- QT interval
-
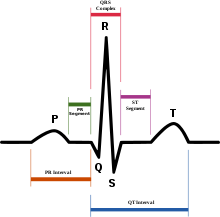 Schematic representation of normal ECG trace (sinus rhythm), with waves, segments, and intervals labeled.
Schematic representation of normal ECG trace (sinus rhythm), with waves, segments, and intervals labeled.
In cardiology, the QT interval is a measure of the time between the start of the Q wave and the end of the T wave in the heart's electrical cycle. In general, the QT interval represents electrical depolarization and repolarization of the left and right ventricles. A prolonged QT interval is a biomarker for ventricular tachyarrhythmias like torsades de pointes and a risk factor for sudden death.
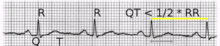 The qt-time is normal, when it is less than half the rr-time.
The qt-time is normal, when it is less than half the rr-time.Contents
Correction for heart rate
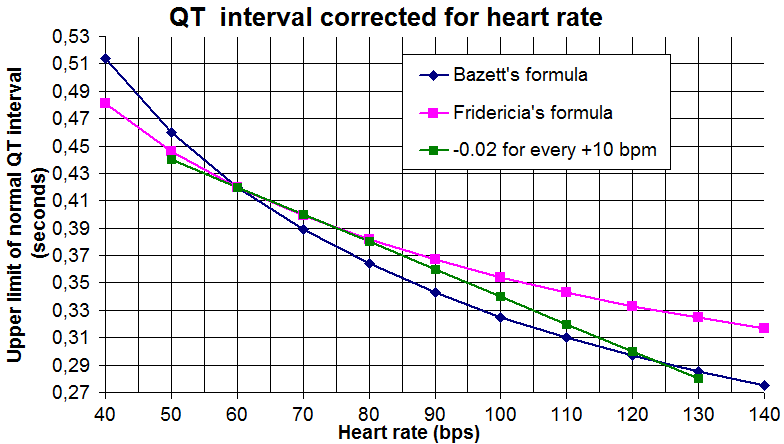
The QT interval is dependent on the heart rate in an obvious way (the faster the heart rate the shorter the QT interval) and may be adjusted to improve the detection of patients at increased risk of ventricular arrhythmia. Modern computer-based ECG machines can easily calculate a corrected QT, but this correction may not aid in the detection of patients at increased risk of arrhythmia.
The standard clinical correction is to use Bazett's formula,[1] named after physiologist Henry Cuthbert Bazett, calculating the heart rate-corrected QT interval QTc.
Bazett's formula is as follows:
QTcB=QT⁄√RR
where QTc is the QT interval corrected for heart rate, and RR is the interval from the onset of one QRS complex to the onset of the next QRS complex, measured in seconds, often derived from the heart rate (HR) as 60/HR (here QT is measured in milliseconds). However, this nonlinear formula, obtained from data in only 39 young men, is not accurate, and over-corrects at high heart rates and under-corrects at low heart rates.[2]
Fridericia[3] has published an alternative correction using the cuberoot of RR.
