- Diabetes mellitus
-
"Diabetes" redirects here. For other uses, see Diabetes (disambiguation).
Diabetes mellitus Classification and external resources 
Universal blue circle symbol for diabetes.[1]ICD-10 E10–E14 ICD-9 250 MedlinePlus 001214 eMedicine med/546 emerg/134 MeSH C18.452.394.750 Diabetes mellitus, often simply referred to as diabetes, is a group of metabolic diseases in which a person has high blood sugar, either because the body does not produce enough insulin, or because cells do not respond to the insulin that is produced. This high blood sugar produces the classical symptoms of polyuria (frequent urination), polydipsia (increased thirst) and polyphagia (increased hunger).
There are three main types of diabetes:
- Type 1 diabetes: results from the body's failure to produce insulin, and presently requires the person to inject insulin. (Also referred to as insulin-dependent diabetes mellitus, IDDM for short, and juvenile diabetes.)
- Type 2 diabetes: results from insulin resistance, a condition in which cells fail to use insulin properly, sometimes combined with an absolute insulin deficiency. (Formerly referred to as non-insulin-dependent diabetes mellitus, NIDDM for short, and adult-onset diabetes.)
- Gestational diabetes: is when pregnant women, who have never had diabetes before, have a high blood glucose level during pregnancy. It may precede development of type 2 DM.
Other forms of diabetes mellitus include congenital diabetes, which is due to genetic defects of insulin secretion, cystic fibrosis-related diabetes, steroid diabetes induced by high doses of glucocorticoids, and several forms of monogenic diabetes.
All forms of diabetes have been treatable since insulin became available in 1921, and type 2 diabetes may be controlled with medications. Both type 1 and 2 are chronic conditions that usually cannot be cured. Pancreas transplants have been tried with limited success in type 1 DM; gastric bypass surgery has been successful in many with morbid obesity and type 2 DM. Gestational diabetes usually resolves after delivery. Diabetes without proper treatments can cause many complications. Acute complications include hypoglycemia, diabetic ketoacidosis, or nonketotic hyperosmolar coma. Serious long-term complications include cardiovascular disease, chronic renal failure, retinal damage. Adequate treatment of diabetes is thus important, as well as blood pressure control and lifestyle factors such as smoking cessation and maintaining a healthy body weight.
As of 2000 at least 171 million people worldwide have diabetes, or 2.8% of the population.[2] Type 2 diabetes is by far the most common, affecting 90 to 95% of the U.S. diabetes population.[3]
Contents
Classification
Most cases of diabetes mellitus fall into three broad categories: type 1, type 2, and gestational diabetes. A few other types are described. The term diabetes, without qualification, usually refers to diabetes mellitus. The rare disease diabetes insipidus has similar symptoms as diabetes mellitus, but without disturbances in the sugar metabolism (insipidus meaning "without taste" in Latin).
Comparison of type 1 and 2 diabetes Feature Type 1 diabetes Type 2 diabetes Onset Sudden[4] Gradual[4] Age at onset Any age
(mostly young)[4]Mostly in adults Body habitus Thin[4] or normal[5] Often obese[4] Ketoacidosis Common[4] Rare[4] Autoantibodies Usually present[4] Absent[4] Endogenous insulin Low or absent[4] Normal, decreased
or increased[4]Concordance
in identical twins50%[4] 90%[4] Prevalence Less prevalent More prevalent
- 90 to 95% of
U.S. diabetics[3]The term "type 1 diabetes" has replaced several former terms, including childhood-onset diabetes, juvenile diabetes, and insulin-dependent diabetes mellitus (IDDM). Likewise, the term "type 2 diabetes" has replaced several former terms, including adult-onset diabetes, obesity-related diabetes, and non-insulin-dependent diabetes mellitus (NIDDM). Beyond these two types, there is no agreed-upon standard nomenclature. Various sources have defined "type 3 diabetes" as: gestational diabetes,[6] insulin-resistant type 1 diabetes (or "double diabetes"), type 2 diabetes which has progressed to require injected insulin, and latent autoimmune diabetes of adults (or LADA or "type 1.5" diabetes).[7]
Type 1 diabetes
Main article: Diabetes mellitus type 1Type 1 diabetes mellitus is characterized by loss of the insulin-producing beta cells of the islets of Langerhans in the pancreas leading to insulin deficiency. This type of diabetes can be further classified as immune-mediated or idiopathic. The majority of type 1 diabetes is of the immune-mediated nature, where beta cell loss is a T-cell mediated autoimmune attack.[8] There is no known preventive measure against type 1 diabetes, which causes approximately 10% of diabetes mellitus cases in North America and Europe. Most affected people are otherwise healthy and of a healthy weight when onset occurs. Sensitivity and responsiveness to insulin are usually normal, especially in the early stages. Type 1 diabetes can affect children or adults but was traditionally termed "juvenile diabetes" because it represents a majority of the diabetes cases in children.
"Brittle" diabetes, also known as unstable diabetes or labile diabetes, is a term that was traditionally used to describe to dramatic and recurrent swings in glucose levels, often occurring for no apparent reason in insulin-dependent diabetes. This term, however, has no biologic basis and should not be used.[9] There are many different reasons for type 1 diabetes to be accompanied by irregular and unpredictable hyperglycemias, frequently with ketosis, and sometimes serious hypoglycemias, including an impaired counterregulatory response to hypoglycemia, occult infection, gastroparesis (which leads to erratic absorption of dietary carbohydrates), and endocrinopathies (eg, Addison's disease).[10] These phenomena are believed to occur no more frequently than in 1% to 2% of persons with type 1 diabetes.[11]
Type 2 diabetes
Main article: Diabetes mellitus type 2Type 2 diabetes mellitus is characterized by insulin resistance which may be combined with relatively reduced insulin secretion. The defective responsiveness of body tissues to insulin is believed to involve the insulin receptor. However, the specific defects are not known. Diabetes mellitus due to a known defect are classified separately. Type 2 diabetes is the most common type.
In the early stage of type 2 diabetes, the predominant abnormality is reduced insulin sensitivity. At this stage hyperglycemia can be reversed by a variety of measures and medications that improve insulin sensitivity or reduce glucose production by the liver.
Gestational diabetes
Main article: Gestational diabetesGestational diabetes mellitus (GDM) resembles type 2 diabetes in several respects, involving a combination of relatively inadequate insulin secretion and responsiveness. It occurs in about 2%–5% of all pregnancies and may improve or disappear after delivery. Gestational diabetes is fully treatable but requires careful medical supervision throughout the pregnancy. About 20%–50% of affected women develop type 2 diabetes later in life.
