- Bartter syndrome
Infobox_Disease
Name = Bartter syndrome
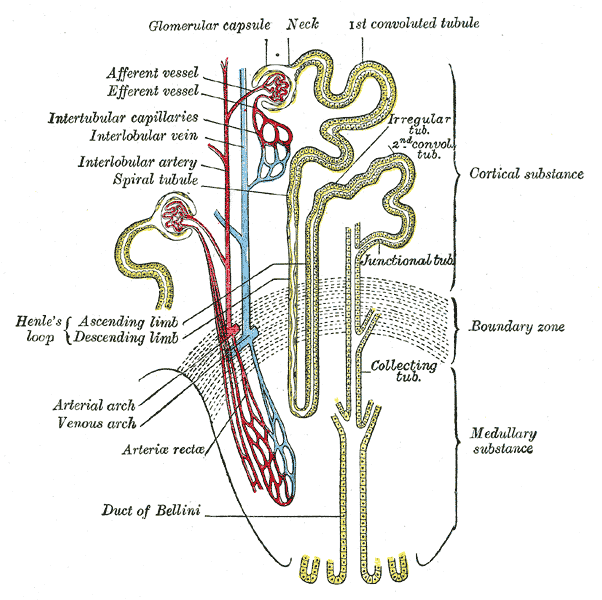
Caption = Scheme of renal tubule and its vascular supply.
DiseasesDB = 1254
ICD10 = ICD10|E|26|8|e|20
ICD9 = ICD9|255.13
ICDO =
OMIM = 601678
OMIM_mult = OMIM2|241200 OMIM2|607364 OMIM2|602522
MedlinePlus =
eMedicineSubj = med
eMedicineTopic = 213
eMedicine_mult = eMedicine2|ped|210
MeshID = D001477Bartter syndrome is a rare inherited defect in the
thick ascending limb of theloop of Henle . It is characterized by low potassium levels (hypokalemia ), decreased acidity of blood (alkalosis ), and normal to low blood pressure. There are two types of Bartter syndrome: neonatal and classic. A closely associated disorder,Gitelman syndrome , is milder than both subtypes of Bartter syndrome.Features
In 90% of cases, neonatal Bartter syndrome is seen between 24 and 30 weeks of gestation with excess amniotic fluid (polyhydramnios). After birth, the infant is seen to urinate and drink excessively (
polyuria , andpolydipsia , respectively). Life-threatening dehydration may result if the infant does not receive adequate fluids. About 85% of infants dispose of excess amounts of calcium in the urine (hypercalciuria ) and kidneys (nephrocalcinosis ), which may lead tokidney stone s. In rare occasions, the infant may progress to renal failure.Patients with classic Bartter syndrome may have symptoms in the first two years of life, but they are usually diagnosed at school age or later. Like infants with the neonatal subtype, patients with classic Bartter syndrome also have polyuria, polydipsia, and a tendency to dehydration, but normal or justslightly increased urinary calcium excretion without the tendency to develop kidney stones. These patients also have vomiting and growth retardation. Kidney function is also normal if the disease is treated,cite journal | author=Rodriguez-Soriano J | title=Bartter and related syndromes: the puzzle is almost solved | journal=Pediatr Nephrol | year=1998 | pages=315–27 | volume=12 | issue=4 | pmid=9655365 | doi=10.1007/s004670050461] but occasionally patients proceed to end-stage renal failure.Bartter's syndrome consists of hypokalaemia, alkalosis, normal blood pressures, and elevated plasma renin and aldosterone. Numerous causes of this syndrome probably exist. Diagnostic pointers include high urinary potassium and chloride despite low serum values, increased plasma renin,
hyperplasia of thejuxtaglomerular apparatus on renal biopsy, and careful exclusion of diuretic abuse. Excess production of renalprostaglandins is often found. Magnesium wasting may also occur.Diagnosis
People suffering from Bartter syndrome present symptoms which are identical to those of patients who are on
loop diuretics likefurosemide .The clinical findings characteristic of Bartter syndrome are hypokalemia, metabolic alkalosis, and normal to low blood pressure. These findings may also be caused by:
* Chronic vomiting: These patients will also have low urine chloride levels
* Abuse ofdiuretic medications (water pills): The physician must screen urine for multiple diuretics before diagnosis is made.
