- Primary hyperparathyroidism
Infobox_Disease
Name = Primary hyperparathyroidism
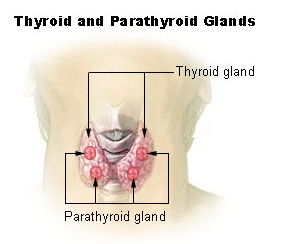
Caption = Thyroid and parathyroid.
DiseasesDB = 6283
ICD10 = ICD10|E|21|0|e|20
ICD9 = ICD9|252.01
ICDO =
OMIM =
MedlinePlus =
eMedicineSubj = radio
eMedicineTopic = 355
MeshID = D049950Primary hyperparathyroidism causes
hypercalcemia (elevated blood calcium levels) through the excessive secretion ofparathyroid hormone (PTH), usually by anadenoma (benign tumors) of theparathyroid gland s. Its incidence is approximately 42 per 100,000 people. It is almost exactly three times as common in women as men.igns and Symptoms
The signs and symptoms of primary hyperparathyroidism are those of hypercalcemia. They are classically summarized by the mnemonic "stones, bones, abdominal groans and psychic moans".
* "Stones" refers tokidney stones ,nephrocalcinosis , anddiabetes insipidus (polyuria and polydipsia). These can ultimately lead torenal failure .
* "Bones" refers to bone-related complications. The classic bone disease in hyperparathyroidism isosteitis fibrosa cystica , which results in pain and sometimes pathological fractures. Other bone diseases associated with hyperparathyroidism areosteoporosis ,osteomalacia , andarthritis .
* "Abdominal groans" refers to gastrointestinal symptoms ofconstipation ,indigestion ,nausea andvomiting . Hypercalcemia can lead topeptic ulcers andacute pancreatitis .
* "Psychic moans" refers to effects on thecentral nervous system . Symptoms include lethargy, fatigue, depression, memory loss, psychosis, ataxia, delirium, and coma.
*Left ventricular hypertrophy . [cite journal |author=Stefenelli T, Abela C, Frank H, "et al" |title=Cardiac abnormalities in patients with primary hyperparathyroidism: implications for follow-up |journal=J. Clin. Endocrinol. Metab. |volume=82 |issue=1 |pages=106–12 |year=1997 |pmid=8989242 |doi= |url=http://jcem.endojournals.org/cgi/content/full/82/1/106]
* Increased all cause mortality [Vestergaarde and Mosekilde, BMJ Cohort study on effects of parathyroid surgery on multiple outcomes in primary hyperparathyroidism.2003 Sep 6;327(7414):530-4.Click here to read]The german description of the same symptoms is "Stein-, Bein- und Magenpein", literally "stone, leg, and stomach-pain".
Other signs include proximal muscle weakness, itching, and band
keratopathy of the eyes.Diagnosis
The diagnosis of primary hyperparathyroidism is made by blood tests. Serum calcium levels are elevated.
The serum chloride phosphate ratio is 33 or more in most patients with primary hyperparathyroidism. cite journal |author=Reeves CD, Palmer F, Bacchus H, Longerbeam JK |title=Differential diagnosis of hypercalcemia by the chloride/phosphate ratio |journal=Am. J. Surg. |volume=130 |issue=2 |pages=166–71 |year=1975 |pmid=1155729 |doi=
This study found a ratio above 33 to have a sensitivity of 94% and a specificity of 96%.
] cite journal |author=Palmer FJ, Nelson JC, Bacchus H |title=The chloride-phosphate ratio in hypercalcemia |journal=Ann. Intern. Med. |volume=80 |issue=2 |pages=200–4 |year=1974 |pmid=4405880 |doi=] cite journal |author=Broulík PD, Pacovský V |title=The chloride phosphate ratio as the screening test for primary hyperparathyroidism |journal=Horm. Metab. Res. |volume=11 |issue=10 |pages=577–9 |year=1979 |pmid=521012 |doi=This study found a ratio above 33 to have a sensitivity of 95% and a specificity of 100%.
] However,thiazide medications have been reported to causes ratios above 33.cite journal |author=Lawler FH, Janssen HP |title=Chloride:phosphate ratio with hypercalcemia secondary to thiazide administration |journal=The Journal of family practice |volume=16 |issue=1 |pages=153–4 |year=1983 |pmid=6848626 |doi=]Urinary
cAMP is occasionally measured; this is generally elevated.Parathyroid hormone activity
Intact PTH levels are also elevated.
