- Methadone
-
"Phy" redirects here. For the abbreviation for the physical layer of the OSI Model, see PHY.
Methadone 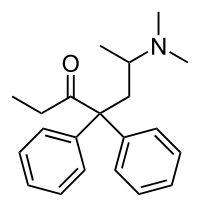
Systematic (IUPAC) name (RS)-6-(Dimethylamino)-4,4-diphenylheptan-3-one Clinical data Trade names Dolophine AHFS/Drugs.com Consumer Drug Information MedlinePlus a682134 Pregnancy cat. Category C[1] Legal status Schedule II (US) Class A (UK) Dependence liability Very High Routes oral, intravenous, insufflation, sublingual, rectal Pharmacokinetic data Bioavailability 40-90% (oral) Metabolism Hepatic Half-life 24-36 h Excretion Urine, Test by specific gravity and bilirubin Identifiers CAS number 76-99-3 
ATC code N02AC52 N07BC02, R05DA06 PubChem CID 4095 IUPHAR ligand 1605 DrugBank DB00333 ChemSpider 3953 UNII UC6VBE7V1Z KEGG D08195 ChEBI CHEBI:6807 
ChEMBL CHEMBL651 Chemical data Formula C21H27NO Mol. mass 309.445 g/mol SMILES eMolecules & PubChem - InChI=1S/C21H27NO/c1-5-20(23)21(16-17(2)22(3)4,18-12-8-6-9-13-18)19-14-10-7-11-15-19/h6-15,17H,5,16H2,1-4H3
Key:USSIQXCVUWKGNF-UHFFFAOYSA-N
 (what is this?) (verify)
(what is this?) (verify)Methadone (also known as Symoron, Dolophine, Amidone, Methadose, Physeptone, Heptadon, Phy and many other names) is a synthetic opioid, used medically as an analgesic and a maintenance anti-addictive for use in patients with opioid dependency. It was developed in Germany in 1937. Although chemically unlike morphine or heroin, methadone acts on the same opioid receptors as these drugs, and thus has many of the same effects. Methadone is also used in managing severe chronic pain, owing to its long duration of action, extremely powerful effects, and very low cost. Methadone was introduced into the United States in 1947 by Eli Lilly and Company.
Methadone is useful in the treatment of opioid dependence. It has cross-tolerance with other opioids including heroin and morphine, offering very similar effects and a long duration of effect. Oral doses of methadone can stabilise patients by mitigating opioid withdrawal syndrome. Higher doses of methadone can block the euphoric effects of heroin, morphine, and similar drugs. As a result, properly dosed methadone patients can reduce or stop altogether their use of these substances.
Methadone is approved for different indications in different countries. Common is approval as an analgesic and approval for the treatment of opioid dependence. It is not intended to reduce the use of non-narcotic drugs such as methamphetamine, or alcohol.
A number of pharmaceutical companies produce and distribute methadone. The racemic hydrochloride is the only form available in most countries, such as the Netherlands, Belgium, France and in the United States, as of March 2008. The tartrate and other salts of the laevorotary form (levomethadone, with trade names including Polamidone and Heptadon) are available in Europe and elsewhere. These are more potent opioid agonists compared to racemic methadone because the dextrorotary form (d-methadone) is not an opioid agonist (it is an NMDA antagonist), therefore by using only the laevorotary form instead of the racemate the opioid agonist potency is doubled. Covidien (formerly Mallinckrodt), is the major racemic methadone producer and sells bulk methadone to producers of generic preparations and distributes its own product in the form of tablets, dispersible tablets and oral concentrate under the brand name Methadose in the United States.[2]
Contents
Medical uses
Methadone maintenance treatment
MMT (Methadone Maintenance Treatment), a form of opiate replacement therapy, reduces and/or eliminates the use of illicit opiates, the criminality associated with opiate use, and allows patients to improve their health and social productivity.[3][4] In addition, enrollment in methadone maintenance has the potential to reduce the transmission of infectious diseases associated with opiate injection, such as hepatitis and HIV.[3] The principal effects of methadone maintenance are to relieve narcotic craving, suppress the abstinence syndrome, and block the euphoric effects associated with opiates. Methadone maintenance has been found to be medically safe and non-sedating.[3] It is also indicated for pregnant women addicted to opiates.[3]
In Russia, methadone treatment is illegal. Health officials there are not convinced of the treatment's efficacy. Instead, doctors encourage immediate abstinence from drug use, rather than the gradual process that methadone substitution therapy entails. Patients are often given sedatives and painkillers to cope with withdrawal symptoms.[5]
Dosage
Dosing considerations in an outpatient treatment program, where individuals carry a high degree of tolerance to opioids and are closely monitored with witnessed daily dosing, is a separate consideration from the patient with chronic pain requiring analgesia. The intermittent follow up of the pain patient, coupled with the relatively unforgiving nature of the drug (compared with other Long acting opioids), should generate caution in the patient and prescriber alike in an outpatient pain environment. A majority of patients in outpatient treatment programs require 80–125 mg/d of methadone, or more, to achieve these effects and require treatment for an indefinite period of time, since methadone maintenance is a corrective but not a curative treatment for opiate addiction.[3] Lower doses are sometimes not as effective, or do not provide an equivalent blockade effect as higher dosages can. Some patients will be prescribed as much as 750 mg of methadone a day;[6] though a dose as low as 30 mg can prove fatal in an opiate naive individual, or in individuals who lack cross-tolerance to other opioids.[citation needed]
In the United States addiction clinics typically start patients at a low dose, generally only starting patients on methadone when they are in withdrawal and providing a small test dose, after which the patients are observed for possible adverse effects. Assuming there are no complications, the remaining portion of the first day's dose is then given. After this the doses are titrated until they reach either a clinically sufficient level that prevents withdrawal, cravings and possible continued use of illicit opioids, or until they reach a maximum dose set by clinic policy. For example, a clinic may start patients at 30 mg and raise the dosage 5 mg a day until the patient reports feeling comfortable (e.g. free of withdrawal symptoms). Alternatively, the clinic may stop dosage at 80 mg, then allow the patient to move up by 5 mg or 10 mg every 2 or 3 days, until they are free from withdrawal symptoms and intense cravings. Once stabilized, patients may require periodic dose adjustments as their clinical or subjective tolerance changes.
The most common and traditional dosing regimens, however, tend to fall far short of providing optimum or even sufficient results for a number of patients. This is due to the ceilings many clinics place on dose levels.[7][8]
Until recently a 100-mg/d dose was regarded as a 'glass ceiling,' rarely to be penetrated. In practice much lower thresholds were maintained even though the optimal dose varies greatly between patients, often quite higher than this and with no inherent threshold in the possible dose, as the toxic dose for patients with very high tolerance can exceed this tenfold or more. The blood concentrations of patients on an equivalent dose (when adjusted for body weight) can vary as much as 17-fold, or up to 41-fold when influenced by other medications, leading to a vast range of potentially required doses.[9][10]
In the United States, federal law was changed in 2001 to eliminate some restrictions imposed on patients dosed on more than 100 mg per day.
Duration
While there is much debate generally over treatment schedules and duration, patients can often obtain indefinite treatment at their methadone clinic—lasting as long as the patient requires it. Many factors determine the treatment schedule, including specific clinic policies which sometimes require patients to taper regardless of their desire to do so. In general, methadone maintenance is seen as ongoing symptom management rather than a curative treatment. This has buttressed the arguments of those who view methadone as just another prescription drug taken for a long-term, chronic condition.
Dosage reduction
A patient's dose of methadone may be reduced by a slow taper with minimal discomfort. Patients undergoing MMT at a clinic where they are given a daily dose have the opportunity to attempt a dose reduction and return to the previous dose if they are feeling discomfort. Policies on dose reduction vary from clinic to clinic, from a focus on eventually tapering the patient off of methadone altogether to a focus on maintaining a high dose to prevent the use of illicit opioids. Many methadone clinics will adjust doses upon personal evaluation of the correct care for the individual patient. A higher methadone dose may be considered preferable by a clinic treating patients addicted to illicit opioids, in order to discourage the use of illegal opioids. This can be due to the large increase in tolerance, a chemical blocking effect caused by methadone above certain doses, or by filling a psychological or physical need that illicit opioids were previously being used for.
To minimize or prevent patient discomfort, the methadone dose must be decreased slowly. Typical reduction rates vary and should be adjusted based on patient response.
Frequently this adjustment is monitored on a daily basis. Most of the literature focuses on methadone maintenance patients visiting clinics daily, focused on heroin substitution. Chronic pain patients wishing to decrease their methadone dose must follow similar titration regimens. However their doctor may substitute alternative opioids during this period, altering what rate is compatible with patient comfort when compared with complete detoxification.
The Centre for Addiction and Mental Health, Ontario, Canada has this recommendation:[11]
Methadone tapering works best when done as a slow and gradual reduction in dose, dropping 5 mg every three to 14 days. At this rate there should be very few, if any, physical symptoms during the taper. Once the dose is lowered to around 20 mg, the tapering may be slowed down to an even more gradual reduction, to reduce or eliminate any symptoms. Nowadays, most methadone providers will allow you to choose the rate at which your dose is reduced.
Aegis Medical Systems Tapering Off of Methadone Maintenance: Evidence-Based Guidelines[12]
recommends regular evaluation of the patient's withdrawal symptoms, counseling where needed, and a generally slow rate, noting:
Dr. J. Thomas Payte, a highly experienced clinician and researcher, has suggested that a 7-10 day period between dose decreases should be adequate time to adjust before the next drop.
Clinical experience reminds us of an important rule in tapering, “THE SLOWER, THE BETTER,”
The College of Pharmacists of British Columbia discusses more specific rates on page 19 of a slide presentation:[13]
Stopping Methadone
- Greater detox. completion rates with greater time spent in MMT & slower taper.
- Taper rate
- < 10 mg or 10% per week.
- Slower taper below 20-30 mg.
Mallinckrodt, the primary manufacturer of methadone in the US, has guidelines[14] that include
For Medically Supervised Withdrawal After a Period of Maintenance Treatment There is considerable variability in the appropriate rate of methadone taper in patients choosing medically supervised withdrawal from methadone treatment. It is generally suggested that dose reductions should be less than 10% of the established tolerance or maintenance dose, and that 10 to 14-day intervals should elapse between dose reductions. Patients should be apprised of the high risk of relapse to illicit drug use associated with discontinuation of methadone maintenance treatment.
Other documents discussing the recommended rate of dose reduction can be found from Health Canada[15] and the Canadian Department Of Health And Human Services[16]
Visits to clinics
Methadone has traditionally been provided to people who are opiate dependent in a highly regulated methadone clinic, generally associated with an outpatient department of a hospital, though this varies country by country. For example in Australia, Methadone maintenance treatment (MMT) is delivered by private pharmacies for a nominal fee to the client (regardless of the fact it is free as it is subsidised by the Federal government). This nominal fee covers the costs of providing the service, such as purchase and maintenance of supplies and equipment like dosing cups and precision measuring devices, supply costs involved in transporting a highly regulated drug from supplier to the pharmacy, extensive record-keeping as per government requirements, and compensation to the pharmacy staff for the time involved in preparing for and dosing a client (none of which are funded by the Federal government).
