- Niacin
-
Niacin 
 Nicotinic acid[citation needed]Systematic namePyridine-3-carboxylic acid[1]Other namesBionic
Nicotinic acid[citation needed]Systematic namePyridine-3-carboxylic acid[1]Other namesBionic
Vitamin B3Identifiers CAS number 59-67-6 
PubChem 938 ChemSpider 913 UNII 2679MF687A EC number 200-441-0 DrugBank DB00627 KEGG D00049 MeSH Niacin ChEBI CHEBI:15940 ChEMBL CHEMBL573 IUPHAR ligand 1588 RTECS number QT0525000 ATC code C04,C10AD02 Beilstein Reference 109591 Gmelin Reference 3340 3DMet B00073 Jmol-3D images Image 1
Image 2- Oc(:o):c1cccnc1
OC(=O)C1=CN=CC=C1
- InChI=1S/C6H5NO2/c8-6(9)5-2-1-3-7-4-5/h1-4H,(H,8,9)
Key: PVNIIMVLHYAWGP-UHFFFAOYSA-N
InChI=1/C6H5NO2/c8-6(9)5-2-1-3-7-4-5/h1-4H,(H,8,9)
Key: PVNIIMVLHYAWGP-UHFFFAOYAA
Properties Molecular formula C6NH5O2 Molar mass 123.1094 g mol-1 Exact mass 123.032028409 g mol-1 Appearance White, translucent crystals Density 1.473 g cm-3 Melting point 237 °C, 510 K, 458 °F
Solubility in water 18 g L-1 log P 0.219 Acidity (pKa) 2.201 Basicity (pKb) 11.796 Isoelectric point 4.75 Refractive index (nD) 1.4936 Dipole moment 0.1271305813 D Thermochemistry Std enthalpy of
formation ΔfHo298-344.9 kJ mol-1 Std enthalpy of
combustion ΔcHo298-2.73083 MJ mol-1 Pharmacology Routes of
administrationIntramuscular, Oral Elimination
half-life20-45 min Hazards EU classification  Xi
XiR-phrases R36/37/38 S-phrases S26, S36 NFPA 704  110
110Flash point 193 °C Autoignition
temperature365 °C  (verify) (what is:
(verify) (what is:  /
/ ?)
?)
Except where noted otherwise, data are given for materials in their standard state (at 25 °C, 100 kPa)Infobox references "Niacin" redirects here. For the neo-fusion band, see Niacin (band).
Niacin (also known as vitamin B3, nicotinic acid and vitamin PP) is an organic compound with the formula C6H5NO2 and, depending on the definition used, one of the forty to eighty essential human nutrients.
Niacin is one of five vitamins associated with a pandemic deficiency disease: niacin deficiency (pellagra), vitamin C deficiency (scurvy), thiamin deficiency (beriberi), vitamin D deficiency (rickets), vitamin A deficiency (night blindness and other symptoms).
Niacin has been used to increase levels of HDL cholesterol in the blood and has been found to modestly decrease the risk of cardiovascular events in a number of controlled human trials. However, in a recent trial AIM-HIGH, a slow-release form of niacin was found to have no effect on cardiovascular event and stroke risk in a group of patients with LDL levels already well-controlled by a statin drug, and the trial was halted prematurely on evidence that niacin addition actually increased stroke risk in this group.[2] The role of niacin in treating cardiovascular risk remains under debate.
This colorless, water-soluble solid is a derivative of pyridine, with a carboxyl group (COOH) at the 3-position. Other forms of vitamin B3 include the corresponding amide, nicotinamide ("niacinamide"), where the carboxyl group has been replaced by a carboxamide group (CONH2), as well as more complex amides and a variety of esters. The terms niacin, nicotinamide, and vitamin B3 are often used interchangeably to refer to any member of this family of compounds, since they have similar biochemical activity.
Niacin cannot be directly converted to nicotinamide, but both compounds could be converted to NAD and NADP in vivo. Although the two are identical in their vitamin activity, nicotinamide does not have the same pharmacological effects (lipid modifying effects) as niacin; these effects occur as side effects of niacin's conversion. Nicotinamide does not reduce cholesterol or cause flushing.[3] Nicotinamide may be toxic to the liver at doses exceeding 3 g/day for adults.[4] Niacin is a precursor to NAD+/NADH and NADP+/NADPH, which play essential metabolic roles in living cells.[5] Niacin is involved in both DNA repair, and the production of steroid hormones in the adrenal gland.
