- Renal artery stenosis
Infobox_Disease
Name = Renal artery stenosis
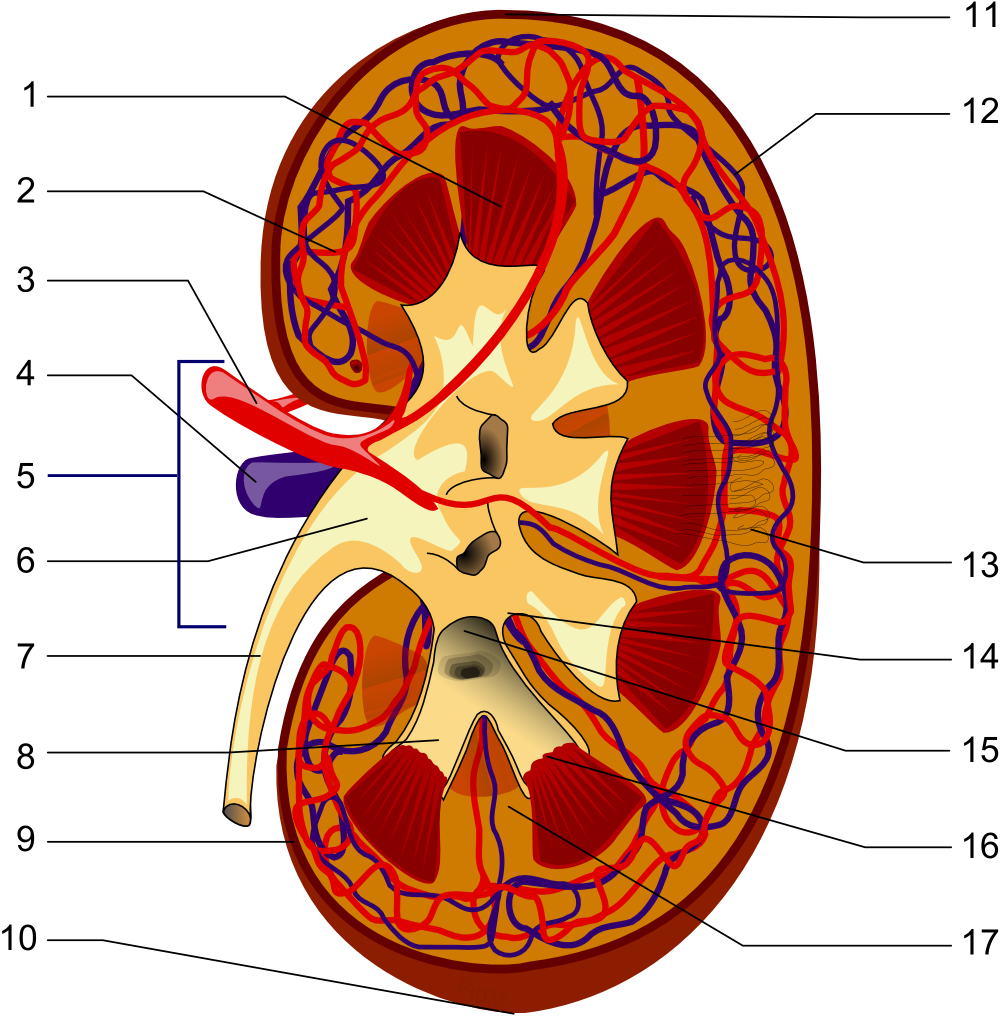
Caption =Renal artery is #3
DiseasesDB = 11255
ICD10 =
ICD9 = ICD9|440.1
ICDO =
OMIM =
MedlinePlus = 001273
eMedicineSubj = med
eMedicineTopic = 2001
MeshID = D012078Renal artery stenosis is the narrowing of the
renal artery , most often caused byatherosclerosis orfibromuscular dysplasia . This narrowing of the renal artery can impede blood flow to the target kidney. Hypertension and atrophy of the affectedkidney may result from renal artery stenosis, ultimately leading torenal failure if not treated.igns and symptoms
Most cases of renal artery stenosis are asymptomatic, and the main problem is high blood pressure that cannot be controlled with medication. Deterioration in
renal function may develop if both kidneys are poorly supplied, or when treatment with anACE inhibitor is initiated. Some patients present with episodes offlash pulmonary edema (sudden left ventricular heart failure). [cite journal |author=Pickering TG, Herman L, Devereux RB, "et al" |title=Recurrent pulmonary oedema in hypertension due to bilateral renal artery stenosis: treatment by angioplasty or surgical revascularisation |journal=Lancet |volume=2 |issue=8610 |pages=551–2 |year=1988 |pmid=2900930 |doi=10.1016/S0140-6736(88)92668-2]Diagnosis
*refractory
hypertension - high blood pressure that can not be controlled adequately withantihypertensives
*auscultation (withstethoscope ) -bruit ("rushing" sound) on affected side, inferior of thecostal margin
*captopril challenge test
*captopril test dose effect on the differential renal function as measured byMAG3 scan .cite journal |author=Roccatello D, Picciotto G |title=Captopril-enhanced scintigraphy using the method of the expected renogram: improved detection of patients with renin-dependent hypertension due to functionally significant renal artery stenosis |journal=Nephrol. Dial. Transplant. |volume=12 |issue=10 |pages=2081–6 |year=1997 |pmid=9351069 |doi= 10.1093/ndt/12.10.2081|url=http://ndt.oxfordjournals.org/cgi/reprint/12/10/2081.pdf |format=PDF]
*renal artery arteriogramA
clinical prediction rule is available to guide diagnosis.cite journal |author=Krijnen P, van Jaarsveld BC, Steyerberg EW, Man in 't Veld AJ, Schalekamp MA, Habbema JD |title=A clinical prediction rule for renal artery stenosis |journal=Ann. Intern. Med. |volume=129 |issue=9 |pages=705–11 |year=1998 |pmid=9841602 |doi=]Etiology
