- Intensive-care medicine
-
"Intensive Care" redirects here. For the album by pop singer Robbie Williams, see Intensive Care (album)."CICU" redirects here. For the radio station, see CICU-FM."High dependency unit" redirects here. For the New Zealand psychedelic rock band, see High Dependency Unit (band).
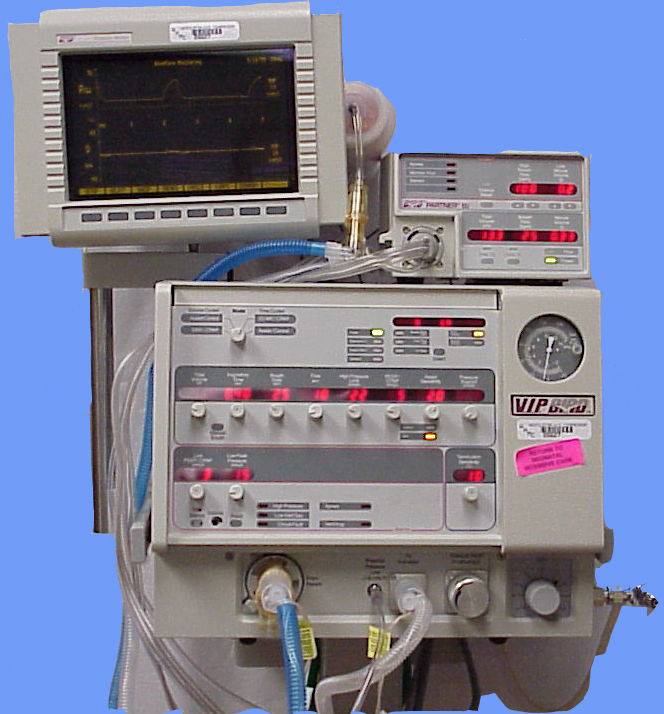
 Mechanical ventilation may be required if a patient's unassisted breathing is insufficient to oxygenate the blood.
Mechanical ventilation may be required if a patient's unassisted breathing is insufficient to oxygenate the blood.
Intensive-care medicine or critical-care medicine is a branch of medicine concerned with the diagnosis and management of life threatening conditions requiring sophisticated organ support and invasive monitoring.
Contents
Overview
Patients requiring intensive care may require support for hemodynamic instability (hypertension/hypotension), airway or respiratory compromise (such as ventilator support), acute renal failure, potentially lethal cardiac arrhythmias, or the cumulative effects of multiple organ failure, more commonly referred to now as multiple organ dysfunction syndrome. They may also be admitted for intensive/invasive monitoring, such as the crucial hours after major surgery when deemed too unstable to transfer to a less intensively monitored unit.
Intensive care is usually only offered to those whose condition is potentially reversible and who have a good chance of surviving with intensive care support. Since the critically ill are so close to dying, the outcome of this intervention is difficult to predict.[citation needed] A prime requisite for admission to an Intensive Care Unit is that the underlying condition can be overcome.
Medical studies suggest a relation between intensive care unit (ICU) volume and quality of care for mechanically ventilated patients.[1] After adjustment for severity of illness, demographic variables, and characteristics of the ICUs (including staffing by intensivists), higher ICU volume was significantly associated with lower ICU and hospital mortality rates. For example, adjusted ICU mortality (for a patient at average predicted risk for ICU death) was 21.2% in hospitals with 87 to 150 mechanically ventilated patients annually, and 14.5% in hospitals with 401 to 617 mechanically ventilated patients annually. Hospitals with intermediate numbers of patients had outcomes between these extremes.
In general, it is the most expensive, technologically advanced and resource-intensive area of medical care. In the United States, estimates of the 2000 expenditure for critical care medicine ranged from US$15–55 billion, accounting for about 0.5% of GDP and about 13% of national health care expenditure (Halpern, 2004).
