- Sleep
-
"Waking up" redirects here. For other uses, see Waking Up (disambiguation).This article is about sleep in general; for specifically non-human sleep see Sleep (non-human); for other uses, see Sleep (disambiguation).
 Sleeping child
Sleeping child
Sleep is a naturally recurring state characterized by reduced or absent consciousness, relatively suspended sensory activity, and inactivity of nearly all voluntary muscles.[1] It is distinguished from quiet wakefulness by a decreased ability to react to stimuli, and is more easily reversible than being in hibernation or a coma. Sleep is also a heightened anabolic state, accentuating the growth and rejuvenation of the immune, nervous, skeletal and muscular systems. It is observed in all mammals, all birds, and many reptiles, amphibians, and fish.
The purposes and mechanisms of sleep are only partially clear and are the subject of intense research.[2] Sleep is often thought to help conserve energy,[3][4] but actually decreases metabolism only about 5–10%.[3][4] Hibernating animals need to sleep despite the hypometabolism seen in hibernation, and in fact they must return from hypothermia to euthermy in order to sleep, making sleeping "energetically expensive."[5]
Contents
Physiology
Sleep stages
In mammals and birds, sleep is divided into two broad types: rapid eye movement (REM) and non-rapid eye movement (NREM or non-REM) sleep. Each type has a distinct set of associated physiological, neurological, and psychological features. The American Academy of Sleep Medicine (AASM) further divides NREM into three stages: N1, N2, and N3, the last of which is also called delta sleep or slow-wave sleep (SWS).[6]
 Hypnogram showing sleep cycles from midnight to 6.30 am, with deep sleep early on. There is more REM (marked red) before waking.
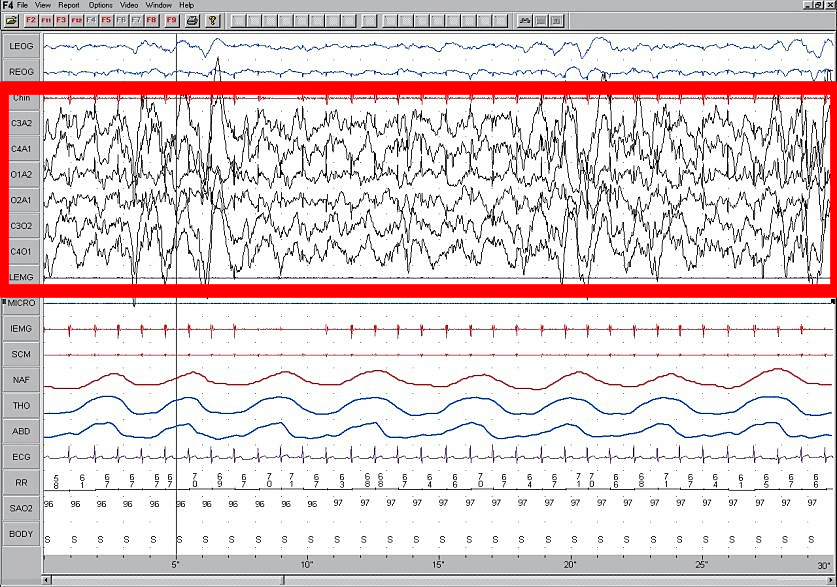
Hypnogram showing sleep cycles from midnight to 6.30 am, with deep sleep early on. There is more REM (marked red) before waking. Stage N3 sleep; EEG highlighted by red box. Thirty seconds of deep sleep, here with greater than 50% delta waves.