Contents
Dietary needs
One recommended daily allowance of niacin is 2–12 mg/day for children, 14 mg/day for women, 16 mg/day for men, and 18 mg/day for pregnant or breast-feeding women.[6] The upper limit for adult men and women is 35 mg/day, which is based on flushing as the critical adverse effect.[citation needed] In general, niacin status is tested through urinary biomarkers,[7] which are believed to be more reliable than plasma levels.[8]
Deficiency
Main article: Pellagra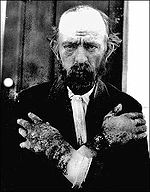 A man with pellagra, which is caused by a chronic lack of vitamin B3 in the diet
A man with pellagra, which is caused by a chronic lack of vitamin B3 in the diet
At present, niacin deficiency is sometimes seen in developed countries, and it is usually apparent in conditions of poverty, malnutrition, and chronic alcoholism.[9] It also tends to occur in areas where people eat maize (corn, the only grain low in digestible niacin) as a staple food. A special cooking technique called nixtamalization is needed to increase the bioavailability of niacin during maize meal/flour production.
Mild niacin deficiency has been shown to slow metabolism, causing decreased tolerance to cold.
Severe deficiency of niacin in the diet causes the disease pellagra, which is characterized by diarrhea, dermatitis, and dementia, as well as “necklace” lesions on the lower neck, hyperpigmentation, thickening of the skin, inflammation of the mouth and tongue, digestive disturbances, amnesia, delirium, and eventually death, if left untreated.[10] Common psychiatric symptoms of niacin deficiency include irritability, poor concentration, anxiety, fatigue, restlessness, apathy, and depression.[10] Studies have indicated that, in patients with alcoholic pellagra, niacin deficiency may be an important factor influencing both the onset and severity of this condition. Alcoholic patients typically experience increased intestinal permeability, leading to negative health outcomes.
Hartnup’s disease is a hereditary nutritional disorder resulting in niacin deficiency.[10] This condition was first identified in the 1950s by the Hartnup family in London. It is due to a deficit in the intestines and kidneys, making it difficult for the body to break down and absorb dietary tryptophan. The resulting condition is similar to pellagra, including symptoms of red, scaly rash, and sensitivity to sunlight. Oral niacin is given as a treatment for this condition in doses ranging from 40–200 mg, with a good prognosis if identified and treated early.[10] Niacin synthesis is also deficient in carcinoid syndrome, because of metabolic diversion of its precursor tryptophan to form serotonin.
Lipid-modifying effects
Niacin blocks the breakdown of fats in adipose tissue. These fats are used to build very-low-density lipoproteins (VLDL) in the liver, which are precursors of low-density lipoprotein (LDL) or "bad" cholesterol. Because niacin blocks the breakdown of fats, it causes a decrease in free fatty acids in the blood and, as a consequence, decreases the secretion of VLDL and cholesterol by the liver.[11]
By lowering VLDL levels, niacin also increases the level of high-density lipoprotein (HDL) or "good" cholesterol in blood, and therefore it is sometimes prescribed for people with low HDL, who are also at high risk of a heart attack.[12][13]
The ARBITER 6-HALTS study, reported at the 2009 annual meeting of the American Heart Association and in the New England Journal of Medicine[14] concluded that, when added to statins, 2000 mg/day of slow-release niacin was more effective than ezetimibe (Zetia) in reducing carotid intima-media thickness, a marker of atherosclerosis.[15] Additionally, a recent meta-analysis covering 11 randomized controlled clinical trials found positive effects of niacin alone or in combination on all cardiovascular events and on atherosclerosis evolution.[16]
However, a 2011 study (AIM-HIGH) was halted early because patients showed no decrease in cardiovascular events, but did experience an increase in the risk of stroke. These patients already had LDL levels well-controlled by a statin drug, and the aim of the study was to evaluate slow-release niacin (2000 mg per day) to see if raising HDL levels had an additional positive effect on risk. In this study, it did not have such an effect, and appeared to increase stroke risk.[17] The role of niacin in patients whose LDL is not well-controlled (as in the majority of previous studies with niacin) is still under study and debate. However, it does not seem to offer benefits via raising HDL, in patients already lowering LDL by taking a statin.
