- Venlafaxine
drugbox
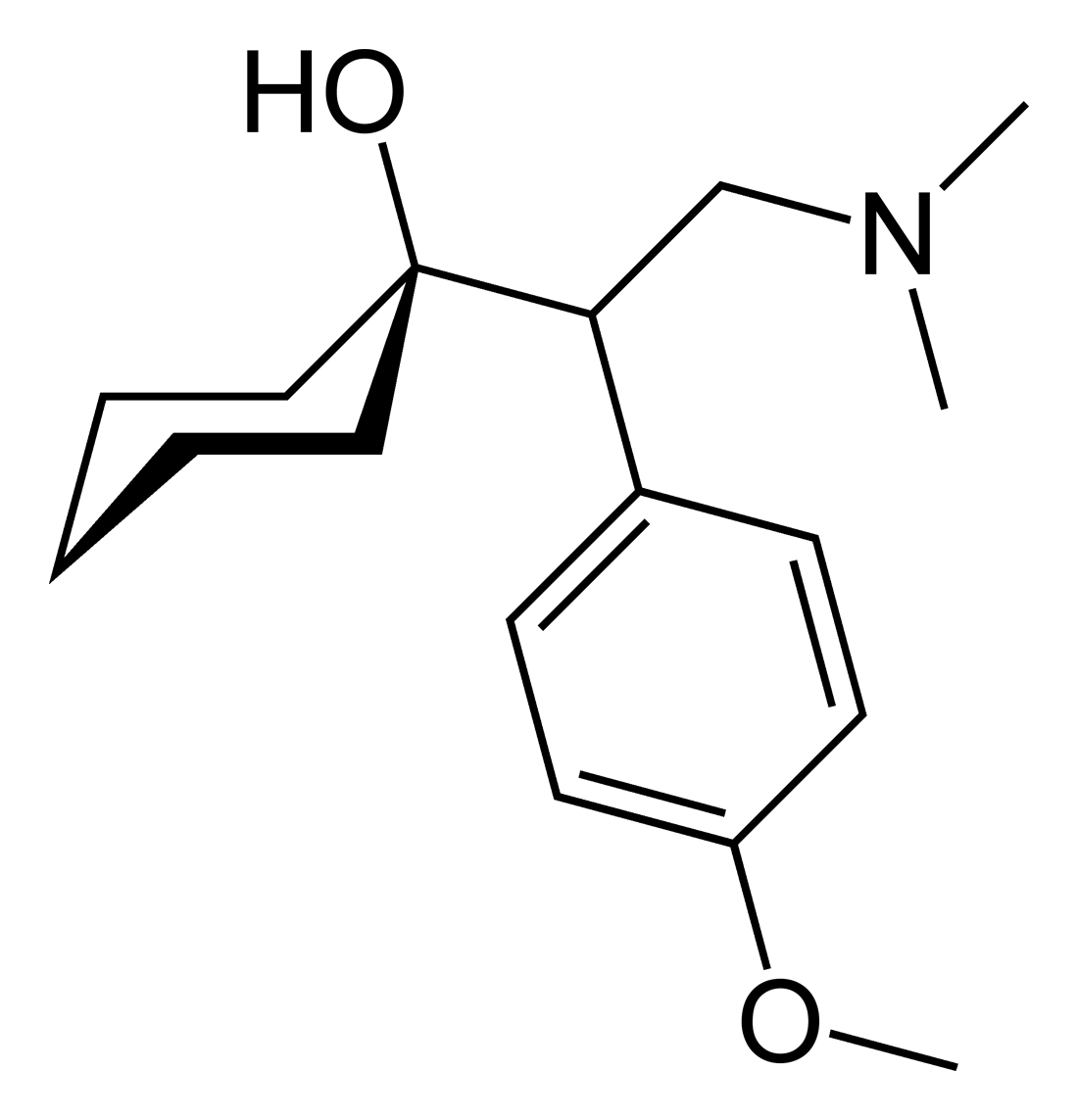
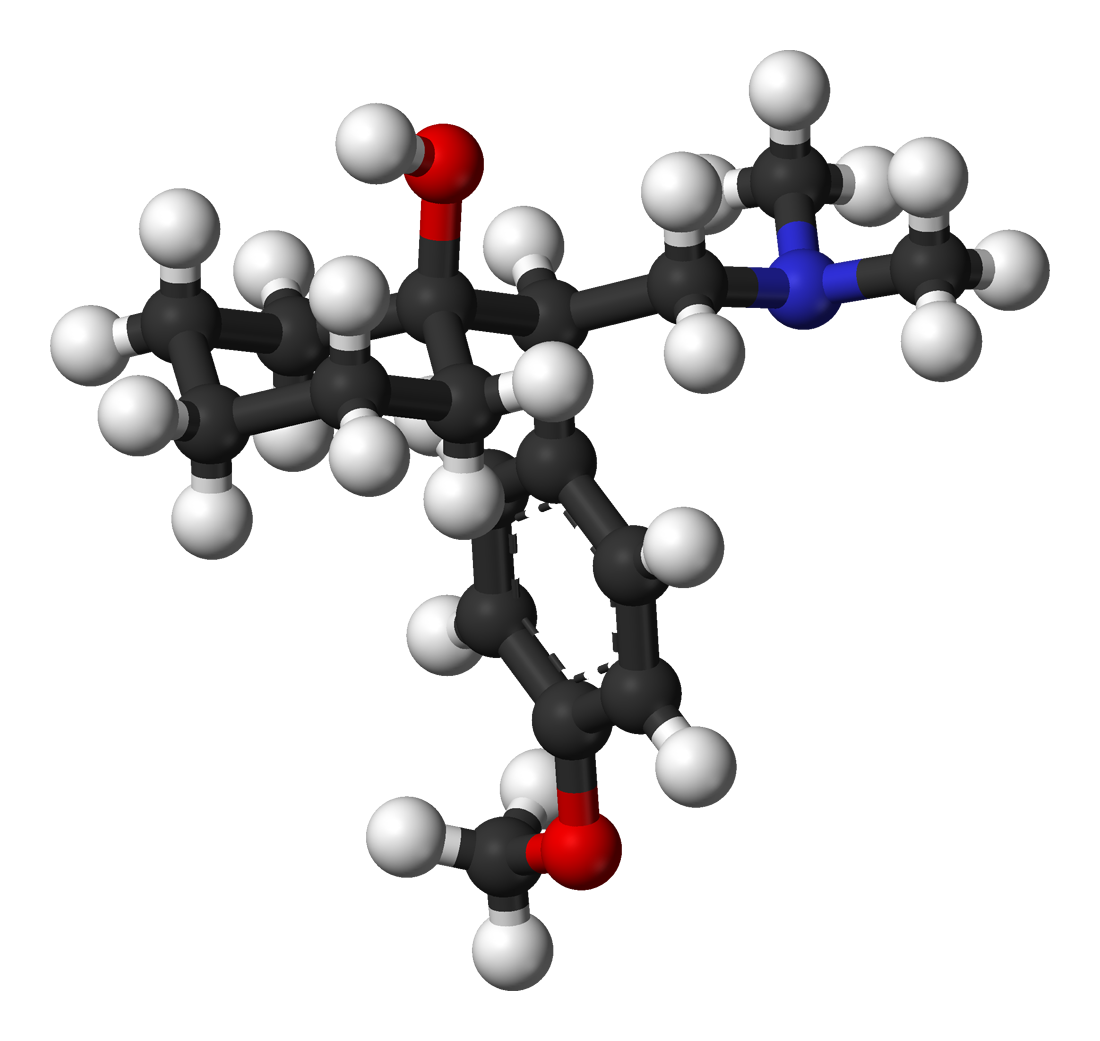
IUPAC_name = 1- [2-dimethylamino-1- (4-methoxyphenyl)- ethyl] cyclohexan-1-ol
CAS_number = 93413-69-5
ChemSpiderID = 56641
ATC_prefix = N06
ATC_suffix = AX16
ATC_supplemental =
PubChem = 5656
DrugBank = APRD00125
smiles = O [C@@] 1(CCCCC1)C(CN(C)C)c2ccc(OC)cc2
C=17 |H=27 |N=1 |O=2
molecular_weight = 277.402 g/mol
bioavailability = 45%
protein_bound = 27%
metabolism =Hepatic
elimination_half-life = 5 ± 2 hours (parent compound); 11 ± 2 hours (active metabolite)
pregnancy_category = C
legal_status = Rx-only, not a controlled drug
routes_of_administration = Oral
excretion = RenalVenlafaxine (Effexor, Efexor) is an
antidepressant of theserotonin-norepinephrine reuptake inhibitor (SNRI) class first introduced byWyeth in 1993. It is prescribed for the treatment of major depression andanxiety disorders , among other uses. Due to the pronounced side effects and suspicions that venlafaxine may significantly increase the risk of suicide, it is not recommended as a first line treatment of depression. However, it is often effective for depression not responding to SSRIs. Venlafaxine was the sixth most widely-used antidepressant based on the number of retail prescriptions in the US (17.1 million) in 2006. [cite web |title=Top 200 brand-name drugs by units. |work=Drug Topics, Mar 5, 2007 |url=http://www.drugtopics.com/drugtopics/article/articleDetail.jsp?id=407652 |accessdate=2007-04-08]Indications
Approved
Venlafaxine is used primarily for the treatment of major depression,
generalized anxiety disorder ,social anxiety disorder , andpanic disorder in adults.Depression
Venlafaxine was shown to be effective for depression in multiple double blind studies. Venlafaxine is similar in efficacy to the
tricyclic antidepressants amitriptyline (Elavil) andimipramine and it was better tolerated than amitriptyline. Venlafaxine appears to have efficacy similar or somewhat better thansertraline (Zoloft) andfluoxetine (Prozac) depending on the criteria and rating scales used. In particular, higher doses of venlafaxine are more effective, and more patients achievedremission or were "very much improved". At the same time the efficacy was similar if the number of patients who achieved "response" or were "improved" was considered. Ameta-analysis comparing venlafaxine and combined groups ofSSRI or tricyclic antidepressants indicated superiority of venlafaxine.cite journal |author=Golden RN, Nicholas L |title=Antidepressant efficacy of venlafaxine |journal=Depression and anxiety |volume=12 Suppl 1 |issue= |pages=45–9 |year=2000 |pmid=11098413 |doi=10.1002/1520-6394(2000)12:1 <45::AID-DA5>3.0.CO;2-5] Based on the same set of criteria, venlafaxine was similar in efficacy to an atypical antidepressantbupropion (Wellbutrin); however, the remission rate was significantly lower for venlafaxine.cite journal |author=Thase ME, Clayton AH, Haight BR, Thompson AH, Modell JG, Johnston JA |title=A double-blind comparison between bupropion XL and venlafaxine XR: sexual functioning, antidepressant efficacy, and tolerability |journal=Journal of clinical psychopharmacology |volume=26 |issue=5 |pages=482–8 |year=2006 |pmid=16974189 |doi=10.1097/01.jcp.0000239790.83707.ab] Venlafaxine was also marginally inferior in efficacy to a newer SSRIescitalopram (Lexapro) and had twice higher frequency of the side effects, in particular, nausea, ejaculation disorder, somnolence and sweating.cite journal |author=Bielski RJ, Ventura D, Chang CC |title=A double-blind comparison of escitalopram and venlafaxine extended release in the treatment of major depressive disorder |journal=The Journal of clinical psychiatry |volume=65 |issue=9 |pages=1190–6 |year=2004 |pmid=15367045 |doi=] In a double-blind study, patients who did not respond to an SSRI were switched to venlafaxine orcitalopram . Similar improvement was observed in both groups.cite journal |author=Lenox-Smith AJ, Jiang Q |title=Venlafaxine extended release versus citalopram in patients with depression unresponsive to a selective serotonin reuptake inhibitor |journal=Int Clin Psychopharmacol |volume=23 |issue=3 |pages=113–9 |year=2008 |pmid=18408525 |doi=10.1097/YIC.0b013e3282f424c2 |url= |doi_brokendate=2008-06-21]A popular magazine "