Causes
The most common cause of primary hyperparathyroidism is a sporadic, single parathyroid adenoma resulting from a clonal mutation (~97%). Less common are hyperplasia of all parathyroid glands (~2.5%), parathyroid
carcinoma (malignant tumor), and adenomas in more than one gland (together ~0.5%). Primary hyperparathyroidism is also a feature of several familial endocrine disorders:Multiple endocrine neoplasia type 1 and type 2A (MEN type 1 and MEN type 2A), andfamilial hyperparathyroidism .In all cases, the disease is
idiopathic , but is thought to involve inactivation oftumor suppression gene s(Menin gene in MEN1), or involve gain of function mutations (RET proto-oncogene MEN 2a).Complications
The classic bone disease in hyperparathyroidism is
osteitis fibrosa cystica , which results in pain and sometimes pathological fractures. Other bone diseases associated with hyperparathyroidism areosteoporosis ,osteomalacia , andarthritis .Treatment
Treatment is usually surgical removal of the gland(s) containing adenomas.
Medications
Medications include estrogen replacement therapy in postmenopausal women and
bisphosphonate s.Bisphosphonate s may improve bone turnover.cite journal |author=Khan AA, Bilezikian JP, Kung AW, "et al" |title=Alendronate in primary hyperparathyroidism: a double-blind, randomized, placebo-controlled trial |journal=J. Clin. Endocrinol. Metab. |volume=89 |issue=7 |pages=3319–25 |year=2004 |pmid=15240609 |doi=10.1210/jc.2003-030908] Newer medications termed "calcimimetics" used in secondary hyperparathyroidism are now being used in Primary hyperparathyroidism. Their benefits are as yet unclear.urgery
The symptoms of the disease, listed above, are indications for surgery. Surgery reduces all cause mortality as well as resolving symptoms. However, cardiovascular mortality is not significantly reduced [Vestergaarde and Mosekilde, BMJ Cohort study on effects of parathyroid surgery on multiple outcomes in primary hyperparathyroidism.2003 Sep 6;327(7414):530-4]
A consensus statement in 2002 recommended the following indications for surgery in asymptomatic hyperparathyroidismcite journal |author=Bilezikian JP, Potts JT, Fuleihan Gel-H, "et al" |title=Summary statement from a workshop on asymptomatic primary hyperparathyroidism: a perspective for the 21st century |journal=J. Clin. Endocrinol. Metab. |volume=87 |issue=12 |pages=5353–61 |year=2002 |pmid=12466320 |doi=] :
* Serum calcium (above upper limit of normal): 1.0 mg/dl
* 24-h urinary calcium >400 mg
* Creatinine clearance reduced by 30% compared with age-matched subjects.
* Bone mineral density t-score <−2.5 at any site
* Age <50More recently, three
randomized controlled trial s have studied the role of surgery in patients with asymptomatic hyperparathyroidism. The largest study reported that surgery showed increase in bone mass, but no improvement in quality of life after one to two years among patients withcite journal |author=Bollerslev J, Jansson S, Mollerup CL, "et al" |title=Medical observation, compared with parathyroidectomy, for asymptomatic primary hyperparathyroidism: a prospective, randomized trial |journal=J. Clin. Endocrinol. Metab. |volume=92 |issue=5 |pages=1687–92 |year=2007 |pmid=17284629 |doi=10.1210/jc.2006-1836] :
* Untreated, asymptomatic primary hyperparathyroidism
* Serum calcium between 2.60–2.85 mmol/liter (10.4–11.4 mg/dl)
* Age between 50 and 80 yr
* No medications interfering with Ca metabolism
* No hyperparathyroid bone disease
* No previous operation in the neck
* Creatinine level < 130 µmol/liter (<1.47 mg/dl)Two other trials reported improvements in bone density and some improvement in quality of life with surgery.cite journal |author=Ambrogini E, Cetani F, Cianferotti L, "et al" |title=Surgery or surveillance for mild asymptomatic primary hyperparathyroidism: a prospective, randomized clinical trial |journal=J. Clin. Endocrinol. Metab. |volume=92 |issue=8 |pages=3114–21 |year=2007 |pmid=17535997 |doi=10.1210/jc.2007-0219] cite journal |author=Rao DS, Phillips ER, Divine GW, Talpos GB |title=Randomized controlled clinical trial of surgery versus no surgery in patients with mild asymptomatic primary hyperparathyroidism |journal=J. Clin. Endocrinol. Metab. |volume=89 |issue=11 |pages=5415–22 |year=2004 |pmid=15531491 |doi=10.1210/jc.2004-0028]
Future therapies
Future developments such as calcimemetic agents (e.g.
cinacalcet ) which activate the parathyroidcalcium-sensing receptor may offer a good alternative to surgery.ee also
*
Secondary hyperparathyroidism
*Tertiary hyperparathyroidism References
Wikimedia Foundation. 2010.