Toxicity
Pharmacological doses of niacin (1.5 - 6 g per day) occasionally lead to side effects that can include dermatological conditions such as skin flushing and itching, dry skin, and skin rashes including eczema exacerbation and acanthosis nigricans. These symptoms are generally related to niacin's role as the rate limiting cofactor in the histidine decarboxylase enzyme which converts l-histidine into histamine.[citation needed] H1 and H2 receptor mediated histamine is metabolized via a sequence of mono (or di-) amine oxidase and COMT into methylhistamine which is then conjugated through the liver's CYP450 pathways. Persistent flushing and other symptoms may indicate deficiencies in one or more of the cofactors responsible for this enzymatic cascade. Gastrointestinal complaints, such as dyspepsia (indigestion), nausea and liver toxicity fulminant hepatic failure, have also been reported. Side effects of hyperglycemia, cardiac arrhythmias and "birth defects in experimental animals" have also been reported.[18] The flush lasts for about 15 to 30 minutes, and is sometimes accompanied by a prickly or itching sensation, in particular, in areas covered by clothing. This effect is mediated by prostaglandin and can be blocked by taking 300 mg of aspirin half an hour before taking niacin, or by taking one tablet of ibuprofen per day. Taking the niacin with meals also helps reduce this side effect. After several weeks of a consistent dose, most patients no longer flush.[19] Slow- or "sustained"-release forms of niacin have been developed to lessen these side effects.[11][20] One study showed the incidence of flushing was significantly lower with a sustained release formulation[21] though doses above 2 g per day have been associated with liver damage, in particular, with slow-release formulations.[18] Flushing is often thought to involve histamine, but histamine has been shown not to be involved in the reaction.[22] Prostaglandin (PGD2) is the primary cause of the flushing reaction, with serotonin appearing to have a secondary role in this reaction.[22]
Although high doses of niacin may elevate blood sugar, thereby worsening diabetes mellitus,[18] recent studies show the actual effect on blood sugar to be only 5–10%. Patients with diabetes who continued to take anti-diabetes drugs containing niacin did not experience major blood glucose changes. Thus looking at the big picture, niacin continues to be recommended as a drug for preventing CVD in patients with diabetes.
Hyperuricemia is another side effect of taking high-dose niacin, and may exacerbate gout.[23]
Niacin in doses used to lower cholesterol levels has been associated with birth defects in laboratory animals, with possible consequences for infant development in pregnant women.[18]
Niacin, particularly the time-release variety, at extremely high doses can cause acute toxic reactions.[24] Extremely high doses of niacin can also cause niacin maculopathy, a thickening of the macula and retina, which leads to blurred vision and blindness. This maculopathy is reversible after niacin intake ceases.[25]
Inositol hexanicotinate
One form of dietary supplement is inositol hexanicotinate (IHN), which is inositol that has been esterified with niacin on all six of inositol's alcohol groups. IHN is usually sold as "flush-free" or "no-flush" niacin in units of 250, 500, or 1000 mg/tablets or capsules. It is sold as an over-the-counter formulation, and often is marketed and labeled as niacin, thus misleading consumers into thinking they are getting the active form of the medication. While this form of niacin does not cause the flushing associated with the immediate-release products, the evidence that it has lipid-modifying functions is contradictory, at best. As the clinical trials date from the early 1960s (Dorner, Welsh) or the late 1970s (Ziliotto, Kruse, Agusti), it is difficult to assess them by today's standards.[26] One of the last of those studies affirmed the superiority of inositol and xantinol esters of nicotinic acid for reducing serum free fatty acid,[27] but other studies conducted during the same period found no benefit.[28] Studies explain that this is primarily because "flush-free" preparations do not contain any free nicotinic acid. A more recent placebo-controlled trial was small (n=11/group), but results after three months at 1500 mg/day showed no trend for improvements in total cholesterol, LDL-C, HDL-C or triglycerides.[29] Thus, so far there is not enough evidence to recommend IHN to treat dyslipidemia. Furthermore, the American Heart Association and the National Cholesterol Education Program both take the position that only prescription niacin should be used to treat dyslipidemias, and only under the management of a physician. The reason given is that niacin at effective intakes of 1500–3000 mg/day can also potentially have severe adverse effects. Thus liver function tests to monitor liver enzymes are necessary when taking therapeutic doses of niacin, including alkaline phosphatase (ALP), aspartate transaminase (AST), and alanine transaminase (ALT).