Even though it may be transient, untreated gestational diabetes can damage the health of the fetus or mother. Risks to the baby include macrosomia (high birth weight), congenital cardiac and central nervous system anomalies, and skeletal muscle malformations. Increased fetal insulin may inhibit fetal surfactant production and cause respiratory distress syndrome. Hyperbilirubinemia may result from red blood cell destruction. In severe cases, perinatal death may occur, most commonly as a result of poor placental perfusion due to vascular impairment. Labor induction may be indicated with decreased placental function. A cesarean section may be performed if there is marked fetal distress or an increased risk of injury associated with macrosomia, such as shoulder dystocia.
A 2008 study completed in the U.S. found that the number of American women entering pregnancy with preexisting diabetes is increasing. In fact the rate of diabetes in expectant mothers has more than doubled in the past 6 years.[12] This is particularly problematic as diabetes raises the risk of complications during pregnancy, as well as increasing the potential that the children of diabetic mothers will also become diabetic in the future.
Other types
Pre-diabetes indicates a condition that occurs when a person's blood glucose levels are higher than normal but not high enough for a diagnosis of type 2 diabetes. Many people destined to develop type 2 diabetes spend many years in a state of pre-diabetes which has been termed "America's largest healthcare epidemic."[13]:10–11
Latent autoimmune diabetes of adults is a condition in which Type 1 diabetes develops in adults. Adults with LADA are frequently initially misdiagnosed as having Type 2 diabetes, based on age rather than etiology.
Some cases of diabetes are caused by the body's tissue receptors not responding to insulin (even when insulin levels are normal, which is what separates it from type 2 diabetes); this form is very uncommon. Genetic mutations (autosomal or mitochondrial) can lead to defects in beta cell function. Abnormal insulin action may also have been genetically determined in some cases. Any disease that causes extensive damage to the pancreas may lead to diabetes (for example, chronic pancreatitis and cystic fibrosis). Diseases associated with excessive secretion of insulin-antagonistic hormones can cause diabetes (which is typically resolved once the hormone excess is removed). Many drugs impair insulin secretion and some toxins damage pancreatic beta cells. The ICD-10 (1992) diagnostic entity, malnutrition-related diabetes mellitus (MRDM or MMDM, ICD-10 code E12), was deprecated by the World Health Organization when the current taxonomy was introduced in 1999.[14]
Signs and symptoms
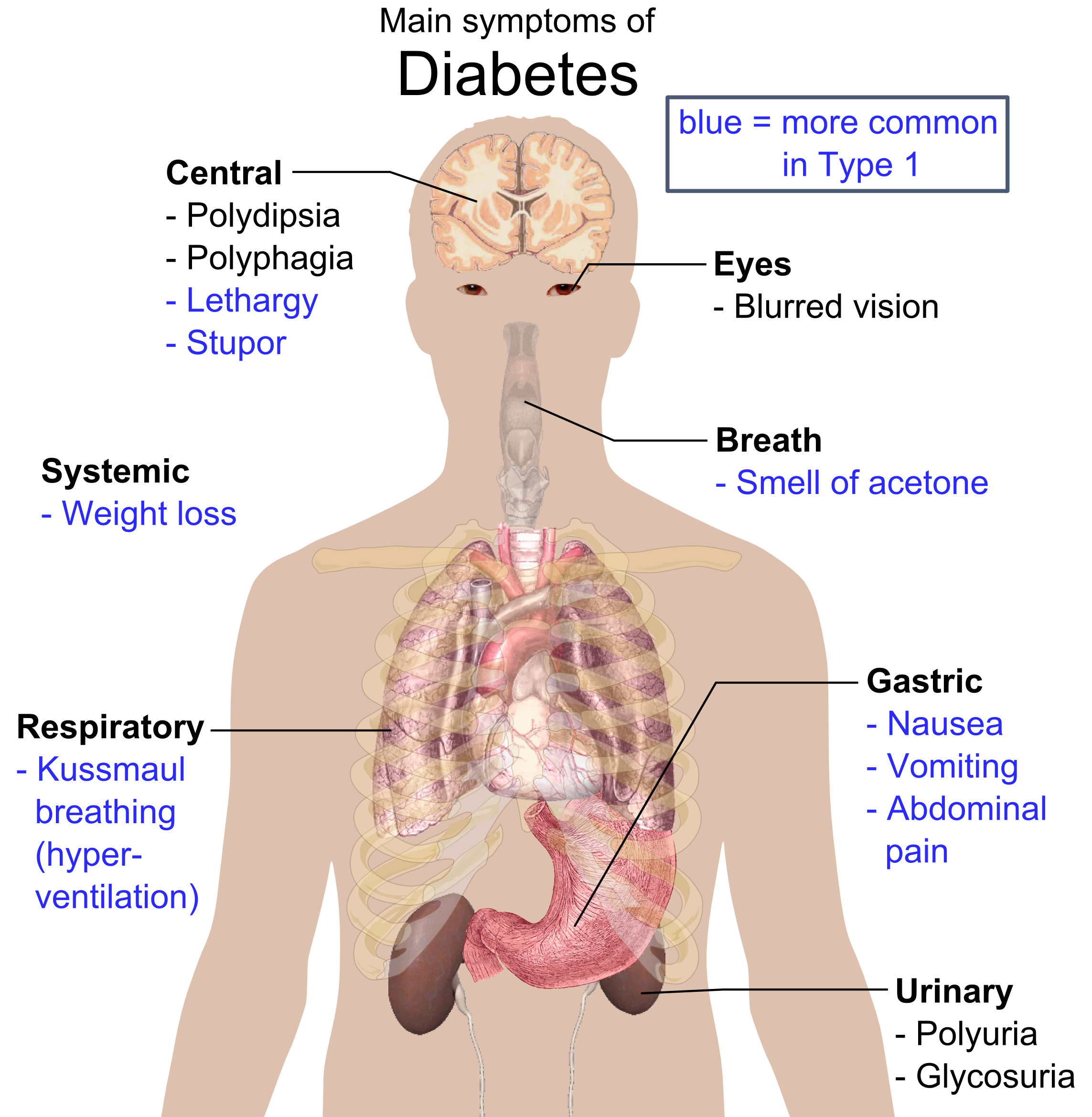
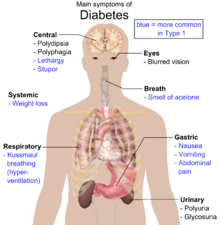 Overview of the most significant symptoms of diabetes.
Overview of the most significant symptoms of diabetes.
Hyperglycemia and osmosis
The classical symptoms of diabetes are polyuria (frequent urination), polydipsia (increased thirst) and polyphagia (increased hunger).[15] Symptoms may develop rapidly (weeks or months) in type 1 diabetes while in type 2 diabetes they usually develop much more slowly and may be subtle or absent.
Prolonged high blood glucose causes glucose absorption, which leads to changes in the shape of the lenses of the eyes, resulting in vision changes; sustained sensible glucose control usually returns the lens to its original shape. Blurred vision is a common complaint leading to a diabetes diagnosis; type 1 should always be suspected in cases of rapid vision change, whereas with type 2 change is generally more gradual, but should still be suspected[citation needed].
