- Liver
-
For other uses, see Liver (disambiguation).
Liver 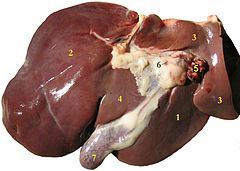
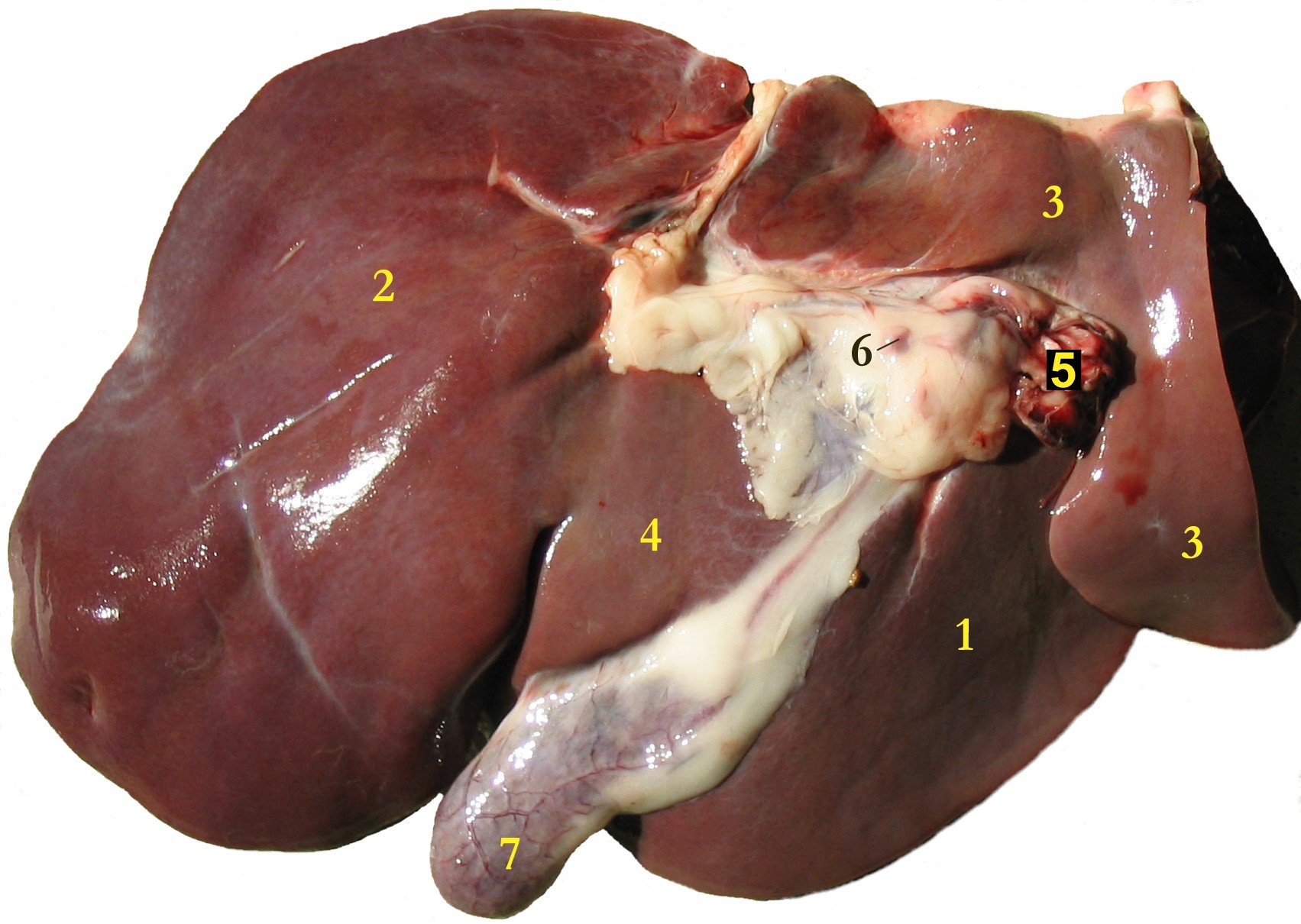
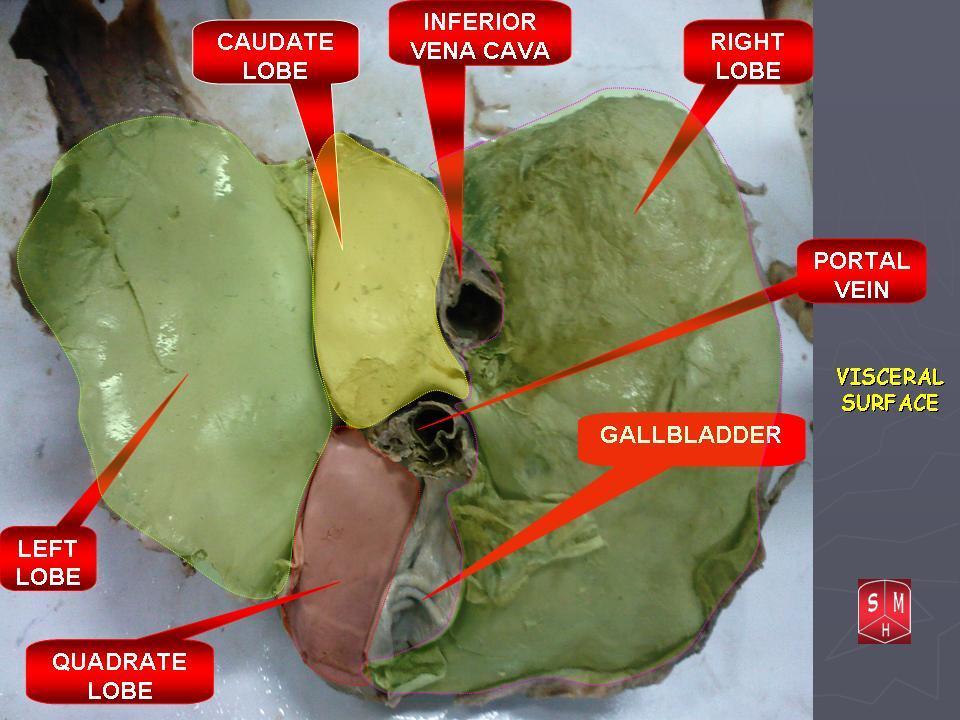
Liver of a sheep: (1) right lobe, (2) left lobe, (3) caudate lobe, (4) quadrate lobe, (5) hepatic artery and portal vein, (6) hepatic lymph nodes, (7) gall bladder. 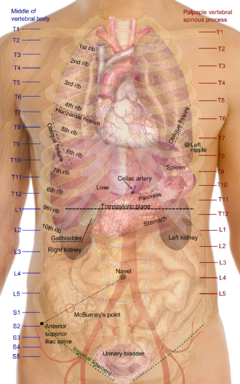
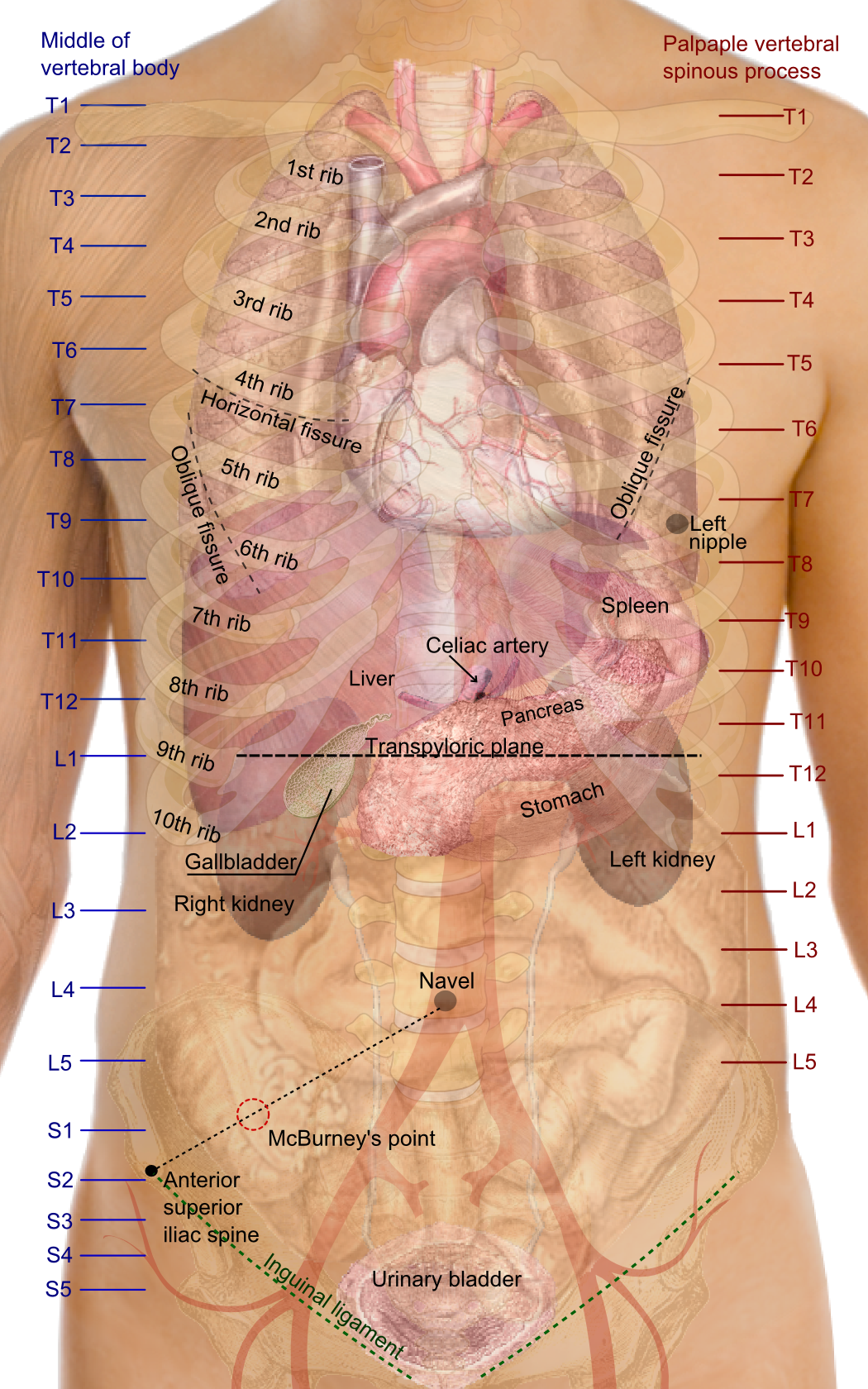
Surface projections of the organs of the trunk, showing liver in center Latin jecur, iecer Gray's subject #250 1188 Vein hepatic vein, hepatic portal vein Nerve celiac ganglia, vagus[1] Precursor foregut MeSH Liver The liver is a vital organ present in vertebrates and some other animals. It has a wide range of functions, including detoxification, protein synthesis, and production of biochemicals necessary for digestion. The liver is necessary for survival; there is currently no way to compensate for the absence of liver function long term, although liver dialysis can be used short term.