Organ systems
Intensive care usually takes a system by system approach to treatment, rather than the SOAP (subjective, objective, analysis, plan) approach of high dependency care. The nine key systems (see below) are each considered on an observation-intervention-impression basis to produce a daily plan. As well as the key systems, intensive-care treatment raises other issues including psychological health, pressure points, mobilisation and physiotherapy, and secondary infections.
The nine key IC systems are (alphabetically): cardiovascular system, central nervous system, endocrine system, gastro-intestinal tract (and nutritional condition), hematology, microbiology (including sepsis status), peripheries (and skin), renal (and metabolic), respiratory system.
The provision of intensive care is, in general, administered in a specialized unit of a hospital called the intensive-care unit (ICU) or critical-care unit (CCU). Many hospitals also have designated intensive-care areas for certain specialities of medicine, such as the coronary intensive-care unit (CCU or sometimes CICU, depending on hospital) for heart disease, medical intensive-care unit (MICU), surgical intensive-care unit (SICU), pediatric intensive-care unit (PICU), neuroscience critical-care unit (NCCU), overnight intensive-recovery (OIR), shock/trauma intensive-care unit (STICU), neonatal intensive-care unit (NICU), and other units as dictated by the needs and available resources of each hospital. The naming is not rigidly standardized. For a time in the early 1960s, it was not clear that specialized intensive care units were needed, so intensive-care resources (see below) were brought to the room of the patient that needed the additional monitoring, care, and resources. It became rapidly evident, however, that a fixed location where intensive-care resources and personnel were available provided better care than ad hoc provision of intensive care services spread throughout a hospital.
Equipment and systems
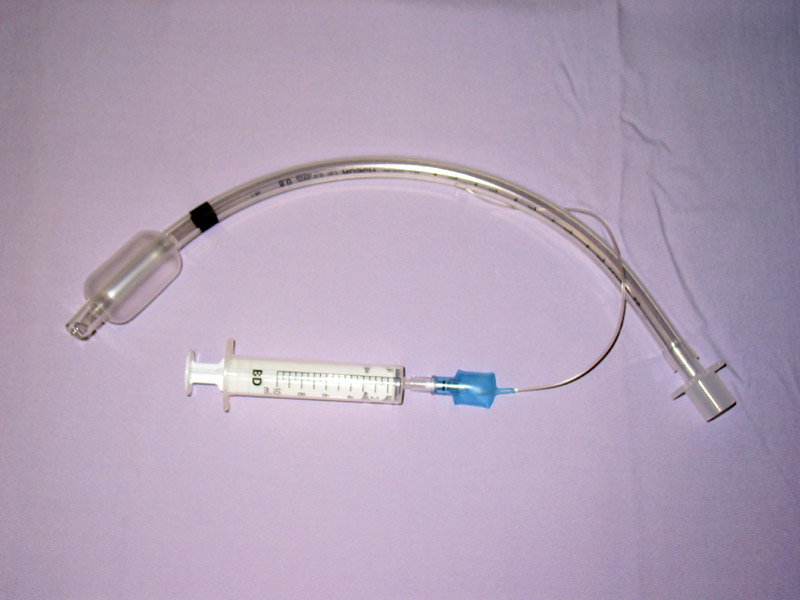
 An endotracheal tube
An endotracheal tubeCommon equipment in an intensive-care unit (ICU) includes mechanical ventilation to assist breathing through an endotracheal tube or a tracheotomy; hemofiltration equipment for acute renal failure; monitoring equipment; intravenous lines for drug infusions fluids or total parenteral nutrition, nasogastric tubes, suction pumps, drains and catheters; and a wide array of drugs including inotropes, sedatives, broad spectrum antibiotics and analgesics.