Diabetic emergencies
People (usually with type 1 diabetes) may also present with diabetic ketoacidosis, a state of metabolic dysregulation characterized by the smell of acetone; a rapid, deep breathing known as Kussmaul breathing; nausea; vomiting and abdominal pain; and altered states of consciousness.
A rarer but equally severe possibility is hyperosmolar nonketotic state, which is more common in type 2 diabetes and is mainly the result of dehydration. Often, the patient has been drinking extreme amounts of sugar-containing drinks, leading to a vicious circle in regard to the water loss.
Complications
Main article: Complications of diabetes mellitusAll forms of diabetes increase the risk of long-term complications. These typically develop after many years (10–20), but may be the first symptom in those who have otherwise not received a diagnosis before that time. The major long-term complications relate to damage to blood vessels.
Diabetes doubles the risk of cardiovascular disease.[16] The main "macrovascular" diseases (related to atherosclerosis of larger arteries) are ischemic heart disease (angina and myocardial infarction), stroke and peripheral vascular disease.
Diabetes also causes "microvascular" complications—damage to the small blood vessels.[17] Diabetic retinopathy, which affects blood vessel formation in the retina of the eye, can lead to visual symptoms, reduced vision, and potentially blindness. Diabetic nephropathy, the impact of diabetes on the kidneys, can lead to scarring changes in the kidney tissue, loss of small or progressively larger amounts of protein in the urine, and eventually chronic kidney disease requiring dialysis. Diabetic neuropathy is the impact of diabetes on the nervous system, most commonly causing numbness, tingling and pain in the feet and also increasing the risk of skin damage due to altered sensation. Together with vascular disease in the legs, neuropathy contributes to the risk of diabetes-related foot problems (such as diabetic foot ulcers) that can be difficult to treat and occasionally require amputation.
Other problems
A number of skin rashes can occur in diabetes that are collectively known as diabetic dermadromes.
Causes
The cause of diabetes depends on the type.
Type 1 diabetes is partly inherited and then triggered by certain infections, with some evidence pointing at Coxsackie B4 virus. There is a genetic element in individual susceptibility to some of these triggers which has been traced to particular HLA genotypes (i.e., the genetic "self" identifiers relied upon by the immune system). However, even in those who have inherited the susceptibility, type 1 diabetes mellitus seems to require an environmental trigger.
Type 2 diabetes is due primarily to lifestyle factors and genetics.[18]
Following is a comprehensive list of other causes of diabetes:[19]
- Genetic defects of β-cell Function
- Maturity onset diabetes of the young (MODY)
- Mitochondrial DNA mutations
- Genetic defects in insulin processing or insulin action
- Defects in proinsulin conversion
- Insulin gene mutations
- Insulin receptor mutations
- Exocrine Pancreatic Defects
- Chronic pancreatitis
- Pancreatectomy
- Pancreatic neoplasia
- Cystic fibrosis
- Hemochromatosis
- Fibrocalculous pancreatopathy
- Endocrinopathies
- Growth hormone excess (acromegaly)
- Cushing syndrome
- Hyperthyroidism
- Pheochromocytoma
- Glucagonoma
- Infections
- Cytomegalovirus infection
- Coxsackievirus B
- Drugs
- Glucocorticoids
- Thyroid hormone
- β-adrenergic agonists
Pathophysiology
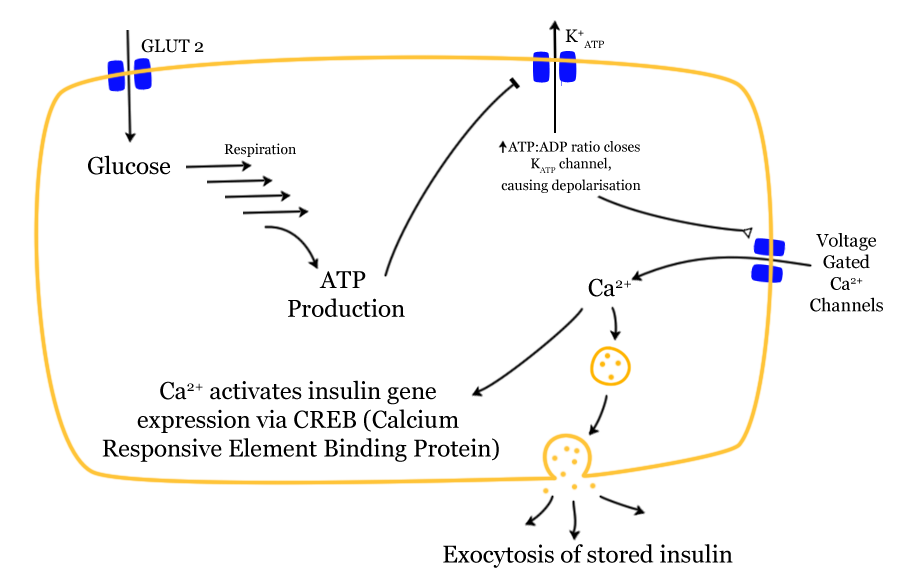
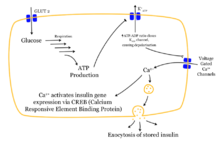 Mechanism of insulin release in normal pancreatic beta cells. Insulin production is more or less constant within the beta cells. Its release is triggered by food, chiefly food containing absorbable glucose.
Mechanism of insulin release in normal pancreatic beta cells. Insulin production is more or less constant within the beta cells. Its release is triggered by food, chiefly food containing absorbable glucose.Insulin is the principal hormone that regulates uptake of glucose from the blood into most cells (primarily muscle and fat cells, but not central nervous system cells). Therefore deficiency of insulin or the insensitivity of its receptors plays a central role in all forms of diabetes mellitus.
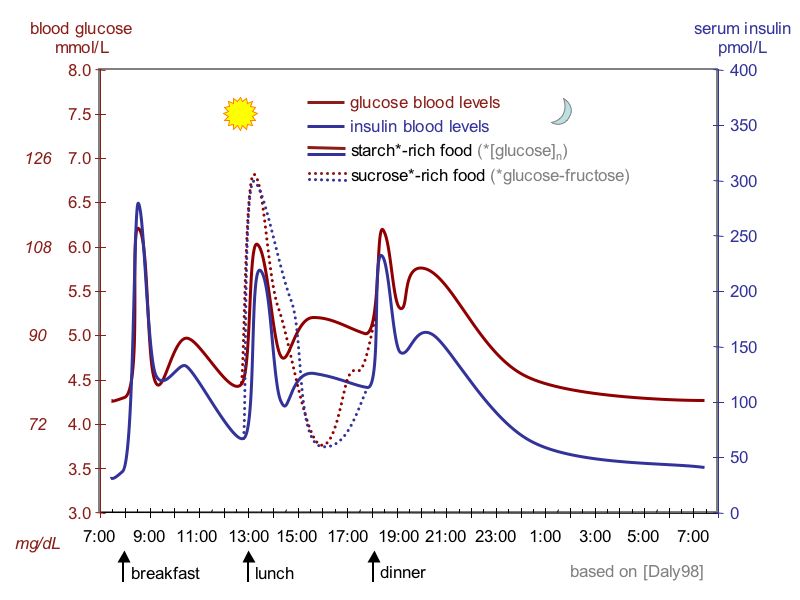
Humans are capable of digesting some carbohydrates, in particular those most common in food; starch, and some disaccharides such as sucrose, are converted within a few hours to simpler forms most notably the monosaccharide glucose, the principal carbohydrate energy source used by the body. The rest are passed on for processing by gut flora largely in the colon. Insulin is released into the blood by beta cells (β-cells), found in the Islets of Langerhans in the pancreas, in response to rising levels of blood glucose, typically after eating. Insulin is used by about two-thirds of the body's cells to absorb glucose from the blood for use as fuel, for conversion to other needed molecules, or for storage.
