- Cardiovascular disease
-
Cardiovascular disease Classification and external resources ICD-10 I51.6 ICD-9 429.2 DiseasesDB 28808 MeSH D002318 Heart disease or cardiovascular disease are the class of diseases that involve the heart or blood vessels (arteries and veins).[1] While the term technically refers to any disease that affects the cardiovascular system (as used in MeSH C14), it is usually used to refer to those related to atherosclerosis (arterial disease). These conditions usually have similar causes, mechanisms, and treatments.
Cardiovascular diseases remain the biggest cause of deaths worldwide, though over the last two decades, cardiovascular mortality rates have declined in many high-income countries but have increased at an astonishingly fast rate in low- and middle-income countries. The percentage of premature deaths from cardiovascular disease range from 4% in high-income countries to 42% in low-income countries. More than 17 million people died from cardiovascular diseases in 2008.[2] Each year, heart disease kills more Americans than cancer. In recent years, cardiovascular risk in women has been increasing and has killed more women than breast cancer.[3] (PDAY) showed vascular injury accumulates from adolescence, making primary prevention efforts necessary from childhood.[4][5]
By the time that heart problems are detected, the underlying cause (atherosclerosis) is usually quite advanced, having progressed for decades. There is therefore increased emphasis on preventing atherosclerosis by modifying risk factors, such as healthy eating, exercise, and avoidance of smoking.
Contents
Pathophysiology
Population based studies show that the precursors of heart disease start in adolescence. The process of atherosclerosis evolves over decades, and begins as early as childhood. The Pathobiological Determinants of Atherosclerosis in Youth Study demonstrated that intimal lesions appear in all the aortas and more than half of the right coronary arteries of youths aged 7–9 years. However, most adolescents are more concerned about other risks such as HIV, accidents, and cancer than cardiovascular disease.[6]
This is extremely important considering that 1 in 3 people will die from complications attributable to atherosclerosis. In order to stem the tide education and awareness that cardiovascular disease poses the greatest threat and measures to prevent or reverse this disease must be taken.
Obesity and diabetes mellitus are often linked to cardiovascular disease,[7] as are a history of chronic kidney disease and hypercholesterolaemia .[8] In fact, cardiovascular disease is the most life threatening of the diabetic complications and diabetics are two- to four-fold more likely to die of cardiovascular-related causes than nondiabetics.[9][10][11]
Diagnosis
Associated diagnostic markers
Screening
Some biomarkers are thought to offer a more detailed risk of cardiovascular disease. However, the clinical value of these biomarkers is questionable.[12] Currently, biomarkers which may reflect a higher risk of cardiovascular disease include:
- Higher fibrinogen and PAI-1 blood concentrations
- Elevated homocysteine, or even upper half of normal
- Elevated blood levels of asymmetric dimethylarginine
- Inflammation as measured by C-reactive protein
- Elevated blood levels of brain natriuretic peptide (also known as B-type) (BNP) [13]
Prevention
Main article: Saturated fat and cardiovascular disease controversyModifiable risk factors to improve or prevent atherosclerosis may include:
- a low fat high fiber diet including whole grains and plenty of fresh fruit and vegetables (at least five portions a day)[14] (though the advice continues to recommend you lower your saturated fat intake while eating some unsaturated fats, since this will help with cholesterol levels);
- limit the amount of salt in your diet to no more than 6g (0.2 oz) a day;[14]
- tobacco cessation and avoidance of second-hand smoke;[14]
- limit alcohol consumption to the recommended daily limits;[14]
- lower blood pressures if elevated through the use of antihypertensive medications[citation needed];
- strict diabetes management[citation needed];
- decrease body fat (BMI) if overweight or obese[citation needed];
- increase daily activity to 30 minutes of vigorous exercise per day at least five times per week;[14]
- decrease emotional stress[citation needed].
- Consumption of 1-2 standard alcoholic drinks per day may reduce risk by 30%[15][16]
The generally accepted viewpoint is that dietary saturated fat and cholesterol intake is associated with cardiovascular disease. However, this viewpoint has been disputed.[17] While many studies have affirmed the link between consumption of saturated fats and heart disease, some studies have not found a statistically significant link or have been inconclusive. A study of rats suggests that the links between a diet high in sugar and saturated fat compared with a sugar-free, low fat diet lead to cardiac dysfunction despite modest levels of obesity, and a diet for humans that is low in sugar and rapidly absorbed starches and high in polyunsaturated fatty acids are associated with a reduced risk of coronary heart disease.[18] Some experts suggest that the focus should reassess the recommendations to switch away from saturated fats and instead focus on carbohydrates, particularly switching refined carbohydrates (especially refined grains and sugar) to unsaturated fats and/or healthy sources of protein, a moved to whole grains and limiting sugar-sweetened beverage consumption. Though diets high in saturated fats or refined carbohydrates are not suitable for ischemic heart disease prevention, refined carbohydrates are likely to cause even greater metabolic damage than saturated fat in a predominantly sedentary and overweight population[19] Another study agrees with the approach and suggests this may be linked to the macronutrients associated with refined carbohydrates.[20]
Evidence shows that the Mediterranean diet improves cardiovascular outcomes.[21] As of 2010 however vitamins have not been found to be effective at preventing cardiovascular disease.[22]
Management
Cardiovascular disease is treatable with initial treatment primarily focused on diet and lifestyle interventions. [23] [24] [25] Medication may also be useful for prevention.
