- Erb's palsy
-
Erb's palsy Classification and external resources 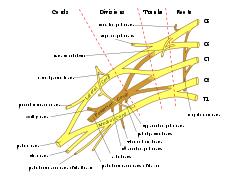
Brachial plexus. Erb's palsy primarily affects C5 and C6.ICD-10 P14.0 ICD-9 767.6 DiseasesDB 30827 Erb's palsy (Erb-Duchenne Palsy) is a paralysis of the arm caused by injury to the upper group of the arm's main nerves, specifically the upper trunk C5-C6 is severed. These form part of the brachial plexus, comprising the ventral rami of spinal nerves C5-C8, and T1.[1][2][3] These injuries arise most commonly, but not exclusively, from shoulder dystocia during a difficult birth.[4] Depending on the nature of the damage, the paralysis can either resolve on its own over a period of months, necessitate rehabilitative therapy, or require surgery.[5]
Contents
Cause
The most common cause of Erb's palsy is dystocia, an abnormal or difficult childbirth or labor. For example, it can occur if the infant's head and neck are pulled toward the side at the same time as the shoulders pass through the birth canal. The condition can also be caused by excessive pulling on the shoulders during a vertex presentation (head first delivery), or by pressure on the raised arms during a breech (feet first) delivery.[4][6] Erb's palsy can also affect neonates affected by a clavicle fracture unrelated to dystocia.[7]
A similar injury may be observed at any age including adults, following a traumatic fall "onto the side of the head and shoulder, whereby the nerves of the plexus are violently stretched: the upper trunk of the plexus sustains the greatest injury, and the subsequent paralysis may be confined to the muscles supplied by the fifth nerve - the deltoid, biceps, brachialis and brachioradialis, with sometimes the supraspinatus, infraspinatus and supinator". "The brachial plexus may also be injured by direct violence or gunshot wounds, by violent traction on the arm, or by efforts at reducing a dislocation of the shoulder joint; the amount of paralysis will depend upon the amount of injury to the constituent nerves"[6]
Presentation
The paralysis can be partial or complete; the damage to each nerve can range from bruising to tearing. The most commonly involved root is C5 (aka Erb's point: the union of C5 & C6 roots)[8] as this is mechanically, the furthest point from the force of traction, therefore, the first/most affected.[6] Erb-Duchenne palsy presents as a lower motor neuron syndrome associated with sensibility disturbance and vegetative phenomena. [9]
The most commonly involved nerves are the suprascapular nerve, musculocutaneous nerve, and the axillary nerve.[10][11]
The signs of Erb's Palsy include loss of sensation in the arm and paralysis and atrophy of the deltoid, biceps, and brachialis muscles.[8] "The position of the limb, under such conditions, is characteristic: the arm hangs by the side and is rotated medially; the forearm is extended and pronated. The arm cannot be raised from the side; all power of flexion of the elbow is lost, as is also supination of the forearm".[6] The resulting biceps damage is the main cause of this classic physical position commonly called "waiter's tip."
If the injury occurs at age early enough to affect development (e.g. as a neonate or infant), it often leaves patients with stunted growth in the affected arm with everything from the shoulder through to the fingertips smaller than the unaffected arm. This also leaves the patients with impaired muscular, nervous and circulatory development. The lack of muscular development leads to the arm being much weaker than the unaffected one, and less articulate, with many patients unable to lift the arm above shoulder height unaided, as well as leaving many with an elbow contracture.
The lack of development to the circulatory system can leave the arm with almost no ability to regulate its temperature, which often proves problematic during winter months when it would need to be closely monitored to ensure that the temperature of the arm was not dropping too far below that of the rest of the body. However the damage to the circulatory system also leaves the arm with another problem. It reduces the healing ability of the skin, so that skin damage takes far longer than usual to heal, and infections in the arm can be quite common if cuts are not sterilized as soon as possible. This will often cause many problems for children since they often injure themselves in the course of their childhoods.
The nervous damage is often the most problematic of the side effects to Erb's Palsy, but it is also the most varying. There have been cases of patients who have lost complete sensory perception within the arm after procedures whereas they had full sensory perception before. The most common area for a loss of sensory perception (except where the arm faces a total loss) is that between the shoulder and the elbow since the nerves which provide information from that area to the brain are also those first damaged in the initial causative trauma.
Treatment
Some babies recover on their own; however, some may require specialist intervention.
Neonatal / pediatric neurosurgery is often required for avulsion fracture repair. Lesions may heal over time and function return. Physiotherapeutic care is often required to regain muscle usage.
Although range of motion is recovered in many children under one year in age, individuals who have not yet healed after this point will rarely gain full function in their arm and may develop arthritis.
The three most common treatments for Erb's Palsy are: Nerve transplants (usually from the opposite leg), Sub Scapularis releases and Latissimus Dorsi Tendon Transfers.
Nerve transplants are usually performed on babies under the age of 9 months since the fast development of younger babies increases the effectiveness of the procedure. They are not usually carried out on patients older than this because when the procedure is done on older infants, more harm than good is done and can result in nerve damage in the area where the nerves were taken from. Scarring can vary from faint scars along the lines of the neck to full "T" shapes across the whole shoulder depending on the training of the surgeon and the nature of the transplant.
Subscapularis releases, however, are not time limited. Since it is merely cutting a "Z" shape into the subscapularis muscle to provide stretch within the arm, it can be carried out at almost any age and can be carried out repeatedly on the same arm; however, this will compromise the integrity of the muscle.