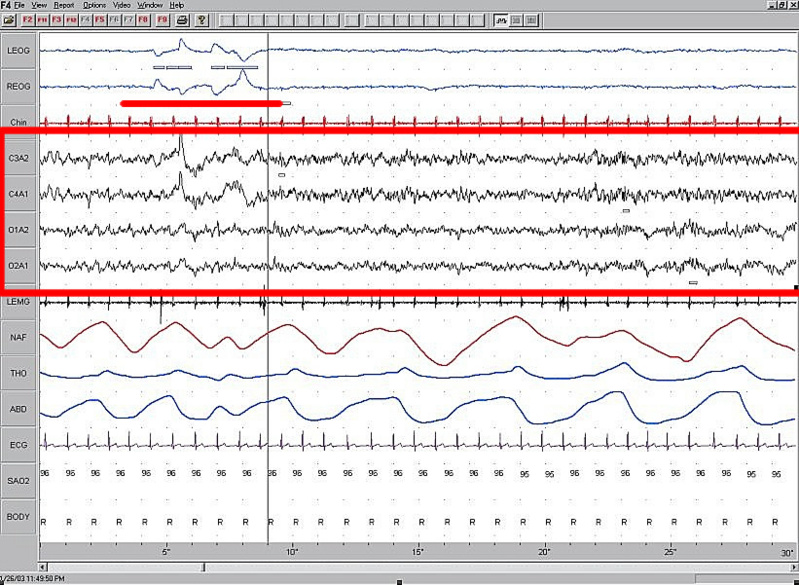
Stage N3 sleep; EEG highlighted by red box. Thirty seconds of deep sleep, here with greater than 50% delta waves. REM sleep; EEG highlighted by red box; eye movements highlighted by red line. Thirty seconds of sleep.
REM sleep; EEG highlighted by red box; eye movements highlighted by red line. Thirty seconds of sleep.Sleep proceeds in cycles of REM and NREM, the order normally being N1 → N2 → N3 → N2 → REM. There is a greater amount of deep sleep (stage N3) earlier in the sleep cycle, while the proportion of REM sleep increases later in the sleep cycle and just before natural awakening.
The stages of sleep were first described in 1937 by Alfred Lee Loomis and his coworkers, who separated the different electroencephalography (EEG) features of sleep into five levels (A to E), which represented the spectrum from wakefulness to deep sleep.[7] In 1953, REM sleep was discovered as distinct, and thus William Dement and Nathaniel Kleitman reclassified sleep into four NREM stages and REM.[8] The staging criteria were standardized in 1968 by Allan Rechtschaffen and Anthony Kales in the "R&K sleep scoring manual."[9] In the R&K standard, NREM sleep was divided into four stages, with slow-wave sleep comprising stages 3 and 4. In stage 3, delta waves made up less than 50% of the total wave patterns, while they made up more than 50% in stage 4. Furthermore, REM sleep was sometimes referred to as stage 5.
In 2004, the AASM commissioned the AASM Visual Scoring Task Force to review the R&K scoring system. The review resulted in several changes, the most significant being the combination of stages 3 and 4 into Stage N3. The revised scoring was published in 2007 as The AASM Manual for the Scoring of Sleep and Associated Events.[10] Arousals and respiratory, cardiac, and movement events were also added.[11][12]
Sleep stages and other characteristics of sleep are commonly assessed by polysomnography in a specialized sleep laboratory. Measurements taken include EEG of brain waves, electrooculography (EOG) of eye movements, and electromyography (EMG) of skeletal muscle activity. In humans, each sleep cycle lasts from 90 to 110 minutes on average,[13] and each stage may have a distinct physiological function. This can result in sleep that exhibits loss of consciousness but does not fulfill its physiological functions (i.e., one may still feel tired after apparently sufficient sleep).
Scientific studies on sleep have shown that sleep stage at awakening is an important factor in amplifying sleep inertia. Alarm clocks involving sleep stage monitoring appeared on the market in 2005.[14] Using sensing technologies such as EEG electrodes or accelerometers, these alarm clocks are supposed to wake people only from light sleep.
NREM sleep
Main article: Non-rapid eye movement sleepAccording to the 2007 AASM standards, NREM consists of three stages. There is relatively little dreaming in NREM.
Stage N1 refers to the transition of the brain from alpha waves having a frequency of 8–13 Hz (common in the awake state) to theta waves having a frequency of 4–7 Hz. This stage is sometimes referred to as somnolence or drowsy sleep. Sudden twitches and hypnic jerks, also known as positive myoclonus, may be associated with the onset of sleep during N1. Some people may also experience hypnagogic hallucinations during this stage. During N1, the subject loses some muscle tone and most conscious awareness of the external environment. To put it in simpler form, you are in a very shallow sleep, can jerk awake easily, are slightly aware of your surroundings, aren't dreaming, and have no rapid eye movement.