Biosynthesis and chemical synthesis
 Biosynthesis
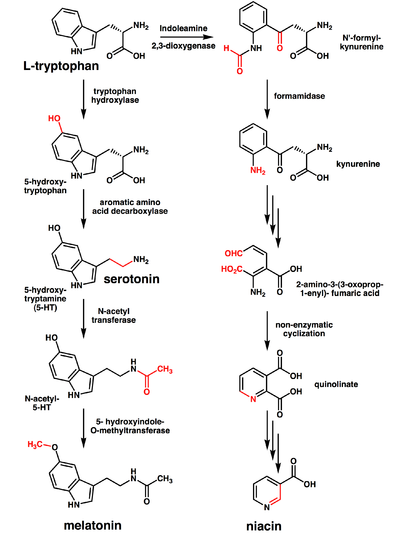
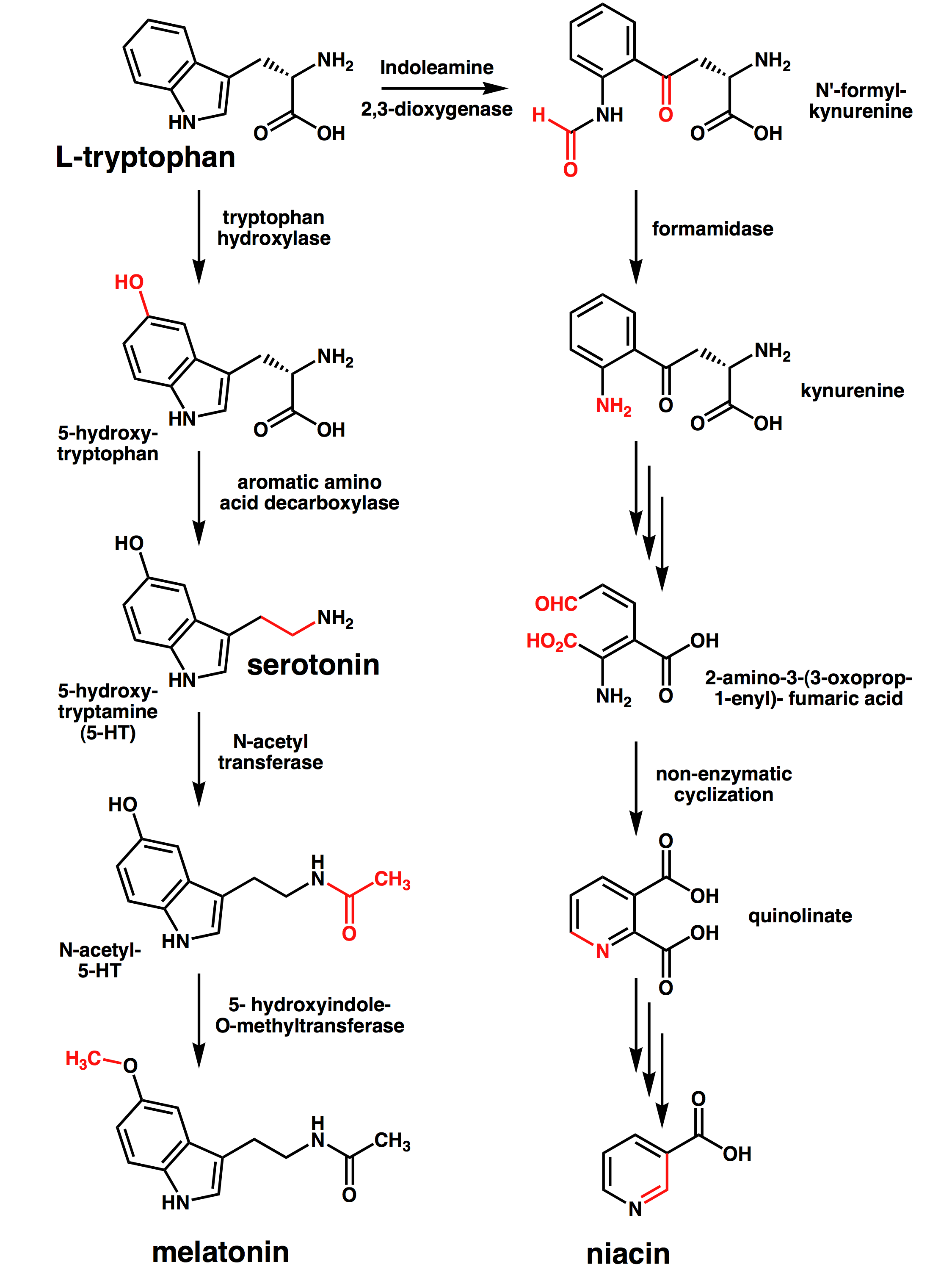
BiosynthesisThe liver can synthesize niacin from the essential amino acid tryptophan, requiring 60 mg of tryptophan to make one mg of niacin.[6] The 5-membered aromatic heterocycle of tryptophan is cleaved and rearranged with the alpha amino group of tryptophan into the 6-membered aromatic heterocycle of niacin. Riboflavin, Vitamin B6 and iron are required in some of the reactions involved in the conversion of tryptophan to NAD.
Several million kilograms of niacin are manufactured each year, starting from 3-methylpyridine.
Receptor
In addition to its effects as NAD and NADP, niacin may have additional effects by receptor activation. The receptor for niacin is a G protein-coupled receptor called HM74A.[30] It couples to the Gi alpha subunit.[31]
Food sources
Niacin is found in variety of foods, including liver, chicken, beef, fish, cereal, peanuts and legumes, and is also synthesized from tryptophan, which is found in meat, dairy and eggs.
Animal products:
Fruits and vegetables:
Seeds:
- nuts
- whole grain products
- legumes
- saltbush seeds
Fungi:
- mushrooms
- brewer's yeast
Other:
- Vegemite (from spent brewer's yeast)
History
Niacin was first described by Hugo Weidel in 1873 in his studies of nicotine.[32] The original preparation remains useful: The oxidation of nicotine using nitric acid.[33] Niacin was extracted from livers by Conrad Elvehjem, who later identified the active ingredient, then referred to as the "pellagra-preventing factor" and the "anti-blacktongue factor."