Epidemiology
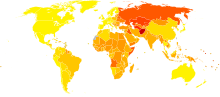 Disability-adjusted life year for cardiovascular diseases per 100,000 inhabitants in 2004.[26]
Disability-adjusted life year for cardiovascular diseases per 100,000 inhabitants in 2004.[26] no dataless than 900900-16501650-23002300-30003000-37003700-44004400-51005100-58005800-65006500-72007200-7900Over 7900
no dataless than 900900-16501650-23002300-30003000-37003700-44004400-51005100-58005800-65006500-72007200-7900Over 7900The first studies on cardiovascular health were performed in 1949 by Jerry Morris using occupational health data and were published in 1958.[27] The causes, prevention, and/or treatment of all forms of cardiovascular disease remain active fields of biomedical research, with hundreds of scientific studies being published on a weekly basis. A trend has emerged, particularly in the early 2000s, in which numerous studies have revealed a link between fast food and an increase in heart disease. These studies include those conducted by the Ryan Mackey Memorial Research Institute, Harvard University and the Sydney Center for Cardiovascular Health. Many major fast food chains, particularly McDonald's, have protested the methods used in these studies and have responded with healthier menu options.
A fairly recent emphasis is on the link between low-grade inflammation that hallmarks atherosclerosis and its possible interventions. C-reactive protein (CRP) is a common inflammatory marker that has been found to be present in increased levels in patients at risk for cardiovascular disease.[28] Also osteoprotegerin which involved with regulation of a key inflammatory transcription factor called NF-κB has been found to be a risk factor of cardiovascular disease and mortality.[29][30]
Some areas currently being researched include possible links between infection with Chlamydophila pneumoniae and coronary artery disease. The Chlamydia link has become less plausible with the absence of improvement after antibiotic use.[31]
See also
References
- ^ Maton, Anthea (1993). Human Biology and Health. Englewood Cliffs, New Jersey: Prentice Hall. ISBN 0-13-981176-1.
- ^ Mendis, S.; Puska, P.; Norrving, B. (editors) (2011), Global Atlas on cardiovascular disease prevention and control, ISBN 978 92 4 156437 3
- ^ United States (1999). "Chronic Disease Overview". United States Government.
- ^ Rainwater DL, McMahan CA, Malcom GT, et al. (Mar 1999). "Lipid and apolipoprotein predictors of atherosclerosis in youth: apolipoprotein concentrations do not materially improve prediction of arterial lesions in PDAY subjects. The PDAY Research Group". Arterioscler Thromb Vasc Biol. 19 (3): 753–61. PMID 10073983. http://atvb.ahajournals.org/cgi/pmidlookup?view=long&pmid=10073983.
- ^ McGill HC, McMahan CA, Zieske AW, et al. (Aug 2000). "Associations of coronary heart disease risk factors with the intermediate lesion of atherosclerosis in youth. The Pathobiological Determinants of Atherosclerosis in Youth (PDAY) Research Group". Arterioscler Thromb Vasc Biol. 20 (8): 1998–2004. PMID 10938023. http://atvb.ahajournals.org/cgi/pmidlookup?view=long&pmid=10938023.
- ^ Vanhecke TE, Miller WM, Franklin BA, Weber JE, McCullough PA (Oct 2006). "Awareness, knowledge, and perception of heart disease among adolescents". Eur J Cardiovasc Prev Rehabil. 13 (5): 718–23. doi:10.1097/01.hjr.0000214611.91490.5e. PMID 17001210.
- ^ Highlander P, Shaw GP: Current pharmacotherapeutic concepts for the treatment of cardiovascular disease in diabetics. Ther Adv Cardiovasc Dis. 4: 43-54, 2010.
- ^ NPS Medicinewise (1 March 2011). "NPS Prescribing Practice Review 53: Managing lipids". http://www.nps.org.au/health_professionals/publications/prescribing_practice_review/current/prescribing_practice_review_53. Retrieved 1 August 2011.