Stage N2 is characterized by sleep spindles ranging from 11 to 16 Hz (most commonly 12–14 Hz) and K-complexes. During this stage, muscular activity as measured by EMG decreases, and conscious awareness of the external environment disappears. This stage occupies 45–55% of total sleep in adults.
Stage N3 (deep or slow-wave sleep) is characterized by the presence of a minimum of 20% delta waves ranging from 0.5–2 Hz and having a peak-to-peak amplitude >75 μV. (EEG standards define delta waves to be from 0 to 4 Hz, but sleep standards in both the original R&K, as well as the new 2007 AASM guidelines have a range of 0.5–2 Hz.) This is the stage in which parasomnias such as night terrors, nocturnal enuresis, sleepwalking, and somniloquy occur. Many illustrations and descriptions still show a stage N3 with 20–50% delta waves and a stage N4 with greater than 50% delta waves; these have been combined as stage N3.
REM sleep
Main article: Rapid eye movement sleepRapid eye movement sleep, or REM sleep, accounts for 20–25% of total sleep time in most human adults. The criteria for REM sleep include rapid eye movements as well as a rapid low-voltage EEG. Most memorable dreaming occurs in this stage. At least in mammals, a descending muscular atonia is seen. Such paralysis may be necessary to protect organisms from self-damage through physically acting out scenes from the often-vivid dreams that occur during this stage.
Timing
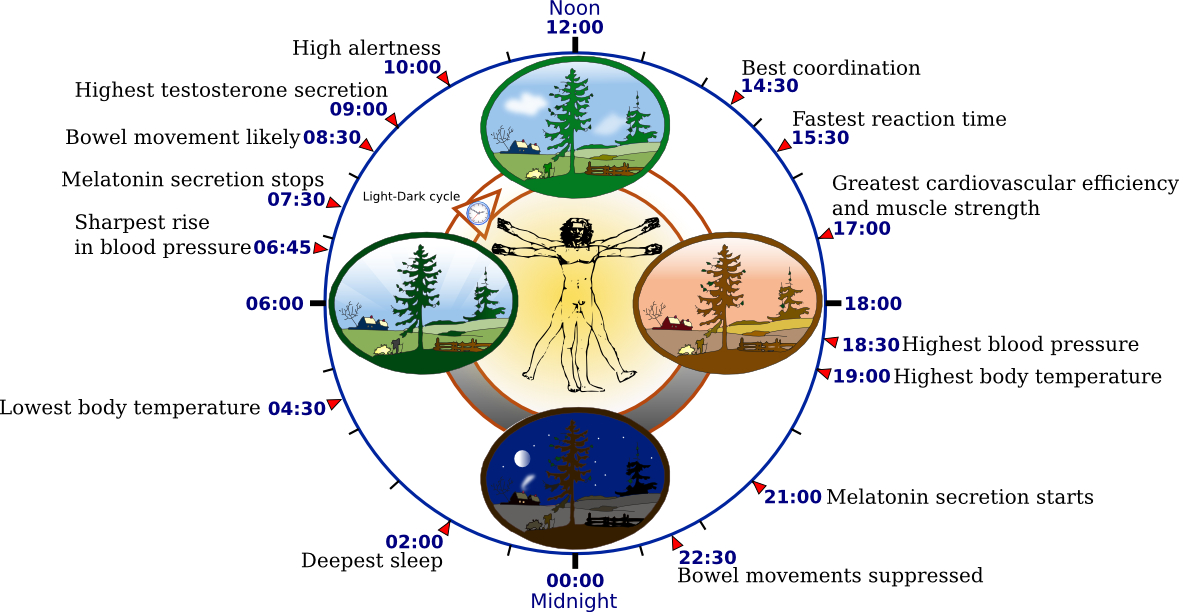
 The human biological clock
The human biological clockSleep timing is controlled by the circadian clock, sleep-wake homeostasis, and in humans, within certain bounds, willed behavior. The circadian clock—an inner timekeeping, temperature-fluctuating, enzyme-controlling device—works in tandem with adenosine, a neurotransmitter that inhibits many of the bodily processes associated with wakefulness. Adenosine is created over the course of the day; high levels of adenosine lead to sleepiness. In diurnal animals, sleepiness occurs as the circadian element causes the release of the hormone melatonin and a gradual decrease in core body temperature. The timing is affected by one's chronotype. It is the circadian rhythm that determines the ideal timing of a correctly structured and restorative sleep episode.[15]
Homeostatic sleep propensity (the need for sleep as a function of the amount of time elapsed since the last adequate sleep episode) must be balanced against the circadian element for satisfactory sleep.[16] Along with corresponding messages from the circadian clock, this tells the body it needs to sleep.[17] Sleep offset (awakening) is primarily determined by circadian rhythm. A person who regularly awakens at an early hour will generally not be able to sleep much later than his or her normal waking time, even if moderately sleep-deprived.
