- Restless legs syndrome
Infobox_Disease
Name = Restless legs syndrome
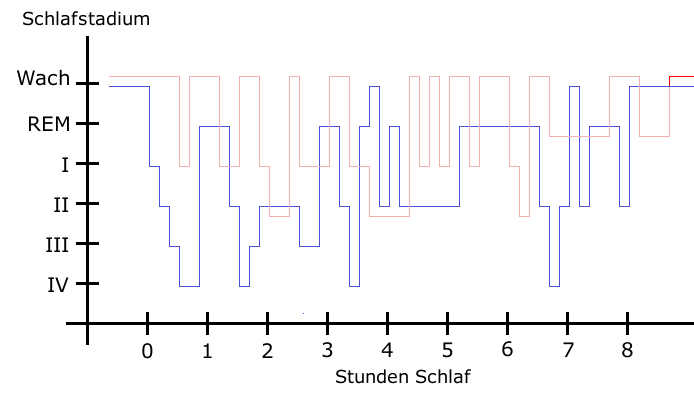
Caption = Sleep pattern of a Restless Legs Syndrome patient (red) vs. a healthy sleep pattern (blue).
DiseasesDB = 29476
ICD10 = ICD10|G|25|8|g|20
ICD9 = ICD9|333.94
ICDO =
OMIM = 102300
OMIM_mult = OMIM2|608831
MedlinePlus =
eMedicineSubj = neuro
eMedicineTopic = 509
MeshID = D012148Restless legs syndrome (RLS, Wittmaack-Ekbom's syndrome, or sometimes, but inaccurately, referred to as
Nocturnal myoclonus ) is a condition that is characterized by an irresistible urge to move one's body to stop uncomfortable or odd sensations. It most commonly affects the legs, but can also be in the arms and torso. Moving the affected body part modulates the sensations, providing temporary relief. RLS causes a sensation in the legs or arms that can most closely be compared to a burning, itching, or tickling sensation in the muscles.Fact|date=April 2008 Some controversy surrounds the marketing of drug treatments for RLS.igns and symptoms
The sensations—and the need to move—may return immediately after ceasing movement, or at a later time. RLS may start at any age, including early childhood, and is a progressive disease for a certain portion of those afflicted, although the symptoms have disappeared permanently in some sufferers.
*"An urge to move, usually due to uncomfortable sensations that occur primarily in the legs, but occasionally in the arms or elsewhere."
:The sensations are unusual and unlike other common sensations, and those with RLS have a hard time describing them. People use words such as: uncomfortable, "antsy", electrical, creeping, painful, itching, pins and needles, pulling, creepy-crawly, ants inside the legs, and many others. The sensation and the urge can occur in any body part; the most cited location is legs, followed by arms. Some people have little or no sensation, yet still have a strong urge to move. While an RLS sufferer may be unable to qualify the sensations to a non-sufferer, someone else with RLS understands the indescribable nature of the unpleasant sensations.
*"Motor restlessness, expressed as activity, that relieves the urge to move."
:Movement will usually bring immediate relief, however, often only temporary and partial. Walking is most common; however, doing stretches, yoga, biking, or other physical activity may relieve the symptoms. Constant and fast up-and-down movement of the leg, coined "sewing machine legs" by at least one RLS sufferer, is often done to keep the sensations at bay without having to walk. Sometimes a specific type of movement will help a person more than another.
*"Worsening of symptoms by relaxation."
:Any type of inactivity involving sitting or lying—reading a book, a plane ride, watching TV or a movie, taking a nap—can trigger the sensations and urge to move. This depends on several factors: the severity of the person’s RLS, the degree of restfulness, the duration of the inactivity, etc.
*"Variability over the course of the day-night cycle, with symptoms worse in the evening and early in the night."
:While some only experience RLS at bedtime and others experience it throughout the day and night, most sufferers experience the worst symptoms in the evening and the least in the morning.
NIH criteria
In 2003, a
National Institutes of Health (NIH) consensus panel modified their criteria to include the following:
#an urge to move the limbs with or without sensations
#improvement with activity
#worsening at rest
#worsening in the evening or night. [cite journal | author = Allen R, Picchietti D, Hening W, Trenkwalder C, Walters A, Montplaisi J | title = Restless legs syndrome: diagnostic criteria, special considerations, and epidemiology. A report from the restless legs syndrome diagnosis and epidemiology workshop at the National Institutes of Health | journal = Sleep Med | volume = 4 | issue = 2 | pages = 101–19 | year = 2003 | pmid = 14592341 | doi = 10.1016/S1389-9457(03)00010-8]RLS is either primary or secondary.