[34] When the biological significance of nicotinic acid was realized, it was thought appropriate to choose a name to dissociate it from nicotine, to avoid the perception that vitamins or niacin-rich food contains nicotine, or that cigarettes contain vitamins. The resulting name 'niacin' was derived from nicotinic acid + vitamin.
Carpenter found in 1951 that niacin in corn is biologically unavailable, and can be released only in very alkaline lime water of pH 11.[35] This process, known as nixtamalization, was discovered by the prehistoric civilizations of Mesoamerica.[36]
Niacin is referred to as vitamin B3 because it was the third of the B vitamins to be discovered. It has historically been referred to as "vitamin PP" or "vitamin P-P".
Research
As of August 2008[update], a combination of niacin with laropiprant is being tested in a clinical trial. Laropiprant reduces facial flushes induced by niacin.[37]
References
- ^ "Niacin — PubChem Public Chemical Database". The PubChem Project. USA: National Center for Biotechnology Information. http://pubchem.ncbi.nlm.nih.gov/summary/summary.cgi?cid=938.
- ^ "NIH stops clinical trial on combination cholesterol treatment". National Institutes of Health. May 26, 2011. http://www.nih.gov/news/health/may2011/nhlbi-26.htm. Retrieved October 4, 2011.
- ^ Jaconello P (October 1992). "Niacin versus niacinamide". CMAJ 147 (7): 990. PMC 1336277. PMID 1393911. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1336277.
