-Methyl-3-phenylnorbornan-2-amine • Nefopam • Nikethamide • Nomifensine • O-2172 • Oxaprotiline • Phthalimidopropiophenone • PNU-99,194 • Propylhexedrine • PRC200-SS • Rasagiline • Rauwolscine • Rubidium chloride • Setazindol • Tametraline • Tandamine • Trazium • UH-232 • Yohimbine
See also Sympathomimetic aminesAnesthetic: General anesthetics (N01A) Inhalation OthersInjection OthersNeurotoxins Animal Poisons & Venoms: Batrachotoxin • Bestoxin • Birtoxin • Bungarotoxin • Charybdotoxin • Conotoxin • Saxitoxin • Tetrodotoxin
Neurotoxic drugs: Amphetamine • Lisdexamfetamine • Methamphetamine • αET • αMT • MBDB • MDA • MDEA • MDMA (Ecstasy) • PBA • PCA • PIA • 1,4-BD • GBL • GHB • Ibotenic Acid • Dizocilpine (MK-801) • Ketamine • Phencyclidine (PCP) • 5,7-DHT • 6-OHDA • MPTP/MPP+ • Norsalsolinol • Ethanol (Alcohol)
Bacterial toxins: Botulinum toxin • Tetanospasmin
Fungal toxins: Bicuculline
Plant toxins: Penitrem A • Picrotoxin
Pesticides: Rotenone
Nerve agents: Cyclosarin EA-3148 • GV (nerve agent) • Novichok agent • Sarin • Soman • Tabun (nerve agent) • VE (nerve agent) • VG (nerve agent) • VM (nerve agent) • VR (nerve agent) • VX (nerve agent)
Neurotransmitters and precursors: Dopamine • Glutamate • L-Tyrosine • L-Phenylalanine • L-DOPA (Levodopa) • L-GlutamineCholinergics Receptor ligands Agonists: 77-LH-28-1 • AC-42 • AC-260,584 • Aceclidine • Acetylcholine • AF30 • AF150(S) • AF267B • AFDX-384 • Alvameline • AQRA-741 • Arecoline • Bethanechol • Butyrylcholine • Carbachol • CDD-0034 • CDD-0078 • CDD-0097 • CDD-0098 • CDD-0102 • Cevimeline • cis-Dioxolane • Ethoxysebacylcholine • LY-593,039 • L-689,660 • LY-2,033,298 • McNA343 • Methacholine • Milameline • Muscarine • NGX-267 • Ocvimeline • Oxotremorine • PD-151,832 • Pilocarpine • RS86 • Sabcomeline • SDZ 210-086 • Sebacylcholine • Suberylcholine • Talsaclidine • Tazomeline • Thiopilocarpine • Vedaclidine • VU-0029767 • VU-0090157 • VU-0152099 • VU-0152100 • VU-0238429 • WAY-132,983 • Xanomeline • YM-796
Antagonists: 3-Quinuclidinyl Benzilate • 4-DAMP • Aclidinium Bromide • Anisodamine • Anisodine • Atropine • Atropine Methonitrate • Benactyzine • Benzatropine (Benztropine) • Benzydamine • BIBN 99 • Biperiden • Bornaprine • CAR-226,086 • CAR-301,060 • CAR-302,196 • CAR-302,282 • CAR-302,368 • CAR-302,537 • CAR-302,668 • CS-27349 • Cyclobenzaprine • Cyclopentolate • Darifenacin • DAU-5884 • Dimethindene • Dexetimide • DIBD • Dicyclomine (Dicycloverine) • Ditran • EA-3167 • EA-3443 • EA-3580 • EA-3834 • Elemicin • Etanautine • Etybenzatropine (Ethylbenztropine) • Flavoxate • Himbacine • HL-031,120 • Ipratropium bromide • J-104,129 • Hyoscyamine • Mamba Toxin 3 • Mamba Toxin 7 • Mazaticol • Mebeverine • Methoctramine • Metixene • Myristicin • N-Ethyl-3-Piperidyl Benzilate • N-Methyl-3-Piperidyl Benzilate • Orphenadrine • Otenzepad • Oxybutynin • PBID • PD-102,807 • PD-0298029 • Phenglutarimide • Phenyltoloxamine • Pirenzepine • Piroheptine • Procyclidine • Profenamine • RU-47,213 • SCH-57,790 • SCH-72,788 • SCH-217,443 • Scopolamine (Hyoscine) • Solifenacin • Telenzepine • Tiotropium bromide • Tolterodine • Trihexyphenidyl • Tripitamine • Tropatepine • Tropicamide • WIN-2299 • Xanomeline • Zamifenacin; Others: 1st Generation Antihistamines (Brompheniramine, chlorphenamine, cyproheptadine, dimenhydrinate, diphenhydramine, doxylamine, mepyramine/pyrilamine, phenindamine, pheniramine, tripelennamine, triprolidine, etc) • Tricyclic Antidepressants (Amitriptyline, doxepin, trimipramine, etc) • Tetracyclic Antidepressants (Amoxapine, maprotiline, etc) • Typical Antipsychotics (Chlorpromazine, thioridazine, etc) • Atypical Antipsychotics (Clozapine, olanzapine, quetiapine, etc)Agonists: 5-HIAA • A-84,543 • A-366,833 • A-582,941 • A-867,744 • ABT-202 • ABT-418 • ABT-560 • ABT-894 • Acetylcholine • Altinicline • Anabasine • Anatoxin-a • AR-R17779 • Butyrylcholine • Carbachol • Cotinine • Cytisine • Decamethonium • Desformylflustrabromine • Dianicline • Dimethylphenylpiperazinium • Epibatidine • Epiboxidine • Ethanol • Ethoxysebacylcholine • EVP-4473 • EVP-6124 • Galantamine • GTS-21 • Ispronicline • Lobeline • MEM-63,908 (RG-3487) • Nicotine • NS-1738 • PHA-543,613 • PHA-709,829 • PNU-120,596 • PNU-282,987 • Pozanicline • Rivanicline • Sazetidine A • Sebacylcholine • SIB-1508Y • SIB-1553A • SSR-180,711 • Suberylcholine • TC-1698 • TC-1734 • TC-1827 • TC-2216 • TC-5214 • TC-5619 • TC-6683 • Tebanicline • Tropisetron • UB-165 • Varenicline • WAY-317,538 • XY-4083
Antagonists: 18-Methoxycoronaridine • α-Bungarotoxin • α-Conotoxin • Alcuronium • Amantadine • Anatruxonium • Atracurium • Bupropion (Amfebutamone) • Chandonium • Chlorisondamine • Cisatracurium • Coclaurine • Coronaridine • Dacuronium • Decamethonium • Dextromethorphan • Dextropropoxyphene • Dextrorphan • Diadonium • DHβE • Dimethyltubocurarine (Metocurine) • Dipyrandium • Dizocilpine (MK-801) • Doxacurium • Duador • Esketamine • Fazadinium • Gallamine • Hexafluronium • Hexamethonium (Benzohexonium) • Ibogaine • Isoflurane • Ketamine • Kynurenic acid • Laudexium (Laudolissin) • Levacetylmethadol • Malouetine • Mecamylamine • Memantine • Methadone • Methorphan (Racemethorphan) • Methyllycaconitine • Metocurine • Mivacurium • Morphanol (Racemorphanol) • Neramexane • Nitrous Oxide • Pancuronium • Pempidine • Pentamine • Pentolinium • Phencyclidine • Pipecuronium • Radafaxine • Rapacuronium • Rocuronium • Surugatoxin • Suxamethonium (Succinylcholine) • Thiocolchicoside • Toxiferine • Trimethaphan • Tropeinium • Tubocurarine • Vecuronium • XenonReuptake inhibitors PlasmalemmalCHT InhibitorsHemicholinium-3 (Hemicholine; HC3) • TriethylcholineVAChT InhibitorsEnzyme inhibitors ChAT inhibitors1-(-Benzoylethyl)pyridinium • 2-(α-Naphthoyl)ethyltrimethylammonium • 3-Chloro-4-stillbazole • 4-(1-Naphthylvinyl)pyridine • Acetylseco hemicholinium-3 • Acryloylcholine • AF64A • B115 • BETA • CM-54,903 • CatabolismAChE inhibitorsReversible: Carbamates: Aldicarb • Bendiocarb • Bufencarb • Carbaryl • Carbendazim • Carbetamide • Carbofuran • Chlorbufam • Chloropropham • Ethienocarb • Ethiofencarb • Fenobucarb • Fenoxycarb • Formetanate • Furadan • Ladostigil • Methiocarb • Methomyl • Miotine • Oxamyl • Phenmedipham • Pinmicarb • Pirimicarb • Propamocarb • Propham • Propoxur; Stigmines: Ganstigmine • Neostigmine • Phenserine • Physostigmine • Pyridostigmine • Rivastigmine; Others: Acotiamide • Ambenonium • Donepezil • Edrophonium • Galantamine • Huperzine A • Minaprine • Tacrine • Zanapezil