This organ plays a major role in metabolism and has a number of functions in the body, including glycogen storage, decomposition of red blood cells, plasma protein synthesis, hormone production, and detoxification. It lies below the diaphragm in the abdominal-pelvic region of the abdomen. It produces bile, an alkaline compound which aids in digestion via the emulsification of lipids. The liver's highly specialized tissues regulate a wide variety of high-volume biochemical reactions, including the synthesis and breakdown of small and complex molecules, many of which are necessary for normal vital functions.[2]
Medical terms related to the liver often start in hepato- or hepatic from the Greek word for liver, hēpar (ἡπαρ).
Contents
Anatomy
The liver is a reddish brown organ with four lobes of unequal size and shape. A human liver normally weighs 1.44–1.66 kg (3.2–3.7 lb),[3] and is a soft, pinkish-brown, triangular organ. It is both the largest internal organ (the skin being the largest organ overall) and the largest gland in the human body. It is located in the right upper quadrant of the abdominal cavity, resting just below the diaphragm. The liver lies to the right of the stomach and overlies the gallbladder. It is connected to two large blood vessels, one called the hepatic artery and one called the portal vein. The hepatic artery carries blood from the aorta, whereas the portal vein carries blood containing digested nutrients from the entire gastrointestinal tract and also from the spleen and pancreas. These blood vessels subdivide into capillaries, which then lead to a lobule. Each lobule is made up of millions of hepatic cells which are the basic metabolic cells.
 Lobes of the liver
Lobes of the liver
Blood flow
The liver gets a dual blood supply from the hepatic portal vein and hepatic arteries. Supplying approximately 75% of the liver's blood supply, the hepatic portal vein carries venous blood drained from the spleen, gastrointestinal tract, and its associated organs. The hepatic arteries supply arterial blood to the liver, accounting for the remainder of its blood flow. Oxygen is provided from both sources; approximately half of the liver's oxygen demand is met by the hepatic portal vein, and half is met by the hepatic arteries.[4]
Blood flows through the liver sinusoids and empties into the central vein of each lobule. The central veins coalesce into hepatic veins, which leave the liver.Biliary flow
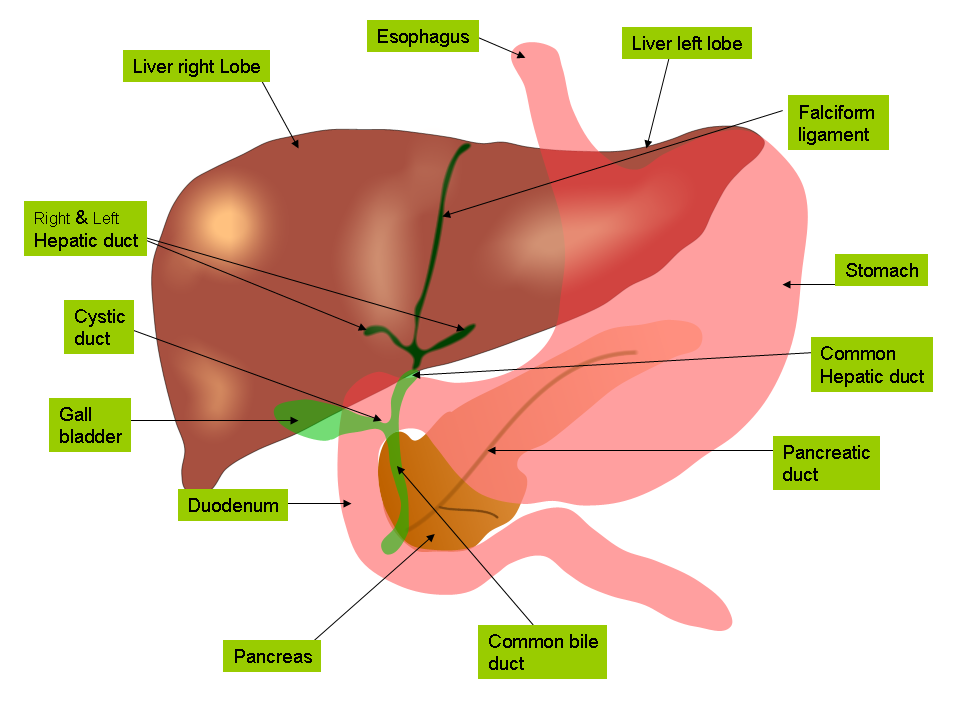
 The biliary tree
The biliary treeThe term biliary tree is derived from the arboreal branches of the bile ducts. The bile produced in the liver is collected in bile canaliculi, which merge to form bile ducts. Within the liver, these ducts are called intrahepatic (within the liver) bile ducts, and once they exit the liver they are considered extrahepatic (outside the liver). The intrahepatic ducts eventually drain into the right and left hepatic ducts, which merge to form the common hepatic duct. The cystic duct from the gallbladder joins with the common hepatic duct to form the common bile duct.
Bile can either drain directly into the duodenum via the common bile duct, or be temporarily stored in the gallbladder via the cystic duct. The common bile duct and the pancreatic duct enter the second part of the duodenum together at the ampulla of Vater.
Surface anatomy
Peritoneal ligaments
Apart from a patch where it connects to the diaphragm (the so-called "bare area"), the liver is covered entirely by visceral peritoneum, a thin, double-layered membrane that reduces friction against other organs. The peritoneum folds back on itself to form the falciform ligament and the right and left triangular ligaments.
These "lits" are in no way related to the true anatomic ligaments in joints, and have essentially no known functional importance, but they are easily recognizable surface landmarks. An exception to this is the falciform ligament, which attaches the liver to the posterior portion of the anterior body wall.
Lobes
Traditional gross anatomy divided the liver into four lobes based on surface features. The falciform ligament is visible on the front (anterior side) of the liver. This divides the liver into a left anatomical lobe, and a right anatomical lobe.