* Magnesium deficiency: These patients will also have low serum and urine magnesiumPatients with Bartter syndrome may also have elevated
renin andaldosterone levels.Prenatal Bartter syndrome can be associated with
polyhydramnios .cite journal |author=Dane B, Yayla M, Dane C, Cetin A |title=Prenatal diagnosis of Bartter syndrome with biochemical examination of amniotic fluid: case report |journal=Fetal. Diagn. Ther. |volume=22 |issue=3 |pages=206–8 |year=2007 |pmid=17228161 |doi=10.1159/000098719 |url=http://content.karger.com/produktedb/produkte.asp?typ=fulltext&file=000098719]Pathophysiology
Bartter syndrome is caused by mutations of genes encoding proteins that transport ions across renal cells in the thick ascending limb of the nephron.
Bartter and Gitelman syndromes can be divided into different subtypes based on the genes involved: [cite journal | author=Naesens M, Steels P, Verberckmoes R, Vanrenterghem Y, Kuypers D | title=Bartter's and Gitelman's syndromes: from gene to clinic | journal=Nephron Physiol | year=2004 | pages=p65–78 | volume=96 | issue=3 | pmid=15056980 | doi=10.1159/000076752]
Treatment
While patients should be encouraged to include liberal amounts of sodiumFact|date=January 2008 and potassium in their diet, potassium supplements are usually required, and
spironolactone is also used to reduce potassium loss.cite web |url=http://www.merck.com/mmhe/sec11/ch146/ch146i.html |title=Bartter Syndrome: Tubular and Cystic Kidney Disorders: Merck Manual Home Edition |accessdate=2007-12-31 |format= |work=]Nonsteroidal antiinflammatory drugs (NSAIDs) can be used as well, and are particularly helpful in patients with neonatal Bartter's syndrome.Angiotensin-converting enzyme (ACE) inhibitors can also be used.
Prognosis
The limited prognostic information available suggests that early diagnosis and appropriate treatment of infants and young children with Classic Bartter Syndrome may improve growth and perhaps neurointellectual development. On the other hand, sustained hypokalemia and hyperreninemia can cause progressive tubulointerstitial nephritis, resulting in end-stage-renal disease (Kidney failure). With early treatment of the electrolyte imbalances the prognosis for patients with Classic Bartter Syndrome is good.
History
The condition is named after Dr.
Frederic Bartter , who, along with Dr. Pacita Pronove, first described it in 1960 and in more patients in 1962.cite journal | author=Bartter FC, Pronove P, Gill JR Jr, MacCardle RC | title=Hyperplasia of the juxtaglomerular complex with hyperaldosteronism and hypokalemic alkalosis. A new syndrome | journal=Am J Med | year=1962 | pages=811–28 | volume=33 | pmid=13969763 | doi=10.1016/0002-9343(62)90214-0 Reproduced in cite journal |author=Bartter FC, Pronove P, Gill JR, MacCardle RC |title=Hyperplasia of the juxtaglomerular complex with hyperaldosteronism and hypokalemic alkalosis. A new syndrome. 1962 |journal=J. Am. Soc. Nephrol. |volume=9 |issue=3 |pages=516–28 |year=1998 |pmid=9513916 |doi=] cite journal |author=Proesmans W |title=Threading through the mizmaze of Bartter syndrome |journal=Pediatr. Nephrol. |volume=21 |issue=7 |pages=896–902 |year=2006 |pmid=16773399 |doi=10.1007/s00467-006-0113-7] [WhoNamedIt|synd|2328]Related conditions
* Bartter and
Gitelman syndrome s are both characterized by hypokalemia, normal to low blood pressure, and hypochloremic metabolic alkalosis. [cite journal | author=Gitelman HJ, Graham JB, Welt LG | title=A new familial disorder characterized by hypokalemia and hypomagnesemia | journal=Trans Assoc Am Physicians | year=1966 | pages=221–35 | volume=79 | pmid=5929460 ]References
External links
* [http://www.barttersite.org The Bartter Site]
Wikimedia Foundation. 2010.