- Rasagiline
-
Rasagiline 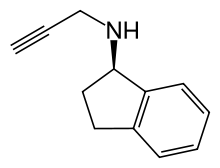

Systematic (IUPAC) name (R)-N-(prop-2-ynyl)-2,3-dihydro-1H-inden-1-amine Clinical data Trade names Azilect AHFS/Drugs.com monograph MedlinePlus a606017 Pregnancy cat. C Legal status ℞ Prescription only Routes Oral Pharmacokinetic data Bioavailability 36% Protein binding 88 – 94% Metabolism Hepatic (CYP1A2-mediated) Half-life 3 hours Excretion Renal and fecal Identifiers CAS number 1875-50-9 
ATC code N04BD02 PubChem CID 3052776 DrugBank DB01367 ChemSpider 2314553 UNII 003N66TS6T 
KEGG D02562 ChEMBL CHEMBL887 Chemical data Formula C12H13N Mol. mass 171.238 g/mol SMILES eMolecules & PubChem - InChI=1S/C12H13N/c1-2-9-13-12-8-7-10-5-3-4-6-11(10)12/h1,3-6,12-13H,7-9H2/t12-/m1/s1
Key:RUOKEQAAGRXIBM-GFCCVEGCSA-N
 (what is this?) (verify)
(what is this?) (verify)Rasagiline (Azilect, AGN 1135) is an irreversible inhibitor of monoamine oxidase[1] used as a monotherapy in early Parkinson's disease or as an adjunct therapy in more advanced cases.[2] It is selective for MAO type B over type A by a factor of fourteen.[3]
It was developed by Teva Neuroscience[4], initially investigated by Prof. Moussa Youdim and Prof. John Finberg of the Faculty of Medicine, Technion – Israel Institute of Technology.[5]
Contents
Mechanism of Action
Human cells contain two forms of monoamine oxidase, MAO-A and MAO-B. Both are found in the brain, but MAO-B is far more prevalent and is responsible for the breakdown of dopamine after its release into the synapse. Parkinson's disease is characterized by the death of cells that use dopamine to transmit their signals, this results in a decrease in synaptic signal strength and concommitant symptomology. By inhibiting the breakdown of dopamine in the synapse, rasagiline permits the signaling neurons to reabsorb more of it for reuse later, somewhat compensating for the diminished quantities manufactured.
Selegiline was the first MAO inhibitor approved for use in Parkinson's disease in the United States. It is chemically similar to methamphetamine and its metabolic breakdown path eventually yields l-methamphetamine derivatives that have been associated with cardiac and psychiatric effects in some patients[citation needed]. The chief metabolite of rasagiline is 1(R)-aminoindan[6] which has no amphetamine characteristics. Some clinicians believe rasagiline will be better tolerated in sensitive patients for these reasons. Aminoindan inhibits both MAO-A and MAO-B in a reversible manner, although considerably weaker than rasagiline.[3]
Laboratory studies show that rasagiline has in vitro and in vivo neuroprotective effects but its neuroprotective effect in Parkinson's disease patients is unknown at present. These studies show that MAO-B metabolizes an opioid-related chemical called MPTP (not an opioid itself), into a neurotoxin called MPP+ that in turn creates free radicals. There is uncertainty because the mechanism of cell death in human PD may or may not involve the actions of free radicals, but there is suggestive evidence that the drug slows disease progression. The ADAGIO study found that early treatment with rasagiline at a dose of 1 mg per day provided benefits that were consistent with a possible disease-modifying effect, but early treatment with rasagiline at a dose of 2 mg per day did not[7].
Metabolism
Rasagiline is broken down via CYP1A2[8], part of the cytochrome P450 metabolic path in the liver. It is probably contraindicated in patients with hepatic insufficiency and its use should be monitored carefully in patients taking other drugs that alter the normal effectiveness of this metabolic path. Examples include but are not limited to fluvoxamine, cimetidine, ciprofloxacin and omeprazole.