- ^ Knip M, Douek IF, Moore WP, et al. (2000). "Safety of high-dose nicotinamide: a review". Diabetologia 43 (11): 1337–45. doi:10.1007/s001250051536. PMID 11126400.
- ^ Cox, Michael; Lehninger, Albert L; Nelson, David R. (2000). Lehninger principles of biochemistry. New York: Worth Publishers. ISBN 1-57259-153-6.
- ^ a b Jacobson, EL (2007). "Niacin". Linus Pauling Institute. http://lpi.oregonstate.edu/infocenter/vitamins/niacin/. Retrieved 2011-08-08.
- ^ Institute of Medicine (2006). Dietary Reference Intakes Research Synthesis: Workshop Summary. National Academies Press. p. 37. http://books.nap.edu/openbook.php?record_id=11767&page=37.
- ^ Jacob RA, Swendseid ME, McKee RW, Fu CS, Clemens RA (April 1989). "Biochemical markers for assessment of niacin status in young men: urinary and blood levels of niacin metabolites". J. Nutr. 119 (4): 591–8. PMID 2522982. http://jn.nutrition.org/cgi/pmidlookup?view=long&pmid=2522982.
- ^ Pitsavas S, Andreou C, Bascialla F, Bozikas VP, Karavatos A (2004). "Pellagra encephalopathy following B-complex vitamin treatment without niacin". Int J Psychiatry Med 34 (1): 91–5. PMID 15242145. http://baywood.metapress.com/link.asp?id=29xv1gg1u17krgjh.
- ^ a b c d Prakash, Ravi; Sachin Gandotra, Lokesh Kumar Singh, Basudeb Das, Anuja Lakra (2008). "Rapid resolution of delusional parasitosis in pellagra with niacin augmentation therapy". General Hospital Psychiatry 30 (6): 581–4. doi:10.1016/j.genhosppsych.2008.04.011. PMID 19061687. http://www.sciencedirect.com/science/article/B6T70-4T24FKB-D/2/f619871a3d1f1d626b775c84523d6d94.
- ^ a b Katzung, Bertram G. (2006). Basic and clinical pharmacology. New York: McGraw-Hill Medical Publishing Division. ISBN 0071451536. http://www.medicinenet.com/niacin/article.htm.
- ^ McGovern ME (2005). "Taking aim at HDL-C. Raising levels to reduce cardiovascular risk". Postgrad Med 117 (4): 29–30, 33–5, 39 passim. PMID 15842130.
- ^ Canner PL, Berge KG, Wenger NK, et al. (1986). "Fifteen year mortality in Coronary Drug Project patients: long-term benefit with niacin". J. Am. Coll. Cardiol. 8 (6): 1245–55. doi:10.1016/S0735-1097(86)80293-5. PMID 3782631.
- ^ Taylor AJ, Villines TC, Stanek EJ, et al. (November 2009). "Extended-release niacin or ezetimibe and carotid intima-media thickness". N. Engl. J. Med. 361 (22): 2113–22. doi:10.1056/NEJMoa0907569. PMID 19915217.
- ^ Singer, Natasha (November 15, 2009). "Study Raises Questions About Cholesterol Drug’s Benefit". The New York Times. http://www.nytimes.com/2009/11/16/health/research/16heart.html. Retrieved November 16, 2009.
- ^ Bruckert, E; Labreuche, J; Amarenco, P (2010). "Meta-analysis of the effect of nicotinic acid alone or in combination on cardiovascular events and atherosclerosis". Atherosclerosis 210 (2): 353–61. doi:10.1016/j.atherosclerosis.2009.12.023. PMID 20079494.
- ^ http://www.npr.org/blogs/health/2011/05/28/136678665/study-boosting-good-cholesterol-with-niacin-did-not-cut-heart-risks?ps=sh_sthdl
- ^ a b c d Keith Parker; Laurence Brunton; Goodman, Louis Sanford; Lazo, John S.; Gilman, Alfred (2006). Goodman & Gilman's the pharmacological basis of therapeutics. New York: McGraw-Hill. ISBN 0071422803.