In many Western countries, new patients are required to visit the clinic daily so that they may be observed taking their dose by the dispensing nurse, but may be allowed to leave the clinic with increasing supplies of "take home doses" or "carries" after several months of adherence to the clinic's regulations, including consistent negative drug-screen results. The way that MMT is delivered in some countries create barriers to scaling up access to the treatment. This can inhibit people's willingness to access treatment due to a lack of confidentiality and anonymity. In most well-designed pharmacies in Australia, however, dosing occurs in a discreet location away from other customers, and may even take place in a room specially designed for this purpose. In some countries or regions, law stipulates that clinics may provide at most one week's worth of methadone (up to 30 days in the USA but states may allow as few as three), except for patients unable to visit the clinic without undue hardship due to a medical disability or infrequent exceptions made for necessary travel to areas without clinics, and this level is only reached after a few years of proper results. A lot of patients report that this type of treatment is the only long term treatment option that has ever continued to be effective for them. A lot of mental issues that come from discontinuing the use of all types of opiates do not cease for years or more. The methadone programs, if correctly monitored, can help the patient get back to their life and be able to function without the constant cravings and insomnia reported after quitting opiates. Methadone can provide a method of stable treatment of the symptoms associated with withdrawal and mental anguish, and, with a proper slow taper, can be discontinued after the patient feels he or she is ready, often after a year or more, which gives the addict time to get away from old habits or triggers.
In the U.S., MMT patients generally receive psycho-social support (i.e. "counseling"), which is provided on site. Although laws vary, this is required in many states and countries regardless of whether a person needs or wants to engage in that kind of intervention (for example, recent changes in Taiwan). Patients are often required to attend 10 hours or more of therapy per week, having their daily dose withheld (thereby inducing withdrawal) for failure to comply. Methadone maintenance is rarely covered by private insurance and patients are encouraged to enroll in public welfare programs or face upwards of $500 USD per month. Since a supervised dose costs more than a take-home dose, and the risk of diversion, clinics are often reluctant to provide take-home privileges.
Cost
In Germany the annual cost per patient is less than 3000 euros, while heroin assisted treatment costs up to 10,000 euros per year.
Methadone clinics in the U.S. charge anywhere from $50–300 per week, which may be covered by private insurance or Medicaid.
MMT cost analyses often compare the cost of clinic visits versus the overall societal costs of illicit opioid use.[17][18]
Analgesic
In recent years, methadone has gained popularity among physicians for the treatment of other medical problems, such as an analgesic in chronic pain. Due to its activity at the NMDA receptor it may be more effective against neuropathic pain; for the same reason tolerance to the analgesic effects maybe lesser compared to other opioids. The increased usage comes as doctors search for an opioid drug that can be dosed less frequently than shorter-acting drugs like morphine or hydrocodone. Another factor in the increased usage is the low cost of methadone.[19][20][21]
While the cost for pain patients varies based on many factors, leading to few specifics in the literature, one source[22] states:
Prices vary; however, in some cases monthly costs to patients for oral methadone can be more than 30-fold less than equianalgesic doses of other generic or brand-name opioid analgesics.
A week's supply will typically have a retail cost of $50–$100 in the United States,[citation needed] compared to hundreds of dollars for alternative opioids. Methadone, with its long half-life (and thus long duration of effect) and good oral bioavailability, is a common second-choice drug for pain that does not respond to weaker agonists. A major drawback is that unlike OxyContin (oxycodone continuous release), methadone is not technologically engineered for sustained release of the drug so blood concentrations will fluctuate greatly between dosing. This problem is overcome to a great extent by the practice of dosing methadone two or three times a day in pain patients. Some physicians also choose methadone for treating chronic pain in patients who are thought to have a propensity for addiction, because it causes less of an intoxicated or euphoric "high". The effect is of morphine-equivalent origin.
On November 29, 2006, the U.S. Food and Drug Administration issued a Public Health Advisory about methadone titled "Methadone Use for Pain Control May Result in Death and Life-Threatening Changes in Breathing and Heart Beat." The advisory went on to say that "the FDA has received reports of death and life-threatening side effects in patients taking methadone. These deaths and life-threatening side effects have occurred in patients newly starting methadone for pain control and in patients who have switched to methadone after being treated for pain with other strong narcotic pain relievers. Methadone can cause slow or shallow breathing and dangerous changes in heart beat that may not be felt by the patient." The advisory urged that physicians use caution when prescribing methadone to patients who are not used to the drug, and that patients take the drug exactly as directed.[23] As with any strong medication that can be fatal in large doses, methadone must be taken properly and with due care. Otherwise, the accumulation of methadone could potentially reach a level of toxicity if the dose is too high or if the user's metabolism of the drug is slow. In such a situation, a patient who fared fine after the first few doses could reach high levels of the drug in his body without ever taking more than was prescribed. For this reason, it is reasonable to make sure that patients who do not have a tolerance to opiates be prescribed methadone in initially small doses, and that when sent home, patients and their families are made very aware of the symptoms characteristic of opiate overdose. Also, there is some evidence that methadone and other opioids may cause cardiac conduction problems (prolonged QTc interval[24][25]) although there are few documented cases of fatalities resulting from this side effect with methadone.
In an effort to turn the tide on reported increases in methadone-related adverse events, the DEA announced in a recent advisory that manufacturers of methadone hydrochloride 40-mg tablets have agreed to restrict their distribution of that particular formulation of the drug.
As of 1. January 2008, manufacturers will ship the methadone hydrochloride 40-mg formulation only to hospitals and facilities that have been authorized for detoxification and maintenance treatment of patients with opioid addiction. In addition, manufacturers of the drug will instruct their wholesale distributors to stop supplying the formulation to any facility that doesn't meet the criteria.
The DEA advisory stresses that the 40-mg formulation of methadone hydrochloride is indicated only for the detoxification and maintenance treatment of opioid-addicted patients and is not FDA-approved for use in pain management.
Federal law does not restrict the prescribing, dispensing or administration of methadone for the treatment of pain, and the 5-mg and 10-mg methadone formulations will continue to be available as a tool that family physicians can use to treat patients for pain. Despite the FDA directive, many doctors continue to prescribe Methadone as a pain killer, but only to patients which have shown to be responsible in their use of previous pain killers. One reason for use of Methadone is its advantages for opioid rotation.
Patients with long-term pain will sometimes have to perform so-called opioid rotation.[26] By this is meant switching from one opioid to another, usually at intervals of between a few weeks and, more commonly, several months. Opioid rotation is good because switching to another opioid gives lower dose, and because of this less side effects, to achieve the desired effect. Then, with the new opioid, tolerance grows, higher doses are needed, and toxicity in relation to analgesic effects increase. So then it is time rotate again to another opioid. Such opioid rotation is standard practice for managing patients with tolerance development problems. Usually, when doing opioid rotation, one cannot go down to a completely naive dose, because there is cross-tolerance, so some of the high tolerance is brought over to the new opioid. However, Methadone has much lower cross-tolerance, when switching to it from other opioids, than other opioids.[27] This means that Methadone can start at a low dose, and the time for the next switch will be longer.
All opioids have tiredness as a major side effect, which can lead to the patient being in an almost half-awake state, in medical terms known as sedation. Many patients report that Methadone's sedation effect is often less pronounced than with other opioids and cite this as a major argument for preferring Methadone as an analgesic.[28]
Antitussive
Methadone linctus, which is about one-third the concentration of the liquid methadone used for opioid maintenance, is used where available and approved for such use as a cough syrup for violent coughing. Some studies have shown narcotic cough suppressants to be useful against dry, unproductive coughing, but others have shown questionable or no benefit.
Natural and semi-synthetic opiates with antitussive effects include codeine, ethylmorphine (also known as dionine or codethyline), dihydrocodeine, benzylmorphine, laudanum, dihydroisocodeine, nicocodeine, nicodicodeine, hydrocodone, hydromorphone, acetyldihydrocodeine, thebacon, diamorphine (heroin), acetylmorphone, noscapine and pholcodine and others. Amongst other synthetics are dimemorfan and dextromethorphan in the morphinan group, tipepidine of the thiambutenes, and other drugs of the open-chain (methadone) type with antitussive efficacy include levomethadone, normethadone and levopropoxyphene. There is also the newer synthetic Zipeprol, classified as 'Other' (not available in the U.S. or CA).
Leukemia
Researchers in Germany have discovered that methadone has surprising killing power against leukemia cells, including treatment-resistant forms of the cancer. Their laboratory study, published in the 1 August 2008 issue of Cancer Research, a journal of the American Association for Cancer Research, suggests that methadone holds promise as a new therapy for leukemia, especially in patients whose cancer no longer responds to chemotherapy and radiation.[29]
Adverse effects
Adverse effects of methadone include:[30][31][32][33][34]
- Thrombus
- Hypoventilation
- Constipation
- Increased sweating and heat intolerance
- Chronic fatigue, sleepiness and exhaustion
- Constricted pupils
- Nausea
- Low blood pressure
- Hallucination
- Headache
- Vomiting
- Cardiac arrhythmia[25]
- Anorexia
- Weight gain
- Sudden Death
- Gynecomastia
- Memory loss
- Stomach pains
- Dry mouth
- Perspiration
- Flushing
- Itching
- Difficulty urinating
- Swelling of the hands, arms, feet, and legs
- Agitation
- Mood changes
- Blurred vision
- Insomnia
- Impotence
- Skin rash
- Seizures
Detection in biological fluids
Methadone and its major metabolite, EDDP, are often measured in urine as part of a drug abuse testing program, in plasma or serum to confirm a diagnosis of poisoning in hospitalized victims, or in whole blood to assist in a forensic investigation of a traffic or other criminal violation or a case of sudden death. Methadone usage history is considered in interpreting the results as a chronic user can develop tolerance to doses that would incapacitate an opioid-naive individual. Chronic users often have high methadone and EDDP baseline values.[35]
Mortality
In the United States, deaths linked to methadone more than quadrupled in the five year period between 1999 and 2004. According to the U.S. National Center for Health Statistics,[36] as well as a 2006 series in the Charleston (West Virginia) Gazette,[37] medical examiners listed methadone as contributing to 3,849 deaths in 2004. That number was up from 790 in 1999. Approximately 82 percent of those deaths were listed as accidental, and most deaths involved combinations of methadone with other drugs (especially benzodiazepines).