Usage
Monotherapy in Early PD
A study called TVP-1012 (an early name for rasagiline) in Early Monotherapy for Parkinson's Disease Outpatients (TEMPO) enrolled 404 patients. A double-blind, randomized, delayed start study, it evaluated patients for a year using a placebo and doses of 1 mg and 2 mg per day. The initial six-month placebo controlled part of the study yielded data that led organizers to conclude both rasagiline doses were superior to placebo. The evaluation compared patients' Unified Parkinson's Disease Rating Scale (UPDRS) scores. The UPDRS is a standard method of measuring PD severity. Starting at six months the placebo treated group received the higher dosage of rasagiline (2 mg) until the conclusion of the study at twelve months and patients' UPDRS scores were compared again. Patients who had consistently received the higher dose had significantly better scores than patients who had received the placebo, and somewhat better scores than other groups. These data suggest but do not prove a neuroprotective effect. Some patients entered an open-label follow up study. About half of them did not require additional dopaminergic therapy two years later. Over a six and a half year period the mean deterioration in UPDRS scores for patients receiving some level of rasagiline therapy was 2-3 points. Other clinical studies of placebo treated patients with early PD reported a diminution of 8-12 points per year.
Adjunct Therapy in Advanced PD
An eighteen week double-blind placebo-controlled study called the Lasting Effect in Adjunct Therapy with Rasagiline Given Once Daily (LARGO) compared the drug to entacapone and a placebo in 687 patients experiencing motor fluctuations, a hallmark symptom of PD.[9] Rasagiline at a 1 mg dose significantly reduced daily off time (1.18 hours) compared to the placebo (0.4 hours) and increased on time without dyskinesia by 0.85 hours. This was approximately the same benefit granted by entacapone.
The Parkinson's Rasagiline: Efficacy and Safety in the Treatment of "OFF" (PRESTO) study monitored 472 patients treated with levodopa for motor fluctuations despite attempts to optimize dopaminergic therapy.[10] PRESTO did not have an active comparison drug; its patients randomly received a 0.5 mg dose, a 1 mg dose, or a placebo. Patients receiving both doses of rasagiline experienced significantly less off time (1.4 hours and 1.8 hours) than did those who received the placebo.
These studies suggest patients with advanced and fluctuating PD benefit in the short term from rasagiline therapy but do not comment on long term effects.
Other
Rasagiline is being investigated for the treatment of Restless Legs Syndrome[11].
Safety
Between the TEMPO, LARGO and PRESTO studies 530 patients were treated with the recommended dosage of 1 mg/day for a total of 212 patient-years. The number of patients who discontinued participation due to adverse symptoms was not significantly different between active drug and placebo.
Although rasagiline is an inhibitor of MAO-B, some concern still exists regarding possible drug interactions with medications that are normally considered contraindicated when taken with general MAO inhibitors since adequate studies to establish rasagiline's selectivity for MAO-B have not been conducted.[4] The concern revolves around a possible serotonin-syndrome effect, which was not known to occur during clinical trials despite patients being allowed to take certain antidepressant drugs that are normally contraindicated with general MAO inhibitors. Concern for a possible interaction between rasagiline and tyramine also exists, although no dietary restrictions were imposed during the TEMPO, PRESTO and LARGO studies and no hypertensive crises resulted due to the possible interaction of tyramine and rasagiline.[12]
See also
- Selegiline
- Ladostigil
References
- ^ Oldfield V, Keating GM, Perry CM (2007). "Rasagiline: a review of its use in the management of Parkinson's disease". Drugs 67 (12): 1725–47. PMID 17683172.
- ^ Gallagher DA, Schrag A (2008). "Impact of newer pharmacological treatments on quality of life in patients with Parkinson's disease". CNS Drugs 22 (7): 563–86. doi:10.2165/00023210-200822070-00003. PMID 18547126.
- ^ a b Binda C, Hubálek F, Li M et al. (2005). "Binding of Rasagiline-related Inhibitors to Human Monoamine Oxidases: A Kinetic and Crystallographic Analysis". Journal of medicinal chemistry 48 (26): 8148–54. doi:10.1021/jm0506266. PMC 2519603. PMID 16366596. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2519603.
- ^ a b "Prescribing Information". Teva Neurosciences. 2005-06. Archived from the original on 2007-01-19. http://web.archive.org/web/20070119131737/http://www.tevaneuro.com/upload/Prescribing_Information.pdf. Retrieved 2007-03-20.
