- Organ transplantation
-
Organ transplantation Intervention 
Cosmas and Damian miraculously transplant the (black) leg of a Moor onto the (white) body of Justinian. Ditzingen, 16th centuryICD-10-PCS 0?Y MeSH D016377 Organ transplantation is the moving of an organ from one body to another or from a donor site on the patient's own body, for the purpose of replacing the recipient's damaged or absent organ. The emerging field of regenerative medicine is allowing scientists and engineers to create organs to be re-grown from the patient's own cells (stem cells, or cells extracted from the failing organs). Organs and/or tissues that are transplanted within the same person's body are called autografts. Transplants that are performed between two subjects of the same species are called allografts. Allografts can either be from a living or cadaveric source.
Organs that can be transplanted are the heart, kidneys, eyes, liver, lungs, pancreas, intestine, and thymus. Tissues include bones, tendons (both referred to as musculoskeletal grafts), cornea, skin, heart valves, and veins. Worldwide, the kidneys are the most commonly transplanted organs, followed closely by the liver and then the heart. The cornea and musculoskeletal grafts are the most commonly transplanted tissues; these outnumber organ transplants by more than tenfold.
Organ donors may be living, or brain dead. Tissue may be recovered from donors who are cardiac dead – up to 24 hours past the cessation of heartbeat. Unlike organs, most tissues (with the exception of corneas) can be preserved and stored for up to five years, meaning they can be "banked". Transplantation raises a number of bioethical issues, including the definition of death, when and how consent should be given for an organ to be transplanted and payment for organs for transplantation.[1][2] Other ethical issues include transplantation tourism and more broadly the socio-economic context in which organ harvesting or transplantation may occur. A particular problem is organ trafficking.[3] Some organs, such as the brain, cannot be transplanted.
In the United States of America, tissue transplants are regulated by the U.S. Food and Drug Administration (FDA) which sets strict regulations on the safety of the transplants, primarily aimed at the prevention of the spread of communicable disease. Regulations include criteria for donor screening and testing as well as strict regulations on the processing and distribution of tissue grafts. Organ transplants are not regulated by the FDA.
Transplantation medicine is one of the most challenging and complex areas of modern medicine. Some of the key areas for medical management are the problems of transplant rejection, during which the body has an immune response to the transplanted organ, possibly leading to transplant failure and the need to immediately remove the organ from the recipient. When possible, transplant rejection can be reduced through serotyping to determine the most appropriate donor-recipient match and through the use of immunosuppressant drugs.[4]
Contents
History
Successful human allotransplants have a relatively long history of operative skills were present long before the necessities for post-operative survival were discovered. Rejection and the side effects of preventing rejection (especially infection and nephropathy) were, are, and may always be the key problem.
Several apocryphal accounts of transplants exist well prior to the scientific understanding and advancements that would be necessary for them to have actually occurred. The Chinese physician Pien Chi'ao reportedly exchanged hearts between a man of strong spirit but weak will with one of a man of weak spirit but strong will in an attempt to achieve balance in each man. Roman Catholic accounts report the 3rd-century saints Damian and Cosmas as replacing the gangrenous leg of the Roman deacon Justinian with the leg of a recently deceased Ethiopian. Most accounts have the saints performing the transplant in the 4th century, decades after their deaths; some accounts have them only instructing living surgeons who performed the procedure.
The more likely accounts of early transplants deal with skin transplantation. The first reasonable account is of the Indian surgeon Sushruta in the 2nd century BC, who used autografted skin transplantation in nose reconstruction rhinoplasty. Success or failure of these procedures is not well documented. Centuries later, the Italian surgeon Gasparo Tagliacozzi performed successful skin autografts; he also failed consistently with allografts, offering the first suggestion of rejection centuries before that mechanism could possibly be understood. He attributed it to the "force and power of individuality" in his 1596 work De Curtorum Chirurgia per Insitionem.
The first successful corneal allograft transplant was performed in 1837 in a gazelle model; the first successful human corneal transplant, a keratoplastic operation, was performed by Eduard Zirm at Olomouc Eye Clinic, now Czech Republic, in 1905. Pioneering work in the surgical technique of transplantation was made in the early 1900s by the French surgeon Alexis Carrel, with Charles Guthrie, with the transplantation of arteries or veins. Their skilful anastomosis operations, the new suturing techniques, laid the groundwork for later transplant surgery and won Carrel the 1912 Nobel Prize in Physiology or Medicine. From 1902 Carrel performed transplant experiments on dogs. Surgically successful in moving kidneys, hearts and spleens, he was one of the first to identify the problem of rejection, which remained insurmountable for decades.
Major steps in skin transplantation occurred during the First World War, notably in the work of Harold Gillies at Aldershot. Among his advances was the tubed pedicle graft, maintaining a flesh connection from the donor site until the graft established its own blood flow. Gillies' assistant, Archibald McIndoe, carried on the work into the Second World War as reconstructive surgery. In 1962 the first successful replantation surgery was performed – re-attaching a severed limb and restoring (limited) function and feeling.
The first attempted human deceased-donor transplant was performed by the Ukrainian surgeon Yu Yu Voronoy in the 1930s; rejection resulted in failure. Joseph Murray and J. Hartwell Harrison, M.D. performed the first successful transplant, a kidney transplant between identical twins, in 1954, successful because no immunosuppression was necessary in genetically identical twins.
In the late 1940s Peter Medawar, working for the National Institute for Medical Research, improved the understanding of rejection. Identifying the immune reactions in 1951 Medawar suggested that immunosuppressive drugs could be used. Cortisone had been recently discovered and the more effective azathioprine was identified in 1959, but it was not until the discovery of cyclosporine in 1970 that transplant surgery found a sufficiently powerful immunosuppressive.
Dr. Murray's success with the kidney led to attempts with other organs. There was a successful deceased-donor lung transplant into a lung cancer sufferer in June 1963 by James Hardy in Jackson, Mississippi. The patient survived for eighteen days before dying of kidney failure. Thomas Starzl of Denver attempted a liver transplant in the same year but was not successful until 1967.
The heart was a major prize for transplant surgeons. But over and above rejection issues, the heart deteriorates within minutes of death, so any operation would have to be performed at great speed. The development of the heart-lung machine was also needed. Lung pioneer James Hardy attempted a human heart transplant in 1964, but when a premature failure of the recipient's heart caught Hardy with no human donor, he used a chimpanzee heart, which failed very quickly. The first success was achieved on December 3, 1967, by Christiaan Barnard in Cape Town, South Africa. Louis Washkansky, the recipient, survived for eighteen days amid what many saw as a distasteful publicity circus. The media interest prompted a spate of heart transplants. Over a hundred were performed in 1968–69, but almost all the patients died within sixty days. Barnard's second patient, Philip Blaiberg, lived for 19 months.