*Primary RLS is considered
idiopathic , or with no known cause. Primary RLS usually begins before approximately 40 to 45 years of age, and can even occur as early as the first year of life. In primary RLS, the onset is often slow. The RLS may disappear for months, or even years. It is often progressive and gets worse as the person ages. RLS in children is often misdiagnosed asgrowing pains .*Secondary RLS often has a sudden onset and may be daily from the very beginning. It often occurs after the age of 40, however it can occur earlier. It is most associated with specific medical conditions or the use of certain drugs (see below).
Causes
Disease mechanism
Most research on the disease mechanism of restless legs syndrome has focused on the
dopamine and iron system.cite journal |author=Allen R |title=Dopamine and iron in the pathophysiology of restless legs syndrome (RLS) |journal=Sleep Med. |volume=5 |issue=4 |pages=385–91 |year=2004 |month=July |pmid=15222997 |doi=10.1016/j.sleep.2004.01.012 |url=http://linkinghub.elsevier.com/retrieve/pii/S1389945704000243] cite journal |author=Clemens S, Rye D, Hochman S |title=Restless legs syndrome: revisiting the Dopamine hypothesis from the spinal cord perspective |journal=Neurology |volume=67 |issue=1 |pages=125–130 |url=http://www.neurology.org/cgi/content/abstract/67/1/125 |doi=10.1212/01.wnl.0000223316.53428.c9 |year=2006 |pmid=16832090] These hypotheses are based on the observation thatlevodopa and iron can be used to treat RLS, but also on findings from functional brain imaging (such aspositron emission tomography andfunctional magnetic resonance imaging ),autopsy series andanimal experiments .cite journal |author=Earley CJ, B Barker P, Horská A, Allen RP |title=MRI-determined regional brain iron concentrations in early- and late-onset restless legs syndrome |journal=Sleep Med. |volume=7 |issue=5 |pages=458–61 |year=2006 |month=August |pmid=16740411 |doi=10.1016/j.sleep.2005.11.009 |url=http://linkinghub.elsevier.com/retrieve/pii/S1389-9457(05)00303-5] Differences in dopamine- and iron-related markers have also been demonstrated in thecerebrospinal fluid of individuals with RLS.cite journal |author=Allen RP, Connor JR, Hyland K, Earley CJ |title=Abnormally increased CSF 3-Ortho-methyldopa (3-OMD) in untreated restless legs syndrome (RLS) patients indicates more severe disease and possibly abnormally increased dopamine synthesis |journal=Sleep Med. |volume= |issue= |pages= |year=2008 |month=January |pmid=18226951 |doi=10.1016/j.sleep.2007.11.012 |url=http://linkinghub.elsevier.com/retrieve/pii/S1389-9457(07)00425-X] A connection between these two systems is demonstrated by the finding of low iron levels in thesubstantia nigra of RLS patients, although other areas may also be involved.cite journal |author=Godau J, Klose U, Di Santo A, Schweitzer K, Berg D |title=Multiregional brain iron deficiency in restless legs syndrome |journal=Mov. Disord. |volume= 23|issue= |pages= 1184|year=2008 |month=April |pmid=18442125 |doi=10.1002/mds.22070]Underlying disorders
The most commonly associated medical condition is iron deficiency (specifically blood
ferritin below 50µg/Lcite journal |author= |title=Restless legs syndrome: detection and management in primary care. National Heart, Lung, and Blood Institute Working Group on Restless Legs Syndrome |journal=Am Fam Physician |volume=62 |issue=1 |pages=108–14 |year=2000 |month=July |pmid=10905782 |doi= |url=] ), which accounts for just over 20% of all cases of RLS. Other conditions associated with RLS includepregnancy ,varicose vein or venous reflux,folate deficiency ,sleep apnea ,uremia , diabetes,thyroid disease ,peripheral neuropathy ,Parkinson's disease and certainauto-immune disorder s such asSjögren's syndrome ,celiac disease , andrheumatoid arthritis . RLS can also worsen inpregnancy .cite journal |author=McParland P, Pearce JM |title=Restless leg syndrome in pregnancy |journal=BMJ |volume=297 |issue=6662 |pages=1543 |year=1988 |pmid=3147073 |doi=] In a recent study, RLS was detected in 36% of patients attending aphlebology (vein disease) clinic, compared to 18% in a control group.>cite journal |author=McDonagh B, King T, Guptan RC |title=Restless legs syndrome in patients with chronic venous disorders: an untold story |journal=Phlebology |volume=22 |issue=4 |pages=156–63 |year=2007 |pmid=18265529 |doi= |url=http://phleb.rsmjournals.com/cgi/pmidlookup?view=long&pmid=18265529]Certain medications may worsen RLS in those who already have it, or cause it secondarily. These include:
anti-nausea drugs , certainantihistamines (often in over-the-counter cold medications), drugs used to treat depression (both oldertricyclics and newerSSRI s),antipsychotic drugs, and certain medications used to controlseizures . Treatment of underlying conditions, or cessation of use of the offending drug, often eliminates the RLS.Both primary and secondary RLS can be worsened by surgery of any kind, however
back surgery or injury can be associated with causing RLS.cite journal |author=Crotti FM, Carai A, Carai M, Sgaramella E, Sias W |title=Entrapment of crural branches of the common peroneal nerve |journal=Acta Neurochir. Suppl. |volume=92 |issue= |pages=69–70 |year=2005 |pmid=15830971 |doi=]Some experts believe RLS and
periodic limb movement disorder are strongly associated with ADHD in some children.Dopamine appears to factor into both conditions. In addition, many types of medication for the treatment of both conditions affect dopamine levels in the brain. [ [http://www.umm.edu/patiented/articles/other_disorders_associated_with_attention-deficit_disorder_000030_5.htm Attention deficit hyperactivity disorder—Other Disorders Associated with ADHD] , University of Maryland Medical Center.]The cause vs. effect of certain conditions and behaviors that are observed in some patients (ex. carrying excess weight, lack of exercise, suffering from depression or other mental illnesses) does not appear to be well established. The loss of sleep due to RLS could be the cause of the conditions, or the medication used to treat a condition could be the cause of an individual's RLS. [cite web|url=http://www.medscape.com/viewarticle/545408_2|title=Exercise and Restless Legs Syndrome|accessdate=2008-05-28] [cite web|url=http://www.sciencedaily.com/releases/2005/10/051031132243.htm|title=Restless Legs Syndrome Linked To Psychiatric Conditions|accessdate=2008-05-28]
Genetics
More than 60% of cases of RLS are familial [cite journal | author = Lavigne GJ, Montplaisir JY | title = Restless legs syndrome and sleep bruxism: prevalence and association among Canadians | journal = Sleep | volume = 17 | issue = 8 | pages = 739–43 | year = 1994 | pmid = 7701186] and are inherited in an
autosomal dominant fashion withvariable penetrance .No one knows the exact cause of RLS at present. Research and brain autopsies have implicated both dopaminergic system and iron insufficiency in the
substantia nigra (study published in Neurology, 2003). [cite journal | author = Connor J, Boyer P, Menzies S, Dellinger B, Allen R, Ondo W, Earley C | title = Neuropathological examination suggests impaired brain iron acquisition in restless legs syndrome | journal = Neurology | volume = 61 | issue = 3 | pages = 304–9 | year = 2003 | pmid = 12913188] Iron is an essential cofactor for the formation of L-dopa, the precursor of dopamine.Five genetic loci found by
linkage are currently known. Other than the first, the remainder of the linkage loci were discovered using an autosomal dominant model of inheritance.*The first genetic locus was discovered in one large
French Canadian family and maps onchromosome 12q. [cite journal | author = Desautels A, Turecki G, Montplaisir J, Sequeira A, Verner A, Rouleau G | title = Identification of a major susceptibility locus for restless legs syndrome on chromosome 12q | journal = Am J Hum Genet | volume = 69 | issue = 6 | pages = 1266–70 | year = 2001 | pmid = 11704926 | doi = 10.1086/324649] [cite journal | author = Desautels A, Turecki G, Montplaisir J, Xiong L, Walters AS, Ehrenberg BL, Brisebois K, Desautels AK, Gingras Y, Johnson WG, Lugaresi E, Coccagna G, Picchietti DL, Lazzarini A, Rouleau GA | title = Restless legs syndrome: confirmation of linkage to chromosome 12q, genetic heterogeneity, and evidence of complexity | journal = Arch Neurol | volume = 62 | issue = 4 | pages = 591–6 | year = 2005 | pmid = 15824258 | doi = 10.1001/archneur.62.4.591] This locus was discovered, however, using anautosomal recessive inheritance model. Evidence for this locus was also found using atransmission disequilibrium test (TDT) in 12Bavarian families. [cite journal | author = Winkelmann J, Lichtner P, Pütz B, Trenkwalder C, Hauk S, Meitinger T, Strom T, Muller-Myhsok B | title = Evidence for further genetic locus heterogeneity and confirmation of RLS-1 in restless legs syndrome | journal = Mov Disord | volume = 21 | issue = 1 | pages = 28–33 | year = 2006 | pmid = 16124010 | doi = 10.1002/mds.20627]*The second RLS locus maps to chromosome 14q and was discovered in one Italian family. [cite journal | author = Bonati MT, Ferini-Strambi L, Aridon P, Oldani A, Zucconi M, Casari G | title = Autosomal dominant restless legs syndrome maps on chromosome 14q | journal = Brain | volume = 126 | issue = Pt 6 | pages = 1485–92 | year = 2003 | pmid = 12764067 | doi = 10.1093/brain/awg137] Evidence for this locus was found in one French Canadian family. [cite journal | author = Levchenko A, Montplaisir J, Dubé M, Riviere J, St-Onge J, Turecki G, Xiong L, Thibodeau P, Desautels A, Verlaan D, Rouleau G | title = The 14q restless legs syndrome locus in the French Canadian population | journal = Ann Neurol | volume = 55 | issue = 6 | pages = 887–91 | year = 2004 | pmid = 15174026 | doi = 10.1002/ana.20140] Also, an