Medical specialties
Critical-care medicine is a relatively new but increasingly important medical specialty. Physicians with training in critical-care medicine are referred to as intensivists.[2] The specialty requires additional fellowship training for physicians having completed their primary residency training in internal medicine, anesthesiology, or surgery. Board certification in critical care medicine is available through all three specialty boards. Respiratory Therapists though already specialists in cardiopulmonary critical care have additional credentialing in Adult Critical Care (ACCS) and Neonatal and Pediatric (NPS) specialties. Nurse intensivists receive their training after basic education through ASTNA. Paramedics are certified to levels of CCEMTP or FP-C. Intensivists-physicians with a primary training in internal medicine sometimes pursue combined fellowship training in another subspecialty such as pulmonary medicine, cardiology, infectious disease, or nephrology. The Society of Critical Care Medicine is a well-established multiprofessional society for practitioners working in the ICU, including intensivists. Most medical research has demonstrated that ICU care provided by intensivists produces better outcomes and more cost-effective care.[3] This has led the Leapfrog Group to make a primary recommendation that all ICU patients be managed or co-managed by a dedicated intensivist who is exclusively responsible for patients in one ICU. However, there is a critical shortage of intensivists in the United States, and most hospitals lack this critical physician team member.
Patient management in intensive-care differs significantly between countries. In Australia, where Intensive Care Medicine is a well-established speciality, ICUs are described as 'closed'. In a closed unit the intensive-care specialist takes on the senior role where the patient's primary doctor now acts as a consultant. The advantage of this system is a more coordinated management of the patient based on a team who work exclusively in ICU. Other countries have open Intensive Care Units, where the primary doctor chooses to admit and, in general, makes the management decisions. There is increasingly strong evidence that 'closed' Intensive-Care Units staffed by Intensivists provide better outcomes for patients.[4][5]
History
Florence Nightingale era
 Florence Nightingale
Florence NightingaleThe ICU's roots can be traced back to the Monitoring Unit of critical patients through nurse Florence Nightingale. The Crimean War began in 1853 when Britain, France, and Turkey declared war on Russia. Because of the lack of critical care and the high rate of infection, there was a high mortality rate of hospitalised soldiers, reaching as high as 40% of the deaths recorded during the war. Nightingale and 38 other volunteers had to leave for the Fields of Scurati, and took their "critical care protocol" with them. Upon arriving, and practicing, the mortality rate fell to 2%. Nightingale contracted typhoid, and returned in 1856 from the war. A school of nursing dedicated to her was formed in 1859 in England. The school was recognised for its professional value and technical calibre, receiving prizes throughout the British government. The school of nursing was established in Saint Thomas Hospital, as a one-year course, and was given to doctors. It used theoretical and practical lessons, as opposed to purely academic lessons. Nightingale's work, and the school, paved the way for intensive care medicine.
Dandy era
Walter Edward Dandy was born in Sedalia, Missouri. He received his BA in 1907 through the University of Missouri and his M.D. in 1910 through the Johns Hopkins University School of Medicine. Dandy worked one year with Dr. Harvey Cushing in the Hunterian Laboratory of Johns Hopkins before entering its boarding school and residence in the Johns Hopkins Hospital. He worked in the Johns Hopkins College in 1914 and remained there until his death in 1946. One of the most important contributions he made for neurosurgery was the air method in ventriculography, in which the cerebrospinal fluid is substituted with air to help an image form on an X-Ray of the ventricular space in the brain. This technique was extremely successful for identifying brain injuries. Dr. Dandy was also a pioneer in the advances in operations for illnesses of the brain affecting the glossopharyngeal as well as Ménière's syndrome, and he published studies that show that high activity can cause sciatic pain. Dandy created the first ICU in the world, 03 beds in Boston in 1926.