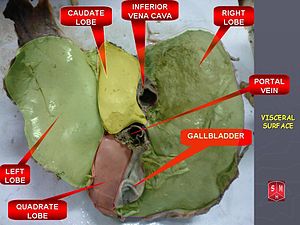
If the liver is flipped over, to look at it from behind (the visceral surface), there are two additional lobes between the right and left. These are the caudate lobe (the more superior) and the quadrate lobe (the more inferior).
From behind, the lobes are divided up by the ligamentum venosum and ligamentum teres (anything left of these is the left lobe), the transverse fissure (or porta hepatis) divides the caudate from the quadrate lobe, and the right sagittal fossa, which the inferior vena cava runs over, separates these two lobes from the right lobe.
Each of the lobes is made up of lobules; a vein goes from the centre, which then joins to the hepatic vein to carry blood out from the liver.
On the surface of the lobules, there are ducts, veins and arteries that carry fluids to and from them.
Functional anatomy
Correspondence between anatomic lobes and Couinaud segments Segment* Couinaud segments Caudate 1 Lateral 2, 3 Medial 4a, 4b Right 5, 6, 7, 8 * or lobe, in the case of the caudate lobe
Each number in the list corresponds to one in the table. 1. Caudate
2. Superior subsegment of the lateral segment
3. Inferior subsegment of the lateral segment
4a. Superior subsegment of the medial segment
4b. Inferior subsegment of the medial segment
5. Inferior subsegment of the anterior segment
6. Inferior subsegment of the posterior segment
7. Superior subsegment of the posterior segment
8. Superior subsegment of the anterior segmentThe central area where the common bile duct, hepatic portal vein, and hepatic artery proper enter is the hilum or "porta hepatis". The duct, vein, and artery divide into left and right branches, and the portions of the liver supplied by these branches constitute the functional left and right lobes.
The functional lobes are separated by an imaginary plane joining the gallbladder fossa to the inferior vena cava. The plane separates the liver into the true right and left lobes. The middle hepatic vein also demarcates the true right and left lobes. The right lobe is further divided into an anterior and posterior segment by the right hepatic vein. The left lobe is divided into the medial and lateral segments by the left hepatic vein. The fissure for the ligamentum teres also separates the medial and lateral segments. The medial segment is also called the quadrate lobe. In the widely used Couinaud (or "French") system, the functional lobes are further divided into a total of eight subsegments based on a transverse plane through the bifurcation of the main portal vein. The caudate lobe is a separate structure which receives blood flow from both the right- and left-sided vascular branches.[5][6]
In other animals
The liver is found in all vertebrates, and is typically the largest visceral organ. Its form varies considerably in different species, and is largely determined by the shape and arrangement of the surrounding organs. Nonetheless, in most species it is divided into right and left lobes; exceptions to this general rule include snakes, where the shape of the body necessitates a simple cigar-like form. The internal structure of the liver is broadly similar in all vertebrates.[7]
An organ sometimes referred to as a liver is found associated with the digestive tract of the primitive chordate Amphioxus. However, this is an enzyme secreting gland, not a metabolic organ, and it is unclear how truly homologous it is to the vertebrate liver.[7]
Physiology
The various functions of the liver are carried out by the liver cells or hepatocytes. Currently, there is no artificial organ or device capable of emulating all the functions of the liver. Some functions can be emulated by liver dialysis, an experimental treatment for liver failure. The liver is thought to be responsible for up to 500 separate functions, usually in combination with other systems and organs.
Synthesis
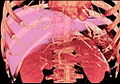
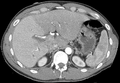
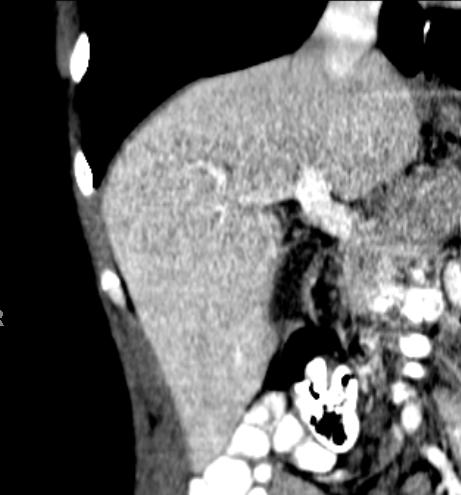
Further information: Proteins produced and secreted by the liver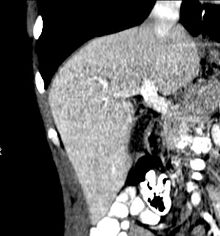 A CT scan in which the liver and portal vein are shown.
A CT scan in which the liver and portal vein are shown.- A large part of amino acid synthesis
- The liver performs several roles in carbohydrate metabolism:
- Gluconeogenesis (the synthesis of glucose from certain amino acids, lactate or glycerol)
- Glycogenolysis (the breakdown of glycogen into glucose)
- Glycogenesis (the formation of glycogen from glucose)(muscle tissues can also do this)
- The liver is responsible for the mainstay of protein metabolism, synthesis as well as degradation
- The liver also performs several roles in lipid metabolism:
- Cholesterol synthesis
- Lipogenesis, the production of triglycerides (fats).
- A bulk of the lipoproteins are synthesized in the liver.
- The liver produces coagulation factors I (fibrinogen), II (prothrombin), V, VII, IX, X and XI, as well as protein C, protein S and antithrombin.
- In the first trimester fetus, the liver is the main site of red blood cell production. By the 32nd week of gestation, the bone marrow has almost completely taken over that task.
- The liver produces and excretes bile (a yellowish liquid) required for emulsifying fats. Some of the bile drains directly into the duodenum, and some is stored in the gallbladder.
- The liver also produces insulin-like growth factor 1 (IGF-1), a polypeptide protein hormone that plays an important role in childhood growth and continues to have anabolic effects in adults.