association study in a large sample 159trios of European descent showed some evidence for this locus. [cite journal | author = Kemlink D, Polo O, Montagna P, Provini F, Stiasny-Kolster K, Oertel W, de Weerd A, Nevsimalova S, Sonka K, Högl B, Frauscher B, Poewe W, Trenkwalder C, Pramstaller PP, Ferini-Strambi L, Zucconi M, Konofal E, Arnulf I, Hadjigeorgiou GM, Happe S, Klein C, Hiller A, Lichtner P, Meitinger T, Müller-Myshok B, Winkelmann J | title = Family-based association study of the restless legs syndrome loci 2 and 3 in a European population | journal = Ann Neurol | volume = 22 | issue = 2 | year = 2007 | pmid = 17133505 | pages = 207–12 | doi = 10.1002/mds.21254]*The third locus maps to chromosome 9p and was discovered in two unrelated American families. [cite journal | author = Chen S, Ondo WG, Rao S, Li L, Chen Q, Wang Q | title = Genomewide linkage scan identifies a novel susceptibility locus for restless legs syndrome on chromosome 9p | journal = Am J Hum Genet | volume = 74 | issue = 5 | year = 2004 | pmid = 15077200 | pages = 876 | doi = 10.1086/420772] Evidence for this locus was also found by the TDT in a large Bavarian family, [cite journal | author = Liebetanz KM, Winkelmann J, Trenkwalder C, Pütz B, Dichgans M, Gasser T, Müller-Myhsok B | title = RLS3: fine-mapping of an autosomal dominant locus in a family with intrafamilial heterogeneity | journal = Neurology | volume = 67 | issue = 2 | year = 2006 | pmid = 16864828 | pages = 320 | doi = 10.1212/01.wnl.0000224886.65213.b5] as well as in a German family, in which significant linkage to this locus was found. [cite journal | author = Lohmann-Hedrich K, Neumann A, Kleensang A, Lohnau T, Muhle H, Djarmati A, König IR, Pramstaller PP, Schwinger E, Kramer PL, Ziegler A, Stephani U, Klein C | title = Evidence for linkage of restless legs syndrome to chromosome 9p | journal = Neurology | volume = 0 | issue = 0 | year = 2007 | pmid = 18032746 | pages = 0]
*The next locus maps to chromosome 20p and was discovered in a large French Canadian family with RLS. [cite journal | author = Levchenko A, Provost S, Montplaisir JY, Xiong L, St-Onge J, Thibodeau P, Rivière JB, Desautels A, Turecki G, Dubé MP, Rouleau GA | title = A novel autosomal dominant restless legs syndrome locus maps to chromosome 20p13 | journal = Neurology | volume =67 | issue = 5 | year = 2006 | pmid = 16966564 | pages = 900 | doi = 10.1212/01.wnl.0000233991.20410.b6]
*The fifth locus maps to chromosome 2p and was found in three related families from population isolate in Bolzano-Bozen. [cite journal | author = Pichler I, Marroni F, Volpato CB, Gusella JF, Klein C, Casari G, De Grandi A, Pramstaller PP | title = Linkage analysis identifies a novel locus for restless legs syndrome on chromosome 2q in a South Tyrolean population isolate | journal = Neurology | volume =79 | issue = 4 | year = 2006 | pmid = 16960808 | pages = 716–23]
Three genes,
MEIS1 ,BTBD9 andMAP2K5 , were found to be associated to RLS. [cite journal | author = Winkelmann J, Schormair B, Lichtner P, Ripke S, Xiong L, Jalilzadeh S, Fulda S, Pütz B, Eckstein G, Hauk S, Trenkwalder C, Zimprich A, Stiasny-Kolster K, Oertel W, Bachmann CG, Paulus W, Peglau I, Eisensehr I, Montplaisir J, Turecki G, Rouleau G, Gieger C, Illig T, Wichmann HE, Holsboer F, Müller-Myhsok B, Meitinger T | title = Genome-wide association study of restless legs syndrome identifies common variants in three genomic regions | journal = Nat Genet | volume =39 | issue = 8 | year = 2006 | pmid = 17637780 | pages = 1000–6 | doi = 10.1038/ng2099] Their role in RLSpathogenesis is still unclear.There is also some evidence that
periodic limb movements in sleep (PLMS) are associated with Gene|BTBD9 on chromosome 6p21.2.cite journal |author=Stefansson H, Rye DB, Hicks A, "et al" |title=A genetic risk factor for periodic limb movements in sleep |journal=N. Engl. J. Med. |volume=357 |issue=7 |pages=639–47 |year=2007 |pmid=17634447 |doi=10.1056/NEJMoa072743 |url=http://content.nejm.org/cgi/pmidlookup?view=short&pmid=17634447&promo=ONFLNS19]Diagnosis
The diagnosis of RLS relies essentially on a good