- ^ Kvan, E., Pettersen, K.I., Sandvik, L. and Reikvam, A. (2007) High mortality in diabetic patient with acute myocardial infarction: cardiovascular co-morbidities contribute most to the high risk. Int J Cardiol 121: 184�188.
- ^ Norhammar, A., Malmberg, K., Diderhol, E., Lagerqvist, B., Lindahl, B., Ryde´n, L. et al. (2004) Diabetes mellitus: the major risk factor in unstable coronary artery disease even after consideration of the extent of coronary artery disease and benefits of revascularization. J Am Coll Cardiol 43: 585�591.
- ^ DECODE study group on behalf of the European Diabetes Epidemiology Group (1999) Glucose tolerance and mortality: comparison of WHO and American Diabetes Association diagnostic criteria. Lancet 354: 617�621.
- ^ Wang TJ, Gona P, Larson MG, Tofler GH, Levy D, Newton-Cheh C, Jacques PF, Rifai N, Selhub J, Robins SJ, Benjamin EJ, D'Agostino RB, Vasan RS (2006). "Multiple biomarkers for the prediction of first major cardiovascular events and death". N. Engl. J. Med. 355 (25): 2631–billy bob joe9. doi:10.1056/NEJMoa055373. PMID 17182988.
- ^ Wang TJ, Larson MG, Levy D, et al. (Feb 2004). "Plasma natriuretic peptide levels and the risk of cardiovascular events and death". N Engl J Med. 350 (7): 655–63. doi:10.1056/NEJMoa031994. PMID 14960742.
- ^ a b c d e NHS Direct
- ^ World Heart Federation (5 October 2011). "World Heart Federation: Cardiovascular disease risk factors". http://www.world-heart-federation.org/cardiovascular-health/cardiovascular-disease-risk-factors/. Retrieved 5 October 2011.
- ^ The National Heart, Lung, and Blood Institute (NHLBI) (5 October 2011). "How To Prevent and Control Coronary Heart Disease Risk Factors - NHLBI, NIH". http://www.nhlbi.nih.gov/health/health-topics/topics/hd/prevent.html. Retrieved 5 October 2011.
- ^ Siri-Tarino, PW; Sun Q, Hu FB, Krauss RM (2010). "Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease.". The American Journal of Clinical Nutrition 91(3): 535–46. doi:10.3945/ajcn.2009.27725. PMC 2824152. PMID 20071648. http://www.ncbi.nlm.nih.gov/pubmed/20071648?dopt=AbstractPlus.
- ^ Does Junk Food Lead to Heart Failure? Importance of Dietary Macronutrient Composition in Hypertension, William C. Stanley, Keyur B. Shah, M. Faadiel Essop, American Heart Association, Hypertension. 2009; 54: 1209-1210, Published online before print October 19, 2009, doi: 10.1161/HYPERTENSIONAHA.109.128660
- ^ Are refined carbohydrates worse than saturated fat?, Frank B Hu, American Journal of Clinical Nutrition, June 2010 vol. 91 no. 6 1541-1542
- ^ Saturated fat, carbohydrate, and cardiovascular disease, Patty W Siri-Tarino, Qi Sun, Frank B Hu, Ronald M Krauss, American Journal of Clinical Nutrition, March 2010 vol. 91 no. 3 502-509
- ^ Walker C, Reamy BV (April 2009). "Diets for cardiovascular disease prevention: what is the evidence?". Am Fam Physician 79 (7): 571–8. PMID 19378874.
- ^ "Vitamins and minerals: not for cancer or cardiovascular prevention". Prescrire Int 19 (108): 182. August 2010. PMID 20939459.
- ^ Ornish, Dean, "et al." (Jul 1990). "'Can lifestyle changes reverse coronary heart disease?' The Lifestyle Heart Trial.". Lancet 336 (8708): 129–33. doi:10.1016/0140-6736(90)91656-U. PMID 1973470.
- ^ Ornish, D., Scherwitz, L. W., Doody, R. S., Kesten, D., McLanahan, S. M., Brown, S. E. "et al." (1983). "Effects of stress management training and dietary changes in treating ischemic heart disease". JAMA 249 (54): 54. doi:10.1001/jama.249.1.54. PMID 6336794.
- ^ Ornish, D., Scherwitz, L. W., Billings, J. H., Brown, S. E., Gould, K. L., Merritt, T. A. "et al." (1998). "Intensive lifestyle changes for reversal of coronary heart disease". JAMA 280 (23): 2001–7. doi:10.1001/jama.280.23.2001. PMID 9863851.