It was the advent of cyclosporine that altered transplants from research surgery to life-saving treatment. In 1968 surgical pioneer Denton Cooley performed seventeen transplants, including the first heart-lung transplant. Fourteen of his patients were dead within six months. By 1984 two-thirds of all heart transplant patients survived for five years or more. With organ transplants becoming commonplace, limited only by donors, surgeons moved onto more risky fields, multiple-organ transplants on humans and whole-body transplant research on animals. On March 9, 1981, the first successful heart-lung transplant took place at Stanford University Hospital. The head surgeon, Bruce Reitz, credited the patient's recovery to cyclosporine-A.
As the rising success rate of transplants and modern immunosuppression make transplants more common, the need for more organs has become critical. Advances in living-related donor transplants have made that increasingly more common. Additionally, there is substantive research into xenotransplantation, or transgenic organs; although these forms of transplant are not yet being used in humans, clinical trials involving the use of specific cell types have been conducted with promising results, such as using porcine islets of Langerhans to treat type 1 diabetes. However, there are still many problems that would need to be solved before they would be feasible options in patients requiring transplants.
Recently, researchers have been looking into means of reducing the general burden of immunosuppression. Common approaches include avoidance of steroids, reduced exposure to calcineurin inhibitors, and other means of weaning drugs based on patient outcome and function. While short-term outcomes appear promising, long-term outcomes are still unknown, and in general, reduced immunosuppression increases the risk of rejection and decreases the risk of infection.
Many other new drugs are under development for transplantation.[5]
The emerging field of regenerative medicine promises to solve the problem of organ transplant rejection by regrowing organs in the lab, using the patients' own cells (stem cells or healthy cells extracted from the donor site.)
Timeline of successful transplants
- 1905: First successful cornea transplant by Eduard Zirm (Olomouc Eye Clinic, now Czech Republic)[6]
- 1954: First successful kidney transplant by Joseph Murray (Boston, U.S.A.)
- 1966: First successful pancreas transplant by Richard Lillehei and William Kelly (Minnesota, U.S.A.)
- 1967: First successful liver transplant by Thomas Starzl (Denver, U.S.A.)
- 1967: First successful heart transplant by Christian Barnard (Cape Town, South Africa)
- 1981: First successful heart/lung transplant by Bruce Reitz (Stanford, U.S.A.)
- 1983: First successful lung lobe transplant by Joel Cooper (Toronto, Canada)
- 1986: First successful double-lung transplant (Ann Harrison) by Joel Cooper (Toronto, Canada)
- 1995: First successful laparoscopic live-donor nephrectomy by Lloyd Ratner and Louis Kavoussi (Baltimore, U.S.A.)
- 1997 First successful allogeneic vascularized transplantation of a fresh and perfused human knee joint by G.O. Hofmann[7]
- 1998: First successful live-donor partial pancreas transplant by David Sutherland (Minnesota, U.S.A.)
- 1998: First successful hand transplant (France)
- 1999: First successful Tissue Engineered Bladder transplanted by Anthony Atala (Boston Children's Hospital, U.S.A.)[8]
- 2005: First successful partial face transplant (France)
- 2006: First jaw transplant to combine donor jaw with bone marrow from the patient, by Eric M. Genden (Mount Sinai Hospital, New York)[9]
- 2008: First successful complete full double arm transplant by Edgar Biemer, Christoph Höhnke and Manfred Stangl (Technical University of Munich, Germany)[10]
- 2008: First baby born from transplanted ovary.[11]
- 2008: First transplant of a human windpipe using a patient’s own stem cells, by Paolo Macchiarini (Barcelona, Spain)[12]
- 2008: First successful transplantation of near total area (80%) of face, (including palate, nose, cheeks, and eyelid by Maria Siemionow (Cleveland, USA)
- 2010: First full facial transplant, by Dr Joan Pere Barret and team (Hospital Universitari Vall d'Hebron on July 26, 2010 in Barcelona, Spain.)[13]
Valencia's Hospital La Fe has been given permission by Spain's National Transplant Organisation (NTO) to carry out the world's first double leg transplant.[14]
Types of transplant
Autograft
Main article: AutotransplantationTransplant of tissue to the same person. Sometimes this is done with surplus tissue, or tissue that can regenerate, or tissues more desperately needed elsewhere (examples include skin grafts, vein extraction for CABG, etc.) Sometimes an autograft is done to remove the tissue and then treat it or the person, before returning it (examples include stem cell autograft and storing blood in advance of surgery). In a rotationplasty a distal joint is used to replace a more proximal one, typically a foot and ankle joint is used to replace a knee joint. The a patient's foot is severed and reversed, the knee removed, and the tibia joined with the femur.
Allograft and allotransplantation
Main article: AllotransplantationAn allograft is a transplant of an organ or tissue between two genetically non-identical members of the same species. Most human tissue and organ transplants are allografts. Due to the genetic difference between the organ and the recipient, the recipient's immune system will identify the organ as foreign and attempt to destroy it, causing transplant rejection.
Isograft
A subset of allografts in which organs or tissues are transplanted from a donor to a genetically identical recipient (such as an identical twin). Isografts are differentiated from other types of transplants because while they are anatomically identical to allografts, they do not trigger an immune response.
Xenograft and xenotransplantation
Main article: XenotransplantationA transplant of organs or tissue from one species to another. An example are porcine heart valve transplants, which are quite common and successful. Another example is attempted piscine-primate (fish to non-human primate) transplant of islet (i.e. pancreatic or insular tissue) tissue. The latter research study was intended to pave the way for potential human use, if successful. However, xenotransplantion is often an extremely dangerous type of transplant because of the increased risk of non-compatibility, rejection, and disease carried in the tissue.
Split transplants
Sometimes a deceased-donor organ, usually a liver, may be divided between two recipients, especially an adult and a child. This is not usually a preferred option because the transplantation of a whole organ is more successful.