Sleep duration is affected by the gene DEC2. Some people have a mutation of this gene; they sleep two hours less than normal. Neurology professor Ying-Hui Fu and her colleagues bred mice that carried the DEC2 mutation and slept less than normal mice.[18][19]
Optimal amount in humans
Adult
The optimal amount of sleep is not a meaningful concept unless the timing of that sleep is seen in relation to an individual's circadian rhythms. A person's major sleep episode is relatively inefficient and inadequate when it occurs at the "wrong" time of day; one should be asleep at least six hours before the lowest body temperature.[20] The timing is correct when the following two circadian markers occur after the middle of the sleep episode and before awakening:[21]
- maximum concentration of the hormone melatonin, and
- minimum core body temperature.
For more information on the human circadian rhythm and body temperature, see Biological markers (in the article Circadian rhythm).
Human sleep needs can vary by age and among individuals, and sleep is considered to be adequate when there is no daytime sleepiness or dysfunction. Moreover, self-reported sleep duration is only moderately correlated with actual sleep time as measured by actigraphy,[22] and those affected with sleep state misperception may typically report having slept only four hours despite having slept a full eight hours.[23]
A University of California, San Diego psychiatry study of more than one million adults found that people who live the longest self-report sleeping for six to seven hours each night.[24] Another study of sleep duration and mortality risk in women showed similar results.[25] Other studies show that "sleeping more than 7 to 8 hours per day has been consistently associated with increased mortality," though this study suggests the cause is probably other factors such as depression and socioeconomic status, which would correlate statistically.[26] It has been suggested that the correlation between lower sleep hours and reduced morbidity only occurs with those who wake after less sleep naturally, rather than those who use an alarm.
Researchers at the University of Warwick and University College London have found that lack of sleep can more than double the risk of death from cardiovascular disease, but that too much sleep can also be associated with a doubling of the risk of death, though not primarily from cardiovascular disease.[28][29] Professor Francesco Cappuccio said, "Short sleep has been shown to be a risk factor for weight gain, hypertension, and Type 2 diabetes, sometimes leading to mortality; but in contrast to the short sleep-mortality association, it appears that no potential mechanisms by which long sleep could be associated with increased mortality have yet been investigated. Some candidate causes for this include depression, low socioeconomic status, and cancer-related fatigue... In terms of prevention, our findings indicate that consistently sleeping around seven hours per night is optimal for health, and a sustained reduction may predispose to ill health."
Furthermore, sleep difficulties are closely associated with psychiatric disorders such as depression, alcoholism, and bipolar disorder.[30] Up to 90% of adults with depression are found to have sleep difficulties. Dysregulation found on EEG includes disturbances in sleep continuity, decreased delta sleep and altered REM patterns with regard to latency, distribution across the night and density of eye movements.[31]
Hours by age
Children need more sleep per day in order to develop and function properly: up to 18 hours for newborn babies, with a declining rate as a child ages.[17] A newborn baby spends almost 9 hours a day in REM sleep. By the age of five or so, only slightly over two hours is spent in REM. Studies say that school age children need about 10 to 11 hours of sleep.[32]
Age and condition Average amount of sleep per day Newborn up to 18 hours 1–12 months 14–18 hours 1–3 years 12–15 hours 3–5 years 11–13 hours 5–12 years 9–11 hours Adolescents 9–10 hours[33] Adults, including elderly 7–8 hours Pregnant women 8(+) hours Sleep debt
Main article: Sleep debtSleep debt is the effect of not getting enough rest and sleep; a large debt causes mental, emotional and physical fatigue.