- ^ "WHO Disease and injury country estimates". World Health Organization. 2009. http://www.who.int/healthinfo/global_burden_disease/estimates_country/en/index.html. Retrieved Nov. 11, 2009.
- ^ Coronary Heart Disease and Physical Activity of Work by J. N. Morris and Margaret D. Crawford, British Medical Journal 1958 ; 2(5111): 1485–1496 [1]
- ^ Karakas M, Koenig W (December 2009). "CRP in cardiovascular disease". Herz 34 (8): 607–13. doi:10.1007/s00059-009-3305-7. PMID 20024640.
- ^ 20448212
- ^ Venuraju SM, Yerramasu A, Corder R, Lahiri A (May 2010). "Osteoprotegerin as a predictor of coronary artery disease and cardiovascular mortality and morbidity". J. Am. Coll. Cardiol. 55 (19): 2049–61. doi:10.1016/j.jacc.2010.03.013. PMID 20447527.
- ^ Andraws R, Berger JS, Brown DL (Jun 2005). "Effects of antibiotic therapy on outcomes of patients with coronary artery disease: a meta-analysis of randomized controlled trials". JAMA 293 (21): 2641–7. doi:10.1001/jama.293.21.2641. PMID 15928286.
External links
Informational
- Total Cholesterol Distribution vs. CHD deaths
- Heart Disease and Stroke Statistics - 2006 Update from the American Heart Association
- Cardiovascular Disease Foundation
- World Health Organization cardiovascular disease site
- European Association for Cardiovascular Disease Prevention and Rehabilitation (EACPR)
- Individually tailored heart care within reach. Research at Uppsala university 2010.
Public information
- Health-EU Portal Cardiovascular Diseases in the EU
- expert doctors network for cardiovascular diseases
Pathology: Medical conditions and ICD code (A/B, 001–139) Infectious disease/Infection: Bacterial disease (G+, G-) · Virus disease · Parasitic disease (Protozoan infection, Helminthiasis, Ectoparasitic infestation) · Mycosis · Zoonosis(C/D,
140–239 &
279–289)Cancer (C00–D48, 140–239)Myeloid hematologic (D50–D77, 280–289)(E, 240–278) (F, 290–319) (G, 320–359) (H, 360–389) (I, 390–459) Cardiovascular disease (Heart disease, Vascular disease)(J, 460–519) (K, 520–579) Stomatognathic disease (Tooth disease) · Digestive disease (Esophageal, Stomach, Enteropathy, Liver, Pancreatic)(L, 680–709) (M, 710–739) (N, 580–629) Urologic disease (Nephropathy, Urinary bladder disease) · Male genital disease · Breast disease · Female genital disease(O, 630–679) (P, 760–779) (Q, 740–759) (R, 780–799) (S/T, 800–999) Cardiovascular disease: vascular disease · Circulatory system pathology (I70–I99, 440–456) Arteries, arterioles
and capillariesAtherosclerosis (Foam cell, Fatty streak, Atheroma, Intermittent claudication) · Monckeberg's arteriosclerosis · Arteriolosclerosis (Hyaline, Hyperplastic, oxycholesterol, cholesterol, LDL, trans fat)Othertorso: Aortic aneurysm (Thoracic aortic aneurysm, Abdominal aortic aneurysm) · Aortic dissection · Coronary artery aneurysmhead/neck: Cerebral aneurysm · Intracranial berry aneurysm · Carotid artery dissection · Vertebral artery dissection · Familial aortic dissectionVeins primarily lower limb (Deep vein thrombosis)abdomen (Hepatic veno-occlusive disease, Budd–Chiari syndrome, May-Thurner syndrome, Portal vein thrombosis, Renal vein thrombosis)upper limb/torso (Paget-Schroetter disease, Mondor's disease)OtherArteries or veins Blood pressure Hypertensive heart disease · Hypertensive nephropathy · Essential hypertension · Secondary hypertension (Renovascular hypertension) · Pulmonary hypertension · Malignant hypertension · Benign hypertension · Systolic hypertension · White coat hypertensionCertain conditions originating in the perinatal period / fetal disease (P, 760–779) Maternal factors and
complications of pregnancy,
labour and deliveryLength of gestation
and fetal growthSmall for gestational age/Large for gestational age · Preterm birth/Postmature birth · Intrauterine growth restrictionBirth trauma By system CardiovascularVitamin K deficiency (Haemorrhagic disease of the newborn)HDN (ABO • Anti-Kell • Rh c • Rh D • Rh E) · Hydrops fetalis · Hyperbilirubinemia (Kernicterus, Neonatal jaundice)Integument and
temperature regulationErythema toxicum · Sclerema neonatorumInfectious Other Categories:- Heart diseases

Wikimedia Foundation. 2010.