Consumer Reports ", which in 2004 had rated venlafaxine as the most effective among six commonly prescribed antidepressants, [Citation |title=Mental health, readers rate antidepressant drugs |newspaper=Consumer Reports |pages= |year=2004 |date=September 2004 |url=] no longer recommends it.Fluoxetine ,citalopram andbupropion have been chosen as Consumer Reports Best Buy drugs in the updated version of their guide, based upon effectiveness, safety, side effects, and cost. [cite web |title=Consumer Reports Best Buy Drugs. Antidepressants. |url=http://www.crbestbuydrugs.org/PDFs/Antidepressants_update.pdf |accessdate=2007-06-23 |author= |authorlink= |coauthors= |date= |format=PDF |work= |publisher=Consumer Reports |pages= |language= |archiveurl= |archivedate= |quote=]Off-label / investigational uses
Many doctors are starting to prescribe venlafaxine "off label" for the treatment of
diabetic neuropathy (in a similar manner toduloxetine ) andmigraine prophylaxis (in some people, however, venlafaxine can exacerbate or cause migraines). Studies have shown venlafaxine's effectiveness for these conditions. [cite journal |author=Rowbotham M, Goli V, Kunz N, Lei D |title=Venlafaxine extended release in the treatment of painful diabetic neuropathy: a double-blind, placebo-controlled study |journal=Pain |volume=110 |issue=3 |pages=697–706 |year=2004 |pmid=15288411 |doi=10.1016/j.pain.2004.05.010] [cite journal |author=Ozyalcin S, Talu G, Kiziltan E, Yucel B, Ertas M, Disci R |title=The efficacy and safety of venlafaxine in the prophylaxis of migraine |journal=Headache |volume=45 |issue=2 |pages=144–52 |year=2005 |pmid=15705120 |doi=10.1111/j.1526-4610.2005.05029.x] It has also been found to reduce the severity of 'hot-flashes' in menopausal women. [cite web |author=Mayo Clinic staff |year=2005 |title=Beyond hormone therapy: Other medicines may help |work=Hot flashes: Ease the discomfort of menopause |publisher=Mayo Clinic |url=http://www.mayoclinic.com/invoke.cfm?id=HQ01409 |accessdaymonth=19 August |accessyear=2005] [ cite journal |author=Schober C, Ansani N |title=Venlafaxine hydrochloride for the treatment of hot flashes |journal=Ann Pharmacother |volume=37 |issue=11 |pages=1703–7 |year=2003 |pmid=14565812 |doi=10.1345/aph.1C483]Substantial weight loss in patients with major depression, generalized anxiety disorder, and social phobia has been noted, but the manufacturer does not recommend use as an
anorectic either alone or in combination with phentermine or other amphetamine-like drugs. Venlafaxine hydrochloride is in the phenethylamine class of modern chemicals, which includes amphetamine, methylendioxymethamphetamine (MDMA), and methamphetamine. This chemical structure likely lends to its activating properties, however some patients find Venlafaxine highly sedating despite its more common stimulatory effects.Venlafaxine is not approved for the treatment of depressive phases of
bipolar disorder ; this has some potential danger as venlafaxine can inducemania , mixed states, rapid cycling and/orpsychosis in some bipolar patients, particularly if they are not also being treated with amood stabilizer . Venlafaxine is perhaps one of the most likely of all modern antidepressants to trigger manic and hypomanic states.Fact |date=September 2007Due to its action on both the serotoninergic and
adrenergic systems, Venlafaxine is also used as a treatment to reduce episodes ofcataplexy , a form of muscle weakness, in patients with thesleep disorder narcolepsy . [cite web |last= |first= |authorlink= |coauthors= |title=Medications |work= |publisher=Stanford University School of Medicine, Center for Narcolepsy |date=Revised 02/07/2003 |url=http://med.stanford.edu/school/Psychiatry/narcolepsy/medications.html |doi= |accessdate=2007-09-03]Venlafaxine was found in one study to be equal to