Irreversible: Organophosphates: Acephate • Azinphos-methyl • Bensulide • Cadusafos • Chlorethoxyfos • Chlorfenvinphos • Chlorpyrifos • Chlorpyrifos-Methyl • Coumaphos • Cyclosarin (GF) • Demeton • Demeton-S-Methyl • Diazinon • Dichlorvos • Dicrotophos • Diisopropyl fluorophosphate (Guthion) • Diisopropylphosphate • Dimethoate • Dioxathion • Disulfoton • EA-3148 • Echothiophate • Ethion • Ethoprop • Fenamiphos • Fenitrothion • Fenthion • Fosthiazate • GV • Isofluorophate • Isoxathion • Malaoxon • Malathion • Methamidophos • Methidathion • Metrifonate • Mevinphos • Monocrotophos • Naled • Novichok agent • Omethoate • Oxydemeton-Methyl • Paraoxon • Parathion • Parathion-Methyl • Phorate • Phosalone • Phosmet • Phostebupirim • Phoxim • Pirimiphos-Methyl • Sarin (GB) • Soman (GD) • Tabun (GA) • Temefos • Terbufos • Tetrachlorvinphos • Tribufos • Trichlorfon • VE • VG • VM • VR • VX; Others: Demecarium • Onchidal (Onchidella binneyi)BChE inhibitorsCymserine * Many of the acetylcholinesterase inhibitors listed above act as butyrylcholinesterase inhibitors.Others Choline (Lecithin) • Citicoline • Cyprodenate • Dimethylethanolamine (DMAE, deanol) • Glycerophosphocholine • Meclofenoxate (Centrophenoxine) • Phosphatidylcholine • Phosphatidylethanolamine • Phosphorylcholine • PirisudanolOthersAcetylcholine releasing agents: α-Latrotoxin • β-Bungarotoxin; Acetylcholine release inhibitors: Botulinum toxin (Botox); Acetylcholinesterase reactivators: Asoxime • Obidoxime • PralidoximeDopaminergics Receptor ligands AgonistsAdamantanes: Amantadine • Memantine • Rimantadine; Aminotetralins: 7-OH-DPAT • 8-OH-PBZI • Rotigotine • UH-232; Benzazepines: 6-Br-APB • Fenoldopam • SKF-38,393 • SKF-77,434 • SKF-81,297 • SKF-82,958 • SKF-83,959; Ergolines: Bromocriptine • Cabergoline • Dihydroergocryptine • Lisuride • LSD • Pergolide; Dihydrexidine derivatives: 2-OH-NPA • A-86,929 • Ciladopa • Dihydrexidine • Dinapsoline • Dinoxyline • Doxanthrine; Others: A-68,930 • A-77,636 • A-412,997 • ABT-670 • ABT-724 • Aplindore • Apomorphine • Aripiprazole • Bifeprunox • BP-897 • CY-208,243 • Dizocilpine • Etilevodopa • Flibanserin • Ketamine • Melevodopa • Modafinil • Pardoprunox • Phencyclidine • PD-128,907 • PD-168,077 • PF-219,061 • Piribedil • Pramipexole • Propylnorapomorphine • Pukateine • Quinagolide • Quinelorane • Quinpirole • RDS-127 • Ro10-5824 • Ropinirole • Rotigotine • Roxindole • Salvinorin A • SKF-89,145 • Sumanirole • Terguride • Umespirone • WAY-100,635AntagonistsTypical antipsychotics: Acepromazine • Azaperone • Benperidol • Bromperidol • Clopenthixol • Chlorpromazine • Chlorprothixene • Droperidol • Flupentixol • Fluphenazine • Fluspirilene • Haloperidol • Loxapine • Mesoridazine • Methotrimeprazine • Nemonapride • Penfluridol • Perazine • Periciazine • Perphenazine • Pimozide • Prochlorperazine • Promazine • Sulforidazine • Sulpiride • Sultopride • Thioridazine • Thiothixene • Trifluoperazine • Triflupromazine • Trifluperidol • Zuclopenthixol; Atypical antipsychotics: Amisulpride • Asenapine • Blonanserin • Cariprazine • Carpipramine • Clocapramine • Clozapine • Gevotroline • Iloperidone • Lurasidone • Melperone • Molindone • Mosapramine • Olanzapine • Paliperidone • Perospirone • Piquindone • Quetiapine • Remoxipride • Risperidone • Sertindole • Tiospirone • Ziprasidone • Zotepine; Antiemetics: AS-8112 • Alizapride • Bromopride • Clebopride • Domperidone • Metoclopramide • Thiethylperazine; Others: Amoxapine • Buspirone • Butaclamol • Ecopipam • EEDQ • Eticlopride • Fananserin • L-745,870 • Nafadotride • Nuciferine • PNU-99,194 • Raclopride • Sarizotan • SB-277,011-A • SCH-23,390 • SKF-83,959 • Sonepiprazole • Spiperone • Spiroxatrine • Stepholidine • Tetrahydropalmatine • Tiapride • UH-232 • YohimbineReuptake inhibitors PlasmalemmalDAT inhibitorsPiperazines: DBL-583 • GBR-12,935 • Nefazodone • Vanoxerine; Piperidines: BTCP • Desoxypipradrol • Dextromethylphenidate • Difemetorex • Ethylphenidate • Methylnaphthidate • Methylphenidate • Phencyclidine • Pipradrol; Pyrrolidines: Diphenylprolinol • Methylenedioxypyrovalerone (MDPV) • Naphyrone • Prolintane • Pyrovalerone; Tropanes: β-CPPIT • Altropane • Brasofensine • CFT • Cocaine • Dichloropane • Difluoropine • FE-β-CPPIT • FP-β-CPPIT • Ioflupane (123I) • Iometopane • RTI-112 • RTI-113 • RTI-121 • RTI-126 • RTI-150 • RTI-177 • RTI-229 • RTI-336 • Tenocyclidine • Tesofensine • Troparil • Tropoxane • WF-11 • WF-23 • WF-31 • WF-33; Others: Adrafinil • Armodafinil • Amfonelic acid • Amineptine • Benzatropine (Benztropine) • Bromantane • BTQ • BTS-74,398 • Bupropion (Amfebutamone) • Ciclazindol • Diclofensine • Dimethocaine • Diphenylpyraline • Dizocilpine • DOV-102,677 • DOV-21,947 • DOV-216,303 • Etybenzatropine (Ethylbenztropine) • EXP-561 • Fencamine • Fencamfamine • Fezolamine • GYKI-52,895 • Indatraline • Ketamine • Lefetamine • Levophacetoperane • LR-5182 • Manifaxine • Mazindol • Medifoxamine • Mesocarb • Modafinil • Nefopam • Nomifensine • NS-2359 • O-2172 • Pridefrine • Propylamphetamine • Radafaxine • SEP-225,289 • SEP-227,162 • Sertraline • Sibutramine • Tametraline • Tedatioxetine • TripelennamineVMAT inhibitorsReleasing agents Morpholines: Fenbutrazate • Morazone • Phendimetrazine • Phenmetrazine; Oxazolines: 4-Methylaminorex (4-MAR, 4-MAX) • Aminorex • Clominorex • Cyclazodone • Fenozolone • Fluminorex • Pemoline • Thozalinone; Phenethylamines (also amphetamines, cathinones, phentermines, etc): 2-Hydroxyphenethylamine (2-OH-PEA) • 4-CAB • 4-Methylamphetamine (4-MA) • 4-Methylmethamphetamine (4-MMA) • Alfetamine • Amfecloral • Amfepentorex • Amfepramone • Amphetamine (Dextroamphetamine, Levoamphetamine) • Amphetaminil • β-Methylphenethylamine (β-Me-PEA) • Benzodioxolylbutanamine (BDB) • Benzodioxolylhydroxybutanamine (BOH) • Benzphetamine • Buphedrone • Butylone • Cathine • Cathinone • Clobenzorex • Clortermine • D-Deprenyl • Dimethoxyamphetamine (DMA) • Dimethoxymethamphetamine (DMMA) • Dimethylamphetamine • Dimethylcathinone (Dimethylpropion, metamfepramone) • Ethcathinone (Ethylpropion) • Ethylamphetamine • Ethylbenzodioxolylbutanamine (EBDB) • Ethylone • Famprofazone • Fenethylline • Fenproporex • Flephedrone • Fludorex • Furfenorex • Hordenine • Lophophine (Homomyristicylamine) • Mefenorex • Mephedrone • Methamphetamine (Desoxyephedrine, Methedrine; Dextromethamphetamine, Levomethamphetamine) • Methcathinone (Methylpropion) • Methedrone • Methoxymethylenedioxyamphetamine (MMDA) • Methoxymethylenedioxymethamphetamine (MMDMA) • Methylbenzodioxolylbutanamine (MBDB) • Methylenedioxyamphetamine (MDA, tenamfetamine) • Methylenedioxyethylamphetamine (MDEA) • Methylenedioxyhydroxyamphetamine (MDOH) • Methylenedioxymethamphetamine (MDMA) • Methylenedioxymethylphenethylamine (MDMPEA, homarylamine) • Methylenedioxyphenethylamine (MDPEA, homopiperonylamine) • Methylone • Ortetamine • Parabromoamphetamine (PBA) • Parachloroamphetamine (PCA) • Parafluoroamphetamine (PFA) • Parafluoromethamphetamine (PFMA) • Parahydroxyamphetamine (PHA) • Paraiodoamphetamine (PIA) • Paredrine (Norpholedrine, Oxamphetamine) • Phenethylamine (PEA) • Pholedrine • Phenpromethamine • Prenylamine • Propylamphetamine • Tiflorex (Flutiorex) • Tyramine (TRA) • Xylopropamine • Zylofuramine; Piperazines: 2,5-Dimethoxy-4-bromobenzylpiperazine (2C-B-BZP) • Benzylpiperazine (BZP) • Methoxyphenylpiperazine (MeOPP, paraperazine) • Methylbenzylpiperazine (MBZP) • Methylenedioxybenzylpiperazine (MDBZP, piperonylpiperazine); Others: 2-Amino-1,2-dihydronaphthalene (2-ADN) • 2-Aminoindane (2-AI) • 2-Aminotetralin (2-AT) • 4-Benzylpiperidine (4-BP) • 5-IAI • Clofenciclan • Cyclopentamine • Cypenamine • Cyprodenate • Feprosidnine • Gilutensin • Heptaminol • Hexacyclonate • Indanylaminopropane (IAP) • Indanorex • Isometheptene • Methylhexanamine • Naphthylaminopropane (NAP) • Octodrine • Phthalimidopropiophenone • Propylhexedrine (Levopropylhexedrine) • Tuaminoheptane (Tuamine)Enzyme inhibitors PAH inhibitors3,4-DihydroxystyreneTH inhibitorsNonselective: Benmoxin • Caroxazone • Echinopsidine • Furazolidone • Hydralazine • Indantadol • Iproclozide • Iproniazid • Isocarboxazid • Isoniazid • Linezolid • Mebanazine • Metfendrazine • Nialamide • Octamoxin • Paraxazone • Phenelzine • Pheniprazine • Phenoxypropazine • Pivalylbenzhydrazine • Procarbazine • Safrazine • Tranylcypromine; MAO-A selective: Amiflamine • Bazinaprine • Befloxatone • Befol • Brofaromine • Cimoxatone • Clorgiline • Esuprone • Harmala alkaloids • Methylene Blue • Metralindole • Minaprine • Moclobemide • Pirlindole • Sercloremine • Tetrindole • Toloxatone • Tyrima; MAO-B selective: D-Deprenyl • L-Deprenyl (Selegiline) • Ladostigil • Lazabemide • Milacemide • Pargyline • Rasagiline • SafinamideDBH inhibitorsOthers L-Phenylalanine → L-Tyrosine → L-DOPA (Levodopa)Ferrous iron (Fe2+) • Tetrahydrobiopterin • Vitamin B3 (Niacin, Nicotinamide → NADPH) • Vitamin B6 (Pyridoxine, Pyridoxamine, Pyridoxal → Pyridoxal phosphate) • Vitamin B9 (Folic acid → Tetrahydrofolic acid) • Vitamin C (Ascorbic acid) • Zinc (Zn2+)OthersActivity enhancers: Benzofuranylpropylaminopentane (BPAP) • Phenylpropylaminopentane (PPAP); Toxins: Oxidopamine (6-Hydroxydopamine)List of dopaminergic drugsGlutamatergics Ionotropic Agonists: 5-Fluorowillardiine • AMPA • Domoic acid • Quisqualic acid; Positive allosteric modulators: Aniracetam • Cyclothiazide • CX-516 • CX-546 • CX-614 • CX-691 • CX-717 • Diazoxide • HCTZ • IDRA-21 • LY-392,098 • LY-404,187 • LY-451,395 • LY-451,646 • LY-503,430 • Oxiracetam • PEPA • Piracetam • Pramiracetam • S-18986 • Sunifiram • Unifiram
Antagonists: ATPO • Barbiturates • Caroverine • CNQX • DNQX • GYKI-52466 • NBQX • Perampanel • Talampanel • Tezampanel • Topiramate; Negative allosteric modulators: GYKI-53,655Agonists: Glutamate/acite site competitive agonists: Aspartate • Glutamate • Homoquinolinic acid • Ibotenic acid • NMDA • Quinolinic acid • Tetrazolylglycine; Glycine site agonists: ACBD • ACPC • ACPD • Alanine • CCG • Cycloserine • DHPG • Fluoroalanine • Glycine • HA-966 • L-687,414 • Milacemide • Sarcosine • Serine • Tetrazolylglycine; Polyamine site agonists: Acamprosate • Spermidine • Spermine