- The liver is a major site of thrombopoietin production. Thrombopoietin is a glycoprotein hormone that regulates the production of platelets by the bone marrow.
Breakdown
- The breakdown of insulin and other hormones
- The liver glucoronidates bilirubin, facilitating its excretion into bile.
- The liver breaks down or modifies toxic substances (e.g., methylation) and most medicinal products in a process called drug metabolism. This sometimes results in toxication, when the metabolite is more toxic than its precursor. Preferably, the toxins are conjugated to avail excretion in bile or urine.
- The liver converts ammonia to urea (urea cycle)
Other functions
- The liver stores a multitude of substances, including glucose (in the form of glycogen), vitamin A (1–2 years' supply), vitamin D (1–4 months' supply), vitamin B12 (1-3 years' supply), iron, and copper.
- The liver is responsible for immunological effects- the reticuloendothelial system of the liver contains many immunologically active cells, acting as a 'sieve' for antigens carried to it via the portal system.
- The liver produces albumin, the major osmolar component of blood serum.
- The liver synthesizes angiotensinogen, a hormone that is responsible for raising the blood pressure when activated by renin, an enzyme that is released when the kidney senses low blood pressure.
Diseases of the liver
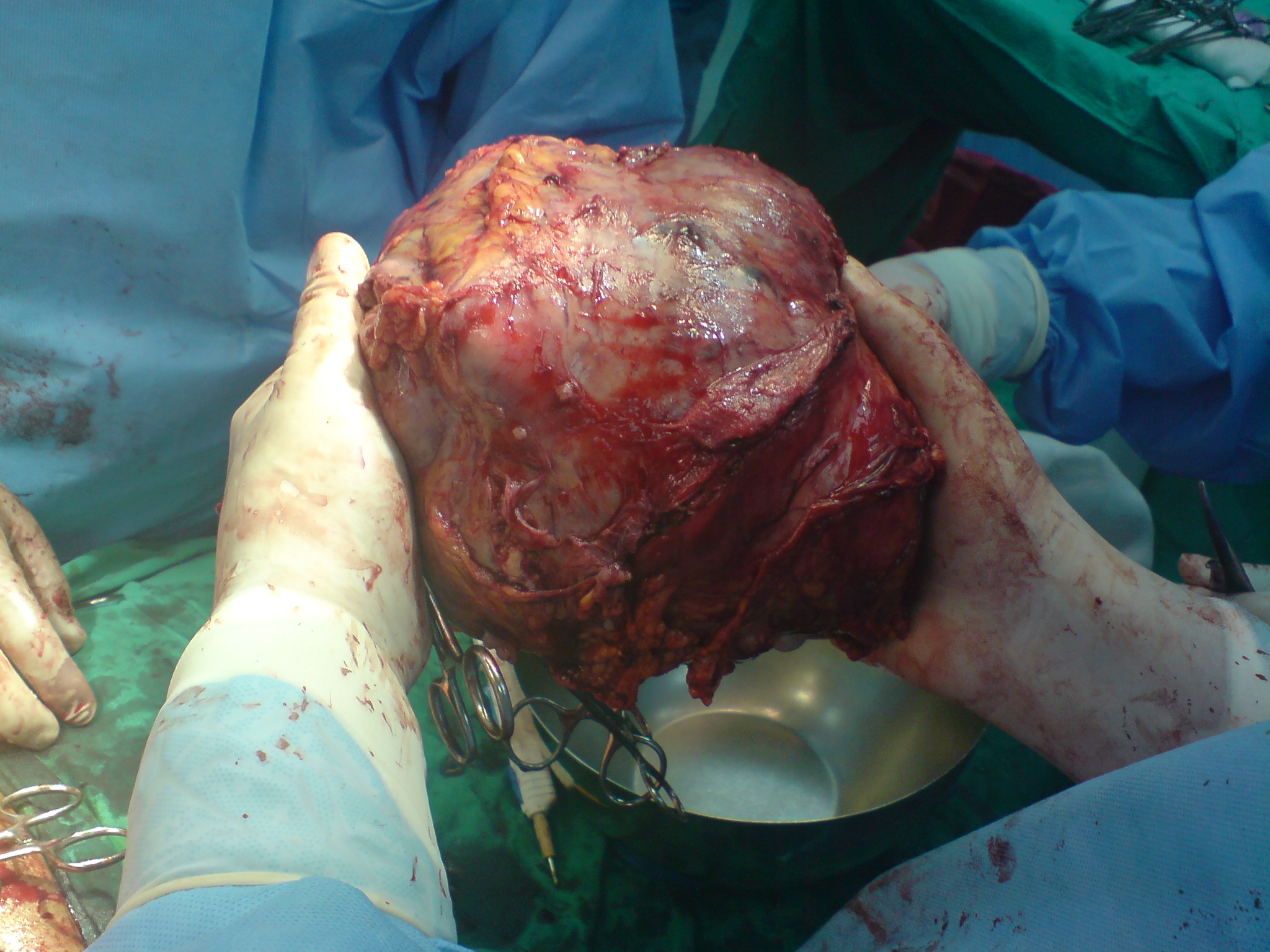
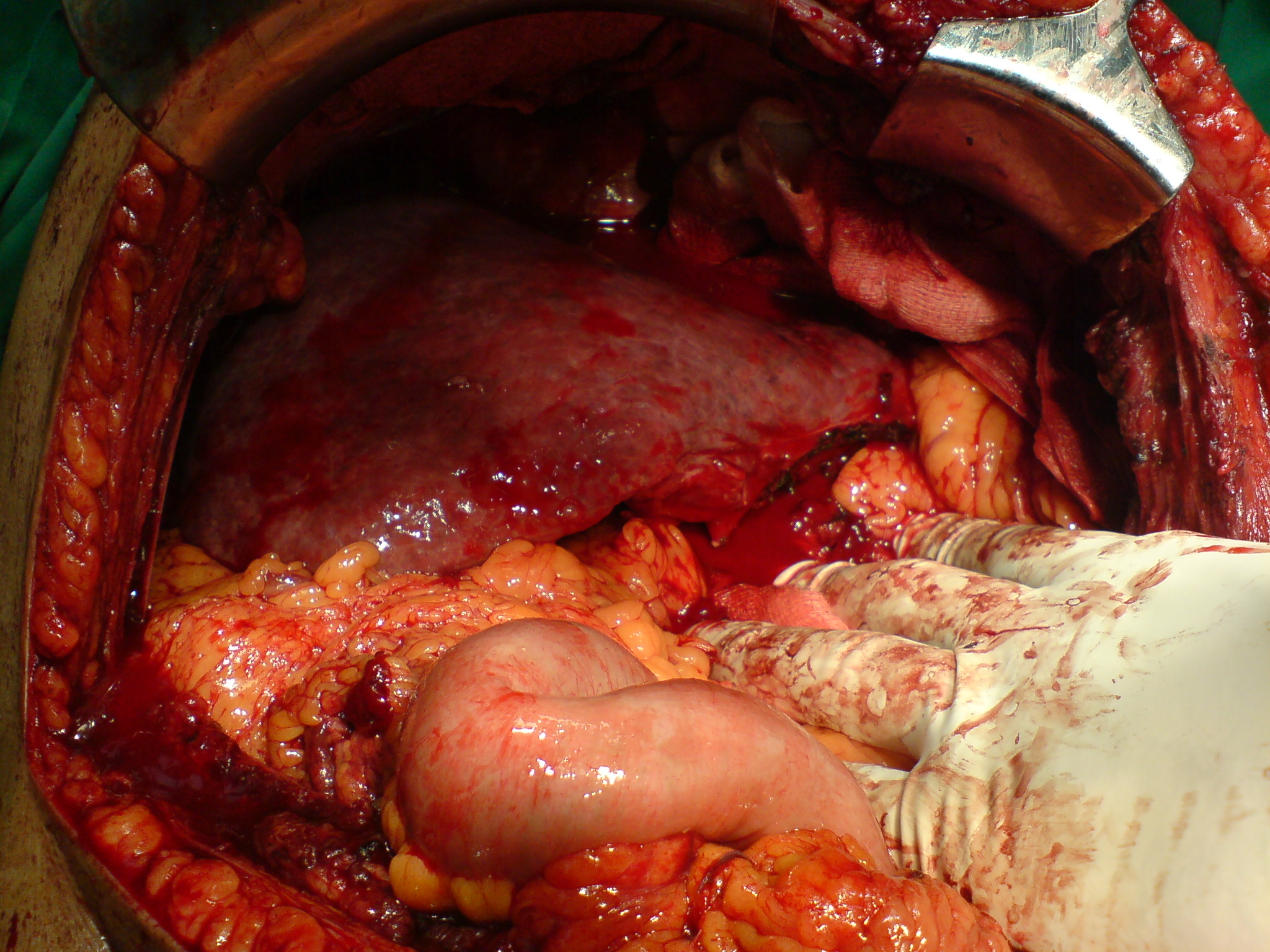
Main article: Liver disease Left lobe liver tumor
Left lobe liver tumorThe liver supports almost every organ in the body and is vital for survival. Because of its strategic location and multidimensional functions, the liver is also prone to many diseases.[8]
The most common include: Infections such as hepatitis A, B, C, E, alcohol damage, fatty liver, cirrhosis, cancer, drug damage (especially acetaminophen (also known as paracetamol) and cancer drugs)