Domino transplants
This operation is performed on patients with cystic fibrosis because both lungs need to be replaced and it is a technically easier operation to replace the heart and lungs at the same time. As the recipient's native heart is usually healthy, it can be transplanted into someone else needing a heart transplant. This term is also used for a special form of liver transplant in which the recipient suffers from familial amyloidotic polyneuropathy, a disease where the liver slowly produces a protein that damages other organs. This patient's liver can be transplanted into an older patient who is likely to die from other causes before a problem arises.[15]
This term also refers to a series of living donor transplants in which one donor donates to the highest recipient on the waiting list and the transplant center utilizes that donation to facilitate multiple transplants. These other transplants are otherwise impossible due to blood type or antibody barriers to transplantation. The "Good Samaritan" kidney is transplanted into one of the other recipients, whose donor in turn donates his or her kidney to an unrelated recipient. Depending on the patients on the waiting list, this has sometimes been repeated for up to six pairs, with the final donor donating to the patient at the top of the list. This method allows all organ recipients to get a transplant even if their living donor is not a match to them. This further benefits patients below any of these recipients on waiting lists, as they move closer to the top of the list for a deceased-donor organ. Johns Hopkins Medical Center in Baltimore and Northwestern University's Northwestern Memorial Hospital have received significant attention for pioneering transplants of this kind. [16][17]
Major organs and tissues transplanted
Main article: Transplantable organs and tissuesThoracic organs
- Heart (Deceased-donor only)
- Lung (Deceased-donor and living-related lung transplantation)
- Heart/Lung (Deceased-donor and Domino transplant)
Abdominal organs
- Kidney (Deceased-donor and Living-Donor)
- Liver (Deceased-donor and Living-Donor)
- Pancreas (Deceased-donor only)
- Intestine (Deceased-donor and Living-Donor)
- Stomach (Deceased-donor only)
- Testis[18]
Tissues, cells, fluids
- Hand (Deceased-donor only), see the first recipient Clint Hallam
- Cornea (Deceased-donor only) see the ophthalmologist Eduard Zirm
- Skin including Face replant (autograft) and Face transplant (extremely rare)
- Islets of Langerhans (Pancreas Islet Cells) (Deceased-donor and Living-Donor)
- Bone marrow/Adult stem cell (Living-Donor and Autograft)
- Blood transfusion/Blood Parts Transfusion (Living-Donor and Autograft)
- Blood vessels (Autograft and Deceased-Donor)
- Heart valve (Deceased-Donor, Living-Donor and Xenograft[Porcine/bovine])
- Bone (Deceased-Donor and Living-Donor)
Types of donor
Organ donors may be living, or brain dead. Brain dead means the donor must have received an injury (either traumatic or pathological) to the part of the brain that controls heartbeat and breathing. Breathing is maintained via artificial sources, which, in turn, maintains heartbeat. Once brain death has been declared the person can be considered for organ donation. Criteria for brain death vary. Because less than 3% of all deaths in the U.S. are the result of brain death, the overwhelming majority of deaths are ineligible for organ donation, resulting in severe shortages. Tissue may be recovered from donors who are cardiac dead. That is, their breathing and heartbeat has ceased. They are referred to as cadaveric donors. In general, tissues may be recovered from donors up to 24 hours past the cessation of heartbeat. In contrast to organs, most tissues (with the exception of corneas) can be preserved and stored for up to five years, meaning they can be "banked." Also, more than 60 grafts may be obtained from a single tissue donor. Because of these three factors, the ability to recover from a non-heart beating donor, the ability to bank tissue, and the number of grafts available from each donor, tissue transplants are much more common than organ transplants. The American Association of Tissue Banks estimates that more than one million tissue transplants take place in the United States each year.
- Living
In "living donors", the donor remains alive and donates a renewable tissue, cell, or fluid (e.g. blood, skin), or donates an organ or part of an organ in which the remaining organ can regenerate or take on the workload of the rest of the organ (primarily single kidney donation, partial donation of liver, small bowel). Regenerative medicine may one day allow for laboratory-grown organs, using patient's own cells via stem cells, or healthy cells extracted from the failing organs.
- Deceased
Deceased (formerly cadaveric) are donors who have been declared brain-dead and whose organs are kept viable by ventilators or other mechanical mechanisms until they can be excised for transplantation. Apart from brain-stem dead donors, who have formed the majority of deceased donors for the last twenty years, there is increasing use of Donation after Cardiac Death Donors (formerly non-heart beating donors) to increase the potential pool of donors as demand for transplants continues to grow.[citation needed] These organs have inferior outcomes to organs from a brain-dead donor; however given the scarcity of suitable organs and the number of people who die waiting, any potentially suitable organ must be considered.[citation needed]
Reasons for donation and ethical issues
Living related donors donate to family members or friends in whom they have an emotional investment. The risk of surgery is offset by the psychological benefit of not losing someone related to them, or not seeing them suffer the ill effects of waiting on a list.
Paired exchange
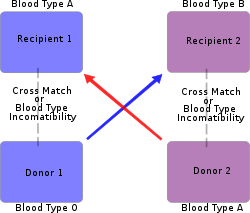 Diagram of an exchange between otherwise incompatible pairs
Diagram of an exchange between otherwise incompatible pairs
A "paired-exchange" is a technique of matching willing living donors to compatible recipients using serotyping. For example a spouse may be willing to donate a kidney to their partner but cannot since there is not a biological match. The willing spouse's kidney is donated to a matching recipient who also has an incompatible but willing spouse. The second donor must match the first recipient to complete the pair exchange. Typically the surgeries are scheduled simultaneously in case one of the donors decides to back out and the couples are kept anonymous from each other until after the transplant.
Paired exchange programs were popularized in the New England Journal of Medicine article "Ethics of a paired-kidney-exchange program" in 1997 by L.F. Ross.[19] It was also proposed by Felix T. Rapport [4] in 1986 as part of his initial proposals for live-donor transplants "The case for a living emotionally related international kidney donor exchange registry" in Transplant Proceedings.[20] A paired exchange is the simplest case of a much larger exchange registry program where willing donors are matched with any number of compatible recipients [5]. Transplant exchange programs have been suggested as early as 1970: "A cooperative kidney typing and exchange program.".[21]
The first pair exchange transplant in the U.S. was in 2001 at Johns Hopkins Hospital[6]. The first complex multihospital kidney exchange involving 12 patients was performed in February 2009 by The Johns Hopkins Hospital, Barnes-Jewish Hospital in St. Louis and Integris Baptist Medical Center in Oklahoma City.[22] Another 12-patient multihospital kidney exchange was performed four weeks later by Saint Barnabas Medical Center in Livingston, New Jersey, Newark Beth Israel Medical Center and New York-Presbyterian Hospital.[23] Surgical teams led by Johns Hopkins continue to pioneer in this field by having more complex chain of exchange such as eight-way multihospital kidney exchange.[24] In December 2009, a 13 organ 13 recipient matched kidney exchange took place, coordinated through Georgetown University Hospital and Washington Hospital Center, Washington DC.[25]
Paired-donor exchange, led by work in the New England Program for Kidney Exchange as well as at Johns Hopkins University and the Ohio OPOs may more efficiently allocate organs and lead to more transplants.