Insulin is also the principal control signal for conversion of glucose to glycogen for internal storage in liver and muscle cells. Lowered glucose levels result both in the reduced release of insulin from the beta cells and in the reverse conversion of glycogen to glucose when glucose levels fall. This is mainly controlled by the hormone glucagon which acts in the opposite manner to insulin. Glucose thus forcibly produced from internal liver cell stores (as glycogen) re-enters the bloodstream; muscle cells lack the necessary export mechanism. Normally liver cells do this when the level of insulin is low (which normally correlates with low levels of blood glucose).
Higher insulin levels increase some anabolic ("building up") processes such as cell growth and duplication, protein synthesis, and fat storage. Insulin (or its lack) is the principal signal in converting many of the bidirectional processes of metabolism from a catabolic to an anabolic direction, and vice versa. In particular, a low insulin level is the trigger for entering or leaving ketosis (the fat burning metabolic phase).
If the amount of insulin available is insufficient, if cells respond poorly to the effects of insulin (insulin insensitivity or resistance), or if the insulin itself is defective, then glucose will not have its usual effect so that glucose will not be absorbed properly by those body cells that require it nor will it be stored appropriately in the liver and muscles. The net effect is persistent high levels of blood glucose, poor protein synthesis, and other metabolic derangements, such as acidosis.
When the glucose concentration in the blood is raised beyond its renal threshold (about 10 mmol/L, although this may be altered in certain conditions, such as pregnancy), reabsorption of glucose in the proximal renal tubuli is incomplete, and part of the glucose remains in the urine (glycosuria). This increases the osmotic pressure of the urine and inhibits reabsorption of water by the kidney, resulting in increased urine production (polyuria) and increased fluid loss. Lost blood volume will be replaced osmotically from water held in body cells and other body compartments, causing dehydration and increased thirst.
Diagnosis
See also: Glycosylated hemoglobin and Glucose tolerance test2006 WHO Diabetes criteria[20] Condition 2 hour glucose Fasting glucose mmol/l(mg/dl) mmol/l(mg/dl) Normal <7.8 (<140) <6.1 (<110) Impaired fasting glycaemia <7.8 (<140) ≥ 6.1(≥110) & <7.0(<126) Impaired glucose tolerance ≥7.8 (≥140) <7.0 (<126) Diabetes mellitus ≥11.1 (≥200) ≥7.0 (≥126) Diabetes mellitus is characterized by recurrent or persistent hyperglycemia, and is diagnosed by demonstrating any one of the following:[14]
- Fasting plasma glucose level ≥ 7.0 mmol/L (126 mg/dL).
- Plasma glucose ≥ 11.1 mmol/L (200 mg/dL) two hours after a 75 g oral glucose load as in a glucose tolerance test.
- Symptoms of hyperglycemia and casual plasma glucose ≥ 11.1 mmol/L (200 mg/dL).
- Glycated hemoglobin (Hb A1C) ≥ 6.5%.[21]
A positive result, in the absence of unequivocal hyperglycemia, should be confirmed by a repeat of any of the above-listed methods on a different day. It is preferable to measure a fasting glucose level because of the ease of measurement and the considerable time commitment of formal glucose tolerance testing, which takes two hours to complete and offers no prognostic advantage over the fasting test.[22] According to the current definition, two fasting glucose measurements above 126 mg/dL (7.0 mmol/L) is considered diagnostic for diabetes mellitus.
People with fasting glucose levels from 100 to 125 mg/dL (5.6 to 6.9 mmol/L) are considered to have impaired fasting glucose. Patients with plasma glucose at or above 140 mg/dL (7.8 mmol/L), but not over 200 mg/dL (11.1 mmol/L), two hours after a 75 g oral glucose load are considered to have impaired glucose tolerance. Of these two pre-diabetic states, the latter in particular is a major risk factor for progression to full-blown diabetes mellitus as well as cardiovascular disease.[23]
Glycated hemoglobin is better than fasting glucose for determining risks of cardiovascular disease and death from any cause.[24]
Management
Main article: Diabetes managementDiabetes mellitus is a chronic disease which cannot be cured except in very specific situations. Management concentrates on keeping blood sugar levels as close to normal ("euglycemia") as possible, without causing hypoglycemia. This can usually be accomplished with diet, exercise, and use of appropriate medications (insulin in the case of type 1 diabetes, oral medications as well as possibly insulin in type 2 diabetes).