Sleep debt results in diminished abilities to perform high-level cognitive functions. Neurophysiological and functional imaging studies have demonstrated that frontal regions of the brain are particularly responsive to homeostatic sleep pressure.[34]
Scientists do not agree on how much sleep debt it is possible to accumulate; whether it is accumulated against an individual's average sleep or some other benchmark; nor on whether the prevalence of sleep debt among adults has changed appreciably in the industrialized world in recent decades. It is likely that children are sleeping less than previously in Western societies.[35]
Genetics
It is suspected that a considerable amount of sleep-related behavior, such as when and how long a person needs to sleep, is regulated by our genetics. Researchers have discovered some evidence that seems to support this assumption.[36]
Functions
 A Kutchi woman sleeping
A Kutchi woman sleepingThe multiple theories proposed to explain the function of sleep reflect the as-yet incomplete understanding of the subject. (When asked, after 50 years of research, what he knew about the reason people sleep William Dement, founder of Stanford University's Sleep Research Center, answered, "As far as I know, the only reason we need to sleep that is really, really solid is because we get sleepy."[37]) It is likely that sleep evolved to fulfill some primeval function and took on multiple functions over time (analogous to the larynx, which controls the passage of food and air, but descended over time to develop speech cabilities).
If sleep were not essential, one would expect to find:
- Animal species that do not sleep at all
- Animals that do not need recovery sleep when they stay awake longer than usual
- Animals that suffer no serious consequences as a result of lack of sleep
Outside of a few basal animals that have no brain or a very simple one, no animals have been found to date that satisfy any of these criteria.[38] While some varieties of shark, such as great whites and hammerheads, must remain in motion at all times to move oxygenated water over their gills, it is possible they still sleep one cerebral hemisphere at a time as marine mammals do. However it remains to be shown definitively whether any fish is capable of unihemispheric sleep.
Some of the many proposed functions of sleep are as follows:
Restoration
Wound healing has been shown to be affected by sleep. A study conducted by Gumustekin et al.[39] in 2004 shows sleep deprivation hindering the healing of burns on rats.
It has been shown that sleep deprivation affects the immune system. In a study by Zager et al. in 2007,[40] rats were deprived of sleep for 24 hours. When compared with a control group, the sleep-deprived rats' blood tests indicated a 20% decrease in white blood cell count, a significant change in the immune system. It is now possible to state that "sleep loss impairs immune function and immune challenge alters sleep," and it has been suggested that mammalian species which invest in longer sleep times are investing in the immune system, as species with the longer sleep times have higher white blood cell counts.[41]
It has yet to be proven that sleep duration affects somatic growth. One study by Jenni et al.[42] in 2007 recorded growth, height, and weight, as correlated to parent-reported time in bed in 305 children over a period of nine years (age 1–10). It was found that "the variation of sleep duration among children does not seem to have an effect on growth." It has been shown that sleep—more specifically, slow-wave sleep (SWS)—does affect growth hormone levels in adult men. During eight hours' sleep, Van Cauter, Leproult, and Plat[43] found that the men with a high percentage of SWS (average 24%) also had high growth hormone secretion, while subjects with a low percentage of SWS (average 9%) had low growth hormone secretion.
There are multiple arguments supporting the restorative function of sleep. The metabolic phase during sleep is anabolic; anabolic hormones such as growth hormones (as mentioned above) are secreted preferentially during sleep. The duration of sleep among species is, in general, inversely related to animal size[citation needed] and directly related to basal metabolic rate. Rats with a very high basal metabolic rate sleep for up to 14 hours a day, whereas elephants and giraffes with lower BMRs sleep only 3–4 hours per day.
Energy conservation could as well have been accomplished by resting quiescent without shutting off the organism from the environment, potentially a dangerous situation. A sedentary nonsleeping animal is more likely to survive predators, while still preserving energy. Sleep, therefore, seems to serve another purpose, or other purposes, than simply conserving energy; for example, hibernating animals waking up from hibernation go into rebound sleep because of lack of sleep during the hibernation period. They are definitely well-rested and are conserving energy during hibernation, but need sleep for something else.[5] Rats kept awake indefinitely develop skin lesions, hyperphagia, loss of body mass, hypothermia, and, eventually, fatal sepsis.[44]
Ontogenesis
According to the ontogenetic hypothesis of REM sleep, the activity occurring during neonatal REM sleep (or active sleep) seems to be particularly important to the developing organism (Marks et al., 1995). Studies investigating the effects of deprivation of active sleep have shown that deprivation early in life can result in behavioral problems, permanent sleep disruption, decreased brain mass (Mirmiran et al., 1983), and an abnormal amount of neuronal cell death (Morrissey, Duntley & Anch, 2004).