Anafranil in the treatment ofOCD with fewer side effects.cite journal |author=Albert U, Aguglia E, Maina G, Bogetto F |title=Venlafaxine versus clomipramine in the treatment of obsessive-compulsive disorder: a preliminary single-blind, 12-week, controlled study |journal=J Clin Psychiatry |volume=63 |issue=11 |pages=1004–9 |year=2002 |month=November |pmid=12444814 |doi= |url=http://www.psychiatrist.com/privatepdf/2002/v63n11/v63n1108.pdf |format=PDF]Due to its tendency to increase blood pressure and its modulative effects on the autonomic nervous system, venlafaxine is often used to treat
orthostatic intolerance andpostural orthostatic tachycardia syndrome . [cite web |last=Hain T |title=Orthostatic Hypotension |work= |publisher=www.dizziness-and-balance.com |date=Revised 12/30/2007 |url=http://www.dizziness-and-balance.com/disorders/medical/orthostatic.html |doi= |accessdate=2008-03-29]Contraindications
Venlafaxine is not recommended in patients hypersensitive to venlafaxine. It should not be taken by anyone who is allergic to the inactive ingredients, which include
gelatin ,cellulose , ethylcellulose,iron oxide ,titanium dioxide andhypromellose . It should never be used in conjunction with amonoamine oxidase inhibitor (MAOI), due to the potential to develop a potentially deadly condition known asserotonin syndrome . At least 14 days time lag are required between the intake of venlafaxine and MAO inhibitors. Caution should also be used in those with a seizure disorder. Venlafaxine is not approved for use in children or adolescents. However, Wyeth does provide information on precautions if venlafaxine is prescribed to this age group for the treatment of non-approved conditions. Studies in these age groups have not established its efficacy or safety. [cite journal |author=Courtney D |title=Selective serotonin reuptake inhibitor and venlafaxine use in children and adolescents with major depressive disorder: a systematic review of published randomized controlled trials |journal=Can J Psychiatry |volume=49 |issue=8 |pages=557–63 |year=2004 |pmid=15453105]Liver, kidney and thyroid Disorders
The prescribed dosage of venlafaxine may have to be adjusted for those with liver, thyroid or kidney problems. It is crucial to inform a doctor of any such disorders before taking venlafaxine.
Glaucoma
Venlafaxine can increase eye pressure, so those with
glaucoma may require more frequent eye checks.Pregnancy, labor, and delivery
There are no adequate and well controlled studies with venlafaxine in pregnant women. Therefore, venlafaxine should only be used during pregnancy if clearly needed. Prospective studies have not shown any statistically significant congenital malformations. [cite journal |author=Gentile S |title=The safety of newer antidepressants in pregnancy and breastfeeding |journal=Drug Saf |volume=28 |issue=2 |pages=137–52 |year=2005 |pmid=15691224 |doi=10.2165/00002018-200528020-00005] There have, however, been some reports of self-limiting effects on newborn infants. [cite journal |author=de Moor R, Mourad L, ter Haar J, Egberts A |title= [Withdrawal symptoms in a neonate following exposure to venlafaxine during pregnancy] |journal=Ned Tijdschr Geneeskd |volume=147 |issue=28 |pages=1370–2 |year=2003 |pmid=12892015] As with other Serotonin Reuptake Inhibitors, these effects are generally short, lasting only 3 to 5 days [cite journal |author=Ferreira E, Carceller AM, Agogué C, Martin BZ, St-André M, Francoeur D, Bérard A |title= [Effects of selective serotonin reuptake inhibitors and venlafaxine during pregnancy in term and preterm neonates] |journal=Pediatrics |volume=119 |issue=1 |pages=52–9 |year=2007 |pmid=17200271 |doi=10.1542/peds.2006-2133] and rarely resulting in severe complications.cite journal |author=Moses-Kolko EL, Bogen D, Perel J, Bregar A, Uhl K, Levin B, Wisner KL |title= [Neonatal signs after late in utero exposure to serotonin reuptake inhibitors: Literature review and implications for clinical applications] |journal=JAMA |volume=293 |issue=19 |pages=2372–83 |year=2005 |pmid=15900008 |doi=10.1001/jama.293.19.2372] Use of Venlafaxine in pregnancy (like other Serotonin Reuptake Inhibitors) should be considered on a case-by-case basis.