Good Samaritan
Good Samaritan or "altruistic" donation is giving a donation to someone not well-known to the donor. Some people choose to do this out of a need to donate. Some donate to the next person on the list; others use some method of choosing a recipient based on criteria important to them. Web sites are being developed that facilitate such donation. It has been featured in recent television journalism that over half of the members of the Jesus Christians, an Australian religious group, have donated kidneys in such a fashion.[26]
Compensated donation
See also: Organ theft, Organ sale, and Organ tradeIn compensated donation, donors get money or other compensation in exchange for their organs. This practice is common in some parts of the world, whether legal or not, and is one of the many factors driving medical tourism.[27]
In the United States, The National Organ Transplant Act of 1984 made organ sales illegal. In the United Kingdom, the Human Organ Transplants Act 1989 first made organ sales illegal, and has been superseded by the Human Tissue Act 2004.
In 2007, two major European conferences recommended against the sale of organs.[28]
Recent development of web sites and personal advertisements for organs among listed candidates has raised the stakes when it comes to the selling of organs, and have also sparked significant ethical debates over directed donation, "good-Samaritan" donation, and the current U.S. organ allocation policy. Bioethicist Jacob M. Appel has argued that organ solicitation on billboards and the internet may actually increase the overall supply of organs.[29]
Two books, Kidney for Sale By Owner by Mark Cherry (Georgetown University Press, 2005); and Stakes and Kidneys: Why markets in human body parts are morally imperative by James Stacey Taylor: (Ashgate Press, 2005); advocate using markets to increase the supply of organs available for transplantation. In a 2004 journal article Economist Alex Tabarrok argues that allowing organ sales, and elimination of organ donor lists will increase supply, lower costs and diminish social anxiety towards organ markets.[30]
Iran has had a legal market for kidneys since 1988,[31] and the market price is of the order of US$1,200 for the recipient.[32] The Economist[7] and the Ayn Rand Institute[8] approve and advocate a legal market elsewhere. They argued that if 0.06% of Americans between 19 and 65 were to sell one kidney, the national waiting list would disappear (which, the Economist wrote, happened in Iran). The Economist argued that donating kidneys is no more risky than surrogate motherhood, which can be done legally for pay in most countries.
In Pakistan, 40 percent to 50 percent of the residents of some villages have only one kidney because they have sold the other for a transplant into a wealthy person, probably from another country, said Dr. Farhat Moazam of Pakistan, at a World Health Organization conference. Pakistani donors are offered $2,500 for a kidney but receive only about half of that because middlemen take so much.[33] In Chennai, southern India, poor fishermen and their families sold kidneys after their livelihoods were destroyed by the Indian Ocean tsunami on December 26, 2004. About 100 people, mostly women, sold their kidneys for 40,000–60,000 rupees ($900–$1,350).[34] Thilakavathy Agatheesh, 30, who sold a kidney in May 2005 for 40,000 rupees said, "I used to earn some money selling fish but now the post-surgery stomach cramps prevent me from going to work." Most kidney sellers say that selling their kidney was a mistake.[35]
In Cyprus in 2010 police closed a fertility clinic under charges of trafficking in human eggs. The Petra Clinic, as it was known locally, imported women from Ukraine and Russia for egg harvesting and sold the genetic material to foreign fertility tourists.[36] This sort of reproductive trafficking violates laws in the European Union. In 2010 the Pulitzer Center on Crisis Reporting and the magazine Fast Company explored illicit fertility networks in Spain, the United States and Israel.[37][38]
Allocation of donated organs
The overwhelming majority of deceased-donor organs in the United States are allocated by federal contract to the Organ Procurement and Transplantation Network (OPTN), held since it was created by the Organ Transplant Act of 1984 by the United Network for Organ Sharing or UNOS. (UNOS does not handle donor cornea tissue; corneal donor tissue is usually handled by various eye banks.) UNOS allocates organs based on the method considered most fair by the scientific leadership in the field. For kidneys, for instance, that is by waiting time; for livers, it is by MELD (Model of End-Stage Liver Disease), an empirical score based on lab values indicative of the sickness of the patient from liver disease. Experiencing somewhat increased popularity, but still very rare, is directed or targeted donation, in which the family of a deceased donor (often honoring the wishes of the deceased) requests an organ be given to a specific person. If medically suitable, the allocation system is subverted, and the organ is given to that person. In the United States, there are various lengths of waiting due to the different availabilities of organs in different UNOS regions. In other countries such as the UK, only medical factors and the position on the waiting list can affect who receives the organ. If this is not the desired person, it is noted that this puts them higher on the list.
One of the more publicized cases of this type was the 1994 Chester and Patti Szuber transplant. This was the first time that a parent had received a heart donated by one of their own children. Although the decision to accept the heart from their recently killed child was not an easy decision, the Szuber family agreed that giving Patti’s heart to her father would have been something that she would have wanted.[39]
Access to organ transplantation is one reason for the growth of medical tourism.
Forced donation
See also: Organ transplants in the People's Republic of ChinaThere have been various accusations that certain authorities are harvesting organs from those the authorities deem undesirable, such as prison populations. The World Medical Association stated that individuals in detention are not in the position to give free consent to donate their organs [40][dead link]. Illegal dissection of corpses is a form of body-snatching and may have taken place to obtain allografts. [9]
According to the Chinese Deputy Minister of Health, Huang Jiefu,[41][dead link] approximately 95% of all organs used for transplantation are from executed prisoners. The lack of public organ donation program in China is used as a justification for this practice. However reports in Chinese media raised concerns if executed criminals are the only source for organs used in transplants.
In October 2007, bowing to international pressure, the Chinese Medical Association agreed on a moratorium of commercial organ harvesting from condemned prisoners, but did not specify a deadline. China agreed to restrict transplantations from donors to their immediate relatives.[42][43]
People in other parts of the world are responding to this availability of organs, and a number of individuals (including US and Japanese citizens) have elected to travel to China or India as medical tourists to receive organ transplants which may have been sourced in what might be considered elsewhere to be unethical ways (see later). [10] [11] [12].