REM sleep appears to be important for development of the brain. REM sleep occupies the majority of time of sleep of infants, who spend most of their time sleeping. Among different species, the more immature the baby is born, the more time it spends in REM sleep. Proponents also suggest that REM-induced muscle inhibition in the presence of brain activation exists to allow for brain development by activating the synapses, yet without any motor consequences that may get the infant in trouble. Additionally, REM deprivation results in developmental abnormalities later in life.
However, this does not explain why older adults still need REM sleep. Aquatic mammal infants do not have REM sleep in infancy;[45] REM sleep in those animals increases as they age.
Memory processing
Further information: Sleep and learning, Sleep and creativity, and Sleep and MemoryScientists have shown numerous ways in which sleep is related to memory. In a study conducted by Turner, Drummond, Salamat, and Brown,[46] working memory was shown to be affected by sleep deprivation. Working memory is important because it keeps information active for further processing and supports higher-level cognitive functions such as decision making, reasoning, and episodic memory. The study allowed 18 women and 22 men to sleep only 26 minutes per night over a four-day period. Subjects were given initial cognitive tests while well-rested, and then were tested again twice a day during the four days of sleep deprivation. On the final test, the average working memory span of the sleep-deprived group had dropped by 38% in comparison to the control group.
Memory seems to be affected differently by certain stages of sleep such as REM and slow-wave sleep (SWS). In one study, cited in Born, Rasch, and Gais,[47] multiple groups of human subjects were used: wake control groups and sleep test groups. Sleep and wake groups were taught a task and were then tested on it, both on early and late nights, with the order of nights balanced across participants. When the subjects' brains were scanned during sleep, hypnograms revealed that SWS was the dominant sleep stage during the early night, representing around 23% on average for sleep stage activity. The early-night test group performed 16% better on the declarative memory test than the control group. During late-night sleep, REM became the most active sleep stage at about 24%, and the late-night test group performed 25% better on the procedural memory test than the control group. This indicates that procedural memory benefits from late, REM-rich sleep, whereas declarative memory benefits from early, SWS-rich sleep.
A study conducted by Datta[48] indirectly supports these results. The subjects chosen were 22 male rats. A box was constructed wherein a single rat could move freely from one end to the other. The bottom of the box was made of a steel grate. A light would shine in the box accompanied by a sound. After a five-second delay, an electrical shock would be applied. Once the shock commenced, the rat could move to the other end of the box, ending the shock immediately. The rat could also use the five-second delay to move to the other end of the box and avoid the shock entirely. The length of the shock never exceeded five seconds. This was repeated 30 times for half the rats. The other half, the control group, was placed in the same trial, but the rats were shocked regardless of their reaction. After each of the training sessions, the rat would be placed in a recording cage for six hours of polygraphic recordings. This process was repeated for three consecutive days. This study found that during the posttrial sleep recording session, rats spent 25.47% more time in REM sleep after learning trials than after control trials. These trials support the results of the Born et al. study, indicating an obvious correlation between REM sleep and procedural knowledge.
An observation of the Datta study is that the learning group spent 180% more time in SWS than did the control group during the post-trial sleep-recording session. This phenomenon is supported by a study performed by Kudrimoti, Barnes, and McNaughton.[49] This study shows that after spatial exploration activity, patterns of hippocampal place cells are reactivated during SWS following the experiment. In a study by Kudrimoti et al., seven rats were run through a linear track using rewards on either end. The rats would then be placed in the track for 30 minutes to allow them to adjust (PRE), then they ran the track with reward-based training for 30 minutes (RUN), and then they were allowed to rest for 30 minutes. During each of these three periods, EEG data were collected for information on the rats' sleep stages. Kudrimoti et al. computed the mean firing rates of hippocampal place cells during prebehavior SWS (PRE) and three ten-minute intervals in postbehavior SWS (POST) by averaging across 22 track-running sessions from seven rats. The results showed that ten minutes after the trial RUN session, there was a 12% increase in the mean firing rate of hippocampal place cells from the PRE level; however, after 20 minutes, the mean firing rate returned rapidly toward the PRE level. The elevated firing of hippocampal place cells during SWS after spatial exploration could explain why there were elevated levels of SWS sleep in Datta's study, as it also dealt with a form of spatial exploration.