Heart disease and hypertension
The FDA has asked the sponsors of all SNRIs to include the potential risk for persistent
pulmonary hypertension (PPHN) in prescribing data as ofJuly 19 ,2006 . Medications containing Venlafaxine caused a mean heart rate increase of 4 b.p.m in clinical trials, along with a sustained increase in blood pressure in some.erotonin syndrome
The development of a potentially life-threatening
serotonin syndrome (also more recently classified as "serotonin toxicity")cite journal |author=Dunkley EJ, Isbister GK, Sibbritt D, Dawson AH, Whyte IM |title=The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity |journal=QJM |volume=96 |issue=9 |pages=635–42 |year=2003 |month=September |pmid=12925718 |doi= |url=http://www.qjmed.oxfordjournals.org/cgi/content/full/96/9/635] may occur with Venlafaxine treatment, particularly with concomitant use of serotonergic drugs (includingSSRI s,SNRI s, and triptans) and with drugs that impair metabolism of serotonin (includingMAOI s). Serotonin syndrome symptoms may include mental status changes (e.g., agitation, hallucinations, coma), autonomic instability (e.g., tachycardia, labile blood pressure, hyperthermia), neuromuscular aberrations (e.g., hyperreflexia, incoordination) and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea). Venlafaxine-induced serotonin syndrome has also been reported when venlafxine has been taken in isolation in overdose.cite journal |author=Kolecki P |title=Isolated venlafaxine-induced serotonin syndrome |journal=J Emerg Med |volume=15 |issue=4 |pages=491–3 |year=1997 |pmid=9279702 |doi= ] An abortive serotonin syndrome state, in which some but not all of the symptoms of the full serotonin syndrome are present, has been reported with venlafaxine at low and mid-range dosages (37.5 and 150 mg per day) (see Abortive Serotonin syndrome).Adverse effects
As with most antidepressants, lack of
sexual desire is a common side effect. In trials,delayed ejaculation anddelayed orgasm occurred in 8-16% of men. Delayed orgasm occurred in 2-8% of women. Venlafaxine can raise blood pressure at high doses, so it is contraindicated for persons withhypertension .It has a higher rate of treatment emergent mania than many modern antidepressants, and many people find it to be a more activating medication (one that increases energy or wakefulness) than other antidepressants.Fact |date=February 2007 Paradoxically, some users find it highly sedating and find that it must be taken in the evening.
There have been false positive
phencyclidine (PCP) results caused by Venlafaxine with certain on-site routine urine-based drug tests.cite journal |author=Santos PM, López-García P, Navarro JS, Fernández AS, Sádaba B, Vidal JP |title=False positive phencyclidine results caused by venlafaxine |journal=Am J Psychiatry |volume=164 |issue=2 |pages=349 |year=2007 |month=February |pmid=17267806 |doi=10.1176/appi.ajp.164.2.349 |url=http://ajp.psychiatryonline.org/cgi/content/full/164/2/349] cite journal |author=Sena SF, Kazimi S, Wu AH |title=False-positive phencyclidine immunoassay results caused by venlafaxine and O-desmethylvenlafaxine |journal=Clin. Chem. |volume=48 |issue=4 |pages=676–7 |year=2002 |pmid=11901076 |doi= |url=http://clinchem.org/cgi/content/full/48/4/676] Positive on-site results should always be sent to a qualifieddrug testing laboratory for confirmation "before" any action is taken against the employee.uicide ideation/risk
The US Food and Drug Administration body (FDA) requires all antidepressants, including venlafaxine, to carry a black box with a generic warning about a possible suicide risk. In addition, the most recent research indicated that patients taking venlafaxine are at increased risk of suicide.
A study conducted in Finland followed more than 15,000 patients for 3.4 years. Venlafaxine increased suicide risk 1.6-fold (statistically significant), as compared to no treatment. At the same time,
fluoxetine (Prozac) halved the suicide risk.cite journal |author=Tiihonen J, Lönnqvist J, Wahlbeck K, Klaukka T, Tanskanen A, Haukka J |title=Antidepressants and the risk of suicide, attempted suicide, and overall mortality in a nationwide cohort |journal=Arch. Gen. Psychiatry |volume=63 |issue=12 |pages=1358–67 |year=2006 |pmid=17146010 |doi=10.1001/archpsyc.63.12.1358]In another study, the data on more than 200,000 cases was obtained from the UK general practice research database. The patients taking venlafaxine had significantly higher risk of completed suicide than the ones on
fluoxetine (Prozac) (2.8 times) orcitalopram (Celexa) (2.4 times). Even after taking into consideration the fact that venlafaxine was generally prescribed for more severe depression, venlafaxine was associated with 1.6-1.7 times more suicides than fluoxetine or citalopram. This difference was no longer statistically significant due to the rarity of completed suicides. However, for the attempted suicides (more frequent event) the 1.2-1.3 times higher risk for venlafaxine still stayed statistically significant after the adjustment.cite journal |author=Rubino A, Roskell N, Tennis P, Mines D, Weich S, Andrews E |title=Risk of suicide during treatment with venlafaxine, citalopram, fluoxetine, and dothiepin: retrospective cohort study |journal=BMJ |volume=334 |issue=7587 |pages=242 |year=2007 |pmid=17164297 |doi=10.1136/bmj.39041.445104.BE]An analysis of clinical trials by the FDA statisticians showed the incidence of suicidal behavior among the adults on venlafaxine to be not significantly different from fluoxetine or placebo.cite web |url=http://www.fda.gov/ohrms/dockets/ac/06/briefing/2006-4272b1-01-FDA.pdf |title=Overview for December 13 Meeting of Psychopharmacologic Drugs Advisory Committee |accessdate=2007-06-20 |author= |authorlink= |coauthors= |date=November 16, 2006 |format=PDF |work= |publisher= |pages= |language= |archiveurl= |archivedate= |quote=] A possible explanation for this discrepancy is that suicidal patients are generally excluded from clinical trials, and so clinical trials are not quite representative of the real population of patients.