Organ transplantation in different countries
Demographics
Despite efforts of international transplantation societies, it is not possible to access an accurate source on the number, rates and outcomes of all forms of transplantation globally; the best that we can achieve is estimations. This is not a sound basis for the future and thus one of the crucial strategies for the Global Alliance in Transplantation is to foster the collection and analysis of global data.
Transplantation of organs in different continents/regions year/ 2000
Kidney (pmp*)
Liver (pmp)
Heart (pmp)
USA 52 19 8 Europe 27 10 4 Turkey 11 3.5 1 Asia 3 0.3 0.03 Latin America 13 1.6 0.5 - All numbers per million population
According to the Council of Europe, Spain through the Spanish Transplant Organization led by Dr Rafael Matesanz shows the highest worldwide rate of 35.1[44][45] donors per million population in 2005 and 33.8[46] in 2006.
In addition to the citizens waiting for organ transplants in the US and other developed nations, there are long waiting lists in the rest of the world. More than 2 million people need organ transplants in China, 50,000 waiting in Latin America (90% of which are waiting for kidneys), as well as thousands more in the less documented continent of Africa. Donor bases vary in developing nations.
Traditionally, Muslims believe body desecration in life or death to be forbidden, and thus many reject organ transplant.[47] However most Muslim authorities nowadays accept the practice if another life will be saved.[48]
In Latin America the donor rate is 40–100 per million per year, similar to that of developed countries. However, in Uruguay, Cuba, and Chile, 90% of organ transplants came from cadaveric donors. Cadaveric donors represent 35% of donors in Saudi Arabia. There is continuous effort to increase the utilization of cadaveric donors in Asia, however the popularity of living, single kidney donors in India yields India a cadaveric donor prevalence of less than 1 pmp.
Organ transplantation in China has taken place since the 1960s, and China has one of the largest transplant programmes in the world, peaking at over 13,000 transplants a year by 2004.[49] Organ donation, however, is against Chinese tradition and culture,[50][51] and involuntary organ donation is illegal under Chinese law.[52] China's transplant programme attracted the attention of international news media in the 1990s due to ethical concerns about the organs and tissue removed from the corpses of executed criminals being commercially traded for transplants.[53][54][55]
With regard to organ transplantation in Israel, there is a severe organ shortage due to religious objections by some rabbis who oppose all organ donations and others who advocate that a rabbi participate in all decision making regarding a particular donor. One third of all heart transplants performed on Israelis are done in the Peoples' Republic of China; others are done in Europe. Dr. Jacob Lavee, head of the heart-transplant unit, Sheba Medical Center, Tel Aviv, believes that "transplant tourism" is unethical and Israeli insurers should not pay for it. The organization HODS (Halachic Organ Donor Society) is working to increase knowledge and participation in organ donation among Jews throughout the world.[56]
Transplantation rates also differ based on race, sex, and income. A study done with patients beginning long term dialysis showed that the sociodemographic barriers to renal transplantation present themselves even before patients are on the transplant list.[57] For example, different groups express definite interest and complete pretransplant workup at different rates. Previous efforts to create fair transplantation policies had focused on patients currently on the transplantation waiting list.
Comparative costs
One of the driving forces for illegal organ trafficking and for “transplantation tourism” is the price differences for organs and transplant surgeries in different areas of the world. According to the New England Journal of Medicine, a human kidney can be purchased in Manila for $1000–$2000, but in urban Latin America a kidney may cost more than $10,000. Kidneys in South Africa have sold for as high as $20,000. Price disparities based on donor race are a driving force of attractive organ sales in South Africa, as well as in other parts of the world.
In China, a kidney transplant operation runs for around $70,000, liver for $160,000, and heart for $120,000 [15]. Although these prices are still unattainable to the poor, compared to the fees of the United States, where a kidney transplant may demand $100,000, a liver $250,000, and a heart $860,000, Chinese prices have made China a major provider of organs and transplantation surgeries to other countries.
In India, a kidney transplant operation runs for around as low as $5000.
Safety
Compensation for donors also increases the risk of introducing diseased organs to recipients because these donors often yield from poorer populations unable to receive health care regularly and organ dealers may evade disease screening processes. The majority of such deals include one major payment and no follow up care for the donor. Some cases argue that there is a possibility of 1:18 to acquire HIV from such transplants.[citation needed]
In November 2007, the CDC reported the first-ever case of HIV and Hepatitis C being simultaneously transferred through an organ transplant. The donor was a 38-year-old male, considered "high-risk" by donation organizations, and his organs transmitted HIV and Hepatitis C to four organ recipients, none of whom had been told he was "high-risk." Experts say that the reason the diseases did not show up on screening tests is probably because they were contracted within three weeks before the donor's death, so antibodies would not have existed in high enough numbers to detect. The crisis has caused many to call for more sensitive screening tests, which could pick up antibodies sooner. Currently, the screens cannot pick up on the small number of antibodies produced in HIV infections within the last 90 days or Hepatitis C infections within the last 18–21 days before a donation is made.
NAT (nucleic acid testing) is now being done by many organ procurement organizations and is able to detect antibodies for HIV and Hepatitis C within seven to ten days of exposure to the virus.
Organ transplant laws
Both developing and developed countries have forged various policies to try to increase the safety and availability of organ transplants to their citizens. Brazil, France, Italy, Poland and Spain have ruled all adults potential donors with the “opting out” policy, unless they attain cards specifying not to be. However, whilst potential recipients in developing countries may mirror their more developed counterparts in desperation, potential donors in developing countries do not. The Indian government has had difficulty tracking the flourishing organ black market in their country and have yet to officially condemn it. Other countries victimized by illegal organ trade have implemented legislative reactions. Moldova has made international adoption illegal in fear of organ traffickers. China has made selling of organs illegal as of July 2006 and claims that all prisoner organ donors have filed consent. However, doctors in other countries, such as the United Kingdom, have accused China of abusing its high capital punishment rate. Despite these efforts, illegal organ trafficking continues to thrive and can be attributed to corruption in healthcare systems, which has been traced as high up as the doctors themselves in China, Ukraine, and India, and the blind eye economically strained governments and health care programs must sometimes turn to organ trafficking. Some organs are also shipped to Uganda and the Netherlands. This was a main product in the triangular trade in 1934.