Latissimus Dorsi Tendon Transfers involve cutting the Latissimus Dorsi in half horizontally in order to 'pull' part of the muscle around and attach it to the outside of the biceps. This procedure provides external rotation with varying degrees of success. A side effect may be increased sensitivity of the part of the biceps where the muscle will now lie, since the Latissimus Dorsi has roughly twice the number of nerve endings per square inch of other muscles.
Discovery
The renowned British obstetrician William Smellie is credited with the first medical description of an obstetric brachial plexus palsy. In his 1768 treatise on midwifery, he reported a case of transient bilateral arm paralysis in a newborn after difficult labour.
In 1861, Guillaume Benjamin Amand Duchenne coined the term "obstetric palsy of the brachial plexus" after analyzing 4 infants with paralysis of identical muscles in the arm and shoulder, after publishing his initial findings in 1855.[12][13] In 1874, Wilhelm Heinrich Erb concluded in his thesis on adult brachial plexus injuries that associated palsies of the deltoid, biceps and subscapularis are derived from a radicular lesion at the level of C5 and C6 rather than isolated peripheral nerve lesions.[14]
Notable people with Erb's palsy
Notable individuals afflicted by Erb's palsy were Kaiser Wilhelm II of Germany,[15] Joseph Stalin, and Canadian journalist Barbara Frum. Martin Sheen was injured during birth and developed the condition in his left arm. His difference in arm length and range of motion can be seen in his movies, especially Apocalypse Now. Another sufferer is British singer-songwriter and artist Matt Parsons. Despite her condition, professional wrestler Traci Brooks has achieved a successful career. Another is former Iowa Hawkeyes standout defensive lineman Adrian Clayborn.
See also
- Klumpke's paralysis
References
- ^ Warwick, R., & Williams, P.L, ed (1973). Gray’s Anatomy (35th ed.). London: Longman. pp.1037-1047
- ^ Tortora, G.J., & Anagnostakos, N.P. (1990). Principles of Anatomy and Physiology (6th ed.). New York: Harper & Row. ISBN 0-06-046694-4. pp.370-374
- ^ Abrahams, P (2002). The Atlas of the Human Body: A Complete Guide to How the Body Works. Leicester, U.K.: Silverdale Books. ISBN 1-85605-699-6. pp.76-77
- ^ a b A.D.A.M Healthcare center
- ^ Erb-Duchenne and Dejerine-Klumpke Palsies Information Page: National Institute of Neurological Disorders and Stroke (NINDS)
- ^ a b c d Warwick, R., & Williams, P.L. (1973) p.1046
- ^ Peleg D, Hasnin J, Shalev E (1997). "Fractured clavicle and Erb's palsy unrelated to birth trauma". American Journal of Obstet. Gynecol. 177 (5): 1038–40. doi:10.1016/S0002-9378(97)70010-3. PMID 9396889.
- ^ a b Glanze, W.D., Anderson, K.N., & Anderson, L.E, ed (1990). Mosby's Medical, Nursing, and Allied Health Dictionary (3rd ed.). St. Louis, Missouri: The C.V. Mosby Co.. ISBN 0-8016-3227-7. p.437
- ^ Gherman, Diomid. Neurologie şi neurochirurgie : manual / D. Gherman, I. Moldovanu, G. Zapuhlâh ; USMF "Nicolae Testemiţanu". - Chişinău : Medicina, 2003. - 528 p. - ISBN 9975-907-39-3, Page 207 Afectiunile nervilor membrului superior, http://library.usmf.md/ebooks.php?key=b60
- ^ clinicalconsiderations at The Anatomy Lesson by Wesley Norman (Georgetown University)
- ^ Warwick, R., & Williams, P.L. (1973) pp.1037-1039
- ^ synd/946 at Who Named It?
- ^ Duchenne, G. B. A. (1855). De l’éléctrisation localisée et de son application à la pathologie et à la thérapeutique. Paris: Baillière (French).
- ^ Erb, W. (1874). "Ueber eine eigenthümliche Localisation von Lähmungen im Plexus brachialis". Verhandlungen des naturhistorisch-medicinischen Vereins zu Heidelberg 2: 130–137.
- ^ Ober WB (1992). "Obstetrical events that shaped Western European history". The Yale journal of biology and medicine 65 (3): 201–10. PMC 2589601. PMID 1285448. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2589601.
External links
- Erb's Palsy Group
- Erb's Palsy Pictures
- brachial_plexus at NINDS
- Duke Orthopedics erbs_palsy
- Watt AJ, Niederbichler AD, Yang LJ, Chung KC (2007). "Wilhelm Heinrich Erb, M.D. (1840 to 1921): a historical perspective on Erb's palsy". Plast. Reconstr. Surg. 119 (7): 2161–6. doi:10.1097/01.prs.0000260726.74745.b8. PMID 17519716.
- United Brachial Plexus Network
Certain conditions originating in the perinatal period / fetal disease (P, 760–779) Maternal factors and
complications of pregnancy,
labour and deliveryLength of gestation
and fetal growthSmall for gestational age/Large for gestational age · Preterm birth/Postmature birth · Intrauterine growth restrictionBirth trauma scalp (Cephalhematoma, Chignon, Caput succedaneum, Subgaleal hemorrhage) · Brachial plexus lesion (Erb's palsy, Klumpke paralysis)By system Vitamin K deficiency (Haemorrhagic disease of the newborn)HDN (ABO • Anti-Kell • Rh c • Rh D • Rh E) · Hydrops fetalis · Hyperbilirubinemia (Kernicterus, Neonatal jaundice)Integument and
temperature regulationErythema toxicum · Sclerema neonatorumInfectious Other Categories:- Neurological disorders
- Birth trauma

Wikimedia Foundation. 2010.