Although deaths from methadone are on the rise, methadone-associated deaths are not being caused primarily by methadone intended for methadone treatment programs, according to a panel of experts convened by the Substance Abuse and Mental Health Services Administration, which released a report titled "Methadone-Associated Mortality, Report of a National Assessment". The consensus report concludes that "although the data remain incomplete, National Assessment meeting participants concurred that methadone tablets and/or diskettes distributed through channels other than opioid treatment programs most likely are the central factor in methadone-associated mortality."[38]
In 2006, the U.S. Food and Drug Administration issued a caution about methadone, titled “Methadone Use for Pain Control May Result in Death.” The FDA also revised the drug's package insert. The change deleted previous information about the usual adult dosage. The Charleston Gazette reported, "The old language about the 'usual adult dose' was potentially deadly, according to pain specialists."[39]
Driving
Methadone treatment may impair driving ability.[40] Drug abuse patients had significantly more involvement in serious crashes than non-abuse patients in a study by Queensland University. In the study of a group of 220 drug abuse patients, most of them poly-drug abusers, 17 were involved in crashes killing people, compared with a control group of other patients randomly selected having no involvement in fatal crashes.[41] However, there have been multiple studies verifying the ability of methadone maintenance patients to drive.[42]
Tolerance and dependence
As with other opioid medications, tolerance and dependence usually develop with repeated doses. There is some clinical evidence that tolerance to analgesia is less with methadone compared to other opioids; this may be due to its activity at the NA receptor. Tolerance to the different physiological effects of methadone varies; tolerance to both analgesic properties and euphoria develops quickly, whereas tolerance to constipation, sedation, and respiratory depression develops slowly (if ever).[43]
Withdrawal symptoms
Physical symptoms[citation needed]
- Lightheadedness
- Tearing
- Runny nose
- Yawning
- Sneezing
- Nausea
- Vomiting
- Diarrhea
- Severe Itching
- Fever
- Sweating
- Chills
- Tremors
- Akathisia
- Tachycardia
- Aches and pains, often in the joints and/or legs
- Elevated pain sensitivity
- Elevated blood pressure
- Reduced breathing (may be fatal between 2–4 hours)
Cognitive symptoms[citation needed]
- Suicidal ideation
- Susceptibility to Cravings
- Depression
- Reduced breathing (may be fatal between 2–4 hours)
- Spontaneous orgasm
- Prolonged insomnia
- Delirium
- Auditory hallucinations
- Visual hallucinations
- Increased perception of odors (olfaction), real or imagined
- Marked decrease in sex drive
- Agitation
- Anxiety
- Panic disorder
- Paranoia
- Delusions
Withdrawal symptoms have shown to be up to twice as severe than those of morphine or heroin at equivalent doses and are significantly more prolonged; methadone withdrawal symptoms can last for several weeks or more. A general guideline is a 1:1 ratio for trouble free detox. Being on a constant dose of say 100 mg. for one year, can take 18–24 months for safe detoxification. At high maintenance doses, sudden cessation of therapy can result in severe withdrawal symptoms lasting from weeks to months.[44]
There is a trend in the management of opiate addiction towards the reduction of a patient's methadone dosage to a point where they can be switched to buprenorphine or another opiate with an easier withdrawal profile. When detoxing at a recommended rate (typically 1-2 mgs per week), withdrawal is either minimal or nonexistent, as the patient's body has time to adjust to each reduction in dose. However, like methadone, buprenorphine produces similar cognitive dehabilitation in multiple areas of mental function in both memory and timed choice task tests, which may persist after cessation of substitution treatment.
Pharmacology
Methadone acts by binding to the µ-opioid receptor, but also has some affinity for the NMDA ionotropic glutamate receptor. It is metabolized by the enzymes CYP3A4, CYP2B6 and CYP2D6, with great variability between individuals. Its main route of administration is oral. Adverse effects include hypoventilation, constipation and miosis, in addition to tolerance, dependence and withdrawal difficulties. The withdrawal period can be much more prolonged than with other opiates, spanning anywhere from two weeks to six months.It can also be found in urine samples six to ten weeks after the last dose. It was generally thought it left the system 2–3 days after last use but this is not the case, many factors contribute to how long it will stay in the system. It depends an individual's body weight, metabolism, history of use/abuse and many more factors. In studies done on Methadone users going through detox, individuals experienced different withdrawal symptoms and withdrawal periods even though they received their last dose at the same time. When they gave blood and urine samples the methadone showed up in some individuals samples as much as four weeks after it was not evident in other individuals samples.
Mechanism of action
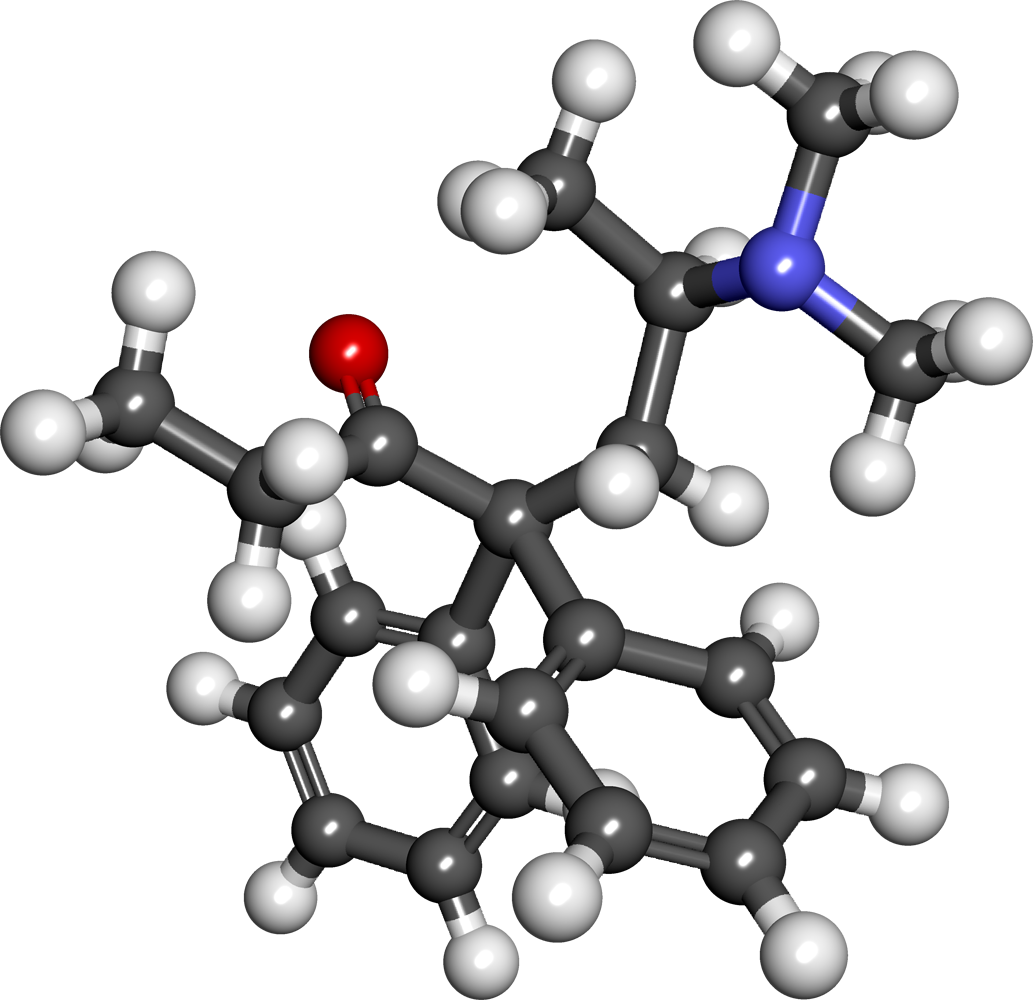
 Ball-and-stick model of methadone
Ball-and-stick model of methadone
Methadone is a full µ-opioid agonist. Methadone also binds to the glutamatergic NMDA (N-methyl-D-aspartate) receptor, and thus acts as a receptor antagonist against glutamate. Glutamate is the primary excitatory neurotransmitter in the CNS. NMDA receptors have a very important role in modulating long term excitation and memory formation. NMDA antagonists such as dextromethorphan (DXM), ketamine (a dissociative anaesthetic, also M.O.A+.), tiletamine (a veterinary anaesthetic) and ibogaine (from the African tree Tabernanthe iboga, also M.O.A+.) are being studied for their role in decreasing the development of tolerance to opioids and as possible for eliminating addiction/tolerance/withdrawal, possibly by disrupting memory circuitry. Acting as an NMDA antagonist may be one mechanism by which methadone decreases craving for opioids and tolerance, and has been proposed as a possible mechanism for its distinguished efficacy regarding the treatment of neuropathic pain. The dextrorotary form (d-methadone) acts as an NMDA antagonist and is devoid of opioid activity: it has been shown to produce analgesia in experimental models of chronic pain. Methadone also acted as a potent, noncompetitive α3β4 neuronal nicotinic acetylcholine receptor antagonist in rat receptors, expressed in human embryonic kidney cell lines.[45]
Metabolism
Methadone has a slow metabolism and very high fat solubility, making it longer lasting than morphine-based drugs. Methadone has a typical elimination half-life of 15 to 60 hours with a mean of around 22. However, metabolism rates vary greatly between individuals, up to a factor of 100,[46][47] ranging from as few as 4 hours to as many as 130 hours,[48] or even 190 hours.[49] This variability is apparently due to genetic variability in the production of the associated enzymes CYP3A4, CYP2B6 and CYP2D6. Many substances can also induce, inhibit or compete with these enzymes further affecting (sometimes dangerously) methadone half-life. A longer half-life frequently allows for administration only once a day in Opioid detoxification and maintenance programs. Patients who metabolize methadone rapidly, on the other hand, may require twice daily dosing to obtain sufficient symptom alleviation while avoiding excessive peaks and troughs in their blood concentrations and associated effects.[48] This can also allow lower total doses in some such patients. The analgesic activity is shorter than the pharmacological half-life; dosing for pain control usually requires multiple doses per day.[citation needed]
The toxic effects of an overdose can be treated with naloxone.[30] Naloxone is preferred to the newer, longer acting antagonist naltrexone. Despite Methadone's much longer duration of action compared to either heroin and other shorter-acting agonists, and the need for repeat doses of the antagonist naloxone, it is still used for overdose therapy. As naltrexone has a longer half-life, it is more difficult to titrate. If too large a dose of opioid antagonist is given to a dependent patient, it will result in withdrawal symptoms (possibly severe). When using naloxone, the naloxone will be quickly eliminated and the withdrawal will be short lived. Doses of naltrexone take longer to be eliminated from the patient's system. A common problem in treating methadone overdoses is that, given the short action of Naloxone (versus the extremely longer-acting Methadone), a dosage of Naloxone given to a Methadone-overdosed patient will initially work to bring the patient out of overdose, but once the Naloxone wears off, if no further Naloxone is administered, the patient can go right back into overdose (based upon time and dosage of the Methadone ingested).
Route of administration
The most common route of administration at a methadone clinic is in a racemic oral solution, though in Germany, only the R enantiomer (the L optical isomer) has traditionally been used, as it is responsible for most of the desired opioid effects.[48] This is becoming less common due to the higher production costs.