Patient education, understanding, and participation is vital since the complications of diabetes are far less common and less severe in people who have well-managed blood sugar levels.[25][26] The goal of treatment is an HbA1C level of 6.5%, but should not be lower than that, and may be set higher.[27] Attention is also paid to other health problems that may accelerate the deleterious effects of diabetes. These include smoking, elevated cholesterol levels, obesity, high blood pressure, and lack of regular exercise.[27]
Lifestyle
See also: Diabetic dietThere are roles for patient education, dietetic support, sensible exercise, with the goal of keeping both short-term and long-term blood glucose levels within acceptable bounds. In addition, given the associated higher risks of cardiovascular disease, lifestyle modifications are recommended to control blood pressure.[28]
Medications
- Oral medications
Main article: Anti-diabetic medicationMetformin is generally recommended as a first line treatment for type 2 diabetes as there is good evidence that it decreases mortality.[29] Routine use of aspirin however has not been found to improve outcomes in uncomplicated diabetes.[30]
- Insulin
Main article: Insulin therapyType 1 diabetes is typically treated with a combinations of regular and NPH insulin, or synthetic insulin analogs. When insulin is used in type 2 diabetes, a long-acting formulation is usually added initially, while continuing oral medications.[29] Doses of insulin are then increased to effect.[29]
Support
In countries using a general practitioner system, such as the United Kingdom, care may take place mainly outside hospitals, with hospital-based specialist care used only in case of complications, difficult blood sugar control, or research projects. In other circumstances, general practitioners and specialists share care of a patient in a team approach. Optometrists, podiatrists/chiropodists, dietitians, physiotherapists, nursing specialists (e.g., DSNs (Diabetic Specialist Nurse)), nurse practitioners, or certified diabetes educators, may jointly provide multidisciplinary expertise.[citation needed]
Epidemiology
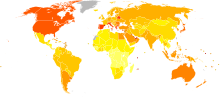 Prevalence of diabetes worldwide in 2000 (per 1000 inhabitants). World average was 2.8%.no data≤ 7.57.5–1515–22.522.5–3030–37.537.5–4545–52.552.5–6060–67.567.5–7575–82.5≥ 82.5
Prevalence of diabetes worldwide in 2000 (per 1000 inhabitants). World average was 2.8%.no data≤ 7.57.5–1515–22.522.5–3030–37.537.5–4545–52.552.5–6060–67.567.5–7575–82.5≥ 82.5 Disability-adjusted life year for diabetes mellitus per 100,000 inhabitants in 2004.no data<100100-200200-300300-400400-500500-600600-700700-800800-900900-10001000-1500>1500
Disability-adjusted life year for diabetes mellitus per 100,000 inhabitants in 2004.no data<100100-200200-300300-400400-500500-600600-700700-800800-900900-10001000-1500>1500In 2000, according to the World Health Organization, at least 171 million people worldwide suffer from diabetes, or 2.8% of the population.[2] Its incidence is increasing rapidly, and it is estimated that by 2030, this number will almost double.[2] Diabetes mellitus occurs throughout the world, but is more common (especially type 2) in the more developed countries. The greatest increase in prevalence is, however, expected to occur in Asia and Africa, where most patients will probably be found by 2030.[2] The increase in incidence of diabetes in developing countries follows the trend of urbanization and lifestyle changes, perhaps most importantly a "Western-style" diet. This has suggested an environmental (i.e., dietary) effect, but there is little understanding of the mechanism(s) at present, though there is much speculation, some of it most compellingly presented.[2]
- Prevalence in the United States
For at least 20 years, diabetes rates in North America have been increasing substantially. In 2010 nearly 26 million people have diabetes in the United States alone, from those 7 million people remain undiagnosed. Another 57 million people are estimated to have pre-diabetes.[31]
The Centers for Disease Control has termed the change an epidemic.[32] The National Diabetes Information Clearinghouse estimates that diabetes costs $132 billion in the United States alone every year. About 5%–10% of diabetes cases in North America are type 1, with the rest being type 2. The fraction of type 1 in other parts of the world differs. Most of this difference is not currently understood. The American Diabetes Association cite the 2003 assessment of the National Center for Chronic Disease Prevention and Health Promotion (Centers for Disease Control and Prevention) that 1 in 3 Americans born after 2000 will develop diabetes in their lifetime.[33][34]
According to the American Diabetes Association, approximately 18.3% (8.6 million) of Americans age 60 and older have diabetes.[35] Diabetes mellitus prevalence increases with age, and the numbers of older persons with diabetes are expected to grow as the elderly population increases in number. The National Health and Nutrition Examination Survey (NHANES III) demonstrated that, in the population over 65 years old, 18% to 20% have diabetes, with 40% having either diabetes or its precursor form of impaired glucose tolerance.[36]
- Prevalence in Australia
Indigenous populations in first world countries have a higher prevalence and increasing incidence of diabetes than their corresponding non-indigenous populations. In Australia the age-standardised prevalence of self-reported diabetes in Indigenous Australians is almost 4 times that of non-indigenous Australians.[37] Preventative community health programs such as Sugar Man (diabetes education) are showing some success in tackling this problem.
Etymology
The word “diabetes” (
 /ˌdaɪ.əˈbiːtiːz/ or /ˌdaɪ.əˈbiːtɨs/) comes from Latin diabētēs, which in turn comes from Ancient Greek διαβήτης (diabētēs) which literally means “a passer through; a siphon.”[38] Ancient Greek physician Aretaeus of Cappadocia (fl. 1st century CE) used that word, with the intended meaning “excessive discharge of urine,” as the name for the disease.[39][40] Ultimately, the word comes from Greek διαβαίνειν (diabainein), meaning “to pass through,”[38] which is composed of δια- (dia-), meaning “through” and βαίνειν (bainein), meaning “to go”.[39] The word “diabetes” is first recorded in English, in the form diabete, in a medical text written around 1425.
/ˌdaɪ.əˈbiːtiːz/ or /ˌdaɪ.əˈbiːtɨs/) comes from Latin diabētēs, which in turn comes from Ancient Greek διαβήτης (diabētēs) which literally means “a passer through; a siphon.”[38] Ancient Greek physician Aretaeus of Cappadocia (fl. 1st century CE) used that word, with the intended meaning “excessive discharge of urine,” as the name for the disease.[39][40] Ultimately, the word comes from Greek διαβαίνειν (diabainein), meaning “to pass through,”[38] which is composed of δια- (dia-), meaning “through” and βαίνειν (bainein), meaning “to go”.[39] The word “diabetes” is first recorded in English, in the form diabete, in a medical text written around 1425.The word “mellitus” (/mɨˈlaɪtəs/ or /ˈmɛlɨtəs/) comes from the classical Latin word mellītus, meaning “mellite”[41] (i.e. sweetened with honey;[41] honey-sweet[42]). The Latin word comes from mell-, which comes from mel, meaning “honey;[41][42] sweetness;[42] pleasant thing,[42]” and the suffix -ītus,[41] whose meaning is the same as that of the English suffix “-ite.”[43] It was Thomas Willis who in 1675 added “mellitus” to the word “diabetes” as a designation for the disease, when he noticed that the urine of a diabetic had a sweet taste (glycosuria).[40] This sweet taste had been noticed in urine by the ancient Greeks, Chinese, Egyptians, Indians, and Persians.
History
Diabetes is one of the oldest known diseases.[40] An Egyptian manuscript from c. 1550 BCE mentions the phrase “the passing of too much urine.”[40] The great Indian physician Sushruta (fl. 6th century BCE)[40] identified the disease and classified it as Medhumeha.[44] He further identified it with obesity and sedentary lifestyle, advising exercises to help "cure" it.[44] The ancient Indians tested for diabetes by observing whether ants were attracted to a person's urine, and called the ailment "sweet urine disease" (Madhumeha).