medical history andphysical examination . Sleep registration in a laboratory (polysomnography ) is not necessary for the diagnosis.Peripheral neuropathy ,radiculopathy andleg cramps should be considered in thedifferential diagnosis ; in these conditions, pain is often more pronounced than the urge to move.Akathisia , a side effect of severalantipsychotics orantidepressants , is a more constant form of leg restlessness without discomfort. DuplexUltrasound evaluation of the vascular system is essential in all cases to rule out venous disorders which is common etiology of RLS. A raresyndrome of painful legs and moving toes has been described, with no known cause.cite journal |author=Aizawa H |title=Gabapentin for painful legs and moving toes syndrome |journal=Intern. Med. |volume=46 |issue=23 |pages=1937 |year=2007 |pmid=18057770 |doi= |url=http://joi.jlc.jst.go.jp/JST.JSTAGE/internalmedicine/46.0416?from=PubMed]Prevention
Restless legs can only be prevented by preventing the underlying causes. No other ways of prevention have been studied.Fact|date=June 2008
Treatment
An algorithm for treating primary RLS (i.e., RLS that is not the result of another medical condition) was created by leading researchers at the
Mayo Clinic and is endorsed by the Restless Legs Syndrome Foundation. This document provides guidance to both the treating physician and the patient, and includes both nonpharmacological and pharmacological treatments. [http://www.mayoclinicproceedings.com/inside.asp?AID=1698&UID Mayo Clinic Algorithm] also available [http://www.mayoclinicproceedings.com/pdf/7907/7907crc.pdf as .pdf] ] Treatment of primary RLS should not be considered until possible precipitating medical conditions are ruled out, especially venous disorders. Drug therapy in RLS is not curative and is known to have significant side effects; expensive (about $100-150 per month for life), and thus it needs to be considered with caution.Secondary RLS has the potential for cure if the precipitating medical conditions, anaemia, venous disorder, etc., are managed effectively. In many instances the alleged secondary conditions might be the only conditions causing the RLS; these include
iron deficiency ,varicose veins , andthyroid problems. Karl Ekbom in his original thesis on RLS in 1945 had suspected of venous disease in about 12.5% of the cases he studied. But due to the unavailability of Duplex ultrasound imaging technology (the diagnostic tool that detects the abnormal blood flow in the veins, "Venous Reflux", the pathological basis for varicose veins) at that time, Ekbom may have underestimated the role of venous disease. In uncontrolled prospective series, improvement of RLS was achieved in a high percentage of patients who had presented with a combination of RLS and venous disease and had sclerotherapy or other treatment for the correction of venous insufficiency.cite journal |author=Hayes CA, Kingsley JR, Hamby KR, Carlow J |title=The effect of endovenous laser ablation on restless legs syndrome |journal=Phlebology / Venous Forum of the Royal Society of Medicine |volume=23 |issue=3 |pages=112–7 |year=2008 |pmid=18467618 |doi=10.1258/phleb.2007.007051 |url=http://phleb.rsmjournals.com/cgi/pmidlookup?view=long&pmid=18467618] cite journal |author=Kanter AH |title=The effect of sclerotherapy on restless legs syndrome |journal=Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.] |volume=21 |issue=4 |pages=328–32 |year=1995 |month=April |pmid=7728485 |doi= |url=]Iron supplements
According to some guidelines Fact|date=December 2007, all people with RLS should have their
ferritin levels tested; ferritin levels should be at least 50 g for those with RLS. Oral iron supplements, taken under a doctor's care, can increase ferritin levels. For some people, increasing ferritin will eliminate or reduce RLS symptoms. A ferritin level of 50 g is not sufficient for some sufferers and increasing the level to 80 g may greatly reduce symptoms. However, at least 40% of people will not notice any improvement. Treatment with IV iron is being tested at the USMayo Clinic andJohns Hopkins Hospital . It is dangerous to take iron supplements without first having ferritin levels tested, as many people with RLS do not have low ferritin and taking iron when it is not called for can causeiron overload disorder , potentially a very dangerous condition.cite journal
author=Oertel WH, Trenkwalder C, Zucconi M, "et al"
title=State of the art in restless legs syndrome therapy: Practice recommendations for treating restless legs syndrome
journal=Mov Disord
volume=22
issue=
pages=S466
year=2007
pmid=17516455
doi=10.1002/mds.21545]Pharmaceuticals
For those whose RLS disrupts or prevents sleep or regular daily activities, medication may be required. Many doctors currently use, and the
Mayo Clinic algorithm includes, medication from four categories:#