Methadone is available in traditional pill, sublingual tablet, and two different formulations designed for the patient to drink. Drinkable forms include ready-to-dispense liquid, and "Disket" which is a tablet designed to disperse itself in water for oral administration, used in a similar fashion to Alka-Seltzer. The liquid form is the most common as it allows for smaller dose changes. Methadone is almost as effective when administered orally as by injection. In fact, injection of methadone does not result in a "rush" as with some other strong opioids such as morphine or hydromorphone, because its extraordinarily high volume of distribution causes it to diffuse into other tissues in the body, particularly fatty tissue; the peak concentration in the blood is achieved at roughly the same time, whether the drug is injected or ingested. When injecting Methadone, only pills have the least-dangerous cautions although it can easily cause collapsed veins, bruising, swelling and possibly other harmful effects. Methadone pills often contain talc[50][51] that, when injected, produces a swarm of tiny solid particles in the blood, causing numerous minor blood clots. These particles cannot be filtered out before injection, and will accumulate in the body over time, especially in the lungs and eyes, producing various complications such as pulmonary hypertension, an irreversible and progressive disease.[52][53][54] Methadose/Methadone should not be injected either.[55] While it has been done in extremely diluted concentrations, instances of cardiac arrest have been reported as well as damaged veins from sugar and other ingredients (Sugar-Free syrups also should not be injected). Oral medication offers safety, simplicity and represents a step away from injection-based drug abuse in those recovering from addiction. U.S. federal regulations require the oral form in addiction treatment programs.[56]
History
 40mg of Methadone
40mg of MethadoneMethadone was developed in 1937 in Germany by scientists working for I.G. Farbenindustrie AG at the Farbwerke Hoechst (it is synthesised from 1,1-diphenylbutane-2-sulfonic acid and dimethylamino-2-chloropropane) who were looking for a synthetic opioid that could be created with readily available precursors, to solve Germany's opium shortage problem.[57] The reason for its swift abandonment as an alternative to morphine was due to the adverse effects it had on German soldiers during early trials. In contrast to morphine, which was used to alleviate pain in the injured but also to boost the esteem, stamina, and drive of German soldiers in combat, methadone had effects that have been described as such; "Dolophine (Methadone) had many adverse effects on the soldiers to whom it was given, leading to apathy, lethargy, and decreased willingness to engage in combat".
On September 11, 1941 Bockmühl and Ehrhart filed an application for a patent for a synthetic substance they called Hoechst 10820 or polamidon (a name still in regular use in Germany) and whose structure had only slight relation to morphine or the opiate alkaloids (Bockmühl and Ehrhart, 1949).
After the war, all German patents, trade names and research records were requisitioned and expropriated by the Allies. The records on the research work of the I.G. Farbenkonzern at the Farbwerke Hoechst were confiscated by the U.S. Department of Commerce Intelligence, investigated by a Technical Industrial Committee of the U.S. Department of State and then brought to the US.
It was only in 1947 that the drug was given the generic name “methadone” by the Council on Pharmacy and Chemistry of the American Medical Association (COUNCIL...1947). Since the patent rights of the I.G. Farbenkonzern and Farbwerke Hoechst were no longer protected each pharmaceutical company interested in the formula could buy the rights for commercial production of methadone for just one dollar (MOLL 1990).
Methadone was introduced into the United States in 1947 by Eli Lilly and Company as an analgesic (they gave it the trade name Dolophine, which is now registered to Roxane Laboratories). Since then, it has been best known for its use in treating narcotic addiction. A great deal of anecdotal evidence was available "on the street" that methadone might prove effective in treating heroin withdrawal and it had even been used in some hospitals. It was not until studies performed at the Rockefeller University in New York City by Professor Vincent Dole, along with Marie Nyswander and Mary Jeanne Kreek, that methadone was systematically studied as a potential substitution therapy. Their studies introduced a sweeping change in the notion that drug addiction was not necessarily a simple character flaw, but rather a disorder to be treated in the same way as other diseases. To date, methadone maintenance therapy has been the most systematically studied and most successful, and most politically polarizing, of any pharmacotherapy for the treatment of drug addiction patients.
Methadone (as Dolophine) was first manufactured in the USA by Eli Lilly and Company Pharmacueticals, who first obtained FDA approval on August 14, 1947, for their Dolophine 5 mg and 10 mg Tablets. Mallinckrodt Pharmaceuticals did not receive approval until December 15, 1947 to manufacture their bulk compounding powder. Mallinckrodt received approval for their branded generic, Methadose, on April 15, 1993 for their 5 mg and 10 mg Methadose Tablets. Mallinckrodt who also makes 5 mg, 10 mg and 40 mg generic tablets in addition to their branded generic Methadose received approval for their plain generic tablets on April 27, 2004.[58]
The results of the early major studies showed methadone could effectively interrupt illicit opioid use and reduce the associated costs to society, findings which have been consistent with later research and backed up by modern knowledge of the psychological, social and pharmacological mechanisms of illicit opioid addiction.
Origin of Dolophine name
A persistent but untrue urban legend claims that the trade name "Dolophine" was coined in tribute to Adolf Hitler by its German creators, and it is sometimes even claimed that the drug was originally named "adolphine" or "adolophine" or "Dolphamine". The claim is still presented as fact by Church of Scientology literature and was repeated by actor and vocal Scientologist Tom Cruise in a 2005 Entertainment Weekly interview.[59] However, as the magazine pointed out, this is not true: the name "Dolophine" was in fact created after the war by the American branch of Eli Lilly,[60] and the pejorative term "adolphine" (never an actual name of the drug) appeared in the United States in the early 1970s.[61]
Similar drugs
See also: Heroin-assisted Treatment and BuprenorphineThere are two methadone isomers that form the racemic mixture which is more common as it is cheaper to produce. The laevorotary isomer, which is isolated by several recrystalisations from racemic methadone, is more expensive to produce than the racemate. It is more potent at the opioid receptor than the racemic mixture and is marketed especially in continental Europe as an analgesic under the trade names Levo-Polamidone, Polamidone, Heptanone, Heptadone, Heptadon and others. It is used as the hydrochloride salt almost exclusively with some uncommon pharmaceuticals and research subjects consisting of the tartrate. The dextrorotary isomer d-methadone is not commercially available. It is devoid of opioid activity and it acts as an NMDA antagonist. It has been shown to be analgesic in experimental models of chronic pain. Clinical trials of d-methadone, to test its analgesic efficacy against neuropathic pain are in progress.
The closest chemical relative of methadone in clinical use is levo-α-acetylmethadol or LAAM. It has a longer duration of action (from 48 to 72 hours), permitting a reduction in frequency of use. In 1994, it was approved as a narcotic addiction treatment. In the Netherlands, like methadone and all other strong opioids, LAAM is a List I drug of the Opium Law, and in Schedule II of the United States Controlled Substances Act. LAAM has since been removed from the US and European markets due to reports of rare cardiac side effects.
Other drugs which are not structurally related to methadone are also used in maintenance treatment, particularly Subutex (buprenorphine) and Suboxone (buprenorphine combined with naloxone). In the NL, Switzerland, the UK and a few other European countries, however, not only buprenorphine and oral methadone but also injectable methadone and pharmaceutical diamorphine (heroin) or other opioids may be used for outpatient maintenance treatment of opiate addiction, and treatment is generally provided in much less heavily regulated environments than in the United States. In the United Kingdom, diamorhpine is used extremely selectively and is not available on prescription to addicts; except in specialist trials which involved no more than 300 participants. A study from Austria indicated that slow release oral morphine (in the form of MS-Contin) under trade names Substitol-Retard and Compensan, provide better results than oral methadone, and studies of heroin maintenance have indicated that a low background dose of methadone combined with heroin maintenance may significantly improve outcomes for less-responsive patients.[62] Since the late 90s in Austria, slow release oral morphine has been used alongside methadone and buprenorphine for OST and more recently it has been approved in Slovenia and Bulgaria, and it has gained approval in other EU nations including the United Kingdom, although its use is not as of yet not as widespread. The more attractive side effect profile of morphine compared to buprenorphine or methadone has led to the adoption of morphine as an OST treatment option, and currently in Vienna over 60 percent of substitution therapy utilizes slow release oral morphine. Illicit diversion has been a problem, but to the many proponents of the utilization of morphine for OST, the benefits far outweigh the costs, taking into account the much higher percentage of addicts who are "held" or, from another perspective, satisfied by this treatment option, as opposed to methadone and buprenorphine treated addicts, who are more likely to forgo their treatment and revert to using heroin etc., in many cases by selling their methadone or buprenorphine prescriptions to afford their opiate of choice. Driving impairment tests done in the Netherlands that have shown morphine to have the least negative effects on cognitive ability on a number of mental tasks also suggest morphines use in OST may allow for better psychological functioning and engagement in society. Other opiates such as dihydrocodeine in both extended-release and immediate-release form are also sometimes used for maintenance treatment as an alternative to methadone or buprenorphine in some European countries.[63]
Another close relative of methadone is dextropropoxyphene, first marketed in 1957 under the trade name of Darvon. Oral analgesic potency is one-half to one-third that of codeine, with 65 mg approximately equivalent to about 600 mg of aspirin. Dextropropoxyphene is prescribed for relief of mild to moderate pain. Bulk dextropropoxyphene is in Schedule II of the United States Controlled Substances Act, while preparations containing it are in Schedule IV. More than 100 tons of dextropropoxyphene are produced in the United States annually, and more than 25 million prescriptions are written for the products. Since dextropropoxyphene produces relatively modest pain relief compared to other opioids but still produces severe respiratory depression at high doses, it is particularly dangerous when abused, as drug users may take dangerously high doses in an attempt to achieve narcotic effects. This narcotic is among the top 10 drugs reported by medical examiners in recreational drug use deaths. However, dextropropoxyphene is still prescribed for the short term relief of opiate withdrawal symptoms, particularly when the aim of treatment is to smooth detoxification to a drug free state rather than a switch to maintenance treatment.
Other analogues of methadone which are still in clinical use are dipipanone (Diconal) and dextromoramide (Palfium) which are shorter-lasting but considerably more effective as analgesics. In the 1980s and beginning of the 1990s, before pharmaceutical grade IV heroin treatment became available to heroin addicts, as either single drug replacement for street heroin, or to be used alongside prescribed methadone, oral dextromoramide was prescribed to heroin addicts instead, because even when taken orally it still produces a strong, so called "rush", without the need of IV administration and any of the risks involved with it. These drugs have a high potential for abuse and dependence and were notorious for being widely abused and sought after by drug addicts in the 1970s. They are still rarely used for the relief of severe pain in the treatment of terminal cancer or other serious medical conditions. Different nations within the EU have different regulations, and in some nations general practitioners have the legal right to maintain addicts with whatever they deem to be most efficacious in maintaining their health and well being.
Notes
- ^ "Methadone Pregnancy and Breastfeeding Warnings". http://www.drugs.com/pregnancy/methadone.html. Retrieved 11-08-2011.
- ^ Pharmaceuticals.Mallinckrodt.com
- ^ a b c d e Joseph H, Stancliff S, Langrod J (2000). "Methadone maintenance treatment (MMT): a review of historical and clinical issues". Mt. Sinai J. Med. 67 (5-6): 347–64. PMID 11064485.
- ^ Connock M, Juarez-Garcia A, Jowett S, et al. (2007). "Methadone and buprenorphine for the management of opioid dependence: a systematic review and economic evaluation". Health technology assessment (Winchester, England) 11 (9): 1–171, iii–iv. PMID 17313907.