Antagonists: Competitive antagonists: AP5 (APV) • AP7 • CGP-37849 • CGP-39551 • CGP-39653 • CGP-40116 • CGS-19755 • CPP • LY-233,053 • LY-235,959 • LY-274,614 • MDL-100,453 • Midafotel (d-CPPene) • NPC-12,626 • NPC-17,742 • PBPD • PEAQX • Perzinfotel • PPDA • SDZ-220581 • Selfotel; Noncompetitive antagonists: ARR-15,896 • Caroverine • Dexanabinol • FPL-12495 • FR-115,427 • Hodgkinsine • Magnesium • MDL-27,266 • NPS-1506 • Psychotridine • Zinc; Uncompetitive pore blockers: 2-MDP • 3-MeO-PCP • 8A-PDHQ • Alaproclate • Amantadine • Aptiganel • ARL-12,495 • ARL-15,896-AR • ARL-16,247 • Budipine • Delucemine • Dexoxadrol • Dextrallorphan • Dieticyclidine • Dizocilpine • Endopsychosin • Esketamine • Etoxadrol • Eticyclidine • Gacyclidine • Ibogaine • Indantadol • Ketamine • Ketobemidone • Loperamide • Memantine • Meperidine (Pethidine) • Methadone • Methorphan (Dextromethorphan, Levomethorphan) • Methoxetamine • Milnacipran • Morphanol (Dextrorphan, Levorphanol) • NEFA • Neramexane • Nitrous oxide • Noribogaine • Orphenadrine • PCPr • Phencyclamine • Phencyclidine • Propoxyphene • Remacemide • Rhynchophylline • Riluzole • Rimantadine • Rolicyclidine • Sabeluzole • Tenocyclidine • Tiletamine • Tramadol • Xenon; Glycine site antagonists: ACEA-1021 • ACEA-1328 • ACPC • Carisoprodol • CGP-39653 • CKA • DCKA • Felbamate • Gavestinel • GV-196,771 • Kynurenic acid • L-689,560 • L-701,324 • Lacosamide • Licostinel • LU-73,068 • MDL-105,519 • Meprobamate • MRZ 2/576 • PNQX • ZD-9379; NR2B subunit antagonists: Besonprodil • CO-101,244 (PD-174,494) • CP-101,606 • Eliprodil • Haloperidol • Ifenprodil • Isoxsuprine • Nylidrin • Ro8-4304 • Ro25-6981 • Traxoprodil; Polyamine site antagonists: Arcaine • Co 101676 • Diaminopropane • Acamprosate • Diethylenetriamine • Huperzine A • Putrescine • Ro 25-6981; Unclassified/unsorted antagonists: Chloroform • Diethyl ether • Enflurane • Ethanol (Alcohol) • Halothane • Isoflurane • Methoxyflurane • Toluene • Trichloroethane • Trichloroethanol • Trichloroethylene • XyleneAgonists: 5-Iodowillardiine • ATPA • Domoic acid • Kainic acid • LY-339,434 • SYM-2081
Antagonists: CNQX • DNQX • LY-382,884 • NBQX • NS102 • Tezampanel • Topiramate • UBP-302; Negative allosteric modulators: NS-3763Metabotropic Agonists: Unselective: ACPD • DHPG • Quisqualic acid; mGlu1-selective: Ro01-6128 • Ro67-4853 • Ro67-7476 • VU-71; mGlu5-selective: ADX-47273 • CDPPB • CHPG • DFB • VU-1545
Antagonists: Unselective: MCPG • NPS-2390; mGlu1-selective: BAY 36-7620 • CPCCOEt • LY-367,385 • LY-456,236; mGlu5-selective: Dipraglurant • DMeOB • Fenobam • LY-344,545 • MPEP • MTEP • SIB-1757 • SIB-1893Agonists: Unselective: L-AP4; mGlu4-selective: PHCCC • VU-001,171 • VU-0155,041; mGlu7-selective: AMN082; mGlu8-selective: DCPG
Antagonists: Unselective: CPPG • MAP4 • MSOP • MPPG • MTPG • UBP-1112; mGlu7-selective: MMPIPTransporter
inhibitorsDHKA • PDC • WAY-213,613vGluTs7-CKA • Evans blueOpioids Opium and
poppy straw
derivativesCrude opiate extracts/
whole opium productsCompote/Kompot/Polish heroin • Diascordium • B & O Supprettes • Dover's powder • Kendal Black Drop • Laudanum • Mithridate • Opium • Paregoric • Poppy straw concentrate • Poppy tea • Smoking opium • Theriac