Many diseases of the liver are accompanied by jaundice caused by increased levels of bilirubin in the system. The bilirubin results from the breakup of the hemoglobin of dead red blood cells; normally, the liver removes bilirubin from the blood and excretes it through bile.
There are also many pediatric liver diseases including biliary atresia, alpha-1 antitrypsin deficiency, alagille syndrome, progressive familial intrahepatic cholestasis, and Langerhans cell histiocytosis, to name but a few.
Diseases that interfere with liver function will lead to derangement of these processes. However, the liver has a great capacity to regenerate and has a large reserve capacity. In most cases, the liver only produces symptoms after extensive damage.
Liver diseases may be diagnosed by liver function tests, for example, by production of acute phase proteins.
Disease symptoms
The classic symptoms of liver damage include the following:
- Pale stools occur when stercobilin, a brown pigment, is absent from the stool. Stercobilin is derived from bilirubin metabolites produced in the liver.
- Dark urine occurs when bilirubin mixes with urine
- Jaundice (yellow skin and/or whites of the eyes) This is where bilirubin deposits in skin, causing an intense itch. Itching is the most common complaint by people who have liver failure. Often this itch cannot be relieved by drugs.
- Swelling of the abdomen, ankles and feet occurs because the liver fails to make albumin.
- Excessive fatigue occurs from a generalized loss of nutrients, minerals and vitamins.
- Bruising and easy bleeding are other features of liver disease. The liver makes substances which help prevent bleeding. When liver damage occurs, these substances are no longer present and severe bleeding can occur.[9]
Diagnosis
The diagnosis of liver function is made by blood tests. Liver function tests can readily pinpoint the extent of liver damage. If infection is suspected, then other serological tests are done. Sometimes, one may require an ultrasound or a CT scan to produce an image of the liver.