- ^ M Schwirtz. "Russia Scorns Methadone for Heroin Addiction." The New York Times. July 22, 2008.
- ^ Joseph, R.; Moselhy, H.F. (2005). "National survey of methadone prescribing for maintenance treatment: 'opiophobia' among substance misuse services?". Psychiatric Bulletin 29 (12): 459–461. doi:10.1192/pb.29.12.459.
- ^ Donny EC, Brasser SM, Bigelow GE, Stitzer ML, Walsh SL (2005). "Methadone doses of 100 mg or greater are more effective than lower doses at suppressing heroin self-administration in opioid-dependent volunteers". Addiction 100 (10): 1496–509. doi:10.1111/j.1360-0443.2005.01232.x. PMID 16185211.
- ^ Latowsky M (2006). "Methadone death, dosage and torsade de pointes: risk-benefit policy implications". Journal of psychoactive drugs 38 (4): 513–9. PMID 17373567.
- ^ Leavitt SB, Shinderman M, Maxwell S, Eap CB, Paris P (2000). "When "Enough" Is Not Enough: New Perspectives on Optimal Methadone Maintenance Dose". Mount Sinai Journal of Medicine 67 (5&6): 404–411.
- ^ Faggiano F, Vigna-Taglianti F, Versino E, Lemma P (2003). "Methadone maintenance at different dosages for opioid dependence". Cochrane database of systematic reviews (3): CD002208. doi:10.1002/14651858.CD002208. PMID 12917925.
- ^ "Centre for Addiction and Mental Health". The Centre for Addiction and Mental Health. http://www.camh.net/Care_Treatment/Resources_clients_families_friends/Methadone_Maintenance_Treatment/mmt_clienthndbk_ch8.html.
- ^ "Tapering Off of Methadone Maintenance: Evidence-Based Guidelines". "Aegis Medical Systems". http://www.aegisuniversity.com/Aegis%20Documents/Tapering%20off%20of%20Methadone%20Maintenance%205-24-02.pdf.
- ^ "Methadone Maintenance Program Overview". The College Of Pharmacists Of British Columbia ("The College Of BC Pharmacists"). http://www.bcpharmacists.org/library/H-Resources/H-4_Pharmacy_Resources/5058-Methadone_Maintenance_Program_Overview.pdf.
- ^ "METHADONE HYDROCHLORIDE TABLETS USP Prescribing Information". Mallinckrodt. http://pharmaceuticals.mallinckrodt.com/_attachments/PackageInserts/18_Methadone%20Hydrochloride%20Tab_REV011309.pdf.
- ^ "Best Practices Methadone Maintenance Treatment". Office of Canada’s Drug Strategy Health Canada. http://www.hc-sc.gc.ca/hl-vs/alt_formats/hecs-sesc/pdf/pubs/adp-apd/methadone-bp-mp/methadone-bp-mp-eng.pdf.
- ^ "Methadone Maintenance Treatment Translating Research Into Policy". Canadian Department Of Health And Human Services. http://edocs.lib.sfu.ca/projects/chodarr/documents/chodarr1448.pdf.
- ^ "Methadone Maintenance Treatment". Drug Policy Alliance Lindesmith Library. http://www.drugpolicy.org/library/research/methadone.cfm.
- ^ "Methadone Research Web Guide". NIDA. http://international.drugabuse.gov/collaboration/guide_methadone/partb_question15.html.
- ^ Leppert, W. . (2009). "The role of methadone in cancer pain treatment--a review". International journal of clinical practice 63 (7): 1095–1109. doi:10.1111/j.1742-1241.2008.01990.x. PMID 19570126.
- ^ Lynch, M. E. (2005). "A review of the use of methadone for the treatment of chronic noncancer pain". Pain research & management : the journal of the Canadian Pain Society = journal de la societe canadienne pour le traitement de la douleur 10 (3): 133–144. PMID 16175249.
- ^ Toombs, J. D.; Kral, L. A. (2005). "Methadone treatment for pain states". American family physician 71 (7): 1353–1358. PMID 15832538.
- ^ "Oral Methadone Dosing For Pain". Pain Treatment Topics. http://pain-topics.org/pdf/OralMethadoneDosing.pdf.
- ^ "2006 Safety Alerts for Drugs, Biologics, Medical Devices, and Dietary Supplements". MedWatch. Food and Drug Administration. http://www.fda.gov/medwatch/safety/2006/safety06.htm#Methadone.
- ^ Maremmani I, Pacini M, Cesaroni C, Lovrecic M, Perugi G, Tagliamonte A (2005). "QTc interval prolongation in patients on long-term methadone maintenance therapy". European addiction research 11 (1): 44–9. doi:10.1159/000081416. PMID 15608471.
- ^ a b John, J.; Amley, X.; Bombino, G.; Gitelis, C.; Topi, B.; Hollander, G.; Ghosh, J. (2010). "Torsade de Pointes due to Methadone Use in a Patient with HIV and Hepatitis C Coinfection". Cardiology Research and Practice 2010: 1–4. doi:10.4061/2010/524764. PMC 3021856. PMID 21253542. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=3021856.
- ^ "Opioid rotation for toxicity reduction in terminal cancer patients". Journal of Pain and Symptom Management. Volume 10, Issue 5, July 1995, Pages 378-384. http://www.sciencedirect.com/science?_ob=ArticleURL&_udi=B6T8R-3XY2J9W-11&_user=10&_rdoc=1&_fmt=&_orig=search&_sort=d&_docanchor=&view=c&_acct=C000050221&_version=1&_urlVersion=0&_userid=10&md5=54eb39149b9c23a294574034d3527cb2.
- ^ "Individualized use of methadone and opioid rotation in the comprehensive management of cancer pain associated with poor prognostic indicators". <pain. Elsevier, Amsterdam, PAYS-BAS, 1996, vol. 67, no1, pp. 115-119 (30 ref.). http://cat.inist.fr/?aModele=afficheN&cpsidt=3220887.
- ^ "Pitfalls of opioid rotation: substituting another opioid for methadone in patients with cancer pain". <pain. 96 (2002) 325–328. http://www.schmerzkrank.de/images/opioid_rotation.pdf.
- ^ Claudia Friesen, Mareike Roscher, Andreas Alt and Erich Miltner (2008). "Methadone, Commonly Used as Maintenance Medication for Outpatient Treatment of Opioid Dependence, Kills Leukemia Cells and Overcomes Chemoresistance". Cancer Research 68 (15): 6059–64. doi:10.1158/0008-5472.CAN-08-1227. PMID 18676827.
- ^ a b Public Health Issue: Methadone Maintenance Therapy RICHARD SADOVSKY, M.D. - Anderson IB, Kearney TE. Use of methadone. West J Med January 2000;172:43-6.
- ^ "Dolophine Drug Description". RxList. http://www.rxlist.com/cgi/generic/methdone.htm.
- ^ "Methadone". MedlinePlus. Archived from the original on 2008-02-27. http://web.archive.org/web/20080227025738/http://www.nlm.nih.gov/medlineplus/druginfo/medmaster/a682134.html.
- ^ "Methadone". Drugs.com. http://www.drugs.com/methadone.html.
- ^ "Methadone". MedicineNet. http://www.medicinenet.com/methadone-dispersible_tablet/article.htm.
- ^ R. Baselt, Disposition of Toxic Drugs and Chemicals in Man, 8th edition, Biomedical Publications, Foster City, CA, 2008, pp. 941-945.
- ^ "Increases in Methadone-Related Deaths:1999-2004". http://www.cdc.gov/nchs/products/pubs/pubd/hestats/methadone1999-04/methadone1999-04.htm.
- ^ "The Killer Cure" The Charleston Gazette 2006
- ^ "Methadone-Associated Mortality, Report of a National Assessment". http://alcoholism.about.com/cs/heroin/a/blsam040209.htm.
- ^ [1] Charleston Gazette, "New warning issued on methadone", Nov. 28, 2006
- ^ Giacomuzzi SM, Ertl M, Vigl A, et al. (July 2005). "Driving capacity of patients treated with methadone and slow-release oral morphine". Addiction 100 (7): 1027. doi:10.1111/j.1360-0443.2005.01148.x. PMID 15955021. http://onlinelibrary.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=0965-2140&date=2005&volume=100&issue=7&spage=1027.
- ^ Reece AS (2008). "Experience of road and other trauma by the opiate dependent patient: a survey report". Subst Abuse Treat Prev Policy 3: 10. doi:10.1186/1747-597X-3-10. PMC 2396610. PMID 18454868. http://www.substanceabusepolicy.com/content/3//10.
- ^ [2]
- ^ Addiction Treatment Forum
- ^ "Methadone, Methadone Addiction & Methadone Side Effects By Narconon Arrowhead & Heroin Addiction". http://www.heroinaddiction.com/heroin_methadone.html. Retrieved 31 October 2008.
- ^ Xiao Y, Smith RD, Caruso FS, Kellar KJ (October 2001). "Blockade of Rat α3β4 Nicotinic Receptor Function by Methadone, Its Metabolites, and Structural Analogs". J. Pharmacol. Exp. Ther. 299 (1): 366–71. PMID 11561100. http://jpet.aspetjournals.org/cgi/pmidlookup?view=long&pmid=11561100.
- ^ Kell MJ (1994). "Utilization of plasma and urine methadone concentrations to optimize treatment in maintenance clinics: I. Measurement techniques for a clinical setting". Journal of addictive diseases: the official journal of the ASAM, American Society of Addiction Medicine 13 (1): 5–26. PMID 8018740.
- ^ Eap CB, DeglonJ-J, Boumann P. (1999). "Pharmacokinetics and pharmacogenetics of methadone: Clinical relevance". Heroin Addiction and Related Clinical Problems: the official journal of EUROPAD, European Opiate Addiction Treatment Association 1 (1): 19–34.
- ^ a b c Eap CB, Buclin T, Baumann P (2002). "Interindividual variability of the clinical pharmacokinetics of methadone: implications for the treatment of opioid dependence". Clinical pharmacokinetics 41 (14): 1153–93. PMID 12405865.
- ^ Manfredonia, John (March 2005). "Prescribing Methadone for Pain Management in End-of-Life Care". JAOA The Journal of the American Osteopathic Association 105. http://www.jaoa.org/cgi/content/full/105/3_suppl/18S.
- ^ "Methadone Hydrochloride Tablets, USP". VistaPharm. http://www.vistapharm.com/methadone_tablets.pdf.
- ^ "Talc retinopathy.". Can J Ophthalmol.. http://www.ncbi.nlm.nih.gov/pubmed/698886.
- ^ "Talc lung in a drug abuser". Springer London. http://www.springerlink.com/content/p4n0q25732v4g620/.
- ^ "Pulmonary Hypertension and Risk of Death in Cardiomyopathy". Circulation. http://circ.ahajournals.org/cgi/content/full/circulationaha;105/14/1663.
- ^ "Improving survival in pulmonary arterial hypertension". European Respiratory Journal. http://www.erj.ersjournals.com/cgi/content/full/25/2/218.