QTcF=QT⁄3√RR
There are several other methods as well. For example a regression-based approach that had been developed by Sagie et al.,[4] as follows:
QTcL= QT + 0.154(1000-RR)
Definitions of normal QTc varies around being equal to or less than 0.40 s (≤400ms),[5] 0.41s (≤410ms),[6] 0.42s (≤420ms)[7] or 0.44s (≤440ms).[8] For risk of sudden cardiac death "Borderline QTc" in males is 431-450 ms, and in females 451-470 ms. An "abnormal" QTc in males is a QTc above 450 ms, and in females, above 470 ms.[9]
If there is not a very high or low heart rate, the upper limits of QT can roughly be estimated by taking QT=QTc at a heart rate of 60 beats per minute (bpm), and subtracting 0.02s from QT for every 10bpm increase in heart rate. For example, taking normal QTc ≤ 0.42s, QT would be expected to be 0.42s or less at a heart rate of 60bpm. For a heart rate of 70 bpm, QT would roughly be expected to be equal to or below 0.40s. Likewise, for 80 bpm, QT would roughly be expected to be equal to or below 0.38s.[5]
Measurement
The QT interval is an important ECG parameter and the identification of ECGs with long QT syndrome is of clinical importance. Considering the required standards for precision, the measurement of QT interval is subjective.[10] This is because the end of the T wave is not always clearly defined and usually merges gradually with the baseline. QT interval in an ECG complex can be measured manually by different methods such as the threshold method, in which the end of the T wave is determined by the point at which the component of the T wave merges with the isoelectric baseline or the tangent method, in which the end of the T wave is determined by the intersection of a line extrapolated from the isoelectric baseline and the tangent line, which touches the terminal part of the T wave at the point of maximum downslope.[11]
With the increased availability of digital ECGs with simultaneous 12-channel recording, QT measurement may also done by the 'superimposed median beat' method. In the superimposed median beat method, a median ECG complex is constructed for each of the 12 leads. The 12 median beats are superimposed on each other and the QT interval is measured either from the earliest onset of the Q wave to the latest offset of the T wave or from the point of maximum convergence for the Q wave onset to the T wave offset...[12]
Abnormal intervals
If abnormally prolonged or shortened, there is a risk of developing ventricular arrhythmias.
Genetic causes
An abnormal prolonged QT interval could be due to Long QT syndrome, whereas an abnormal shortened QT interval could be due to Short QT syndrome.
The length of the interval was found to associate with variations in NOS1AP gene.[13]
Due to adverse drug reactions
Prolongation of the QT interval may be due to an adverse drug reaction.[14] Many drugs such as haloperidol[15] and methadone[citation needed] can prolong the QT interval. Some antiarrhythmic drugs, like amiodarone or sotalol work by getting a pharmacological QT prolongation. Additionally, some second generation of antihistamines, such as astemizole, have this effect. Additionally, alcohol in high blood concentrations prolong the QT interval.[16]
Due to pathological conditions
Hypothyroidism, a condition of low function of the thyroid gland, can give QTc prolongation at the electrocardiogram. Acute hypocalcemia causes prolongation of the QT interval, which may lead to ventricular dysrhythmias.
A shortened QT can be associated with hypercalcemia.[17]
Use in drug studies for FDA approval
Since 2005, the FDA and European regulators have required that nearly all new molecular entities are evaluated in a Thorough QT (TQT) study to determine a drug's effect on the QT interval.[18] The TQT study serves to assess the potential arrhythmia liability of a drug. Traditionally, the QT interval has been evaluated by having individual human readers measure approximately nine cardiac beats per clinical timepoint. However, a number of recent drug approvals have used a highly automated approach, blending automated software algorithms with expert human readers reviewing a portion of the cardiac beats, to enable the assessment of significantly more beats per timepoint in order to improve precision and reduce cost.[19] As the pharmaceutical industry has gained experience in performing TQT studies, it has also become evident that traditional QT correction formulas such as QTcF, QTcB, and QTcI may not always be suitable for evaluation of drugs impacting autonomic tone.[20] Current efforts are underway by industry and regulators to consider alternative methods to help evaluate QT liability in drugs affecting autonomic tone, such as QT beat-to-beat and Holter-bin methodologies.[21]
See also
References
- ^ a b Bazett HC. (1920). "An analysis of the time-relations of electrocardiograms". Heart (7): 353–370.
- ^ Salvi V, Karnad DR, Panicker GK, Kothari S. (2010). "Update on the evaluation of a new drug for effects on cardiac repolarization in humans: issues in early drug development". Br J Pharmacol. 159 (1): 34–48. doi:10.1111/j.1476-5381.2009.00427.x. PMC 2823350. PMID 19775279. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2823350.
- ^ a b Fridericia LS (1920). "The duration of systole in the electrocardiogram of normal subjects and of patients with heart disease". Acta Medica Scandinavica (53): 469–486.
- ^ Sagie A, Larson MG, Goldberg RJ, Bengston JR, Levy D (1992). "An improved method for adjusting the QT interval for heart rate (the Framingham Heart Study)". Am J Cardiol 70 (7): 797–801. doi:10.1016/0002-9149(92)90562-D. PMID 1519533.