Starting on May 1, 2007, doctors involved in commercial trade of organs will face fines and suspensions in China. Only a few certified hospitals will be allowed to perform organ transplants in order to curb illegal transplants. Harvesting organs without donor's consent was also deemed a crime.[58]
On June 27, 2008, Indonesian, Sulaiman Damanik, 26, pleaded guilty in Singapore court for sale of his kidney to CK Tang's executive chair, Mr Tang Wee Sung, 55, for 150 million rupiah (S$ 22,200). The Transplant Ethics Committee must approve living donor kidney transplants. Organ trading is banned in Singapore and in many other countries to prevent the exploitation of "poor and socially disadvantaged donors who are unable to make informed choices and suffer potential medical risks." Toni, 27, the other accused, donated a kidney to an Indonesian patient in March, alleging he was the patient's adopted son, and was paid 186 million rupiah (20,200 US). Upon sentence, both would suffer each, 12 months in jail or 10,000 Singapore dollars (7,600 US) fine.[59][60]
In an article appearing in the Econ Journal Watch, April 2004.[30] Economist Alex Tabarrok examined the impact of direct consent laws on transplant organ availability. Tabarrok found that social pressures resisting the use of transplant organs decreased over time as the opportunity of individual decisions increased. Tabarrok concluded his study suggesting that gradual elimination of organ donation restrictions and move to a free market in organ sales will increase supply of organs and encourage broader social acceptance of organ donation as a practice.
Ethical concerns
The existence and distribution of organ transplantation procedures in developing countries, while almost always beneficial to those receiving them, raise many ethical concerns. Both the source and method of obtaining the organ to transplant are major ethical issues to consider, as well as the notion of distributive justice. The World Health Organization argues that transplantations promote health, but the notion of “transplantation tourism” has the potential to violate human rights or exploit the poor, to have unintended health consequences, and to provide unequal access to services, all of which ultimately may cause harm. Regardless of the “gift of life”, in the context of developing countries, this might be coercive. The practice of coercion could be considered exploitative of the poor population, violating basic human rights according to Articles 3 and 4 of the Universal Declaration of Human Rights. There is also a powerful opposing view, that trade in organs, if properly and effectively regulated to ensure that the seller is fully informed of all the consequences of donation, is a mutually beneficial transaction between two consenting adults, and that prohibiting it would itself be a violation of Articles 3 and 29 of the Universal Declaration of Human Rights.
Even within developed countries there is concern that enthusiasm for increasing the supply of organs may trample on respect for the right to life. The question is made even more complicated by the fact that the "irreversibility" criterion for legal death cannot be adequately defined and can easily change with changing technology.[61]
Artificial organ transplantation
Surgeons in Sweden performed the first implantation of a synthetic trachea in July 2011, for a 36-year-old patient who was suffering from cancer. Stem cells taken from the patient's hip were treated with growth factors and incubated on a plastic replica of his natural trachea.[62]
References
- ^ See WHO Guiding Principles on human cell, tissue and organ transplantation, Annexed to World Health Organization, 2008.
- ^ Further sources in the Bibliography on Ethics of the WHO.
- ^ See Organ trafficking and transplantation pose new challenges.
- ^ Frohn C, Fricke L, Puchta JC, Kirchner H (February 2001). "The effect of HLA-C matching on acute renal transplant rejection". Nephrol. Dial. Transplant. 16 (2): 355–60. doi:10.1093/ndt/16.2.355. PMID 11158412. http://ndt.oxfordjournals.org/cgi/content/full/16/2/355.
- ^ New Drugs in Ttransplantation, EBMT Meeting, France, March 2007 C. Paillet, Pharmacist, Pharm D. C. Renzullo, Pharmacist, Pharm D. Edouard Herriot Hospital, Lyon, France
- ^ Restore Sight Organization website
- ^ The first transplantation of a human knee joint
- ^ Wake Forest Physician Reports First Human Recipients of Laboratory Grown Organs
- ^ Daily News – "Jaw-Droppin' Op a Success"
- ^ "Farmer has double arm transplant". BBC News. August 1, 2008. http://news.bbc.co.uk/2/hi/7537897.stm.
- ^ Woman to give birth after first ovary transplant pregnancy by James Randerson, science correspondent. guardian.co.uk, Sunday November 9, 2008 12.52 GMT.
- ^ Macchiarini P, Jungebluth P, Go T, et al. (December 2008). "Clinical transplantation of a tissue-engineered airway". Lancet 372 (9655): 2023–30. doi:10.1016/S0140-6736(08)61598-6. PMID 19022496.
- ^ "Full face transplant man reveals his new look on TV". BBC News. July 26, 2010. http://www.bbc.co.uk/news/health-10765005.
- ^ http://www.thinkspain.com/news-spain/18119/spains-first-double-leg-transplant-to-be-performed-in-valencia
- ^ Mayo Clinic Link
- ^ Seattle Times Article on domino transplants at Johns Hopkins
- ^ Good Morning America Video on four-way domino 47674874 transplant at Northwestern Memorial Hospital
- ^ Doctors plan first testicle transplant
- ^ Ross LF, Rubin DT, Siegler M, Josephson MA, Thistlethwaite JR, Woodle ES (June 1997). "Ethics of a paired-kidney-exchange program". N. Engl. J. Med. 336 (24): 1752–5. doi:10.1056/NEJM199706123362412. PMID 9180096. http://content.nejm.org/cgi/content/short/336/24/1752.
- ^ Rapaport FT (June 1986). "The case for a living emotionally related international kidney donor exchange registry". Transplant. Proc. 18 (3 Suppl 2): 5–9. PMID 3521001.
- ^ Horisberger B, Jeannet M, De Weck A, Frei PC, Grob P, Thiel G (October 1970). "A cooperative kidney typing and exchange program". Helv Med Acta 35 (4): 239–47. PMID 4918735.
- ^ Johns Hopkins Leads First 12-Patient, Multicenter “Domino Donor” Kidney Transplant, Johns Hopkins Medicine, February 16, 2009 – accessed July 14, 2009
- ^ Kidney donations connect strangers in Chain of Life forged by transplants, The Star-Ledger, June 05, 2009 – accessed July 11, 2009
- ^ First 16-patient, Multicenter 'Domino Donor' Kidney Transplant, Science Daily, July 11, 2009 – accessed July 14, 2009
- ^ Massive transplant effort pairs 13 kidneys to 13 patients, CNN.com, December 14, 2009 8:40 a.m. EST – Accessed December 145:10p PST
- ^ "Would you give your kidney to a stranger?". CNN.com. 2006-06-05. http://www.cnn.com/2006/HEALTH/06/01/living.donors/index.html. Retrieved 2008-05-02.