Concerning the sweetness of urine, it is to be noted that the Chinese, Japanese and Korean words for diabetes are based on the same ideographs (糖尿病) which mean "sugar urine disease". It was in 1776 that Matthew Dobson confirmed that the sweet taste comes from an excess of a kind of sugar in the urine and blood.[45]
The first complete clinical description of diabetes was given by the Ancient Greek physician Aretaeus of Cappadocia (fl. 1st century CE), who noted the excessive amount of urine which passed through the kidneys and gave the disease the name “diabetes.”[40]
Diabetes mellitus appears to have been a death sentence in the ancient era. Hippocrates makes no mention of it, which may indicate that he felt the disease was incurable. Aretaeus did attempt to treat it but could not give a good prognosis; he commented that "life (with diabetes) is short, disgusting and painful."[46]
In medieval Persia, Avicenna (980–1037) provided a detailed account on diabetes mellitus in The Canon of Medicine, "describing the abnormal appetite and the collapse of sexual functions," and he documented the sweet taste of diabetic urine. Like Aretaeus before him, Avicenna recognized a primary and secondary diabetes. He also described diabetic gangrene, and treated diabetes using a mixture of lupine, trigonella (fenugreek), and zedoary seed, which produces a considerable reduction in the excretion of sugar, a treatment which is still prescribed in modern times. Avicenna also "described diabetes insipidus very precisely for the first time", though it was later Johann Peter Frank (1745–1821) who first differentiated between diabetes mellitus and diabetes insipidus.[47][verification needed]
Although diabetes has been recognized since antiquity, and treatments of various efficacy have been known in various regions since the Middle Ages, and in legend for much longer, pathogenesis of diabetes has only been understood experimentally since about 1900.[48] The discovery of a role for the pancreas in diabetes is generally ascribed to Joseph von Mering and Oskar Minkowski, who in 1889 found that dogs whose pancreas was removed developed all the signs and symptoms of diabetes and died shortly afterwards.[49] In 1910, Sir Edward Albert Sharpey-Schafer suggested that people with diabetes were deficient in a single chemical that was normally produced by the pancreas—he proposed calling this substance insulin, from the Latin insula, meaning island, in reference to the insulin-producing islets of Langerhans in the pancreas.
The endocrine role of the pancreas in metabolism, and indeed the existence of insulin, was not further clarified until 1921, when Sir Frederick Grant Banting and Charles Herbert Best repeated the work of Von Mering and Minkowski, and went further to demonstrate they could reverse induced diabetes in dogs by giving them an extract from the pancreatic islets of Langerhans of healthy dogs.[50] Banting, Best, and colleagues (especially the chemist Collip) went on to purify the hormone insulin from bovine pancreases at the University of Toronto. This led to the availability of an effective treatment—insulin injections—and the first patient was treated in 1922. For this, Banting and laboratory director MacLeod received the Nobel Prize in Physiology or Medicine in 1923; both shared their Prize money with others in the team who were not recognized, in particular Best and Collip. Banting and Best made the patent available without charge and did not attempt to control commercial production. Insulin production and therapy rapidly spread around the world, largely as a result of this decision. Banting is honored by World Diabetes Day which is held on his birthday, November 14.
The distinction between what is now known as type 1 diabetes and type 2 diabetes was first clearly made by Sir Harold Percival (Harry) Himsworth, and published in January 1936.[51]
Despite the availability of treatment, diabetes has remained a major cause of death. For instance, statistics reveal that the cause-specific mortality rate during 1927 amounted to about 47.7 per 100,000 population in Malta.[52]
Other landmark discoveries include:[48]
- Identification of the first of the sulfonylureas in 1942
- Reintroduction of the use of biguanides for Type 2 diabetes in the late 1950s. The initial phenformin was withdrawn worldwide (in the U.S. in 1977) due to its potential for sometimes fatal lactic acidosis and metformin was first marketed in France in 1979, but not until 1994 in the US.
- The determination of the amino acid sequence of insulin (by Sir Frederick Sanger, for which he received a Nobel Prize)
- The radioimmunoassay for insulin, as discovered by Rosalyn Yalow and Solomon Berson (gaining Yalow the 1977 Nobel Prize in Physiology or Medicine)[53]
- The three-dimensional structure of insulin (PDB 2INS)
- Dr Gerald Reaven's identification of the constellation of symptoms now called metabolic syndrome in 1988
- Demonstration that intensive glycemic control in type 1 diabetes reduces chronic side effects more as glucose levels approach 'normal' in a large longitudinal study,[54] and also in type 2 diabetics in other large studies
- Identification of the first thiazolidinedione as an effective insulin sensitizer during the 1990s
In 1980, U.S. biotech company Genentech developed biosynthetic human insulin. The insulin was isolated from genetically altered bacteria (the bacteria contain the human gene for synthesizing synthetic human insulin), which produce large quantities of insulin. The purified insulin is distributed to pharmacies for use by diabetes patients. Initially, this development was not regarded by the medical profession as a clinically meaningful development. However, by 1996, the advent of insulin analogues which had vastly improved absorption, distribution, metabolism, and excretion (ADME) characteristics which were clinically meaningful based on this early biotechnology development.
Society and culture
The 1990 "St. Vincent Declaration"[55][56] was the result of international efforts to improve the care accorded to those with diabetes. Doing so is important both in terms of quality of life and life expectancy but also economically—expenses due to diabetes have been shown to be a major drain on health-and productivity-related resources for healthcare systems and governments.
Several countries established more and less successful national diabetes programmes to improve treatment of the disease.[57]
A study shows that diabetic patients with neuropathic symptoms such as numbness or tingling in feet or hands are twice as likely to be unemployed as those without the symptoms.[58]
In other animals
Main articles: diabetes in dogs and diabetes in catsIn animals, diabetes is most commonly encountered in dogs and cats. Middle-aged animals are most commonly affected. Female dogs are twice as likely to be affected as males, while according to some sources male cats are also more prone than females. In both species, all breeds may be affected, but some small dog breeds are particularly likely to develop diabetes, such as Miniature Poodles.[59] The symptoms may relate to fluid loss and polyuria, but the course may also be insidious. Diabetic animals are more prone to infections. The long-term complications recognised in humans are much rarer in animals. The principles of treatment (weight loss, oral antidiabetics, subcutaneous insulin) and management of emergencies (e.g. ketoacidosis) are similar to those in humans.[59]
References
- ^ "Diabetes Blue Circle Symbol". International Diabetes Federation. 17 March 2006. http://www.diabetesbluecircle.org.
- ^ a b c d e Wild S, Roglic G, Green A, Sicree R, King H (May 2004). "Global prevalence of diabetes: estimates for 2000 and projections for 2030". Diabetes Care 27 (5): 1047–53. doi:10.2337/diacare.27.5.1047. PMID 15111519.
- ^ a b "Type 2 Diabetes Overview". Web MD. http://diabetes.webmd.com/guide/type-2-diabetes.
- ^ a b c d e f g h i j k l m Elizabeth D Agabegi; Agabegi, Steven S. (2008). Step-Up to Medicine (Step-Up Series). Hagerstwon, MD: Lippincott Williams & Wilkins. ISBN 0-7817-7153-6.
- ^ Lambert, P. (2002). "What is Type 1 Diabetes?". Medicine 30: 1–5. doi:10.1383/medc.30.1.1.28264.