Dopamine agonist s such asropinirole ,pramipexole ,carbidopa /levodopa orpergolide .Ropinirole (Requip) was first approved In 2005 by theUS Food and Drug Administration (FDA) to treat moderate to severe Restless Legs Syndrome. The drug was first approved forParkinson's disease in 1997.Pramipexole (Mirapex, Sifrol, Mirapexen in the EU) received a positive recommendation by the EU Scientific Committee in February 2006. The FDA approved Mirapex for sale in the US in 2006.Rotigotine (Neupro), which is delivered by atransdermal patch was approved by the FDA in May 2007. It was approved for sale in the EU in 2007. There are some issues with the use of dopamine augmentation. Dopamine agonists may cause augmentation. This is a medical condition where the drug itself causes symptoms to increase in severity and/or occur earlier in the day. Dopamine agonists may also cause rebound, when symptoms increase as the drug wears off. Also, a recent study indicated that dopamine agonists used in restless leg patients can lead to an increase incompulsive gambling . [ [http://www.mayoclinic.org/news2007-rst/3918.html "Medical Therapy for Restless Legs Syndrome may Trigger Compulsive Gambling", Mayo Clinic in Rochester, February 08, 2007] ]
#Opioid s such aspropoxyphene ,oxycodone , ormethadone , etc.
#Benzodiazepine s, which often assist in staying asleep and reducing awakenings from the movements
#Anticonvulsant s, which often help people who experience the RLS sensations as painful, such ascarbamazepine [cite journal| journal =Am Fam Physician| year =1986| month =Jan| volume =33| issue =1| pages =147–52| title =Restless legs syndrome| author =Fox GN| pmid =3510520 ]Recently, several major pharmaceutical companies are reported to be marketing drugs without an explicit approval for RLS, which are "
off-label " applications for drugs approved for other diseases. The Restless Legs Syndrome Foundation [* [http://www.rls.org/NETCOMMUNITY/Page.aspx?&pid=471&srcid=-2 RLS Foundation] ] received 44% of its $1.4 million in funding from these pharmaceutical groups [ [http://www.newscientist.com/channel/health/mg19225755.100-patient-groups-special-swallowing-the-best-advice.html Marshall, Jessica, and Peter Aldhous. "Patient Groups Special." New Scientist, 10/26/06] ]Ropinirole vs. Pramipexole
A
meta-study published November 2007 compared previous 6-12 week long studies done for ropinirole and pramipexole for adverse reactions and efficacy. It found that while both drugs had the same efficacy, pramipexole had significantly lower incidences of nausea, vomiting and dizziness. This led the authors to conclude "differences in efficacy and tolerability favouring pramipexole over ropinirole can be observed."cite journal| author=Quilici S "et al." | title=Meta-analysis of the efficacy and tolerability of pramipexole versus ropinirole in the treatment of restless legs syndrome | journal=Sleep Med | year=2008 | doi=10.1016/j.sleep.2007.11.020 ] While a 52 weekopen label study found that "ropinirole treatment for RLS over 52 weeks was found to be well tolerated and appropriate for long-term use." cite journal| author=Garcia-Borreguero, Diego "et al."| title=A 52-week open-label study of the long-term safety of ropinirole in patients with restless legs syndrome| journal=Sleep Medicine| year=2007| pages=742–752| doi=10.1016/j.sleep.2006.09.009| volume=8 ]The non drug musculoskeletal approach
The non-drug musculoskeletal approach has been developed by a small group of doctors working at the London College of Osteopathic Medicine, London, UK and appears to produces relief of symptoms in 80–90% of patients. A small pilot study carried out at the London College of Osteopathic Medicine, using a specific form of manipulation, showed successful relief of symptoms in more that 80% of sufferers [Peters T W, "Restless Legs", "Osteopathy Today", October 2001.] . This followed the empirical observation that a large proportion of RLS sufferers have a "somatic dysfunction" at the lowermost level of the lumbar spine, and that a specific type of gentle manipulation could relieve their symptoms. One study has shown that RLS patients have increased rather than the normal decreased spinal cord excitability during sleep [Bara J et al. "Periodic limb movements in sleep: state dependent excitability of the spinal flexor reflex". "Neurology" 2000: 54(8):1609–1616. Cited in "Medical Bulletin", The Restless Legs Foundation, www.rls.org.] and this fits with the osteopathic concept of spinal facilitation postulated by Korr. Specific types of manipulation appear to reduce this excessive sensory input and relieve symptoms. This non drug treatment approach is free of the side effects associated with many of the drug treatments outlined above.
