- Gastric varices
DiseaseDisorder infobox
Name = Gastric varices
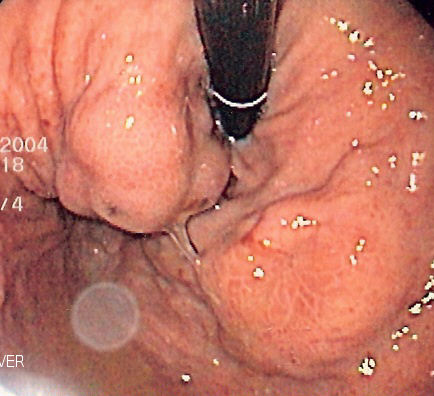
Caption = Isolated gastric varices of Sarin classification IGV-1 seen ongastroscopy in a patient withportal hypertension
ICD10 = ICD10|I|86|4|i|80
ICD9 =Gastric varices are dilated submucosal
vein s in thestomach , which can be a life-threatening cause ofupper gastrointestinal hemorrhage . They are most commonly found in patients withportal hypertension , or elevated pressure in theportal vein system, which may be a complication ofcirrhosis . Gastric varices may also be found in patients with thrombosis of thesplenic vein , into which the short gastric veins which drain thefundus of the stomach flow. The latter may be a complication ofacute pancreatitis ,pancreatic cancer , or other abdominal tumours. Patients with bleeding gastric varices can present with bloody vomiting (hematemesis ), dark, tarry stools (melena ), or frank rectal bleeding. The bleeding may be brisk, and patients may soon develop shock. Treatment of gastric varices can include injection of the varices withcyanoacrylate glue, or a radiological procedure to decrease the pressure in the portal vein, termedtransjugular intrahepatic portosystemic shunt or TIPS. Treatment with intravenousoctreotide is also useful to shunt blood flow away from the stomach's circulation. More aggressive treament includingsplenectomy (or surgical removal of thespleen ) orliver transplantation may be required in some cases.Clinical presentation
Gastric varices can present in two major ways. First, patients with
cirrhosis may be enrolled in screeninggastroscopy programs to detectesophageal varices . These evaluations may detect gastric varices that are asymptomatic. When gastric varices are symptomatic, however, they usually present acutely and dramatically withupper GI hemorrhage . The symptoms can includehematemesis , orvomiting blood;melena , passing black, tarry stools; or passing maroon stools or frank blood in the stools. Many patients with bleeding gastric varices present in shock due to the profound loss of blood.Finally, patients with
acute pancreatitis may present with gastric varices as a complication of thrombosis of thesplenic vein . The splenic vein sits over the pancreas anatomically and inflammation or cancers of the pancreas may result in thrombosis, or clotting of the splenic vein. As the short gastric veins of thefundus of the stomach drain into the splenic vein, thrombosis of the splenic vein will result in increased pressure and engorgement of the short veins, leading to varices in the fundus of the stomach.Laboratory testing usually shows
anemia and oftenthrombocytopenia (a lowplatelet count). If cirrhosis is present, there may becoagulopathy manifested by a prolonged INR; both of these may worsen the hemorrhage from gastric varices.In very rare cases, gastric varices are caused by splenic vein occlusion as a result of the mass effect of slow-growing pancreatic neuroendocrine tumors.
Diagnosis and classification
Diagnosis of gastric varices is often made at the time of upper
endoscopy .The Sarin classification of gastric varices identifies four different anatomical types of gastric varices, which differ in terms of treatment modalities.
Treatment
Initial treatment of bleeding from gastric varices focuses on resuscitation, much as with
esophageal varices . This includes administration of fluids, blood products, and antibiotics.The results from the only two randomized trials comparing band ligation vs cyanocarylate suggests that endoscopic injection of
cyanoacrylate , known as gastric variceal obliteration or GVO is superior to band ligation in preventing rebleeding rates. Cyanoacrylate, a common component insuper glue is often mixed 1:1 withlipiodol to prevent polymerization in the endoscopy delivery optics, and to show on radiographic imaging. GVO is usually performed is specialized therapeutic endoscopy centers. Complications include sepsis, embolization of glue, and obstruction from polymerization in the lumen of thestomach .Other techniques for refractory bleeding include:
*Transjugular intrahepatic portosystemic shunts (TIPS)
*Balloon occluded retrograde transvenous obliteration techniques (BORTO)
*Gastric variceal ligation, although this modality is falling out of favour
*Intra-gastricballoon tamponade as a bridge to further therapy
**a caveat is that a larger balloon is required to occupy thefundus of the stomach where gastric varices commonly occur
*Liver transplantation
Wikimedia Foundation. 2010.