Venlafaxine is contraindicated to children, adolescents and young adults. According to the FDA analysis of clinical trials venlafaxine caused a 5-fold increase (statistically significant) of suicidal ideation and behavior in subjects younger than 25. In another analysis, venlafaxine was no better than placebo among children (7-11 years old) and improved the depression in adolescents (12-17 years old). However, in both groups hostility and suicidal behavior were increased in comparison to the placebo treatment.cite journal |author=Emslie GJ, Findling RL, Yeung PP, Kunz NR, Li Y |title=Venlafaxine ER for the treatment of pediatric subjects with depression: results of two placebo-controlled trials |journal=Journal of the American Academy of Child and Adolescent Psychiatry |volume=46 |issue=4 |pages=479–88 |year=2007 |pmid=17420682 |doi=10.1097/chi.0b013e31802f5f03]
erotonin syndrome
Another risk is
serotonin syndrome (also more recently classified as "serotonin toxicity").This is a rare but serious side effect that can be caused by interactions with otherserotonergic drugs, and is potentially fatal. [cite journal |author=Adan-Manes J, Novalbos J, López-Rodríguez R, Ayuso-Mateos J, Abad-Santos F |title=Lithium and venlafaxine interaction: a case of serotonin syndrome |journal=J Clin Pharm Ther |volume=31 |issue=4 |pages=397–400 |year=2006 |pmid=16882112 |doi=10.1111/j.1365-2710.2006.00745.x] This risk necessitates clear information to patients and proper medical history. For example, the drug abuse by at-risk patients of certain non-prescription drugs can cause this serious effect, and emphasizes the importance of good medical history sharing between general practitioners and psychiatrists, as both may prescribe venlafaxine. Involvement of family in awareness of risk factors is highlighted in Wyeth information sheets on Effexor. Venlafaxine-induced serotonin syndrome has also been reported when venlafxine has been taken in isolation in overdose.Abortive Serotonin syndrome
An abortive serotonin syndrome state, in which some but not all of the symptoms of the full serotonin syndrome are present, has been reported with venlafaxine at mid-range dosages (150 mg per day) [cite web |url=http://www.priory.com/psych/venhall.htm |title=Hallucinations as a side effect of venlafaxine treatment |accessdate=2008-06-17 |author=Ebert D. et al. |publisher=Psychiatry On-line] A case of a patient with serotonin syndrome induced by low-dose venlafaxine (37.5 mg per day) has also been reported.cite journal |author=Pan JJ, Shen WW |title=Serotonin syndrome induced by low-dose venlafaxine |journal=Ann Pharmacother |volume=37 |issue=2 |pages=209–11 |year=2003 |month=February |pmid=12549949 |doi= |url=]
Following the publication of "The Hunter Serotonin Toxicity Criteria", such cases (as with cases of the full serotonin syndrome) are classified as cases of "serotonin toxicity". As a result it is now clear that, even when venlafaxine is the sole serotonergic agent, susceptible individuals may develop venlafaxine-induced serotonin toxicity regardless of the dosage of the drug involved. However, it may also be the case that at lower dosages venlafaxine's relatively short half-life may allow recovery to begin before all of the symptoms of serotonin toxicity develop.
Common side effects
NOTE: The percentage of occurrences for each side effect listed comes from clinical trial data provided by Wyeth Pharmaceuticals Inc. The percentages indicate the percentage of people that experienced the side effect in clinical trials.
*
Nausea (21-35%)
*Headache (34%)
*Apathy
*Constipation
* OngoingIrritable Bowel Syndrome
*Dizziness (11-20%)
* Fatigue
*Insomnia (15-23%)
* Vertigo
*Dry mouth (12-16%)
*Sexual dysfunction (14-34%)
*Sweating (10-14%)
*Orthostatic hypotension (postural drop in blood pressure)
* Vivid/Abnormaldream s (3-7%)
* Impulsive Actions
* Increasedblood pressure
* Decreased Appetite (8-20%)
* Electric shock-like sensations also called "Brain zaps "
* Increased anxiety at the start of treatment
*Akathisia (Agitation) (3-4%)
* Memory LossLess common to rare side-effects
Note 'Rare' adverse effects occur in fewer than 1 in 1000 patients. 'Infrequent' adverse effects occur in 1 in 100 to 1 in 1000 patients.
*
Cardiac arrhythmia
* Increased serum cholesterol
* Gas or stomach pain
* Abnormal vision
* Nervousness, agitation or increased anxiety
*Panic Attack s
* Depressed feelings
* Suicidal thoughts
* Confusion
*Neuroleptic malignant syndrome
* Loss of appetite
*Tremor
* Drowsiness
* Allergic skin reactions
* External bleeding
* Seriousbone marrow damage (thrombocytopenia ,agranulocytosis )
*Hepatitis
*Pancreatitis
*Seizure
*Tardive dyskinesia
* Difficulty swallowing
* Psychosis
* Hair Loss
* Hostility
* Activation of mania/hypomania.
* Weight Loss (of concern when treating patients suffering fromanorexia nervosa )
* Weight gain (effect not clear, but of concern when treating people who may haveBody Dysmorphic Disorder ).