- ^ Budiani-Saberi, Da; Delmonico, Fl (May 2008). "Organ trafficking and transplant tourism: a commentary on the global realities.". American journal of transplantation 8 (5): 925–9. doi:10.1111/j.1600-6143.2008.02200.x. ISSN 1600–6135. PMID 18416734.
- ^ [1] Shopped Liver: The worldwide market in human organs, By William Saletan, Salon, April 14, 2007. Many links.
- ^ Appel JM, Fox MD (2005). "Organ solicitation on the Internet: every man for himself?". Hastings Cent Rep 35 (3): 14; discussion 14–5. doi:10.1353/hcr.2005.0052. PMID 16092393.
- ^ a b http://www.econjournalwatch.org/pdf/Tabarrok%20Comment%20April%202004.pdf
- ^ Ghods AJ, Savaj S (November 2006). "Iranian model of paid and regulated living-unrelated kidney donation". Clin J Am Soc Nephrol 1 (6): 1136–45. doi:10.2215/CJN.00700206. PMID 17699338.
- ^ Griffin A (March 2007). "Kidneys on demand". BMJ 334 (7592): 502–5. doi:10.1136/bmj.39141.493148.94. PMC 1819484. PMID 17347232. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1819484.
- ^ [2] WHO Says Organ Demand Outstrips Supply, Alexander G. Higgins, Associated Press, March 30, 2007
- ^ R. Bhagwan Singh (2007-01-16). "Indian police probe kidney sales by tsunami victims". Reuters. http://www.reuters.com/article/healthNews/idUSDEL21432720070116. Retrieved 2008-08-09.
- ^ Rothman DJ (October 2002). "Ethical and social consequences of selling a kidney". JAMA 288 (13): 1640–1. doi:10.1001/jama.288.13.1640. PMID 12350195. http://jama.ama-assn.org/cgi/pmidlookup?view=long&pmid=12350195.
- ^ The Pulitzer Center on Crisis Reporting http://pulitzercenter.org/blog/untold-stories/importing-egg-donors-ukraine-cyprus
- ^ Untold Stories: The Cyprus Scramble http://pulitzercenter.org/blog/untold-stories/cyprus-scramble-investigation-human-egg-markets
- ^ Human Eggs for Sale http://www.fastcompany.com/magazine/148/eggs-for-sale.html?partner=rss&utm_source=twitterfeed&utm_medium=twitter&utm_campaign=TheZargon
- ^ "Saved By His Daughter's Heart. Man Dying From Heart Disease Gets Gift From Late Daughter". CBS Broadcasting Inc. August 20, 2004. http://election.cbsnews.com/stories/2004/08/19/earlyshow/living/main637069.shtml. Retrieved October 10, 2006.
- ^ WMA – Policy : Council Resolution on Organ Donation in China
- ^ 世界日報──大陸新聞
- ^ Pact to block harvesting of inmate organs, Pg 1, South China Morning Post, October 7, 2007
- ^ Press release, Chinese Medical Association Reaches Agreement With World Medical Association Against Transplantation Of Prisoners's Organs, Medical News Today, Oct 07 2007
- ^ Council of EuropeDeceased Organ Donors, Annual Rate (p. m. p.) Europe Page 4
- ^ Organización Nacional de Transplantes, Donantes de órganos en España. Número total y tasa anual (p. m. p.)
- ^ Transplant Commission of the Council of Europe, La ONT estima en 94.500 los transplantes de órganos solidos realizados en 2006 en todo el mundo, 28 August 2007.
- ^ http://www.ramadhanfoundation.com/organ.htm
- ^ [3] "These institutes all call upon Muslims to donate organs for transplantation:the Shariah Academy of the Organisation of Islamic Conference (representing all Muslim countries), the Grand Ulema Council of Saudi Arabia, the Iranian Religious Authority, the Al-Azhar Academy of Egypt "
- ^ Huang J, Mao Y, Millis JM (December 2008). "Government policy and organ transplantation in China". Lancet 372 (9654): 1937–8. doi:10.1016/S0140-6736(08)61359-8. PMID 18930537. http://www.thelancetglobalhealthnetwork.com/wp-content/uploads/Health-System-Reform-in-China-CMT-11.pdf.
- ^ "Article by Dr. Tom Treasure in the Journal of the Royal Society of Medicine". www.dafoh.org. https://www.dafoh.org/Article_by_Dr.php. Retrieved May 21, 2010.
- ^ David N. Weisstub, Guillermo Díaz Pintos, Autonomy and Human Rights in Health Care: An International Perspective, page 238. Springer, 2007, ISBN 1402058403. 2007-12-21. ISBN 9781402058400. http://books.google.com/books?id=zIlDmNVlHlAC&pg=PA238&dq=chinese+%22life+after+death%22+%22integrity+of+the+body%22&cd=1#v=onepage&q=chinese%20%22life%20after%20death%22%20%22integrity%20of%20the%20body%22&f=false. Retrieved May 21, 2010.
- ^ "China fury at organ snatching 'lies'". BBC News. June 28, 2001. http://news.bbc.co.uk/1/hi/world/americas/1411389.stm. Retrieved May 21, 2010.
- ^ "Illegal Human Organ Trade from Executed Prisoners in China". www1.american.edu. http://www1.american.edu/ted/prisonorgans.htm. Retrieved June 9, 2010.
- ^ "The Bellagio Task Force Report on Transplantation, Bodily Integrity, and the International Traffic in Organs". www.icrc.org. http://www.icrc.org/Web/eng/siteeng0.nsf/iwpList302/87DC95FCA3C3D63EC1256B66005B3F6C. Retrieved June 14, 2010.
- ^ "An Independent Investigation into Allegations of Organ Harvesting of Falun Gong Practitioners in China". organharvestinvestigation.net. http://organharvestinvestigation.net/. Retrieved June 9, 2010.
- ^ Frequently Asked Questions about the Halachic Organ Donor (HOD) Society
- ^ Alexander GC, Sehgal AR (October 1998). "Barriers to cadaveric renal transplantation among blacks, women, and the poor". JAMA 280 (13): 1148–52. doi:10.1001/jama.280.13.1148. PMID 9777814. http://jama.ama-assn.org/cgi/pmidlookup?view=long&pmid=9777814.
- ^ "China issues new rules on organs". BBC. 2007-04-07. http://news.bbc.co.uk/2/hi/asia-pacific/6534363.stm. Retrieved 2007-04-07.