- ^ a b c Lesson III. Characteristics of the Normal ECG Frank G. Yanowitz, MD. Professor of Medicine. University of Utah School of Medicine. Retrieved on Mars 23, 2010
- ^ Loyola University Chicago Stritch School of Medicine > Medicine I By Matthew Fitz, M.D. Retrieved on Mars 23, 2010
- ^ ecglibrary.com > A normal adult 12-lead ECG Retrieved on Mars 23, 2010
- ^ Image for Cardiovascular Physiology Concepts > Electrocardiogram (EKG, ECG) By Richard E Klabunde PhD
- ^ medscape.com > QTc Prolongation and Risk of Sudden Cardiac Death: Is the Debate Over? February 3, 2006
- ^ Panicker GK, Karnad DR, Joshi R, Shetty S, Vyas N, Kothari S, Narula D (2009). "Z-score for benchmarking reader competence in a central ECG laboratory". Ann Noninvasive Electrocardiol 14 (14(1)): 19–25. doi:10.1111/j.1542-474X.2008.00269.x. PMID 19149789.
- ^ Panicker GK, Karnad DR, Natekar M, Kothari S, Narula D, Lokhandwala Y (2009). "Intra- and interreader variability in QT interval measurement by tangent and threshold methods in a central electrocardiogram laboratory". J Electrocardiol 42 (42(4)): 348–52. doi:10.1016/j.jelectrocard.2009.01.003. PMID 19261293.
- ^ Salvi V, Karnad DR, Panicker GK, Natekar M, Hingorani P, Kerkar V, Ramasamy A, de Vries M, Zumbrunnen T, Kothari S, Narula D (2011). "Comparison of 5 methods of QT interval measurements on electrocardiograms from a thorough QT/QTc study: effect on assay sensitivity and categorical outliers". J Electrocardiol 44 (44(2)): 96–104. doi:10.1016/j.jelectrocard.2010.11.010. PMID 21238976.
- ^ Arking DE, Pfeufer A, Post W, Kao WH, Newton-Cheh C, Ikeda M, West K, Kashuk C, Akyol M, Perz S, Jalilzadeh S, Illig T, Gieger C, Guo CY, Larson MG, Wichmann HE, Marbán E, O'Donnell CJ, Hirschhorn JN, Kääb S, Spooner PM, Meitinger T, Chakravarti A (June 2006). "A common genetic variant in the NOS1 regulator NOS1AP modulates cardiac repolarization". Nat. Genet. 38 (6): 644–51. doi:10.1038/ng1790. PMID 16648850.
- ^ Leitch A, McGinness P, Wallbridge D (September 2007). "Calculate the QT interval in patients taking drugs for dementia". BMJ 335 (7619): 557. doi:10.1136/bmj.39020.710602.47. PMC 1976518. PMID 17855324. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1976518.
- ^ "Information for Healthcare Professionals: Haloperidol (marketed as Haldol, Haldol Decanoate and Haldol Lactate)". Archived from the original on 2007-10-11. http://web.archive.org/web/20071011025019/http://www.fda.gov/cder/drug/InfoSheets/HCP/haloperidol.htm. Retrieved 2007-09-18.
- ^ Willy Aasebø, Jan Erikssen, Jørgen Jonsbu and Knut Stavem. ECG changes in patients with acute ethanol intoxication. Scand Cardiovasc J, 41 (2) 79-84 (2007)
- ^ http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/endocrinology/hypercalcemia/
- ^ http://www.fda.gov/downloads/RegulatoryInformation/Guidances/UCM129357.pdf
- ^ http://appliedclinicaltrialsonline.findpharma.com/appliedclinicaltrials/News/iCardiac-Applies-Automated-Approach-to-Thorough-QT/ArticleStandard/Article/detail/560528?contextCategoryId=44906&ref=25
- ^ http://thew-project.org/document/2009%20THEW%20meeting/Garnett.pdf
- ^ http://thew-project.org/document/FDA%20CPI%20project.pdf
External links
Categories:

Wikimedia Foundation. 2010.