Natural opiates Opium alkaloids
see also: Components of opiumCodeine • Morphine • Oripavine • Pseudomorphine • Thebaine
Alkaloid salts mixtures Semisynthetics
including
Bentley compoundsMorphine family 3,6-diesters of morphine Acetylpropionylmorphine • Diacetyldihydromorphine (Dihydroheroin, Acetylmorphinol) • Dibenzoylmorphine • Dipropanoylmorphine • Heroin (Diacetylmorphine) • Nicomorphine
Codeine-dionine family Morphinones and morphols 14-Cinnamoyloxycodeinone • 14-Ethoxymetopon • 14-Methoxymetopon • 14-Phenylpropoxymetopon • 7-Spiroindanyloxymorphone • Acetylmorphone • Codeinone • Codorphone • Codoxime • Thebacon (Acetyldihydrocodeinone / Dihydrocodeinone enol acetate) • Hydrocodone • Hydromorphone • Metopon • Morphinone • N-Phenethyl-14-ethoxymetopon • Oxycodone • Oxymorphol • Oxymorphone • Pentamorphone • Semorphone
Morphides Dihydrocodeine series 14-hydroxydihydrocodeine • Acetyldihydrocodeine • Dihydrocodeine • Nicocodeine • Nicodicodeine
Nitrogen morphine derivatives Hydrazones Halogenated morphine derivatives 1-Iodomorphine
Active opiate
metabolitesMorphine-6-glucuronide • 6-Monoacetylmorphine • Norcodeine • Normorphine
Morphinans Morphinan series Cyclorphan • Dextrallorphan • Levorphanol • Levophenacylmorphan • Levomethorphan • Norlevorphanol • Oxilorphan • Phenomorphan • Methorphan / Racemethorphan • Morphanol / Racemorphanol • Ro4-1539 • Xorphanol
Others Benzomorphans 8-Carboxamidocyclazocine • Alazocine • Bremazocine • Dezocine • Ketazocine • Metazocine • Pentazocine • Phenazocine
4-Phenylpiperidines Pethidines
(Meperidines)4-Fluoromeperidine • Allylnorpethidine • Anileridine • Benzethidine • Carperidine • Difenoxin • Diphenoxylate • Etoxeridine (Carbetidine) • Furethidine • Hydroxypethidine (Bemidone) • Morpheridine • Oxpheneridine (Carbamethidine) • Pethidine (Meperidine) • Pethidine Intermediate A • Pethidine Intermediate B (Norpethidine) • Pethidine Intermediate C (Pethidinic Acid) • Pheneridine • Phenoperidine • Piminodine • Properidine (Ipropethidine) • Sameridine
Prodines Ketobemidones Others Open chain
opioidsAmidones Methadols Moramides Dextromoramide • Levomoramide • Racemoramide
Thiambutenes Phenalkoxams Ampromides Others IC-26 • Isoaminile • Lefetamine • R-4066
Anilidopiperidines 3-Allylfentanyl • 3-Methylfentanyl • 3-Methylthiofentanyl • 4-Phenylfentanyl • Alfentanil • α-methylacetylfentanyl • α-methylfentanyl • α-methylthiofentanyl • β-hydroxyfentanyl • β-hydroxythiofentanyl • β-methylfentanyl • Brifentanil • Carfentanil • Fentanyl • Lofentanil • Mirfentanil • Ocfentanil • Ohmefentanyl • Parafluorofentanyl • Phenaridine • Remifentanil • Sufentanil • Thiofentanyl • Trefentanil
Oripavine
derivativesPhenazepanes Pirinitramides Benzimidazoles Indoles Diphenylmethylpiperazines Opioid peptides
see also: Opioid neuropeptidesAdrenorphin • Amidorphin • Casomorphin • DADLE • DAMGO • Dermorphin • Dynorphin • Endomorphin • Endorphins • Enkephalin • Gliadorphin • Morphiceptin • Nociceptin • Octreotide • Opiorphin • Rubiscolin • TRIMU 5
Others AD-1211 • AH-7921 • Azaprocin • BDPC • BRL-52537 • Bromadoline • C-8813 • Ciramadol • Doxpicomine • Enadoline • Faxeladol • GR-89696 • Herkinorin • ICI-199,441 • ICI-204,448 • J-113,397 • JTC-801 • Ketamine • LPK-26 • Methopholine • MT-45 • N-Desmethylclozapine • NNC 63-0532 • Nortilidine • O-Desmethyltramadol • Phencyclidine • Prodilidine • Profadol • Ro64-6198 • Salvinorin A • SB-612,111 • SC-17599 • RWJ-394,674 • TAN-67 • Tapentadol • Tifluadom • Tilidine • Tramadol • Trimebutine • U-50,488 • U-69,593 • Viminol • W-18