Physical examination of the liver is not accurate in determining the extent of liver damage. It can only reveal presence of tenderness or the size of liver, but in all cases, some type of radiological study is required to examine it.[10]
Biopsy
The ideal way to determine damage to the liver is with a biopsy. A biopsy is not required in all cases, but may be necessary when the cause is unknown. A needle is inserted into the skin just below the rib cage and a biopsy is obtained. The tissue is sent to the laboratory, where it is analyzed under a microscope. Sometimes, a radiologist may assist the physician performing a liver biopsy by providing ultrasound guidance.[11]
Regeneration
The liver is the only internal human organ capable of natural regeneration of lost tissue; as little as 25% of a liver can regenerate into a whole liver. This is, however, not true regeneration but rather compensatory growth.[12] The lobes that are removed do not regrow and the growth of the liver is a restoration of function, not original form. This contrasts with true regeneration where both original function and form are restored.
This is predominantly due to the hepatocytes re-entering the cell cycle. That is, the hepatocytes go from the quiescent G0 phase to the G1 phase and undergo mitosis. This process is activated by the p75 receptors.[13] There is also some evidence of bipotential stem cells, called ovalocytes or hepatic oval cells, which are thought to reside in the canals of Hering. These cells can differentiate into either hepatocytes or cholangiocytes, the latter being the cells that line the bile ducts.
Scientific and medical works about liver regeneration often refer to the Greek Titan Prometheus who was chained to a rock in the Caucasus where, each day, his liver was devoured by an eagle, only to grow back each night. Some think the myth indicates the ancient Greeks knew about the liver’s remarkable capacity for self-repair, though this claim has been challenged.[14]
Liver transplantation
Main article: Liver transplantationHuman liver transplants were first performed by Thomas Starzl in the United States and Roy Calne in Cambridge, England in 1963 and 1965, respectively.
 After resection of left lobe liver tumor
After resection of left lobe liver tumorLiver transplantation is the only option for those with irreversible liver failure. Most transplants are done for chronic liver diseases leading to cirrhosis, such as chronic hepatitis C, alcoholism, autoimmune hepatitis, and many others. Less commonly, liver transplantation is done for fulminant hepatic failure, in which liver failure occurs over days to weeks.
Liver allografts for transplant usually come from donors who have died from fatal brain injury. Living donor liver transplantation is a technique in which a portion of a living person's liver is removed and used to replace the entire liver of the recipient. This was first performed in 1989 for pediatric liver transplantation. Only 20 percent of an adult's liver (Couinaud segments 2 and 3) is needed to serve as a liver allograft for an infant or small child.
More recently, adult-to-adult liver transplantation has been done using the donor's right hepatic lobe, which amounts to 60 percent of the liver. Due to the ability of the liver to regenerate, both the donor and recipient end up with normal liver function if all goes well. This procedure is more controversial, as it entails performing a much larger operation on the donor, and indeed there have been at least two donor deaths out of the first several hundred cases. A recent publication has addressed the problem of donor mortality, and at least 14 cases have been found.[15] The risk of postoperative complications (and death) is far greater in right-sided operations than that in left-sided operations.
With the recent advances of noninvasive imaging, living liver donors usually have to undergo imaging examinations for liver anatomy to decide if the anatomy is feasible for donation. The evaluation is usually performed by multidetector row computed tomography (MDCT) and magnetic resonance imaging (MRI). MDCT is good in vascular anatomy and volumetry. MRI is used for biliary tree anatomy. Donors with very unusual vascular anatomy, which makes them unsuitable for donation, could be screened out to avoid unnecessary operations.
-

MDCT image. Arterial anatomy contraindicated for liver donation
-

MDCT image. Portal venous anatomy contraindicated for liver donation
-
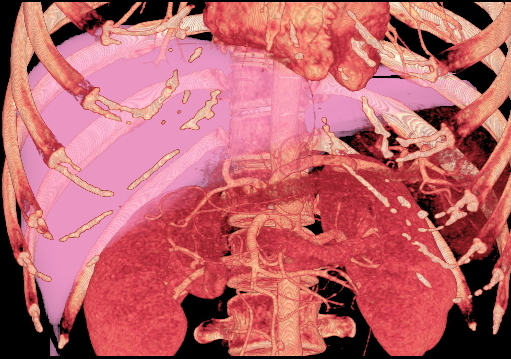
MDCT image. 3D image created by MDCT can clearly visualize the liver, measure the liver volume, and plan the dissection plane to facilitate the liver transplantation procedure.
-
Phase contrast CT image. Contrast is perfusing the right liver but not the left due to a left portal vein thrombus.
Development
Fetal blood supply
In the growing fetus, a major source of blood to the liver is the umbilical vein which supplies nutrients to the growing fetus. The umbilical vein enters the abdomen at the umbilicus, and passes upward along the free margin of the falciform ligament of the liver to the inferior surface of the liver. There it joins with the left branch of the portal vein. The ductus venosus carries blood from the left portal vein to the left hepatic vein and then to the inferior vena cava, allowing placental blood to bypass the liver.
In the fetus, the liver develops throughout normal gestation, and does not perform the normal filtration of the infant liver. The liver does not perform digestive processes because the fetus does not consume meals directly, but receives nourishment from the mother via the placenta. The fetal liver releases some blood stem cells that migrate to the fetal thymus, so initially the lymphocytes, called T-cells, are created from fetal liver stem cells. Once the fetus is delivered, the formation of blood stem cells in infants shifts to the red bone marrow.
After birth, the umbilical vein and ductus venosus are completely obliterated in two to five days; the former becomes the ligamentum teres and the latter becomes the ligamentum venosum. In the disease state of cirrhosis and portal hypertension, the umbilical vein can open up again.
As food
Main article: Liver (food)Cultural allusions
In Greek mythology, Prometheus was punished by the gods for revealing fire to humans, by being chained to a rock where a vulture (or an eagle) would peck out his liver, which would regenerate overnight. (The liver is the only human internal organ that actually can regenerate itself to a significant extent.) Many ancient peoples of the Near East and Mediterranean areas practiced a type of divination called haruspicy, where they tried to obtain information by examining the livers of sheep and other animals.