- ^ Nicholas Lintzeris, Michael Lenne, Alison Ritter (1999). "Methadone injecting in Australia: A Tale of Two Cities". Addiction 94 (8): 1175–1178. doi:10.1046/j.1360-0443.1999.94811757.x. PMID 10615732.
- ^ Code of Federal Regulations, Title 42, Sec 8.
- ^ M. Bockmuhl, Über eine neue Klasse von analgetisch wirkenden Verbindungen Ann. Chem. 561, 52 (1948)
- ^ Accessdata.FDA.gov
- ^ Tom Responds, Entertainment Weekly, May 11, 2005
- ^ "Methadone Briefing". Archived from the original on 2003-11-20. http://web.archive.org/web/20031120200050/http://www.exchangesupplies.org/publications/methadone_briefing/section1.html. Retrieved 2007-07-09.
- ^ Indro-Online.de (PDF format)
- ^ Michels II, Stöver H, Gerlach R (2007). "Substitution treatment for opioid addicts in Germany". Harm Reduct J 4: 5. doi:10.1186/1477-7517-4-5. PMC 1797169. PMID 17270059. http://www.harmreductionjournal.com/content/4//5.
- ^ Robertson JR, Raab GM, Bruce M, McKenzie JS, Storkey HR, Salter A (December 2006). "Addressing the efficacy of dihydrocodeine versus methadone as an alternative maintenance treatment for opiate dependence: A randomized controlled trial". Addiction 101 (12): 1752–9. doi:10.1111/j.1360-0443.2006.01603.x. PMID 17156174. http://onlinelibrary.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=0965-2140&date=2006&volume=101&issue=12&spage=1752.
External links
- ONDCP Fact Sheet
- Clinic Locator, United States
- DHHS, Centers for Disease Control and Prevention (CDC)
- Methadone.org
- Methadone Support Org - Pregnancy, Methadone Anonymous (MA)
- TAPERING OFF OF METHADONE MAINTENANCE: EVIDENCE-BASED GUIDELINES
- Methadone Package Insert
- BEST PRACTICES: Methadone Maintenance Treatment
- U.S. National Library of Medicine: Drug Information Portal - Methadone
- Methadone.us: A resource center on opioid addiction treatment
Antiaddictives (N07B) Nicotine dependence/
(Nicotinic agonist)Nicotine • Dianicline • Varenicline • Lobeline • Mecamylamine • Scopolamine
NDRI (Bupropion) • AA (Clonidine) • CB1 (Surinabant)Alcohol dependence Opioid dependence Buprenorphine • Methadone • Levacetylmethadol • Dihydrocodeine • Dihydroetorphine • AA (Clonidine) • Lofexidine • Extended Release Morphine • Extended Release Hydromorphone • Baclofen • IbogaineStimulant dependence Benzodiazepine dependence Cocaine dependence Sedative-Hypnotic dependence Cholinergics Receptor ligands Agonists: 77-LH-28-1 • AC-42 • AC-260,584 • Aceclidine • Acetylcholine • AF30 • AF150(S) • AF267B • AFDX-384 • Alvameline • AQRA-741 • Arecoline • Bethanechol • Butyrylcholine • Carbachol • CDD-0034 • CDD-0078 • CDD-0097 • CDD-0098 • CDD-0102 • Cevimeline • cis-Dioxolane • Ethoxysebacylcholine • LY-593,039 • L-689,660 • LY-2,033,298 • McNA343 • Methacholine • Milameline • Muscarine • NGX-267 • Ocvimeline • Oxotremorine • PD-151,832 • Pilocarpine • RS86 • Sabcomeline • SDZ 210-086 • Sebacylcholine • Suberylcholine • Talsaclidine • Tazomeline • Thiopilocarpine • Vedaclidine • VU-0029767 • VU-0090157 • VU-0152099 • VU-0152100 • VU-0238429 • WAY-132,983 • Xanomeline • YM-796
Antagonists: 3-Quinuclidinyl Benzilate • 4-DAMP • Aclidinium Bromide • Anisodamine • Anisodine • Atropine • Atropine Methonitrate • Benactyzine • Benzatropine (Benztropine) • Benzydamine • BIBN 99 • Biperiden • Bornaprine • CAR-226,086 • CAR-301,060 • CAR-302,196 • CAR-302,282 • CAR-302,368 • CAR-302,537 • CAR-302,668 • CS-27349 • Cyclobenzaprine • Cyclopentolate • Darifenacin • DAU-5884 • Dimethindene • Dexetimide • DIBD • Dicyclomine (Dicycloverine) • Ditran • EA-3167 • EA-3443 • EA-3580 • EA-3834 • Elemicin • Etanautine • Etybenzatropine (Ethylbenztropine) • Flavoxate • Himbacine • HL-031,120 • Ipratropium bromide • J-104,129 • Hyoscyamine • Mamba Toxin 3 • Mamba Toxin 7 • Mazaticol • Mebeverine • Methoctramine • Metixene • Myristicin • N-Ethyl-3-Piperidyl Benzilate • N-Methyl-3-Piperidyl Benzilate • Orphenadrine • Otenzepad • Oxybutynin • PBID • PD-102,807 • PD-0298029 • Phenglutarimide • Phenyltoloxamine • Pirenzepine • Piroheptine • Procyclidine • Profenamine • RU-47,213 • SCH-57,790 • SCH-72,788 • SCH-217,443 • Scopolamine (Hyoscine) • Solifenacin • Telenzepine • Tiotropium bromide • Tolterodine • Trihexyphenidyl • Tripitamine • Tropatepine • Tropicamide • WIN-2299 • Xanomeline • Zamifenacin; Others: 1st Generation Antihistamines (Brompheniramine, chlorphenamine, cyproheptadine, dimenhydrinate, diphenhydramine, doxylamine, mepyramine/pyrilamine, phenindamine, pheniramine, tripelennamine, triprolidine, etc) • Tricyclic Antidepressants (Amitriptyline, doxepin, trimipramine, etc) • Tetracyclic Antidepressants (Amoxapine, maprotiline, etc) • Typical Antipsychotics (Chlorpromazine, thioridazine, etc) • Atypical Antipsychotics (Clozapine, olanzapine, quetiapine, etc)Agonists: 5-HIAA • A-84,543 • A-366,833 • A-582,941 • A-867,744 • ABT-202 • ABT-418 • ABT-560 • ABT-894 • Acetylcholine • Altinicline • Anabasine • Anatoxin-a • AR-R17779 • Butyrylcholine • Carbachol • Cotinine • Cytisine • Decamethonium • Desformylflustrabromine • Dianicline • Dimethylphenylpiperazinium • Epibatidine • Epiboxidine • Ethanol • Ethoxysebacylcholine • EVP-4473 • EVP-6124 • Galantamine • GTS-21 • Ispronicline • Lobeline • MEM-63,908 (RG-3487) • Nicotine • NS-1738 • PHA-543,613 • PHA-709,829 • PNU-120,596 • PNU-282,987 • Pozanicline • Rivanicline • Sazetidine A • Sebacylcholine • SIB-1508Y • SIB-1553A • SSR-180,711 • Suberylcholine • TC-1698 • TC-1734 • TC-1827 • TC-2216 • TC-5214 • TC-5619 • TC-6683 • Tebanicline • Tropisetron • UB-165 • Varenicline • WAY-317,538 • XY-4083
Antagonists: 18-Methoxycoronaridine • α-Bungarotoxin • α-Conotoxin • Alcuronium • Amantadine • Anatruxonium • Atracurium • Bupropion (Amfebutamone) • Chandonium • Chlorisondamine • Cisatracurium • Coclaurine • Coronaridine • Dacuronium • Decamethonium • Dextromethorphan • Dextropropoxyphene • Dextrorphan • Diadonium • DHβE • Dimethyltubocurarine (Metocurine) • Dipyrandium • Dizocilpine (MK-801) • Doxacurium • Duador • Esketamine • Fazadinium • Gallamine • Hexafluronium • Hexamethonium (Benzohexonium) • Ibogaine • Isoflurane • Ketamine • Kynurenic acid • Laudexium (Laudolissin) • Levacetylmethadol • Malouetine • Mecamylamine • Memantine • Methadone • Methorphan (Racemethorphan) • Methyllycaconitine • Metocurine • Mivacurium • Morphanol (Racemorphanol) • Neramexane • Nitrous Oxide • Pancuronium • Pempidine • Pentamine • Pentolinium • Phencyclidine • Pipecuronium • Radafaxine • Rapacuronium • Rocuronium • Surugatoxin • Suxamethonium (Succinylcholine) • Thiocolchicoside • Toxiferine • Trimethaphan • Tropeinium • Tubocurarine • Vecuronium • XenonReuptake inhibitors PlasmalemmalCHT InhibitorsHemicholinium-3 (Hemicholine; HC3) • TriethylcholineVAChT InhibitorsEnzyme inhibitors ChAT inhibitors1-(-Benzoylethyl)pyridinium • 2-(α-Naphthoyl)ethyltrimethylammonium • 3-Chloro-4-stillbazole • 4-(1-Naphthylvinyl)pyridine • Acetylseco hemicholinium-3 • Acryloylcholine • AF64A • B115 • BETA • CM-54,903 • CatabolismAChE inhibitorsReversible: Carbamates: Aldicarb • Bendiocarb • Bufencarb • Carbaryl • Carbendazim • Carbetamide • Carbofuran • Chlorbufam • Chloropropham • Ethienocarb • Ethiofencarb • Fenobucarb • Fenoxycarb • Formetanate • Furadan • Ladostigil • Methiocarb • Methomyl • Miotine • Oxamyl • Phenmedipham • Pinmicarb • Pirimicarb • Propamocarb • Propham • Propoxur; Stigmines: Ganstigmine • Neostigmine • Phenserine • Physostigmine • Pyridostigmine • Rivastigmine; Others: Acotiamide • Ambenonium • Donepezil • Edrophonium • Galantamine • Huperzine A • Minaprine • Tacrine • Zanapezil