* Homicidal Thoughts
* Aggression
*Depersonalization
* Visual Hallucinations
* Swollen and/or bleeding gums
* Frequent urinationDose dependency of adverse events
A comparison of adverse event rates in a fixed-dose study comparing venlafaxine 75, 225, and 375 mg/day with
placebo revealed a dose dependency for some of the more common adverse events associated with venlafaxine use. The rule for including events was to enumerate those that occurred at an incidence of 5% or more for at least one of the venlafaxine groups and for which the incidence was at least twice the placebo incidence for at least one venlafaxine group. Tests for potential dose relationships for these events (Cochran-Armitage Test, with a criterion of exact 2-sided p-value <=0.05) suggested a dose-dependency for several adverse events in this list, including chills, hypertension, anorexia, nausea, agitation, dizziness, somnolence, tremor, yawning, sweating, and abnormal ejaculation.Memory Loss
In a study of the tolerability of venlafaxine at a dose range higher than the recommended maximum 375 mg per day (from 375 to 600 mg per day) for treating DSM-IV major depressive disorder "failing memory" was reported in 44.4% of cases, significantly more severely than at typical doses of 75-375 mg per day. cite journal |author=Harrison CL, Ferrier N, Young AH |title=Tolerability of high-dose venlafaxine in depressed patients |journal=J. Psychopharmacol. (Oxford) |volume=18 |issue=2 |pages=200–4 |year=2004 |month=June |pmid=15260908 |doi=10.1177/0269881104042621 |url=]
Physical and psychological dependency
In vitro studies revealed that venlafaxine has virtually no affinity for opiate, benzodiazepine, phencyclidine (
PCP ), or N-methyl-D-aspartic acid (NMDA ) receptors. It has no significant CNS stimulant activity in rodents. In primate drug discrimination studies, venlafaxine showed no significant stimulant or depressant abuse liability.Notwithstanding these in-vitro and non-human research findings, some patients using venlafaxine may become dependent on this drug. This is especially noted if a patient misses a dose, but can also occur when reduction of dosage is done with a doctor's care. This may result in experiencing
withdrawal symptoms described as severe discontinuation syndrome. The high risk of withdrawal symptoms may reflect venlafaxine's short half-life.cite journal |author=Haddad PM |title=Antidepressant discontinuation syndromes |journal=Drug Saf |volume=24 |issue=3 |pages=183–97 |year=2001 |pmid=11347722 |doi=10.2165/00002018-200124030-00003 |url=] Missing even a single dose can induce discontinuation effects in some patients. Discontinuation is similar in nature to those of SSRIs such asParoxetine (Paxil orSeroxat ). Sudden discontinuation of venlafaxine has a high risk of causing potentially severewithdrawal symptoms.cite journal |author=Fava M, Mulroy R, Alpert J, Nierenberg A, Rosenbaum J |title=Emergence of adverse events following discontinuation of treatment with extended-release venlafaxine |journal=Am J Psychiatry |volume=154 |issue=12 |pages=1760–2 |year=1997 |pmid=9396960] As reported in 2001 by Haddad in the journal "Drug Safety", "another strategy to consider is switching to fluoxetine, which may suppress the discontinuation symptoms, but which has little tendency to cause such symptoms itself," and then discontinuing that.As the drug has direct impact on mood (i.e., anti-depressant), many users who have suffered the effects of attempted withdrawal from this drug define their dependency on the drug also as being addicted. Although many other drugs can cause withdrawal symptoms which are not associated with addiction or dependence, for example,
anticonvulsants ,beta-blockers , nitrates,diuretic s, centrally acting antihypertensives,sympathomimetic s,heparin ,tamoxifen , dopaminergic agents,antipsychotics , and lithium, addiction or dependence is a more common effect described for drugs that (are thought to, or may) improve mental well-being.cite journal |author=Double D |title=Prescribing antidepressants in general practice. People may become psychologically dependent on antidepressants |journal=BMJ |volume=314 |issue=7083 |pages=829 |year=1997 |pmid=9081020]Combined Serotonin Toxicity and SSRI Discontinuation Syndrome
Venlafaxine may be particularly hazardous to those individuals who are susceptible to both venlafaxine-induced serotonin toxicity (previously named
serotonin syndrome ) andSSRI discontinuation syndrome . In such cases individuals who have developed the potentially fatal serotonin toxicity and/or may be at risk of doing so may find cessation or dose reduction unachievable placing them at continuing risk. As it is not possible to determine which patients are likely to develop the most severe symptoms of the discontinuation syndrome before cessation or dose reduction is attempted, this dual risk requires that all patients are closely monitored during any increase in dosage (when the patient is most at risk of developing serotonin toxicity) [Venlafaxine (marketed as Effexor) FDA Alert: SSRIs/SNRI/Triptan and Serotonin Syndrome [issued 7/2006] ] and that such increases are carried out in the smallest incremental steps possible. Additionally, patients who recommence venlafaxine or revert to a higher dosage following a failed attempt to discontinue the drug or reduce dosage are another group with an increased risk of developing serotonin toxicity. The possibility of developing serotonin toxicity following such a failed attempt at cessation or dose reduction should be considered as part of the process of withdrawal from venlafaxine and in accordance with best practice for preventing or minimising SSRI discontinuation syndrome. [Leo Sher "Prevention of the serotonin reuptake inhibitor discontinuation syndrome" Medical Hypotheses Volume 59, Issue 1, July 2002, Pages 92-94 ]Available forms
Effexor is distributed in pentagon-shaped peach-colored tablets of 25 mg, 37.5 mg, 50 mg, 75 mg, and 100 mg. There is also an extended-release version distributed in capsules of 37.5 mg (gray/peach), 75 mg (peach), and 150 mg (brownish red).