- ^ "Other "types" of diabetes". American Diabetes Association. August 25, 2005. http://www.diabetes.org/other-types.jsp.
- ^ "Diseases: Johns Hopkins Autoimmune Disease Research Center". http://autoimmune.pathology.jhmi.edu/diseases.cfm?systemID=3&DiseaseID=23. Retrieved 2007-09-23.
- ^ Rother KI (April 2007). "Diabetes treatment—bridging the divide". The New England Journal of Medicine 356 (15): 1499–501. doi:10.1056/NEJMp078030. PMID 17429082.
- ^ "Diabetes Mellitus (DM): Diabetes Mellitus and Disorders of Carbohydrate Metabolism: Merck Manual Professional". Merck.com. http://www.merck.com/mmpe/sec12/ch158/ch158b.html#sec12-ch158-ch158b-1206. Retrieved 2010-07-30.
- ^ "Diabetes Mellitus (DM): Diabetes Mellitus and Disorders of Carbohydrate Metabolism: Merck Manual Professional". Merck.com. http://www.merck.com/mmpe/sec12/ch158/ch158b.html#sec12-ch158-ch158b-1206. Retrieved 2010-07-30.
- ^ Dorner M, Pinget M, Brogard JM (May 1977). "Essential labile diabetes" (in German). MMW Munch Med Wochenschr 119 (19): 671–4. PMID 406527.
- ^ Lawrence JM, Contreras R, Chen W, Sacks DA (May 2008). "Trends in the prevalence of preexisting diabetes and gestational diabetes mellitus among a racially/ethnically diverse population of pregnant women, 1999–2005". Diabetes Care 31 (5): 899–904. doi:10.2337/dc07-2345. PMID 18223030.
- ^ Handelsman Yehuda, MD. "A Doctor's Diagnosis: Prediabetes". Power of Prevention 1 (2): 2009.
- ^ a b World Health Organisation Department of Noncommunicable Disease Surveillance (1999). "Definition, Diagnosis and Classification of Diabetes Mellitus and its Complications" (PDF). http://whqlibdoc.who.int/hq/1999/WHO_NCD_NCS_99.2.pdf.
- ^ Cooke DW, Plotnick L (November 2008). "Type 1 diabetes mellitus in pediatrics". Pediatr Rev 29 (11): 374–84; quiz 385. doi:10.1542/pir.29-11-374. PMID 18977856.
- ^ "Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies : The Lancet". http://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2810%2960484-9/fulltext.
- ^ Boussageon R, Bejan-Angoulvant T, Saadatian-Elahi M, et al. (2011). "Effect of intensive glucose lowering treatment on all cause mortality, cardiovascular death, and microvascular events in type 2 diabetes: meta-analysis of randomised controlled trials". BMJ 343: d4169. doi:10.1136/bmj.d4169. PMC 3144314. PMID 21791495. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=3144314.
- ^ Risérus U, Willett WC, Hu FB (January 2009). "Dietary fats and prevention of type 2 diabetes". Progress in Lipid Research 48 (1): 44–51. doi:10.1016/j.plipres.2008.10.002. PMC 2654180. PMID 19032965. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2654180.
- ^ Unless otherwise specified, reference is: Table 20-5 in Mitchell, Richard Sheppard; Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson. Robbins Basic Pathology. Philadelphia: Saunders. ISBN 1-4160-2973-7. 8th edition.
- ^ "Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycemia" (pdf). World Health Organization. www.who.int. 2006. http://www.who.int/diabetes/publications/Definition%20and%20diagnosis%20of%20diabetes_new.pdf. Retrieved 2011-02-20.
- ^ ""Diabetes Care" January 2010". American Diabetes Association. http://care.diabetesjournals.org/content/33/Supplement_1/S3.full. Retrieved 2010-01-29.
- ^ Saydah SH, Miret M, Sung J, Varas C, Gause D, Brancati FL (August 2001). "Postchallenge hyperglycemia and mortality in a national sample of U.S. adults". Diabetes Care 24 (8): 1397–402. doi:10.2337/diacare.24.8.1397. PMID 11473076.
- ^ Santaguida PL, Balion C, Hunt D, Morrison K, Gerstein H, Raina P, Booker L, Yazdi H. "Diagnosis, Prognosis, and Treatment of Impaired Glucose Tolerance and Impaired Fasting Glucose". Summary of Evidence Report/Technology Assessment, No. 128. Agency for Healthcare Research and Quality. http://www.ahrq.gov/clinic/epcsums/impglusum.htm. Retrieved 2008-07-20.
- ^ Selvin E, Steffes MW, Zhu H et al (2010). "Glycated hemoglobin, diabetes, and cardiovascular risk in nondiabetic adults". N. Engl. J. Med. 362 (9): 800–11. doi:10.1056/NEJMoa0908359. PMC 2872990. PMID 20200384. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2872990.
- ^ Nathan DM, Cleary PA, Backlund JY, et al. (December 2005). "Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes". The New England Journal of Medicine 353 (25): 2643–53. doi:10.1056/NEJMoa052187. PMC 2637991. PMID 16371630. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2637991.
- ^ "The effect of intensive diabetes therapy on the development and progression of neuropathy. The Diabetes Control and Complications Trial Research Group". Annals of Internal Medicine 122 (8): 561–8. April 1995. doi:10.1059/0003-4819-122-8-199504150-00001 (inactive 2009-10-31). PMID 7887548. http://www.annals.org/cgi/pmidlookup?view=long&pmid=7887548.
- ^ a b National Institute for Health and Clinical Excellence. Clinical guideline 66: Type 2 diabetes. London, 2008.
- ^ Adler AI, Stratton IM, Neil HA, et al. (August 2000). "Association of systolic blood pressure with macrovascular and microvascular complications of type 2 diabetes (UKPDS 36): prospective observational study". BMJ 321 (7258): 412–9. doi:10.1136/bmj.321.7258.412. PMC 27455. PMID 10938049. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=27455.
- ^ a b c Ripsin, CM; Kang, H, Urban, RJ (2009-01-01). "Management of blood glucose in type 2 diabetes mellitus". American family physician 79 (1): 29–36. PMID 19145963.
- ^ Pignone M, Alberts MJ, Colwell JA, et al. (June 2010). "Aspirin for primary prevention of cardiovascular events in people with diabetes: a position statement of the American Diabetes Association, a scientific statement of the American Heart Association, and an expert consensus document of the American College of Cardiology Foundation". Diabetes Care 33 (6): 1395–402. doi:10.2337/dc10-0555. PMC 2875463. PMID 20508233. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2875463.
- ^ CDC.gov
- ^ "CDC's Diabetes Program-News and Information-Press Releases-October 26, 2000". http://www.cdc.gov/Diabetes/news/docs/010126.htm. Retrieved 2008-06-23.
- ^ Narayan KM, Boyle JP, Thompson TJ, Sorensen SW, Williamson DF (October 2003). "Lifetime risk for diabetes mellitus in the United States". JAMA 290 (14): 1884–90. doi:10.1001/jama.290.14.1884. PMID 14532317.