Irreversible: Organophosphates: Acephate • Azinphos-methyl • Bensulide • Cadusafos • Chlorethoxyfos • Chlorfenvinphos • Chlorpyrifos • Chlorpyrifos-Methyl • Coumaphos • Cyclosarin (GF) • Demeton • Demeton-S-Methyl • Diazinon • Dichlorvos • Dicrotophos • Diisopropyl fluorophosphate (Guthion) • Diisopropylphosphate • Dimethoate • Dioxathion • Disulfoton • EA-3148 • Echothiophate • Ethion • Ethoprop • Fenamiphos • Fenitrothion • Fenthion • Fosthiazate • GV • Isofluorophate • Isoxathion • Malaoxon • Malathion • Methamidophos • Methidathion • Metrifonate • Mevinphos • Monocrotophos • Naled • Novichok agent • Omethoate • Oxydemeton-Methyl • Paraoxon • Parathion • Parathion-Methyl • Phorate • Phosalone • Phosmet • Phostebupirim • Phoxim • Pirimiphos-Methyl • Sarin (GB) • Soman (GD) • Tabun (GA) • Temefos • Terbufos • Tetrachlorvinphos • Tribufos • Trichlorfon • VE • VG • VM • VR • VX; Others: Demecarium • Onchidal (Onchidella binneyi)BChE inhibitorsCymserine * Many of the acetylcholinesterase inhibitors listed above act as butyrylcholinesterase inhibitors.Others Choline (Lecithin) • Citicoline • Cyprodenate • Dimethylethanolamine (DMAE, deanol) • Glycerophosphocholine • Meclofenoxate (Centrophenoxine) • Phosphatidylcholine • Phosphatidylethanolamine • Phosphorylcholine • PirisudanolOthersAcetylcholine releasing agents: α-Latrotoxin • β-Bungarotoxin; Acetylcholine release inhibitors: Botulinum toxin (Botox); Acetylcholinesterase reactivators: Asoxime • Obidoxime • PralidoximeSerotonergics 5-HT1 receptor ligands Agonists: Azapirones: Alnespirone • Binospirone • Buspirone • Enilospirone • Eptapirone • Gepirone • Ipsapirone • Perospirone • Revospirone • Tandospirone • Tiospirone • Umespirone • Zalospirone; Antidepressants: Etoperidone • Nefazodone • Trazodone • Vortioxetine; Antipsychotics: Aripiprazole • Asenapine • Clozapine • Quetiapine • Ziprasidone; Ergolines: Dihydroergotamine • Ergotamine • Lisuride • Methysergide • LSD; Tryptamines: 5-CT • 5-MeO-DMT • 5-MT • Bufotenin • DMT • Indorenate • Psilocin • Psilocybin; Others: 8-OH-DPAT • Adatanserin • Befiradol • BMY-14802 • Cannabidiol • Dimemebfe • Ebalzotan • Eltoprazine • F-11,461 • F-12,826 • F-13,714 • F-14,679 • F-15,063 • F-15,599 • Flesinoxan • Flibanserin • Lesopitron • LY-293,284 • LY-301,317 • MKC-242 • NBUMP • Osemozotan • Oxaflozane • Pardoprunox • Piclozotan • Rauwolscine • Repinotan • Roxindole • RU-24,969 • S 14,506 • S-14,671 • S-15,535 • Sarizotan • SSR-181,507 • Sunepitron • U-92,016-A • Urapidil • Vilazodone • Xaliproden • Yohimbine
Antagonists: Antipsychotics: Iloperidone • Risperidone • Sertindole; Beta blockers: Alprenolol • Cyanopindolol • Iodocyanopindolol • Oxprenolol • Pindobind • Pindolol • Propranolol • Tertatolol; Others: AV965 • BMY-7,378 • CSP-2503 • Dotarizine • Flopropione • GR-46611 • Isamoltane • Lecozotan • Mefway • Metitepine/Methiothepin • MPPF • NAN-190 • PRX-00023 • Robalzotan • S-15535 • SB-649,915 • SDZ 216-525 • Spiperone • Spiramide • Spiroxatrine • UH-301 • WAY-100,135 • WAY-100,635 • XylamidineAgonists: Lysergamides: Dihydroergotamine • Ergotamine • Methysergide; Piperazines: Eltoprazine • TFMPP; Triptans: Avitriptan • Eletriptan • Sumatriptan • Zolmitriptan; Tryptamines: 5-CT • 5-MT; Others: CGS-12066A • CP-93,129 • CP-94,253 • CP-135,807 • RU-24,969 • Vortioxetine
Antagonists: Lysergamides: Metergoline; Others: AR-A000002 • Elzasonan • GR-127,935 • Isamoltane • Metitepine/Methiothepin • SB-216,641 • SB-224,289 • SB-236,057 • YohimbineAgonists: Lysergamides: Dihydroergotamine • Methysergide; Triptans: Almotriptan • Avitriptan • Eletriptan • Frovatriptan • Naratriptan • Rizatriptan • Sumatriptan • Zolmitriptan; Tryptamines: 5-CT • 5-Ethyl-DMT • 5-MT • 5-(Nonyloxy)tryptamine; Others: CP-135,807 • CP-286,601 • GR-46611 • L-694,247 • L-772,405 • PNU-109,291 • PNU-142,633
Antagonists: Lysergamides: Metergoline; Others: Alniditan • BRL-15,572 • Elzasonan • GR-127,935 • Ketanserin • LY-310,762 • LY-367,642 • LY-456,219 • LY-456,220 • Metitepine/Methiothepin • Ritanserin • Yohimbine • ZiprasidoneAgonists: Lysergamides: Methysergide; Triptans: Eletriptan; Tryptamines: BRL-54443 • Tryptamine
Antagonists: Metitepine/MethiothepinAgonists: Triptans: Eletriptan • Naratriptan • Sumatriptan; Tryptamines: 5-MT; Others: BRL-54443 • Lasmiditan • LY-334,370
Antagonists: Metitepine/Methiothepin5-HT2 receptor ligands Agonists: Lysergamides: ALD-52 • Ergometrine • Lisuride • LA-SS-Az • LSD • LSD-Pip • Lysergic acid 2-butyl amide • Lysergic acid 3-pentyl amide • Methysergide; Phenethylamines: 25I-NBF • 25I-NBMD • 25I-NBOH • 25I-NBOMe • 2C-B • 2C-B-FLY • 2CB-Ind • 2C-C-NBOMe • 2C-E • 2C-I • 2C-TFM-NBOMe • 2C-T-2 • 2C-T-7 • 2C-T-21 • 2CBCB-NBOMe • 2CBFly-NBOMe • Bromo-DragonFLY • DOB • DOC • DOI • DOM • MDA • MDMA • Mescaline • TCB-2 • TFMFly; Piperazines: BZP • Quipazine • TFMPP; Tryptamines: 5-CT • 5-MeO-α-ET • 5-MeO-α-MT • 5-MeO-DET • 5-MeO-DiPT • 5-MeO-DMT • 5-MeO-DPT • 5-MT • α-ET • α-Methyl-5-HT • α-MT • Bufotenin • DET • DiPT • DMT • DPT • Psilocin • Psilocybin; Others: AL-34662 • AL-37350A • Dimemebfe • Medifoxamine • Oxaflozane • PNU-22394 • RH-34
Antagonists: Atypical antipsychotics: Amperozide • Aripiprazole • Carpipramine • Clocapramine • Clozapine • Gevotroline • Iloperidone • Melperone • Mosapramine • Olanzapine • Paliperidone • Pimozide • Quetiapine • Risperidone • Sertindole • Ziprasidone • Zotepine; Typical antipsychotics: Loxapine • Pipamperone; Antidepressants: Amitriptyline • Amoxapine • Aptazapine • Etoperidone • Mianserin • Mirtazapine • Nefazodone • Teniloxazine • Trazodone; Others: 5-I-R91150 • AC-90179 • Adatanserin • Altanserin • AMDA • APD-215 • Blonanserin • Cinanserin • CSP-2503 • Cyproheptadine • Deramciclane • Dotarizine • Eplivanserin • Esmirtazapine • Fananserin • Flibanserin • Ketanserin • KML-010 • Lubazodone • Mepiprazole • Metitepine/Methiothepin • Nantenine • Pimavanserin • Pizotifen • Pruvanserin • Rauwolscine • Ritanserin • S-14,671 • Sarpogrelate • Setoperone • Spiperone • Spiramide • SR-46349B • Volinanserin • Xylamidine • YohimbineAgonists: Oxazolines: 4-Methylaminorex • Aminorex; Phenethylamines: Chlorphentermine • Cloforex • DOB • DOC • DOI • DOM • Fenfluramine • MDA • MDMA • Norfenfluramine; Tryptamines: 5-CT • 5-MT • α-Methyl-5-HT; Others: BW-723C86 • Cabergoline • mCPP • Pergolide • PNU-22394 • Ro60-0175
Antagonists: Agomelatine • Asenapine • EGIS-7625 • Ketanserin • Lisuride • LY-272,015 • Metitepine/Methiothepin • PRX-08066 • Rauwolscine • Ritanserin • RS-127,445 • Sarpogrelate • SB-200,646 • SB-204,741 • SB-206,553 • SB-215,505 • SB-221,284 • SB-228,357 • SDZ SER-082 • Tegaserod • YohimbineAgonists: Phenethylamines: 2C-B • 2C-E • 2C-I • 2C-T-2 • 2C-T-7 • 2C-T-21 • DOB • DOC • DOI • DOM • MDA • MDMA • Mescaline; Piperazines: Aripiprazole • mCPP • TFMPP; Tryptamines: 5-CT • 5-MeO-α-ET • 5-MeO-α-MT • 5-MeO-DET • 5-MeO-DiPT • 5-MeO-DMT • 5-MeO-DPT • 5-MT • α-ET • α-Methyl-5-HT • α-MT • Bufotenin • DET • DiPT • DMT • DPT • Psilocin • Psilocybin; Others: A-372,159 • AL-38022A • CP-809,101 • Dimemebfe • Lorcaserin• Medifoxamine • MK-212 • Org 12,962 • ORG-37,684 • Oxaflozane • PNU-22394 • Ro60-0175 • Ro60-0213 • Vabicaserin • WAY-629 • WAY-161,503 • YM-348
Antagonists: Atypical antipsychotics: Clozapine • Iloperidone • Melperone • Olanzapine • Paliperidone • Pimozide • Quetiapine • Risperidone • Sertindole • Ziprasidone • Zotepine; Typical antipsychotics: Chlorpromazine • Loxapine • Pipamperone; Antidepressants: Agomelatine • Amitriptyline • Amoxapine • Aptazapine • Etoperidone • Fluoxetine • Mianserin • Mirtazapine • Nefazodone • Nortriptyline • Tedatioxetine • Trazodone; Others: Adatanserin • Cinanserin • Cyproheptadine • Deramciclane • Dotarizine • Eltoprazine • Esmirtazapine • FR-260,010 • Ketanserin • Ketotifen • Latrepirdine • Metitepine/Methiothepin • Methysergide • Pizotifen • Ritanserin • RS-102,221 • S-14,671 • SB-200,646 • SB-206,553 • SB-221,284 • SB-228,357 • SB-242,084 • SB-243,213 • SDZ SER-082 • Xylamidine5-HT3, 5-HT4, 5-HT5, 5-HT6, 5-HT7 ligands Agonists: Piperazines: BZP • Quipazine; Tryptamines: 2-Methyl-5-HT • 5-CT; Others: Chlorophenylbiguanide • Butanol • Ethanol • Halothane • Isoflurane • RS-56812 • SR-57,227 • SR-57,227-A • Toluene • Trichloroethane • Trichloroethanol • Trichloroethylene • YM-31636
Antagonists: Antiemetics: AS-8112 • Alosetron • Azasetron • Batanopride • Bemesetron • Cilansetron • Dazopride • Dolasetron • Granisetron • Lerisetron • Ondansetron • Palonosetron • Ramosetron • Renzapride • Tropisetron • Zacopride • Zatosetron; Atypical antipsychotics: Clozapine • Olanzapine • Quetiapine; Tetracyclic antidepressants: Amoxapine • Mianserin • Mirtazapine; Others: CSP-2503 • ICS-205,930 • MDL-72,222 • Memantine • Nitrous Oxide • Ricasetron • Sevoflurane • Tedatioxetine • Thujone • Vortioxetine • XenonAgonists: Gastroprokinetic Agents: Cinitapride • Cisapride • Dazopride • Metoclopramide • Mosapride • Prucalopride • Renzapride • Tegaserod • Velusetrag • Zacopride; Others: 5-MT • BIMU8 • CJ-033,466 • PRX-03140 • RS-67333 • RS-67506 • SL65.0155 • Antagonists: GR-113,808 • GR-125,487 • L-Lysine • Piboserod • RS-39604 • RS-67532 • SB-203,186 • SB-204,070Agonists: Lysergamides: Ergotamine • LSD; Tryptamines: 5-CT; Others: Valerenic Acid