Venlafaxine extended release (XR)
Venlafaxine extended release is chemically the same as normal venlafaxine. The extended release version (sometimes referred to as controlled release) controls the release of the drug into the
gastrointestinal tract over a longer period than normal venlafaxine. This results in a lower peak plasma concentration. Studies have shown that the extended release formula has a lower incidence of patients suffering fromnausea as a side effect resulting in a lower number of patients stopping their treatment due tonausea . [cite journal |author=DeVane CL. |title=Immediate-release versus controlled-release formulations: pharmacokinetics of newer antidepressants in relation to nausea |journal=J Clin Psychiatry |volume=64 |issue=Suppl 18 |pages=14–9 |year=2003 |pmid=14700450] In Australia, New Zealand and Switzerland,Wyeth sells their venlafaxine XR tablets under the name "Efexor-XR" (note the spelling with one 'f', rather than "Effexor-XR"). In Brazil Medley sells a venlafaxine XR capsule under the brand name Alenthus XR.Generic
Generic venlafaxine is available in the
United States as of August 2006 and in Canada as of December 2006. A generic form of the extended-release version is available in Canada as of January 2007 and will become available in the United States in 2010. [Citation |last=Wigginton |first=Catherine |title=Wyeth's Battle for Effexor Continues |date=2006-09-19 |publisher=IP Law & Business |url=http://www.law.com/jsp/article.jsp?id=1158582919715 |accessdate=2007-04-25] Generic versions of both drug forms are available now in India.Overdose
Most patients overdosing with venlafaxine develop only mild symptoms. However, severe toxicity is reported with the most common symptoms being
CNS depression , serotonin toxicity,seizure , or cardiac conduction abnormalities. [cite journal |author=Blythe D, Hackett L |title=Cardiovascular and neurological toxicity of venlafaxine |journal=Hum Exp Toxicol |volume=18 |issue=5 |pages=309–13 |year=1999 |pmid=10372752 |doi=10.1191/096032799678840165] Venlafaxine's toxicity appears to be higher than other SSRIs, with a fatal toxic dose closer to that of thetricyclic antidepressant s than the SSRIs. Doses of 900 mg or more are likely to cause moderate toxicity. Deaths have been reported following very large doses.cite journal |author=Mazur J, Doty J, Krygiel A |title=Fatality related to a 30-g venlafaxine overdose |journal=Pharmacotherapy |volume=23 |issue=12 |pages=1668–72 |year=2003 |pmid=14695048 |doi=10.1592/phco.23.15.1668.31951] [cite journal |author=Banham N |title=Fatal venlafaxine overdose |journal=Med J Aust |volume=169 |issue=8 |pages=445, 448 |year=1998 |pmid=9830400]On May 31 2006, The
Medicines and Healthcare products Regulatory Agency (MHRA) UK has concluded its review into all the latest safety evidence relating to venlafaxine particularly looked at the risks associated with overdose. The advice are, the need for specialist supervision in those severely depressed or hospitalized patients who need doses 300 mg or more; cardiac contra-indications are more targeted towards high risk groups; patients with uncontrolled hypertension should not take venlafaxine, and blood pressure monitoring is recommended for all patients; and updated advice on possible drug interactions. [cite journal |author=MHRA UK |title=Updated product information for venlafaxine |journal=Safeguarding public health |volume= 120|issue= |pages= 778|year=2006 |month=31 May |doi=10.1016/j.puhe.2006.03.006]On October 17, 2006 Wyeth and the FDA notified healthcare professionals of revisions to the Overdosage/Human Experience section of the prescribing information for Effexor (venlafaxine), indicated for treatment of major depressive disorder. In postmarketing experience, there have been reports of overdose with venlafaxine, occurring predominantly in combination with alcohol and/or other drugs. Published retrospective studies report that venlafaxine overdosage may be associated with an increased risk of fatal outcome compared to that observed with SSRI antidepressant products, but lower than that for tricyclic antidepressants. Healthcare professionals are advised to prescribe Effexor and Effexor XR in the smallest quantity of capsules consistent with good patient management to reduce the risk of overdose. [cite web |year=2006 |title=Wyeth Letter to Health Care Providers |publisher=Wyeth Pharmaceuticals Inc |url=http://www.fda.gov/medwatch/SAFETY/2006/effexor_DHCPletter.pdf |accessdaymonth=30 January |accessyear=2007|format=PDF]
A report in the
British Medical Journal in 2002 by Dr. Nicholas Buckley and colleagues at the Department of Clinical Pharmacology and Toxicology,Canberra Hospital,Australia studying fatal toxicity index (deaths per million prescriptions) found that venlafaxine's fatal toxicity is higher than that of other serotoninergic antidepressants but it is similar to that of some of the less toxictricyclic antidepressants . Overall they found serious toxicity could occur following venlafaxine overdose with reports of deaths, arrythmias, and seizures. They did, however, state that this type of data is open to criticism pointing out that mortality data may be influenced by previous literature and that "less toxic" drugs may be preferentially prescribed to patients at higher risk of poisoning and suicide but they are also less likely to be listed as the sole cause of death from overdose. It also assumes that drugs are taken in overdose with similar frequency and in similar amounts. They suggested "clinicians need to consider whether factors in their patients reduce or compensate for this risk before prescribing venlafaxine." [cite journal |author=Buckley N, McManus P |title=Fatal toxicity of serotoninergic and other antidepressant drugs: analysis of United Kingdom mortality data |journal=BMJ |volume=325 |issue=7376 |pages=1332–3 |year=2002 |pmid=12468481 |doi=10.1136/bmj.325.7376.1332]The February 27, 2007 Vancouver Sun reported that the BC Drug and Poison Information Centre has alerted doctors that the drug poses a significant risk of death from overdose, saying that venlafaxine "appears more toxic than it was originally hoped". [cite web |last=Fayerman |first=Pamela |title=Warning issued over drug |publisher=Vancouver Sun |date=February 27 2007 |url=http://www.canada.com/vancouversun/news/story.html?id=83f35b4e-ac13-4c09-b8de-44d16750b70b&k=58837 |accessdate=2007-06-02] A doctor from the Department of Pharmacy Services College of Pharmacy, Medical University of South Carolina, Charleston, South Carolina, reported on the death of a 39-year-old patient with a 30 g overdose. To put this into perspective, a patient would have to take over 66 of the infrequently prescribed 450mg high dosage pills, or 400 of the commonly prescribed 75mg pills.