- ^ "Guidelines for Niacin Therapy For the Treatment of Elevated Lipoprotein a (Lpa)". Rush Hemophilia & Thrombophilia Center. August 15, 2002, Revised July 27, 2005. http://www.rush.edu/Rush_Document/Niacin%20therapy%20for%20elevated%20Lpa,0.pdf. Retrieved 20 November 2009. "facial flushing is a common side effect of niacin therapy that usually subsides after several weeks of consistent niacin use"
- ^ Barter, P (2006). "Options for therapeutic intervention: How effective are the different agents?". European Heart Journal Supplements 8 (F): F47–F53. doi:10.1093/eurheartj/sul041.
- ^ Chapman MJ, Assmann G, Fruchart JC, Shepherd J, Sirtori C (2004). "Raising high-density lipoprotein cholesterol with reduction of cardiovascular risk: the role of nicotinic acid—a position paper developed by the European Consensus Panel on HDL-C". Curr Med Res Opin 20 (8): 1253–68. doi:10.1185/030079904125004402. PMID 15324528.
- ^ a b Papaliodis D, Boucher W, Kempuraj D, Michaelian M, Wolfberg A, House M, Theoharides TC (December 2008). "Niacin-induced "Flush" Involves Release of Prostaglandin D2 from Mast Cells and Serotonin from Platelets: Evidence from Human Cells in Vitro and an Animal Model". J Pharmacol Exp Ther 327 (3): 665–72. doi:10.1124/jpet.108.141333. PMID 18784348. http://jpet.aspetjournals.org/cgi/pmidlookup?view=long&pmid=18784348.
- ^ Capuzzi DM, Morgan JM, Brusco OA, Intenzo CM (2000). "Niacin dosing: relationship to benefits and adverse effects". Curr Atheroscler Rep 2 (1): 64–71. doi:10.1007/s11883-000-0096-y. PMID 11122726.
- ^ Mittal MK, Florin T, Perrone J, Delgado JH, Osterhoudt KC (2007). "Toxicity from the use of niacin to beat urine drug screening". Ann Emerg Med 50 (5): 587–90. doi:10.1016/j.annemergmed.2007.01.014. PMID 17418450.
- ^ Gass JD (2003). "Nicotinic acid maculopathy. 1973". Retina (Philadelphia, Pa.) 23 (6 Suppl): 500–10. PMID 15035390.
- ^ Taheri, R (2003-01-15). "No-Flush Niacin for the Treatment of Hyperlipidemia". Medscape. http://www.medscape.com/viewarticle/447528. Retrieved 2008-03-31.
- ^ Kruse W, Kruse W, Raetzer H, Heuck CC, Oster P, Schellenberg B, Schlierf G (1979). "Nocturnal inhibition of lipolysis in man by nicotinic acid and derivatives". European Journal of Clinical Pharmacology 16 (1): 11–15. doi:10.1007/BF00644960. PMID 499296.
- ^ Meyers CD, Carr MC, Park S, Brunzell JD (2003). "Varying cost and free nicotinic acid content in over-the-counter niacin preparations for dyslipidemia". Annals of Internal Medicine 139 (12): 996–1002. PMID 14678919. http://www.annals.org/content/139/12/996.full.pdf+html.
- ^ Benjó AM, Maranhão RC, Coimbra SR, Andrade AC, Favarato D, Molina MS, Brandizzi LI, da Luz PL (2006). "Accumulation of chylomicron remnants and impaired vascular reactivity occur in subjects with isolated low HDL cholesterol: effects of niacin treatment". Atherosclerosis 187 (1): 116–122. doi:10.1016/j.atherosclerosis.2005.08.025. PMID 16458316.
- ^ Zhang Y, Schmidt RJ, Foxworthy P, et al. (2005). "Niacin mediates lipolysis in adipose tissue through its G-protein coupled receptor HM74A". Biochem. Biophys. Res. Commun. 334 (2): 729–32. doi:10.1016/j.bbrc.2005.06.141. PMID 16018973.
- ^ Zellner C, Pullinger CR, Aouizerat BE, et al. (2005). "Variations in human HM74 (GPR109B) and HM74A (GPR109A) niacin receptors". Hum. Mutat. 25 (1): 18–21. doi:10.1002/humu.20121. PMID 15580557.