Ibsen era
Bjørn Aage Ibsen (1915–2007) graduated in 1940 from medical school at the University of Copenhagen and trained in anesthesiology from 1949 to 1950 at the Massachusetts General Hospital, Boston. He became involved in the 1952 poliomyelitis outbreak in Denmark[6], where 2722 patients developed the illness in a 6 month period, with 316 suffering respiratory or airway paralysis. Treatment had involved the use of the few negative pressure respirators available, but these devices, while helpful, were limited and did not protect against aspiration of secretions. Ibsen changed management directly, instituting protracted positive pressure ventilation by means of intubation into the trachea, and enlisting 200 medical students to manually pump oxygen and air into the patients lungs[7]. At this time Carl-Gunnar Engström had developed one of the first positive pressure volume controlled ventilators, which eventually replaced the medical students. In this fashion, mortality declined from 90% to around 25%. Patients were managed in 3 special 35 bed areas, which aided charting and other management. In 1953, Ibsen set up what became the world's first Medical/Surgical ICU in a converted student nurse classroom in Kommunehospitalet (The Municipal Hospital) in Copenhagen[8], and provided one of the first accounts of the management of tetanus with muscle relaxants and controlled ventilation. In 1954 Ibsen was elected Head of the Department of Anaesthesiology at that institution. He jointly authored the first known account of ICU management principles in Nordisk Medicin, September 18, 1958: ‘Arbejdet på en Anæsthesiologisk Observationsafdeling’ (‘The Work in an Anaesthesiologic Observation Unit’) with Tone Dahl Kvittingen from Norway. He died in 2007.
Safar era
Peter Safar, the first Intensivist doctor in the USA,[citation needed] was born in Austria as the son of two doctors. He first migrated to the United States in 1949. Safar first got certification as an anesthesiologist, and, in the 1950s, he started and praised the "Urgency & Emergency" room setup (now known as an ICU)[citation needed]. It was at this time the ABC (Airway, Breathing, and Circulation) protocols were formed, and artificial ventilation as well as cardiopulmonary resuscitation became popular.[citation needed] These experiments counted on volunteers of its team, and used only minimal sedation. It was through these experiments that the techniques for maintaining life in the critical patient were established.[citation needed]
The first surgical ICU was established in Baltimore, and, in 1962, in the University of Pittsburgh, the first Critical Care Residency was established in the United States. It was around this time that the induction of hypothermia in critical patients was also tested.[citation needed]
In 1970, the Society of Critical Care Medicine was formed.[9]
See also
- Neonatal Intensive Care Unit
- Intensive Care Unit
- Respiratory monitoring
Notes
- ^ Kahn JM, Goss CH, Heagerty PJ, Kramer AA, O'Brien CR, Rubenfeld GD., JM; Goss, CH; Heagerty, PJ; Kramer, AA; O'Brien, CR; Rubenfeld, GD (2006). "Hospital volume and the outcomes of mechanical ventilation". New England Journal of Medicine 355 (1): 41–50. doi:10.1056/NEJMsa053993. PMID 16822995.
- ^ http://www.hfma.org/forums/What_Intensivist.htm
- ^ Association between Critical Care Physician Management and Patient Mortality in the Intensive Care Unit. Annals of Internal Medicine; 3 June 2008 | Volume 148 Issue 11 | Pages 801-809
- ^ Manthous CA, Amoateng-Adjepong Y, al-Kharrat T, Jacob B, Alnuaimat HM, Chatila W, Hall JB., CA; Amoateng-Adjepong, Y; Al-Kharrat, T; Jacob, B; Alnuaimat, HM; Chatila, W; Hall, JB (1997). "Effects of a medical intensivist on patient care in a community teaching hospital" (Abstract). Mayo Clinic Proceedings 72 (5): 391–9. doi:10.4065/72.5.391. PMID 9146680.
- ^ Hanson CW 3rd, Deutschman CS, Anderson HL 3rd, Reilly PM, Behringer EC, Schwab CW, Price J., 3rd; Deutschman, CS; Anderson Hl, 3rd; Reilly, PM; Behringer, EC; Schwab, CW; Price, J (1999). "Effects of an organized critical care service on outcomes and resource utilization: a cohort study" (Abstract). Critical Care Medicine 27 (2): 270–4. doi:10.1097/00003246-199902000-00030. PMID 10075049.