In Plato, and in later physiology, the liver was thought to be the seat of the darkest emotions (specifically wrath, jealousy and greed) which drive men to action.[16] The Talmud (tractate Berakhot 61b) refers to the liver as the seat of anger, with the gallbladder counteracting this.
The Persian, Urdu, and Hindi languages (جگر or जिगर or jigar) refer to the liver in figurative speech to indicate courage and strong feelings, or "their best"; e.g., "This Mecca has thrown to you the pieces of its liver!".[17] The term jan e jigar, literally "the strength (power) of my liver", is a term of endearment in Urdu. In Persian slang, jigar is used as an adjective for any object which is desirable, especially women. In the Zulu language, the word for liver (isibindi) is the same as the word for courage.
The legend of Liver-Eating Johnson says that he would cut out and eat the liver of each man killed after dinner.
In the motion picture The Message, Hind bint Utbah is implied or portrayed eating the liver of Hamza ibn ‘Abd al-Muttalib during the Battle of Uhud. Although there are narrations that suggest that Hind did "taste", rather than eat, the liver of Hamza, the authenticity of these narrations has to be questioned.
See also
- Artificial liver
- Bile
- Bile canaliculus
- Hepatic cyst (liver cyst)
- Hepatocyte
- Liver function tests
- Liver shot (martial arts strike)
- Polycystic liver disease
- Porto-Systemic anastomosis
References
- ^ Physiology at MCG 6/6ch2/s6ch2_30
- ^ Maton, Anthea; Jean Hopkins, Charles William McLaughlin, Susan Johnson, Maryanna Quon Warner, David LaHart, Jill D. Wright (1993). Human Biology and Health. Englewood Cliffs, New Jersey, USA: Prentice Hall. ISBN 0-13-981176-1. OCLC 32308337.
- ^ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, MO: Elsevier Saunders. p. 878. ISBN 0-7216-0187-1.
- ^ Benjamin L. Shneider; Sherman, Philip M. (2008). Pediatric Gastrointestinal Disease. Connecticut: PMPH-USA. pp. 751. ISBN 1-55009-364-9.
- ^ "Three-dimensional Anatomy of the Couinaud Liver Segments". http://dpi.radiology.uiowa.edu/nlm/app/livertoc/liver/liver.html. Retrieved 2009-02-17.
- ^ "Prof. Dr. Holger Strunk". http://www.uni-bonn.de/~umm705/quiz0403.htm. Retrieved 2009-02-17.
- ^ a b Romer, Alfred Sherwood; Parsons, Thomas S. (1977). The Vertebrate Body. Philadelphia, PA: Holt-Saunders International. pp. 354–5. ISBN 0-03-910284-X.
- ^ Cirrhosis Overview National Digestive Diseases Information Clearinghouse. Retrieved on 2010-01-22
- ^ Extraintestinal Complications: Liver Disease Crohn's & Colitis Foundation of America. Retrieved on 2010-01-22
- ^ Liver Information HealthLine. Retrieved on 2010-01-22
- ^ Liver.. The largest gland in the body MedicineNet. Retrieved on 2010-01-22
- ^ Robbins and Cotran Pathologic Basis of Disease (7th ed.). 1999. p. 101. ISBN 0-8089-2302-1.
- ^ Suzuki K, Tanaka M, Watanabe N, Saito S, Nonaka H, Miyajima A (July 2008). "p75 Neurotrophin receptor is a marker for precursors of stellate cells and portal fibroblasts in mouse fetal liver". Gastroenterology 135 (1): 270–281.e3. doi:10.1053/j.gastro.2008.03.075. PMID 18515089. http://linkinghub.elsevier.com/retrieve/pii/S0016-5085(08)00571-4.
- ^ An argument for the ancient Greek’s knowing about liver regeneration is provided by Chen T and Chen P (1994). "The Myth of Prometheus and the Liver". Journal of the Royal Society of Medicine 87(12): 754-755. A counterargument is provided by Power C and Rasko J (2008). "Whither Prometheus' Liver? Greek Myth and the Science of Regeneration". Annals of Internal Medicine 149(6): 421-426.
- ^ Bramstedt K (2006). "Living liver donor mortality: where do we stand?". Am. J. Gastrointestinal 101 (4): 755–9. doi:10.1111/j.1572-0241.2006.00421.x. PMID 16494593.
- ^ Krishna, Gopi; Hillman, James (commentary) (1970). Kundalini – the evolutionary energy in man. London: Stuart & Watkins. pp. 77. SBN 7224 0115 9. http://www.scribd.com/doc/7577310/KUNDALINI-the-evolutionary-energy-in-man.
- ^ THE GREAT BATTLE OF BADAR (Yaum-e-Furqan)
External links
- Liver at the Open Directory Project.
- VIRTUAL Liver - online learning resource
- Liver enzymes
Human systems and organs TA 2–4:
MSBone (Carpus · Collar bone (clavicle) · Thigh bone (femur) · Fibula · Humerus · Mandible · Metacarpus · Metatarsus · Ossicles · Patella · Phalanges · Radius · Skull (cranium) · Tarsus · Tibia · Ulna · Rib · Vertebra · Pelvis · Sternum) · CartilageTA 5–11:
splanchnic/
viscusmostly
Thoracicmostly
AbdominopelvicDigestive system+
adnexaMouth (Salivary gland, Tongue) · upper GI (Oropharynx, Laryngopharynx, Esophagus, Stomach) · lower GI (Small intestine, Appendix, Colon, Rectum, Anus) · accessory (Liver, Biliary tract, Pancreas)TA 12–16 Blood
(Non-TA)General anatomy: systems and organs, regional anatomy, planes and lines, superficial axial anatomy, superficial anatomy of limbs Categories:- Liver
- Organs



Wikimedia Foundation. 2010.