- ^ Weidel, H (1873). "Zur Kenntniss des Nicotins". Justus Liebig's Annalen der Chemie und Pharmacie 165 (2): 330–349. doi:10.1002/jlac.18731650212.
- ^ Samuel M. McElvain (1941), "Nicotinic Acid", Org. Synth., http://www.orgsyn.org/orgsyn/orgsyn/prepContent.asp?prep=CV1P0385.pdf; Coll. Vol. 1: 385
- ^ Elvehjem CA, Madden RJ, Strongandd FM, Woolley DW (1938). "The isolation and identification of the anti-blacktongue factor J" (PDF). J. Biol. Chem. 123: 137–149. http://www.jbc.org/content/123/1/137.full.pdf.
- ^ LAGUNA J, CARPENTER KJ (September 1951). "Raw versus processed corn in niacin-deficient diets". J. Nutr. 45 (1): 21–8. PMID 14880960. http://jn.nutrition.org/cgi/pmidlookup?view=long&pmid=14880960.
- ^ "Vitamin B3". University of Maryland Medical Center. 2002-01-04. http://www.umm.edu/altmed/articles/vitamin-b3-000335.htm. Retrieved 2008-03-31.
- ^ Paolini JF, Bays HE, Ballantyne CM, et al. (November 2008). "Extended-release niacin/laropiprant: reducing niacin-induced flushing to better realize the benefit of niacin in improving cardiovascular risk factors". Cardiol Clin 26 (4): 547–60. doi:10.1016/j.ccl.2008.06.007. PMID 19031552.
Vitamins (A11) Fat soluble D2 (Ergosterol, Ergocalciferol#) · D3 (7-Dehydrocholesterol, Previtamin D3, Cholecalciferol, 25-hydroxycholecalciferol, Calcitriol (1,25-dihydroxycholecalciferol), Calcitroic acid) · D4 (Dihydroergocalciferol) · D5 · D analogues (Dihydrotachysterol, Calcipotriol, Tacalcitol, Paricalcitol)Water soluble B1 (Thiamine#) · B2 (Riboflavin#) · B3 (Niacin, Nicotinamide#) · B5 (Pantothenic acid, Dexpanthenol, Pantethine) · B6 (Pyridoxine#, Pyridoxal phosphate, Pyridoxamine) · B7 (Biotin) · B9 (Folic acid, Dihydrofolic acid, Folinic acid) · B12 (Cyanocobalamin, Hydroxocobalamin, Methylcobalamin, Cobamamide) · CholineCombinations M: NUT
cof, enz, met
noco, nuvi, sysi/epon, met
drug(A8/11/12)
Peripheral vasodilators (C04) 2-amino-1-phenylethanol derivatives Isoxsuprine • Buphenine • BamethanImidazoline derivatives/
Alpha blockersNiacin and derivatives Niacin • Nicotinyl alcohol • Inositol nicotinate • CiclonicatePurine derivatives Pentifylline • Xantinol nicotinate • Pentoxifylline • Etofylline nicotinateErgot alkaloids Other peripheral vasodilators Cyclandelate • Phenoxybenzamine • Vincamine • Moxisylyte • Bencyclane • Vinburnine • Sulcotidil • Buflomedil • Naftidrofuryl • Butalamine • Visnadine • Cetiedil • Cinepazide • Ifenprodil • Azapetine • FasudilLipid modifying agents (C10) GI tract Ezetimibe • SCH-48461Liver Simvastatin# • Atorvastatin • Fluvastatin • Lovastatin • Mevastatin • Pitavastatin • Pravastatin • Rosuvastatin • Cerivastatin‡Blood vessels CETP inhibitors (HDL)Combinations Other Dextrothyroxine • Probucol • Tiadenol • Benfluorex • Meglutol • Omega-3-triglycerides • Magnesium pyridoxal 5-phosphate glutamate • Policosanol • Lapaquistat§ • Alipogene tiparvovecCategories:- Hypolipidemic agents
- B vitamins
- Inositol
- Nicotinic acids
- Oc(:o):c1cccnc1



Wikimedia Foundation. 2010.