Prognosis
Epidemiology
Claims about the prevalence of restless legs syndrome can be confusing because its severity and frequency varies enormously between individual sufferers. RLS affects an estimated 7% to 10% of the general population in North America and Europe.cite journal |author=Gamaldo CE, Earley CJ |title=Restless legs syndrome: a clinical update |journal=Chest |volume=130 |issue=5 |pages=1596–604 |year=2006 |month=November |pmid=17099042 |doi=10.1378/chest.130.5.1596 |url=http://www.chestjournal.org/cgi/pmidlookup?view=long&pmid=17099042] cite journal |author=Allen R, Walters A, Montplaisir J, Hening W, Myers A, Bell T, Ferini-Strambi L |title=Restless legs syndrome prevalence and impact: REST general population study |journal=Arch. Intern. Med. |volume=165 |issue=11 |pages=1286–92 |year=2005 |pmid=15956009 |doi=10.1001/archinte.165.11.1286] cite journal |author=Wenning GK, Kiechl S, Seppi K, "et al" |title=Prevalence of movement disorders in men and women aged 50-89 years (Bruneck Study cohort): a population-based study |journal=Lancet Neurol |volume=4 |issue=12 |pages=815–20 |year=2005 |month=December |pmid=16297839 |doi=10.1016/S1474-4422(05)70226-X |url=http://linkinghub.elsevier.com/retrieve/pii/S1474-4422(05)70226-X] Only a minority of sufferers (around 2.7% of the population) experience daily or severe symptoms. RLS is twice as common in women as in men,cite journal |author=Berger K, Luedemann J, Trenkwalder C, John U, Kessler C |title=Sex and the risk of restless legs syndrome in the general population |journal=Arch. Intern. Med. |volume=164 |issue=2 |pages=196–202 |year=2004 |month=January |pmid=14744844 |doi=10.1001/archinte.164.2.196 |url=http://archinte.ama-assn.org/cgi/pmidlookup?view=long&pmid=14744844] and whites are more prone to RLS than African Americans. RLS occurs in 3% of individuals from the Mediterranean or Middle Eastern region, and in 1-5% of those from the Far East, indicating that different genetic or environmental factors, including diet, may play a role in the prevalence of this syndrome. [cite web |url=http://www.sleepfoundation.org/site/c.huIXKjM0IxF/b.2417141/k.C60C/Welcome.htm |title=Welcome - National Sleep Foundation |accessdate=2007-07-23 |format= |work=] With age, RLS becomes more common, and RLS diagnosed at an older age runs a more severe course.cite journal |author=Allen RP, Earley CJ |title=Restless legs syndrome: a review of clinical and pathophysiologic features |journal=J Clin Neurophysiol |volume=18 |issue=2 |pages=128–47 |year=2001 |month=March |pmid=11435804 |doi= |url=http://meta.wkhealth.com/pt/pt-core/template-journal/lwwgateway/media/landingpage.htm?issn=0736-0258&volume=18&issue=2&spage=128]
RLS is even more common in individuals with iron deficiency, pregnancy and end-stage renal disease.cite journal |author=Lee KA, Zaffke ME, Baratte-Beebe K |title=Restless legs syndrome and sleep disturbance during pregnancy: the role of folate and iron |journal=J Womens Health Gend Based Med |volume=10 |issue=4 |pages=335–41 |year=2001 |month=May |pmid=11445024 |doi=10.1089/152460901750269652] cite journal |author=Merlino G, Piani A, Dolso P, "et al" |title=Sleep disorders in patients with end-stage renal disease undergoing dialysis therapy |journal=Nephrol. Dial. Transplant. |volume=21 |issue=1 |pages=184–90 |year=2006 |month=January |pmid=16144846 |doi=10.1093/ndt/gfi144 |url=http://ndt.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=16144846] Neurologic conditions linked to RLS include