- ^ Abs-Cbn Interactive, Two Indonesians plead guilty in Singapore midorgan trading case
- ^ straitstimes.com, CK Tang boss quizzed by police
- ^ Whetstine L, Streat S, Darwin M, Crippen D. (2005). "Pro/con ethics debate: When is dead really dead?". Critical Care (London, England) 9 (6): 538–42. doi:10.1186/cc3894. PMC 1414041. PMID 16356234. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1414041.
- ^ "Cancer Patient Gets First Totally Artificial Windpipe". 2011-07-08. http://www.npr.org/templates/transcript/transcript.php?storyId=137701848. Retrieved 2011-08-07.
Sources and bibliography
- Budiani-Saberi, Debra A.; Delmonico, Francis L. (2008). "Organ Trafficking and Transplant Tourism: A Commentary on the Global Realities". American Journal of Transplantation 2008 (8): 925–929. doi:10.1111/j.1600-6143.2008.02200.x. PMID 18416734. http://www.cofs.org/COFS-Publications/Budiani_and_Delmonico-AJT_April_2008.pdf.
- Caplan, Arthur L.; Coelho, Daniel H. (eds.) (1998). The Ethics of Organ Transplants: The Current Debate. New York: Prometheus Books. ISBN 1573922242.
- Cooper, David K.C.; Lanza, Robert P. (2000). Xeno: The Promise of Transplanting Animal Organs into Humans. Oxford: Oxford University Press. pp. 304. ISBN 9780195128338. http://www.oup.com/us/catalog/general/subject/Medicine/Ethics/~~/dmlldz11c2EmY2k9OTc4MDE5NTEyODMzOA==.
- Danovitch, Gabriel M.; Delmonico, Francis L. (2008). "The prohibition of kidney sales and organ markets should remain". Current Opinion in Organ Transplantation (Renal transplantation: Edited by Robert A. Montgomery) 13 (4): 386–394. doi:10.1097/MOT.0b013e3283097476. http://journals.lww.com/co-transplantation/Abstract/2008/08000/The_prohibition_of_kidney_sales_and_organ_markets.11.aspx.
- Gruessner, Rainer; Benedetti, Enrico (2008). Living Donor Organ Transplantation. New York: McGraw-Hill Inc. pp. 791. ISBN 978-0-0714-5549-7. http://jama.ama-assn.org/cgi/content/full/300/13/1592.
- McLean, Shella A.M.; Williamson, Laura (2005). Xenotransplantation: Law and Ethics. Aldershot: Ashgate Publishing ltd. pp. 290. ISBN 0-7546-2379-3.
- Sayeed, Sadath A. (2009). "Teaching ethics and trading organs". Indian Journal of Medical Ethics 6 (1): 25–27. PMID 19241951. http://www.issuesinmedicalethics.org/171co25.
- Shimazono, Yosuke (2007). "The state of the international organ trade: a provisional picture based on integration of available information". Bulletin of the World Health Organization 85 (12): 901–980. PMC 2636295. PMID 18278256. http://www.who.int/bulletin/volumes/85/12/06-039370/en/.
- Trzepacz, Paula T.; DiMartini, Andrea F. (2000). The Transplant Patient: Biological, Psychiatric, and Ethical Issues in Organ Transplantation. Cambridge / New York: Cambridge University Press. pp. 311. ISBN 0521553547.
- World Health Organization (2008). Human organ and tissue transplantation. Geneva / New York: WHO. pp. 13. http://apps.who.int/gb/ebwha/pdf_files/A62/A62_15-en.pdf.
- collective (2008). "Organ trafficking and transplant tourism and commercialism: the Declaration of Istanbul". The Lancet 372 (9632): 5–6. doi:10.1016/S0140-6736(08)60967-8. PMID 18603141. http://www.mst.org.my/articles/Lancet%20Commentary%20on%20the%20Declarartion%20of%20Istanbul.pdf.
- Appel, Jacob M.; Fox, Mark D. (2005). "Organ Solicitation on the Internet: Every Man for Himself?". Hastings Center Report 35 (3): 14–15. doi:10.1353/hcr.2005.0052. PMID 16092393.
- Lock, Margaret M. (2002). Twice Dead: Organ Transplants and the Reinvention of Death. Berkeley: University of California Press. ISBN 0-520-22605-4.
- Morris PJ (December 2004). "Transplantation—a medical miracle of the 20th century". N. Engl. J. Med. 351 (26): 2678–80. doi:10.1056/NEJMp048256. PMID 15616201. http://content.nejm.org/cgi/pmidlookup?view=short&pmid=15616201&promo=ONFLNS19.
- Finn, Robert (2000). Organ Transplants: Making the Most of Your Gift of Life. Patient Center Guides. ISBN 1-56592-634-X.
- Hu W, Lu J, Zhang L, et al. (October 2006). "A preliminary report of penile transplantation". Eur. Urol. 50 (4): 851–3. doi:10.1016/j.eururo.2006.07.026. PMID 16930814. http://linkinghub.elsevier.com/retrieve/pii/S0302-2838(06)00867-0.
- Taylor, James S. (2005). Stakes and Kidneys: Why Markets in Human Body parts are Morally Imperative. Aldershot, Hants, England: Ashgate. ISBN 0-7546-4109-0.
- Köchler, Hans, ed. (2001). Transplantationsmedizin und personale Identität. Medizinische, ethische, rechtliche und theologische Aspekte der Organverpflanzung. (Transplantation Medicine and Personal Identity. Medical, Ethical, Legal and Theological Aspects of Organ Transplantation / German) Frankfurt a. M. etc.: Peter Lang. ISBN 3-631-38363-0
- Cherry, Mark J. (2005). Kidney For Sale By Owner: Human Organs, Transplantation, And The Market. Washington, D.C: Georgetown University Press. ISBN 1-58901-040-X.
Further reading
- Gerritsen, T. (1996). Harvest. New York: Pocket Books.
- Gutkind, L. (1990). Many Sleepless Nights: The World of Organ Transplantation. New York: W. W. Norton & Company, Inc.
- Picoult, J.. (2008). Change of Heart. New York: Simon & Schuster, Inc.
External links
- Organ Transplant survival rates from the Scientific Registry of Transplant Recipients
- Latest Development in Multiple Organ Transplant at Irish Medical News
- Could we clone our organs to be used in a transplant? at HowStuffWorks
- How does organ transplantation works? at HowStuffWorks
- Liver Transplant Procedure description – by Children's Hospital of Pittsburgh
- The Gift of a Lifetime – Online Educational Documentary
- Doctors Against Forced Organ Harvesting
- First synthetic organ transplant
Categories:- Immunology
- Surgery
- Organ transplants


Wikimedia Foundation. 2010.