Atherosclerosis is the predominant cause of renal artery stenosis in the majority of patients, usually those with a sudden onset of hypertension at age 50 or older.
Fibromuscular dysplasia is the predominant cause in young patients, usually females under 40 years of age. A variety of other causes exist. These includearteritis , renal artery aneurysm, extrinsic compression (eg.neoplasm s), neurofibromatosis, and fibrous bands.Pathophysiology
The
macula densa of the kidney senses a decreased systemic blood pressure due to the pressure drop over the stenosis. The response of the kidney to this decreased blood pressure is activation of therenin-angiotension aldosterone system , which normally counteracts low blood pressure, but in this case lead to hypertension (high blood pressure). The decreased perfusion pressure (caused by the stenosis) leads to decreased blood flow (hypoperfusion ) to the kidney and a decrease in the GFR. If the stenosis is long standing and severe the GFR in the affected kidneys never increases again and (pre-renal)renal failure is the result.Treatment
When high-grade renal artery stenosis is documented and blood pressure cannot be controlled with medication, or if renal function deteriorates, renal artery stenosis is often treated invasively. Renal artery stenosis is most commonly treated by endovascular techniques (i.e.
angioplasty with or withoutstent ing). A 2003meta-analysis found that angioplasty was safe and effective in this context. [cite journal |author=Nordmann AJ, Woo K, Parkes R, Logan AG |title=Balloon angioplasty or medical therapy for hypertensive patients with atherosclerotic renal artery stenosis? A meta-analysis of randomized controlled trials |journal=Am. J. Med. |volume=114 |issue=1 |pages=44–50 |year=2003 |pmid=12557864 |doi=10.1016/S0002-9343(02)01396-7] There are ongoing clinical trials to compare medical management and angioplasty with stenting to medical management alone. These include CORAL and ASTRAL, both scheduled to report results in 2010. In addition to endovascular treatment, surgical resection and anastomosis is a rarely-used option.ee also
*
Renovascular hypertension References
Wikimedia Foundation. 2010.