- ^ American Diabetes Association (2005). "Total Prevalence of Diabetes & Pre-diabetes". Archived from the original on 2006-02-08. http://web.archive.org/web/20060208032127/http://www.diabetes.org/diabetes-statistics/prevalence.jsp. Retrieved 2006-03-17.
- ^ "Seniors and Diabetes". Elderly And Diabetes-Diabetes and Seniors. LifeMed Media. 2006. http://www.dlife.com/dLife/do/ShowContent/daily_living/seniors/. Retrieved 2007-05-14.
- ^ Harris MI, Flegal KM, Cowie CC, et al. (April 1998). "Prevalence of diabetes, impaired fasting glucose, and impaired glucose tolerance in U.S. adults. The Third National Health and Nutrition Examination Survey, 1988–1994". Diabetes Care 21 (4): 518–24. doi:10.2337/diacare.21.4.518. PMID 9571335.
- ^ Australian Institute for Health and Welfare. "Diabetes, an overview". Archived from the original on 2008-06-17. http://web.archive.org/web/20080617222036/http://www.aihw.gov.au/indigenous/health/diabetes.cfm. Retrieved 2008-06-23.
- ^ a b Oxford English Dictionary. diabetes. Retrieved 2011-06-10.
- ^ a b Harper, Douglas (2001–2010). "Online Etymology Dictionary. diabetes.". http://www.etymonline.com/index.php?search=diabetes&searchmode=none. Retrieved 2011-06-10
- ^ a b c d e f Dallas, John (2011). "Royal College of Physicians of Edinburgh. Diabetes, Doctors and Dogs: An exhibition on Diabetes and Endocrinology by the College Library for the 43rd St. Andrew's Day Festival Symposium". http://www.rcpe.ac.uk/library/exhibitions/diabetes/
- ^ a b c d Oxford English Dictionary. mellite. Retrieved 2011-06-10.
- ^ a b c d "MyEtimology. mellitus.". http://www.myetymology.com/latin/mellitus.html. Retrieved 2011-06-10
- ^ Oxford English Dictionary. -ite. Retrieved 2011-06-10.
- ^ a b Dwivedi, Girish & Dwivedi, Shridhar (2007). History of Medicine: Sushruta – the Clinician – Teacher par Excellence. National Informatics Centre (Government of India).
- ^ Dobson, M. (1776). "Nature of the urine in diabetes". Medical Observations and Inquiries 5: 298–310.
- ^ Medvei, Victor Cornelius (1993). The history of clinical endocrinology. Carnforth, Lancs., U.K: Parthenon Pub. Group. pp. 23–34. ISBN 1-85070-427-9.
- ^ Nabipour, I. (2003). "Clinical Endocrinology in the Islamic Civilization in Iran". International Journal of Endocrinology and Metabolism 1: 43–45 [44–5].
- ^ a b Patlak M (December 2002). "New weapons to combat an ancient disease: treating diabetes". The FASEB Journal 16 (14): 1853. PMID 12468446. http://www.fasebj.org/content/16/14/1853.2.
- ^ Von Mehring J, Minkowski O. (1890). "Diabetes mellitus nach pankreasexstirpation". Arch Exp Pathol Pharmakol 26 (5–6): 371–387. doi:10.1007/BF01831214.
- ^ Banting FG, Best CH, Collip JB, Campbell WR, Fletcher AA (November 1991). "Pancreatic extracts in the treatment of diabetes mellitus: preliminary report. 1922". CMAJ 145 (10): 1281–6. PMC 1335942. PMID 1933711. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1335942.
- ^ Himsworth (1936). "Diabetes mellitus: its differentiation into insulin-sensitive and insulin-insensitive types". Lancet i (5864): 127–30. doi:10.1016/S0140-6736(01)36134-2.
- ^ Department of Health (Malta), 1897–1972:Annual Reports.
- ^ Yalow RS, Berson SA (July 1960). "Immunoassay of endogenous plasma insulin in man". The Journal of Clinical Investigation 39 (7): 1157–75. doi:10.1172/JCI104130. PMC 441860. PMID 13846364. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=441860.
- ^ The Diabetes Control And Complications Trial Research Group (September 1993). "The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group". The New England Journal of Medicine 329 (14): 977–86. doi:10.1056/NEJM199309303291401. PMID 8366922.
- ^ Theodore H. Tulchinsky, Elena A. Varavikova (2008). The New Public Health, Second Edition. New York: Academic Press. p. 200. ISBN 0-12-370890-7.
- ^ Piwernetz K, Home PD, Snorgaard O, Antsiferov M, Staehr-Johansen K, Krans M (May 1993). "Monitoring the targets of the St Vincent Declaration and the implementation of quality management in diabetes care: the DIABCARE initiative. The DIABCARE Monitoring Group of the St Vincent Declaration Steering Committee". Diabetic Medicine 10 (4): 371–7. doi:10.1111/j.1464-5491.1993.tb00083.x. PMID 8508624.
- ^ Dubois, HFW and Bankauskaite, V (2005). "Type 2 diabetes programmes in Europe" (PDF). Euro Observer 7 (2): 5–6. http://www.euro.who.int/Document/Obs/EuroObserver7_3.pdf.
- ^ Stewart WF, Ricci JA, Chee E, Hirsch AG, Brandenburg NA (June 2007). "Lost productive time and costs due to diabetes and diabetic neuropathic pain in the US workforce". J. Occup. Environ. Med. 49 (6): 672–9. doi:10.1097/JOM.0b013e318065b83a. PMID 17563611.
- ^ a b "Diabetes mellitus". Merck Veterinary Manual, 9th edition (online version). 2005. http://www.merckvetmanual.com/mvm/index.jsp?cfile=htm/bc/40302.htm. Retrieved 2011-10-23.
External links
- Diabetes at the Open Directory Project
- American Diabetes Association
- IDF Diabetes Atlas
- International Diabetes Federation
- National Diabetes Education Program
- Peers for Progress
- World Diabetes Day
Diabetes (E10–E14, 250) Types of diabetes Prediabetes (Impaired fasting glucose, Impaired glucose tolerance)Blood tests Diabetes management Complications/prognosis Diabetic comas (Diabetic hypoglycemia, Diabetic ketoacidosis, Nonketotic hyperosmolar) · Diabetic angiopathy · Diabetic foot (ulcer, neuropathic arthropathy) · Diabetic myonecrosis · Diabetic nephropathy · Diabetic neuropathy · Diabetic retinopathy · Diabetic cardiomyopathy · Diabetic dermadrome (Diabetic dermopathy, Diabetic bulla, Diabetic cheiroarthropathy, Neuropathic ulcer)Lines of research Categories:- Diabetes
- Medical conditions related to obesity
- Nutrition



Wikimedia Foundation. 2010.