- ^ Lakhan SE. From a Parkinson's disease expert: Rasagiline and the Future of Therapy. Molecular Neurodegeneration 2007;2(13).
- ^ Chen JJ, Swope DM (August 2005). "Clinical pharmacology of rasagiline: a novel, second-generation propargylamine for the treatment of Parkinson disease". J Clin Pharmacol 45 (8): 878–94. doi:10.1177/0091270005277935. PMID 16027398. http://jcp.sagepub.com/cgi/pmidlookup?view=long&pmid=16027398.
- ^ C. Warren Olanow, Olivier Rascol et al. (2009). "A Double-Blind, Delayed-Start Trial of Rasagiline in Parkinson's Disease". New England Journal of Medicine 361 (13): 1268–78. doi:10.1056/NEJMoa0809335. PMID 19776408.
- ^ Lecht S, Haroutiunian S, Hoffman A, Lazarovici P (June 2007). "Rasagiline – a novel MAO B inhibitor in Parkinson's disease therapy". Ther Clin Risk Manag 3 (3): 467–74. PMC 2386362. PMID 18488080. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2386362.
- ^ Rascol O, Brooks DJ, Melamed E et al. (2005). "Rasagiline as an adjunct to levodopa in patients with Parkinson's disease and motor fluctuations (LARGO, Lasting effect in Adjunct therapy with Rasagiline Given Once daily, study): a randomised, double-blind, parallel-group trial". Lancet 365 (9463): 947–54. doi:10.1016/S0140-6736(05)71083-7. PMID 15766996. http://linkinghub.elsevier.com/retrieve/pii/S0140-6736(05)71083-7.
- ^ Parkinson Study, Group (February 2005). "A randomized placebo-controlled trial of rasagiline in levodopa-treated patients with Parkinson disease and motor fluctuations: the PRESTO study". Arch. Neurol. 62 (2): 241–8. doi:10.1001/archneur.62.2.241. PMID 15710852. http://archneur.ama-assn.org/cgi/pmidlookup?view=long&pmid=15710852.
- ^ http://www.healthcareilluminated.com/articles/20203-parkinson-s-drug-may-also-treat-restless-leg-syndrome
- ^ White WB, Salzman P, Schwid SR (August 2008). "Transtelephonic Home Blood Pressure to Assess the Monoamine Oxidase-B Inhibitor Rasagiline in Parkinson Disease". Hypertension 52 (3): 587–93. doi:10.1161/HYPERTENSIONAHA.108.115873. PMID 18678789. http://hyper.ahajournals.org/cgi/pmidlookup?view=reprint&pmid=18678789.
Antiparkinson agents (N04) Dopaminergics DA receptor agonistsAplindore • Apomorphine • Bromocriptine • Cabergoline • Ciladopa • Dihydroergocryptine • Lisuride • Pardoprunox • Pergolide • Piribedil • Pramipexole • Ropinirole • RotigotineAnticholinergics Benzatropine • Biperiden# • Bornaprine • Chlorphenoxamine • Cyrimine • Dexetimide • Dimenhydrinate • Diphenhydramine • Etanautine • Etybenzatropine • Mazaticol • Metixene • Orphenadrine • Phenglutarimide • Piroheptine • Procyclidine • Profenamine • Trihexyphenidyl • TropatepineOthers Antidepressants (N06A) Specific reuptake inhibitors (RIs), enhancers (REs), and releasing agents (RAs) Alaproclate • Citalopram • Escitalopram • Femoxetine • Fluoxetine# • Fluvoxamine • Indalpine • Ifoxetine • Litoxetine • Lubazodone • Panuramine • Paroxetine • Pirandamine • Seproxetine • Sertraline# • Vilazodone • Zimelidine‡Bicifadine • Clovoxamine • Desvenlafaxine • Duloxetine • Levomilnacipran • Eclanamine • Milnacipran • Sibutramine • VenlafaxineSerotonin–norepinephrine–dopamine reuptake inhibitors (SNDRIs)Brasofensine • BTS-74,398 • Cocaine • Diclofensine • DOV-21,947 • DOV-102,677 • DOV-216,303 • EXP-561 • Fezolamine • JNJ-7925476 • NS-2359 • PRC200-SS • Pridefine • SEP-225,289 • SEP-227,162 • TesofensineAmedalin • Atomoxetine/Tomoxetine • Binedaline • Ciclazindol • Daledalin • Esreboxetine • Lortalamine • Mazindol • Nisoxetine • Reboxetine • Talopram • Talsupram • Tandamine • ViloxazineDopamine reuptake inhibitors (DRIs)Amineptine • Bupropion/Amfebutamone# • Cilobamine • Manifaxine • Methylphenidate • Nomifensine • Radafaxine • TametralineNorepinephrine-dopamine releasing agents (NDRAs)Serotonin-norepinephrine-dopamine releasing agents (SNDRAs)4-Methyl-αMT • αET/Etryptamine • αMT/MetryptamineOthersIndeloxazine • Teniloxazine • Tramadol • ViqualineReceptor antagonists and/or reuptake inhibitors Serotonin antagonists and reuptake inhibitors (SARIs)Serotonin modulators and stimulators (SMSs)VortioxetineTricyclic and tetracyclic antidepressants (TCAs/TeCAs) TricyclicsAmezepine • Amineptine • Amitriptyline# • Amitriptylinoxide • Azepindole • Butriptyline • Cianopramine • Clomipramine • Cotriptyline • Cyanodothiepin • Demexiptiline • Depramine/Balipramine • Desipramine • Dibenzepin • Dimetacrine • Dosulepin/Dothiepin • Doxepin • Enprazepine • Fluotracen • Hepzidine • Homopipramol • Imipramine • Imipraminoxide • Intriptyline • Iprindole • Ketipramine • Litracen • Lofepramine • Losindole • Mariptiline • Melitracen • Metapramine • Mezepine • Naranol • Nitroxazepine • Nortriptyline • Noxiptiline • Octriptyline • Opipramol • Pipofezine • Propizepine • Protriptyline • Quinupramine • Tampramine • Tianeptine • Tienopramine • Trimipramine;7-OH-Amoxapine • Amoxapine • Aptazapine • Azipramine • Ciclazindol • Ciclopramine • Esmirtazapine • Loxapine • Maprotiline • Mazindol • Mianserin • Mirtazapine • Oxaprotiline • Setiptiline/TeciptilineMonoamine oxidase inhibitors (MAOIs) NonselectiveIrreversible: Benmoxin • Echinopsidine • Iproclozide • Iproniazid • Isocarboxazid • Mebanazine • Metfendrazine • Nialamide • Octamoxin • Phenelzine • Pheniprazine • Phenoxypropazine • Pivalylbenzhydrazine • Safrazine • Tranylcypromine; Reversible: Caroxazone • Paraxazone;MAOA-SelectiveIrreversible: Clorgiline; Reversible: Amiflamine • Bazinaprine • Befloxatone • Befol • Brofaromine • Cimoxatone • Esuperone • Harmala Alkaloids (Harmine, Harmaline, Tetrahydroharmine, Harman, Norharman, etc) • Methylene Blue • Metralindole • Minaprine • Moclobemide • Pirlindole • Sercloremine • Tetrindole • Toloxatone • Tyrima;MAOB-SelectiveIrreversible: Ladostigil • Mofegiline • Pargyline • Rasagiline • Selegiline; Reversible: Lazabemide • MilacemideAzapirones and other 5-HT1A receptor agonists Alnespirone • Aripiprazole • Befiradol • Buspirone • Eptapirone • Flesinoxan • Flibanserin • Gepirone • Ipsapirone • Oxaflozane • Tandospirone • Vilazodone • ZalospironeAntioxidants Acetyl-L-Carnitine (ALCAR) • Alpha-Lipoic