Opioid antagonists
&
inverse agonists5'-Guanidinonaltrindole • Alvimopan • Chlornaltrexamine • Cyclazocine • Cyprodime • Diprenorphine (M5050) • JDTic • Levallorphan • Methylnaltrexone • Nalfurafine • Nalmefene • Naloxazone • Naloxonazine • Naloxone • Nalorphine • Naltrexol-d4 • Naltrexone • Naltriben • Naltrindole • Norbinaltorphimine • Oxilorphan
List of opioidsCategories:- General anesthetics
- German inventions
- Dissociative drugs
- NMDA receptor antagonists
- Piperidines
- Sigma agonists
- Euphoriants
Wikimedia Foundation. 2010.
Look at other dictionaries:
Phencyclidine — Structure de la phencyclidine Général Nom IUPAC 1 (1 phenylcyclohexyl) pipéridine … Wikipédia en Français
phencyclidine — ● phencyclidine nom féminin Anesthésique et stupéfiant doté de propriétés hallucinogènes, d une grande toxicité. (Nom usuel : poudre d ange.) … Encyclopédie Universelle
phencyclidine — [fen sik′lə din, fensī′klədin; fen sik′lə dēn, fen sī′klədēn΄] n. see PCP1 … English World dictionary
Phéncyclidine — « Angel dust » redirige ici. Pour l album de Faith No More, voir Angel Dust. Phéncyclidine … Wikipédia en Français
phencyclidine — noun a drug used as an anesthetic by veterinarians; illicitly taken (originally in the form of powder or dust ) for its effects as a hallucinogen • Syn: ↑phencyclidine hydrochloride, ↑PCP, ↑angel dust • Hypernyms: ↑hallucinogen, ↑hallucinogenic… … Useful english dictionary
phencyclidine-induced hallucination — Phencyclidine is known under many names, including angel dust, angeldustine, and rocket fuel. The term is a truncation of the chemical name 1 (1 phenylcyclohexyl)piperidine. Abbreviated to PCP, it is classified as a dissociative anaesthetic… … Dictionary of Hallucinations
Phencyclidine (data page) — OrganicBox complete synthetic=yes wiki name=Phencyclidine name=1 (1 phenylcyclohexyl)piperidine ref N|1|a = GENERAL INFORMATION = C=17 | H=25 | N=1 mass=243.387 ref N|1|b abbreviation=PCP synonyms=Angel {dust/hair/mist} Animal tranquilizer Aurora … Wikipedia
phencyclidine hydrochloride — noun a drug used as an anesthetic by veterinarians; illicitly taken (originally in the form of powder or dust ) for its effects as a hallucinogen • Syn: ↑phencyclidine, ↑PCP, ↑angel dust • Hypernyms: ↑hallucinogen, ↑hallucinogenic drug,… … Useful english dictionary
phencyclidine — noun Etymology: phen + cycl + idine Date: 1959 a piperidine derivative C17H25N used chiefly in the form of its hydrochloride especially as a veterinary anesthetic and sometimes illicitly as a psychedelic drug called also angel dust, PCP … New Collegiate Dictionary
phencyclidine — (= 1 (1 phenylcyclohexyl) piperidine; Angel dust; PCP) Anaesthetic and drug of a kind that can produce marked behavioural effects. Interacts with the NMDA receptor … Dictionary of molecular biology
 18+© Academic, 2000-2025
18+© Academic, 2000-2025- Contact us: Technical Support, Advertising
Dictionaries export, created on PHP, Joomla, Drupal, WordPress, MODx.
- InChI=1S/C17H25N/c1-4-10-16(11-5-1)17(12-6-2-7-13-17)18-14-8-3-9-15-18/h1,4-5,10-11H,2-3,6-9,12-15H2