- ^ "The Danish anaesthesiologist Björn Ibsen a pioneer of long-term ventilation on the upper airways, Louise Reisner-Sénélar, 2009". https://dl-web.dropbox.com/get/Public/The%20Danish%20anaesthesiologist%20Bj%C3%B6rn%20Ibsen%2C%20Louise%20Reisner-S%C3%A9n%C3%A9lar%2C%202009.pdf?w=a25aff0a.
- ^ Louise Reisner-Sénélar (2011) The birth of intensive care medicine: Björn Ibsen’s records, Intensive Care Medicine
- ^ "The Danish anaesthesiologist Björn Ibsen a pioneer of long-term ventilation on the upper airways, Louise Reisner-Sénélar, 2009". https://dl-web.dropbox.com/get/Public/The%20Danish%20anaesthesiologist%20Bj%C3%B6rn%20Ibsen%2C%20Louise%20Reisner-S%C3%A9n%C3%A9lar%2C%202009.pdf?w=a25aff0a.
- ^ history reference: Brazilian Society of Critical Care SOBRATI Video:ICU History Historical photos
References
- Intensive Care Medicine by Irwin and Rippe
- Civetta, Taylor, and Kirby's Critical Care
- The ICU Book by Marino
- Procedures and Techniques in Intensive Care Medicine by Irwin and Rippe
- Halpern NA, Pastores SM, Greenstein RJ (June 2004). "Critical care medicine in the United States 1985-2000: an analysis of bed numbers, use, and costs.". Critical care medicine 32 (6): 1254–9. doi:10.1097/01.CCM.0000128577.31689.4C. PMID 15187502..
- History Reference:
- Brazilian Society of Intensive Care - SOBRATI
- History
- Society of Critical Care Medicine
External links
- Society of Critical Care Medicine
- Veterinary Emergency And Critical Care Society
- ESICM : European Society of Intensive Care Medicine
- ICUsteps - Intensive care patient support charity
- CCN - A peer-to-peer forum for intensive care clinicians
- - UK Intensive Care Society
- Scottish Intensive Care Society
- Critical Care Mailing List [CCM-L [1]]
- The Danish anaesthesiologist Björn Ibsen a pioneer of long-term ventilation on the upper airways, Louise Reisner-Sénélar, 2009
Medical Specialities Specialties
and
subspecialtiesCardiac surgery · Cardiothoracic surgery · Colorectal surgery · General surgery · Neurosurgery · Ophthalmology · Oral and maxillofacial surgery · Orthopedic surgery · Hand surgery · Otolaryngology (ENT) · Pediatric surgery · Plastic surgery · Surgical oncology · Thoracic surgery · Transplant surgery · Trauma surgery · Urology · Vascular surgery
Allergy/Immunology · Andrology · Angiology (Vascular Medicine) · Cardiology · Endocrinology · Gastroenterology (Hepatology) · Geriatrics · Gynaecology · Hematology · Infectious disease · Nephrology · Oncology · Pulmonology · Rheumatology
DiagnosticHealthcare sciences (Clinical chemistry, Clinical immunology, Cytopathology, Medical microbiology, Transfusion medicine) · Radiology (Interventional radiology, Nuclear medicine) · Pathology (Anatomical, Clinical) · Clinical neurophysiology
Other specialtiesAddiction medicine · Adolescent medicine · Anesthesiology · Dermatology · Disaster medicine · Emergency medicine · Family medicine · General practice · Hospital medicine · Intensive-care medicine · Medical genetics · Neurology · Obstetrics · Occupational medicine · Pain management (Algiatry) · Palliative care · Pediatrics (Neonatology) · Physical medicine and rehabilitation (Physiatry) · Preventive medicine · Psychiatry · Radiation oncology · Reproductive medicine (Reproductive endocrinology and infertility, Reproductive surgery) · Sexual medicine · Sleep medicine · Sports medicine · Transplantation medicine · Tropical medicine (Travel medicine) · Urogynecology
Others Categories:

Wikimedia Foundation. 2010.