Management of overdosage
There is no specific
antidote for venlafaxine and management is generally supportive, providing treatment for the immediate symptoms. Administration ofactivated charcoal can prevent absorption of the drug. Monitoring of cardiac rhythm and vital signs is indicated. Seizures are managed withbenzodiazepine s or other anti-convulsants.Forced diuresis ,hemodialysis ,exchange transfusion , orhemoperfusion are unlikely to be of benefit in hastening the removal of venlafaxine, due to the drug's highvolume of distribution . [cite journal |author=Hanekamp B, Zijlstra J, Tulleken J, Ligtenberg J, van der Werf T, Hofstra L |title=Serotonin syndrome and rhabdomyolysis in venlafaxine poisoning: a case report |journal=Neth J Med |volume=63 |issue=8 |pages=316–8 |year=2005 |pmid=16186642]Mechanism of action
Venlafaxine is a
bicyclic antidepressant, and is usually categorized as aserotonin-norepinephrine reuptake inhibitor (SNRI), but it has been referred to as aserotonin-norepinephrine-dopamine reuptake inhibitor . [cite web |author= [No Authors listed] |year= |title=Acute Effectiveness of Additional Drugs to the Standard Treatment of Depression |publisher=ClinicalTrials.gov |url=http://www.clinicaltrials.gov/ct/show/NCT00001483 |accessdaymonth=23 June |accessyear=2005] [cite journal |author=Goeringer K, McIntyre I, Drummer O |title=Postmortem tissue concentrations of venlafaxine |journal=Forensic Sci Int |volume=121 |issue=1-2 |pages=70–5 |year=2001 |pmid=11516890 |doi=10.1016/S0379-0738(01)00455-8] It works by blocking the transporter "reuptake" proteins for keyneurotransmitter s affecting mood, thereby leaving more active neurotransmitters in thesynapse . The neurotransmitters affected areserotonin (5-hydroxytryptamine) andnorepinephrine (noradrenaline). Additionally, in high doses it weakly inhibits the reuptake ofdopamine ,cite journal |author=Wellington K, Perry C |title=Venlafaxine extended-release: a review of its use in the management of major depression |journal=CNS Drugs |volume=15 |issue=8 |pages=643–69 |year=2001 |pmid=11524036 |doi=10.2165/00023210-200115080-00007] with recent evidence showing that thenorepinephrine transporter also transports somedopamine as well, implying thatSNRI s may also increasedopamine transmission. This is becauseSNRI s work by inhibiting reuptake, i.e. preventing theserotonin and norepinephrine transporters from taking their respectiveneurotransmitter s back to their storage vesicles for later use. If thenorepinephrine transporter normally recycles somedopamine too, thenSNRI s will also enhancedopaminergic transmission. Therefore, theantidepressant effects associated with increasing norepinephrine levels may also be partly or largely due to the concurrent increase indopamine (particularly in theprefrontal cortex ).Pharmacokinetics
Venlafaxine is well absorbed with at least 92% of an oral dose being absorbed into systemic circulation. It is extensively metabolized in the liver via the
CYP2D6 isoenzyme to O-desmethylvenlafaxine, which is just as potent a serotonin-norepinephrine reuptake inhibitor as the parent compound, meaning that the differences in metabolism between extensive andpoor metabolizer s are not clinically important in terms of efficacy. Side effects, however, are reported to be more severe inCYP2D6 poor metabolizers.cite journal |author=Shams ME et al |title=CYP2D6 polymorphism and clinical effect of the antidepressant venlafaxine |journal=J Clin Pharm Ther |volume=31 |issue=5 |pages=493–502 |year=2006 |pmid=16958828 |doi=10.1111/j.1365-2710.2006.00763.x] Steady-state concentrations of venlafaxine and itsmetabolite are attained in theblood within 3 days. Therapeutic effects are usually achieved within 3 to 4 weeks. No accumulation of venlafaxine has been observed during chronic administration in healthy subjects. The primary route of excretion of venlafaxine and its metabolites is via thekidneys .cite web |year=2006 |title=Effexor Medicines Data Sheet |publisher=Wyeth Pharmaceuticals Inc |url=http://www.wyeth.com/content/ShowLabeling.asp?id=100 |accessdaymonth=17 September |accessyear=2006] Thehalf-life of venlafaxine is relatively short, therefore patients are directed to adhere to a strict medication routine, avoiding missing a dose. Even a single missed dose can result in the withdrawal symptoms.cite journal |author=Parker G, Blennerhassett J |title=Withdrawal reactions associated with venlafaxine |journal=Aust N Z J Psychiatry |volume=32 |issue=2 |pages=291–4 |year=1998 |pmid=9588310 |doi=10.3109/00048679809062742]Drug interactions
Venlafaxine should be taken with caution when using
St John's wort . [cite book |title=2006 Lippincott's Nursing Drug Guide |last=Karch |first=Amy |year=2006 |publisher=Lippincott Williams & Wilkins |location=Philadephia, Baltimore, New York, London, Buenos Aires, Hong Kong, Sydney, Tokyo |isbn=1-58255-436-6] Venlafaxine may lower the seizure threshold, and co-administration with other drugs that lower the seizure threshold such asbupropion andtramadol should be done with caution and at low doses.cite journal |author=Thundiyil JG, Kearney TE, Olson KR |title=Evolving epidemiology of drug-induced seizures reported to a Poison Control Center System |journal=J Med Toxicol |volume=3 |issue=1 |pages=15–9 |year=2007 |month=March |pmid=18072153 |doi= |url=] Seizures have also anecdotally been reported with combination of venlafaxine andmarijuana . [ [http://www.erowid.org/experiences/exp.php?ID=37418 Do Not Combine!Venlafaxine (Effexor) & Cannabis.] ] [ [http://www.erowid.org/experiences/exp.php?ID=66068 Combo Sent Me Into Seizure.Venlafaxine (Effexor XR) & Cannabis.] ]Physical/chemical properties
The
chemical structure of venlafaxine is designated (R/S)-1- [2-(dimethylamino)-1-(4 methoxyphenyl)ethyl] cyclohexanol hydrochloride or (±)-1- [a [a- (dimethylamino)methyl] p-methoxybenzyl] cyclohexanol hydrochloride and it has theempirical formula of C17H27NO2. It is a white to off-white crystalline solid. Venlafaxine is structurally and pharmacologically related to theanalgesic tramadol , but not to any of the conventional antidepressant drugs, includingtricyclic antidepressant s,Selective serotonin reuptake inhibitor s (SSRI),Monoamine oxidase inhibitor s (MAOI), or reversible inhibitors of monoamine oxidase A (RIMA).cite journal |author=Whyte I, Dawson A, Buckley N |title=Relative toxicity of venlafaxine and selective serotonin reuptake inhibitors in overdose compared to tricyclic antidepressants |journal=QJM |volume=96 |issue=5 |pages=369–74 |year=2003 |pmid=12702786 |doi=10.1093/qjmed/hcg062]ee also
*
Desvenlafaxine Footnotes
External links
Drug information
* [http://www.fda.gov/CDER/drug/infopage/effexor/default.htm U.S. Food and Drug Administration information on Effexor]
* [http://emc.medicines.org.uk/emc/assets/c/html/displaydoc.asp?documentid=2209 Efexor patient information leaflet] Efexor patient information leaflet
* [http://www.wyeth.com/content/ShowLabeling.asp?id=100 Effexor XR® prescribing information for healthcare professionals (pdf) (USA only)]
* [http://www.rxlist.com/cgi/generic/venlafax_pi.htm Detailed Patient/Parent Information on Effexor]
* [http://www.merck.com/mmpe/lexicomp/venlafaxine.html#N18219E List of international brand names for Venlafaxine]Diagnostic Tools
* [http://www.qjmed.oxfordjournals.org/cgi/content/full/96/9/635 The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity]
Patient experiences
* [http://www.nytimes.com/2007/05/06/magazine/06antidepressant-t.html?_r=1&ei=5087%0A&em=&en=cdeb03773a3deee0&ex=1178596800&pagewanted=all&oref=slogin Stutz, Bruce "Self-Nonmedication" New York Times Magazine May 6, 2007]
Wikimedia Foundation. 2010.