Acid (ALA) • Ascorbic Acid (Vitamin C) • Carotenoids (Vitamin A) • Curcumin • Edaravone • Polyphenols • Glutathione • Hydroxytyrosol • L-Carnitine • Ladostigil • Melatonin • N-Acetylcysteine (NAC) • N-Acetylserotonin (NAS) • Oleocanthal • Oleuropein • Rasagiline • Resveratrol • Selegiline • Selenium • Tocopherols (Vitamin E) • Tocotrienols (Vitamin E) • Tyrosol • Ubiquinone (Coenzyme Q) • Uric AcidDopaminergics Reuptake inhibitors PlasmalemmalDAT inhibitorsPiperazines: DBL-583 • GBR-12,935 • Nefazodone • Vanoxerine; Piperidines: BTCP • Desoxypipradrol • Dextromethylphenidate • Difemetorex • Ethylphenidate • Methylnaphthidate • Methylphenidate • Phencyclidine • Pipradrol; Pyrrolidines: Diphenylprolinol • Methylenedioxypyrovalerone (MDPV) • Naphyrone • Prolintane • Pyrovalerone; Tropanes: β-CPPIT • Altropane • Brasofensine • CFT • Cocaine • Dichloropane • Difluoropine • FE-β-CPPIT • FP-β-CPPIT • Ioflupane (123I) • Iometopane • RTI-112 • RTI-113 • RTI-121 • RTI-126 • RTI-150 • RTI-177 • RTI-229 • RTI-336 • Tenocyclidine • Tesofensine • Troparil • Tropoxane • WF-11 • WF-23 • WF-31 • WF-33; Others: Adrafinil • Armodafinil • Amfonelic acid • Amineptine • Benzatropine (Benztropine) • Bromantane • BTQ • BTS-74,398 • Bupropion (Amfebutamone) • Ciclazindol • Diclofensine • Dimethocaine • Diphenylpyraline • Dizocilpine • DOV-102,677 • DOV-21,947 • DOV-216,303 • Etybenzatropine (Ethylbenztropine) • EXP-561 • Fencamine • Fencamfamine • Fezolamine • GYKI-52,895 • Indatraline • Ketamine • Lefetamine • Levophacetoperane • LR-5182 • Manifaxine • Mazindol • Medifoxamine • Mesocarb • Modafinil • Nefopam • Nomifensine • NS-2359 • O-2172 • Pridefrine • Propylamphetamine • Radafaxine • SEP-225,289 • SEP-227,162 • Sertraline • Sibutramine • Tametraline • Tedatioxetine • TripelennamineVMAT inhibitorsReleasing agents Morpholines: Fenbutrazate • Morazone • Phendimetrazine • Phenmetrazine; Oxazolines: 4-Methylaminorex (4-MAR, 4-MAX) • Aminorex • Clominorex • Cyclazodone • Fenozolone • Fluminorex • Pemoline • Thozalinone; Phenethylamines (also amphetamines, cathinones, phentermines, etc): 2-Hydroxyphenethylamine (2-OH-PEA) • 4-CAB • 4-Methylamphetamine (4-MA) • 4-Methylmethamphetamine (4-MMA) • Alfetamine • Amfecloral • Amfepentorex • Amfepramone • Amphetamine (Dextroamphetamine, Levoamphetamine) • Amphetaminil • β-Methylphenethylamine (β-Me-PEA) • Benzodioxolylbutanamine (BDB) • Benzodioxolylhydroxybutanamine (BOH) • Benzphetamine • Buphedrone • Butylone • Cathine • Cathinone • Clobenzorex • Clortermine • D-Deprenyl • Dimethoxyamphetamine (DMA) • Dimethoxymethamphetamine (DMMA) • Dimethylamphetamine • Dimethylcathinone (Dimethylpropion, metamfepramone) • Ethcathinone (Ethylpropion) • Ethylamphetamine • Ethylbenzodioxolylbutanamine (EBDB) • Ethylone • Famprofazone • Fenethylline • Fenproporex • Flephedrone • Fludorex • Furfenorex • Hordenine • Lophophine (Homomyristicylamine) • Mefenorex • Mephedrone • Methamphetamine (Desoxyephedrine, Methedrine; Dextromethamphetamine, Levomethamphetamine) • Methcathinone (Methylpropion) • Methedrone • Methoxymethylenedioxyamphetamine (MMDA) • Methoxymethylenedioxymethamphetamine (MMDMA) • Methylbenzodioxolylbutanamine (MBDB) • Methylenedioxyamphetamine (MDA, tenamfetamine) • Methylenedioxyethylamphetamine (MDEA) • Methylenedioxyhydroxyamphetamine (MDOH) • Methylenedioxymethamphetamine (MDMA) • Methylenedioxymethylphenethylamine (MDMPEA, homarylamine) • Methylenedioxyphenethylamine (MDPEA, homopiperonylamine) • Methylone • Ortetamine • Parabromoamphetamine (PBA) • Parachloroamphetamine (PCA) • Parafluoroamphetamine (PFA) • Parafluoromethamphetamine (PFMA) • Parahydroxyamphetamine (PHA) • Paraiodoamphetamine (PIA) • Paredrine (Norpholedrine, Oxamphetamine) • Phenethylamine (PEA) • Pholedrine • Phenpromethamine • Prenylamine • Propylamphetamine • Tiflorex (Flutiorex) • Tyramine (TRA) • Xylopropamine • Zylofuramine; Piperazines: 2,5-Dimethoxy-4-bromobenzylpiperazine (2C-B-BZP) • Benzylpiperazine (BZP) • Methoxyphenylpiperazine (MeOPP, paraperazine) • Methylbenzylpiperazine (MBZP) • Methylenedioxybenzylpiperazine (MDBZP, piperonylpiperazine); Others: 2-Amino-1,2-dihydronaphthalene (2-ADN) • 2-Aminoindane (2-AI) • 2-Aminotetralin (2-AT) • 4-Benzylpiperidine (4-BP) • 5-IAI • Clofenciclan • Cyclopentamine • Cypenamine • Cyprodenate • Feprosidnine • Gilutensin • Heptaminol • Hexacyclonate • Indanylaminopropane (IAP) • Indanorex • Isometheptene • Methylhexanamine • Naphthylaminopropane (NAP) • Octodrine • Phthalimidopropiophenone • Propylhexedrine (Levopropylhexedrine) • Tuaminoheptane (Tuamine)Enzyme inhibitors PAH inhibitors3,4-DihydroxystyreneTH inhibitorsNonselective: Benmoxin • Caroxazone • Echinopsidine • Furazolidone • Hydralazine • Indantadol • Iproclozide • Iproniazid • Isocarboxazid • Isoniazid • Linezolid • Mebanazine • Metfendrazine • Nialamide • Octamoxin • Paraxazone • Phenelzine • Pheniprazine • Phenoxypropazine • Pivalylbenzhydrazine • Procarbazine • Safrazine • Tranylcypromine; MAO-A selective: Amiflamine • Bazinaprine • Befloxatone • Befol • Brofaromine • Cimoxatone • Clorgiline • Esuprone • Harmala alkaloids • Methylene Blue • Metralindole • Minaprine • Moclobemide • Pirlindole • Sercloremine • Tetrindole • Toloxatone • Tyrima; MAO-B selective: D-Deprenyl • L-Deprenyl (Selegiline) • Ladostigil • Lazabemide • Milacemide • Pargyline • Rasagiline • SafinamideDBH inhibitorsOthers L-Phenylalanine → L-Tyrosine → L-DOPA (Levodopa)Ferrous iron (Fe2+) • Tetrahydrobiopterin • Vitamin B3 (Niacin, Nicotinamide → NADPH) • Vitamin B6 (Pyridoxine, Pyridoxamine, Pyridoxal → Pyridoxal phosphate) • Vitamin B9 (Folic acid → Tetrahydrofolic acid) • Vitamin C (Ascorbic acid) • Zinc (Zn2+)OthersActivity enhancers: Benzofuranylpropylaminopentane (BPAP) • Phenylpropylaminopentane (PPAP); Toxins: Oxidopamine (6-Hydroxydopamine)List of dopaminergic drugsCategories:- Nootropics
- Monoamine oxidase inhibitors
- Antiparkinsonian agents
- Indanes
- Alkynes
- InChI=1S/C12H13N/c1-2-9-13-12-8-7-10-5-3-4-6-11(10)12/h1,3-6,12-13H,7-9H2/t12-/m1/s1


Wikimedia Foundation. 2010.