Parkinson disease ,spinal cerebellar atrophy ,spinal stenosis , lumbar sacralradiculopathy andCharcot-Marie-Tooth disease type 2. Approximately 80–90% of people with RLS also have periodic limb movement disorder (PLMD), which causes slow "jerks" or flexions of the affected body part. These occur during sleep (PLMS = periodic limb movement while sleeping) or while awake (PLMW—periodic limb movement while waking).The
National Sleep Foundation 's 1998 "Sleep in America" poll showed that up to 15 percent ofpregnant women developed RLS during the third trimester. [ [http://www.sleepfoundation.org/site/c.huIXKjM0IxF/b.2419237/k.83BF/Sleeping_By_Trimesters_3rd_Trimester.htm Sleep in America Poll] .National Sleep Foundation .]History
Earlier studies were done by
Thomas Willis (1622–1675) and byTheodor Wittmaack .WhoNamedIt|synd|2337|Wittmaack-Ekbom syndrome] Another early description of the disease and its symptoms were made byGeorge Miller Beard (1839-1883). In a 1945 publication titled 'Restless Legs', Swedish neurologistKarl-Axel Ekbom (1907-1977) described the disease and presented eight cases used for his studies. [Ekbom, K.-A. Restless legs: a clinical study. Acta Med. Scand. (Suppl.) 158: 1–123, 1945.]Controversy
As with many diseases with diffuse symptoms, there is controversy among physicians as to whether RLS is a distinct syndrome. The U.S.
National Institute of Neurological Disorders and Stroke publishes an information sheet [ [http://www.ninds.nih.gov/disorders/restless_legs/detail_restless_legs.htm Restless Legs Syndrome Fact Sheet] ] characterizing the syndrome but acknowledging it as a difficult diagnosis. Some physicians doubt that RLS actually exists as a legitimate clinical entity, but believe it to be a kind of "catch-all" category, perhaps related to a general heightenedsympathetic nervous system response that could be caused by any number of physical or emotional factors Fact|date=August 2007. Other physicians consider it a real entity that has specific diagnostic criteria. [cite journal |author=Montplaisir J; Boucher S; Nicolas A; Lesperance P; Gosselin A; Rompré P; Lavigne G |journal=Movement disorders |volume=13 |issue=2 |pages=324–9 |year=1998|pmid=9539348|url=http://www.ncbi.nlm.nih.gov/sites/entrez?db=PubMed&cmd=retrieve&dopt=AbstractPlus&list_uids=9539348 |title=Immobilization tests and periodic leg movements in sleep for the diagnosis of restless leg syndrome |doi=10.1002/mds.870130220]The U.K. support group for RLS calls itself the "Ekbom support group" and explains that RLS and "Ekbom's Syndrome" are two names for the same condition. [http://www.ekbom.org.uk/ Ekbom (Restless Legs) Support Group (UK)] ] However, RLS and
delusional parasitosis are entirely different conditions that share part of the Wittmaack-Ekbom syndrome eponym, as both syndromes were described by the same person, Karl-Axel Ekbom.Many doctors express the view that the incidence of restless leg syndrome is exaggerated by manufacturers of drugs used to treat it. [cite journal |author=Woloshin S, Schwartz L |title=Giving legs to restless legs: a case study of how the media helps make people sick |journal=PLoS Med. |volume=3 |issue=4 |pages=e170 |year=2006 |pmid=16597175 |doi=10.1371/journal.pmed.0030170] Others believe it is an underrecognized and undertreated disorder.
ee also
*
Actigraphy
*Akathisia : A similar condition.
*Disease mongering
*Parasomnia
*Sleep medicine References
External links
* [http://www.neuro.jhmi.edu/rls/about-us.html Center for RLS] , [http://www.neuro.jhmi.edu/rls/edu.htm education] at
Johns Hopkins
*Medicinenet|restless_leg_syndrome
*NINDS|restless_legs|restless legs
*DMOZ|Health/Conditions_and_Diseases/Sleep_Disorders/Restless_Legs_Syndrome/
Wikimedia Foundation. 2010.