Antagonists: Asenapine • Latrepirdine • Metitepine/Methiothepin • Ritanserin • SB-699,551
* Note that the 5-HT5B receptor is not functional in humans.Agonists: Lysergamides: Dihydroergotamine • Ergotamine • Lisuride • LSD • Mesulergine • Metergoline • Methysergide; Tryptamines: 2-Methyl-5-HT • 5-BT • 5-CT • 5-MT • Bufotenin • E-6801 • E-6837 • EMD-386,088 • EMDT • LY-586,713 • Tryptamine; Others: WAY-181,187 • WAY-208,466
Antagonists: Antidepressants: Amitriptyline • Amoxapine • Clomipramine • Doxepin • Mianserin • Nortriptyline; Atypical antipsychotics: Aripiprazole • Asenapine • Clozapine • Fluperlapine • Iloperidone • Olanzapine • Tiospirone; Typical antipsychotics: Chlorpromazine • Loxapine; Others: BGC20-760 • BVT-5182 • BVT-74316 • Cerlapirdine • EGIS-12,233 • GW-742,457 • Ketanserin • Latrepirdine • Lu AE58054 • Metitepine/Methiothepin • MS-245 • PRX-07034 • Ritanserin • Ro04-6790 • Ro 63-0563 • SB-258,585 • SB-271,046 • SB-357,134 • SB-399,885 • SB-742,457Agonists: Lysergamides: LSD; Tryptamines: 5-CT • 5-MT • Bufotenin; Others: 8-OH-DPAT • AS-19 • Bifeprunox • E-55888 • LP-12 • LP-44 • RU-24,969 • Sarizotan
Antagonists: Lysergamides: 2-Bromo-LSD • Bromocriptine • Dihydroergotamine • Ergotamine • Mesulergine • Metergoline • Methysergide; Antidepressants: Amitriptyline • Amoxapine • Clomipramine • Imipramine • Maprotiline • Mianserin; Atypical antipsychotics: Amisulpride • Aripiprazole • Clozapine • Olanzapine • Risperidone • Sertindole • Tiospirone • Ziprasidone • Zotepine; Typical antipsychotics: Chlorpromazine • Loxapine; Others: Butaclamol • EGIS-12,233 • Ketanserin • LY-215,840 • Metitepine/Methiothepin • Pimozide • Ritanserin • SB-258,719 • SB-258,741 • SB-269,970 • SB-656,104 • SB-656,104-A • SB-691,673 • SLV-313 • SLV-314 • Spiperone • SSR-181,507 • VortioxetineReuptake inhibitors Selective serotonin reuptake inhibitors (SSRIs): Alaproclate • Citalopram • Dapoxetine • Desmethylcitalopram • Desmethylsertraline • Escitalopram • Femoxetine • Fluoxetine • Fluvoxamine • Indalpine • Ifoxetine • Litoxetine • Lubazodone • Panuramine • Paroxetine • Pirandamine • RTI-353 • Seproxetine • Sertraline • Tedatioxetine • Vilazodone • Vortioxetine • Zimelidine; Serotonin-norepinephrine reuptake inhibitors (SNRIs): Bicifadine • Desvenlafaxine • Duloxetine • Eclanamine • Levomilnacipran • Milnacipran • Sibutramine • Venlafaxine; Serotonin-norepinephrine-dopamine reuptake inhibitors (SNDRIs): Brasofensine • Diclofensine • DOV-102,677 • DOV-21,947 • DOV-216,303 • NS-2359 • SEP-225289 • SEP-227,162 • Tesofensine; Tricyclic antidepressants (TCAs): Amitriptyline • Butriptyline • Cianopramine • Clomipramine • Desipramine • Dosulepin • Doxepin • Imipramine • Lofepramine • Nortriptyline • Pipofezine • Protriptyline • Trimipramine; Tetracyclic antidepressants (TeCAs): Amoxapine; Piperazines: Nefazodone • Trazodone; Antihistamines: Brompheniramine • Chlorphenamine • Diphenhydramine • Mepyramine/Pyrilamine • Pheniramine • Tripelennamine; Opioids: Pethidine • Methadone • Propoxyphene; Others: Cocaine • CP-39,332 • Cyclobenzaprine • Dextromethorphan • Dextrorphan • EXP-561 • Fezolamine • Mesembrine • Nefopam • PIM-35 • Pridefine • Roxindole • SB-649,915 • ZiprasidoneReleasing agents Aminoindanes: 5-IAI • AMMI • ETAI • MDAI • MDMAI • MMAI • TAI; Aminotetralins: 6-CAT • 8-OH-DPAT • MDAT • MDMAT; Oxazolines: 4-Methylaminorex • Aminorex • Clominorex • Fluminorex; Phenethylamines (also Amphetamines, Cathinones, Phentermines, etc): 2-Methyl-MDA • 4-CAB • 4-FA • 4-FMA • 4-HA • 4-MTA • 5-APDB • 5-Methyl-MDA • 6-APDB • 6-Methyl-MDA • AEMMA • Amiflamine • BDB • BOH • Brephedrone • Butylone • Chlorphentermine • Cloforex • Amfepramone • Metamfepramone • DCA • DFMDA • DMA • DMMA • EBDB • EDMA • Ethylone • Etolorex • Fenfluramine (Dexfenfluramine) • Flephedrone • IAP • IMP • Lophophine • MBDB • MDA • MDEA • MDHMA • MDMA • MDMPEA • MDOH • MDPEA • Mephedrone • Methedrone • Methylone • MMA • MMDA • MMDMA • MMMA • NAP • Norfenfluramine • 4-TFMA • pBA • pCA • pIA • PMA • PMEA • PMMA • TAP; Piperazines: 2C-B-BZP • 2-BZP • 3-MeOPP • BZP • DCPP • MBZP • mCPP • MDBZP • MeOPP • Mepiprazole • pCPP • pFPP • pTFMPP • TFMPP; Tryptamines: 4-Methyl-αET • 4-Methyl-αMT • 5-CT • 5-MeO-αET • 5-MeO-αMT • 5-MT • αET • αMT • DMT • Tryptamine (itself); Others: Indeloxazine • Tramadol • ViqualineEnzyme inhibitors AGN-2979 • FenclonineNonselective: Benmoxin • Caroxazone • Echinopsidine • Furazolidone • Hydralazine • Indantadol • Iproclozide • Iproniazid • Isocarboxazid • Isoniazid • Linezolid • Mebanazine • Metfendrazine • Nialamide • Octamoxin • Paraxazone • Phenelzine • Pheniprazine • Phenoxypropazine • Pivalylbenzhydrazine • Procarbazine • Safrazine • Tranylcypromine; MAO-A Selective: Amiflamine • Bazinaprine • Befloxatone • Befol • Brofaromine • Cimoxatone • Clorgiline • Esuprone • Harmala alkaloids (Harmine, Harmaline, Tetrahydroharmine, Harman, Norharman, etc) • Methylene Blue • Metralindole • Minaprine • Moclobemide • Pirlindole • Sercloremine • Tetrindole • Toloxatone • TyrimaOthers Ferrous iron (Fe2+) • Magnesium (Mg2+) • Tetrahydrobiopterin • Vitamin B3 (Niacin, Nicotinamide → NADPH) • Vitamin B6 (Pyridoxine, Pyridoxamine, Pyridoxal → Pyridoxal phosphate) • Vitamin B9 (Folic Acid → Tetrahydrofolic acid) • Vitamin C (Ascorbic acid) • Zinc (Zn2+)OthersCategories:- Eli Lilly and Company
- Synthetic opioids
- Drug rehabilitation
- German inventions
- Inventions of the Third Reich
- Ketones
- Amines
- Mu-opioid agonists
Wikimedia Foundation. 2010.
Look at other dictionaries:
Méthadone — Général Nom IUPAC (RS) 6 (diméthylamino) 4,4 diphényl 3 heptanone No CAS … Wikipédia en Français
Methadone — Méthadone Méthadone Général Nom IUPAC (RS) 6 (diméthylamino) 4,4 diphényl 3 heptanone No CAS … Wikipédia en Français
méthadone — [ metadɔn ] n. f. • 1971; angl. amér. methadon(e), de meth(yl)a(mino), d(iphenyl) et (heptan)one ♦ Dérivé synthétique de la morphine, utilisé comme produit de substitution à l héroïne dans certaines cures de désintoxication. ● méthadone nom… … Encyclopédie Universelle
methadone — 1947, generic designation for 6 dimethylamino 4, 4 diphenyl 3 heptanone. For origins of the syllables, see METHYL (Cf. methyl) + AMINO (Cf. amino) + DI (Cf. di ) + ONE (Cf. one) … Etymology dictionary
methadone — ► NOUN ▪ a powerful synthetic painkiller, used as a substitute for morphine and heroin in the treatment of addiction. ORIGIN from its chemical name … English terms dictionary
methadone — [meth′ə dōn΄] n. [< (6 di)meth(yl)a(mino 4,4 )d(iphenyl 3 heptan)one] a synthetic narcotic drug, C21H27NO, used in medicine to treat heroin and morphine addicts: it is more potent than morphine, with a longer duration of action and milder… … English World dictionary
methadone — /meth euh dohn /, n. Pharm. a synthetic narcotic, C21H28ClNO, similar to morphine but effective orally, used in the relief of pain and as a heroin substitute in the treatment of heroin addiction. Also, methadon /meth euh don /. [1945 50, Amer.;… … Universalium
methadone — methadon methadon, methadone methadone . a narcotic drug similar to morphine but less habit forming; used in treating heroin addiction. Syn: methadone hydrochloride. [WordNet 1.5] … The Collaborative International Dictionary of English
Methadone — A synthetic opiate. The most common medical use for methadone is as a legal substitute for heroin in some treatment programs for drug addiction. It is administered to participating addicts daily at a drug clinic in the form of a green, tasteless… … Medical dictionary
methadone — noun Methadone is used before these nouns: ↑clinic … Collocations dictionary
 18+© Academic, 2000-2026
18+© Academic, 2000-2026- Contact us: Technical Support, Advertising
Dictionaries export, created on PHP, Joomla, Drupal, WordPress, MODx.
- InChI=1S/C21H27NO/c1-5-20(23)21(16-17(2)22(3)4,18-12-8-6-9-13-18)19-14-10-7-11-15-19/h6-15,17H,5,16H2,1-4H3