A study has also been done involving direct current stimulation to the prefrontal cortex to increase the amount of slow oscillations during SWSfe(Marshall et al., 2006, as cited in Walker, 2009). The direct current stimulation greatly enhanced word-pair retention the following day, giving evidence that SWS plays a large role in the consolidation of episodic memories.[50]
The different studies all suggest that there is a correlation between sleep and the complex functions of memory. Harvard sleep researchers Saper and Stickgold[51] point out that an essential part of memory and learning consists of nerve cell dendrites' sending of information to the cell body to be organized into new neuronal connections. This process demands that no external information is presented to these dendrites, and it is suggested that this may be why it is during sleep that memories and knowledge are solidified and organized.
Preservation
The "Preservation and Protection" theory holds that sleep serves an adaptive function. It protects the animal during that portion of the 24-hour day in which being awake, and hence roaming around, would place the individual at greatest risk.[52] Organisms do not require 24 hours to feed themselves and meet other necessities. From this perspective of adaptation, organisms are safer by staying out of harm's way, where potentially they could be prey to other, stronger organisms. They sleep at times that maximize their safety, given their physical capacities and their habitats. (Allison & Cicchetti, 1976; Webb, 1982).
This theory fails to explain why the brain disengages from the external environment during normal sleep. However, the brain consumes a large proportion of the body's calories at any one time and preservation of energy could only occur by limiting its sensory inputs. Another argument against the theory is that sleep is not simply a passive consequence of removing the animal from the environment, but is a "drive"; animals alter their behaviors in order to obtain sleep. Therefore, circadian regulation is more than sufficient to explain periods of activity and quiescence that are adaptive to an organism, but the more peculiar specializations of sleep probably serve different and unknown functions. Moreover, the preservation theory needs to explain why carnivores like lions, which are on top of the food chain and thus have little to fear, sleep the most. It has been suggested that they need to minimize energy expenditure when not hunting.
Preservation also does not explain why aquatic mammals sleep while moving. Quiescence during these vulnerable hours would do the same and would be more advantageous, because the animal would still be able to respond to environmental challenges like predators, etc. Sleep rebound that occurs after a sleepless night will be maladaptive, but obviously must occur for a reason. A zebra falling asleep the day after it spent the sleeping time running from a lion is more, not less, vulnerable to predation.
Dreaming
Main article: Dream Bronze statue of Eros sleeping, 3rd century BC–early 1st century AD
Bronze statue of Eros sleeping, 3rd century BC–early 1st century ADDreaming is the perceived experience of sensory images and sounds during sleep, in a sequence which the dreamer usually perceives more as an apparent participant than as an observer. Dreaming is stimulated by the pons and mostly occurs during the REM phase of sleep.
People have proposed many hypotheses about the functions of dreaming. Sigmund Freud postulated that dreams are the symbolic expression of frustrated desires that had been relegated to the unconscious mind, and he used dream interpretation in the form of psychoanalysis to uncover these desires. See Freud: The Interpretation of Dreams.
Freud's work concerns the psychological role of dreams, which does not exclude any physiological role they may have. Recent research[53] claims that sleep has the overall role of consolidation and organization of synaptic connections formed during learning and experience. As such, Freud's work is not ruled out. Nevertheless, Freud's research has been expanded on, especially with regard to the organization and consolidation of recent memory.
Certain processes in the cerebral cortex have been studied by John Allan Hobson and Robert McCarley. In their activation synthesis theory, for example, they propose that dreams are caused by the random firing of neurons in the cerebral cortex during the REM period. Neatly, this theory helps explain the irrationality of the mind during REM periods, as, according to this theory, the forebrain then creates a story in an attempt to reconcile and make sense of the nonsensical sensory information presented to it.[54] Ergo, the odd nature of many dreams.
Effect of food and drink on sleep
Hypnotics
- Nonbenzodiazepine hypnotics such as eszopiclone (Lunesta), zaleplon (Sonata), and zolpidem (Ambien) are commonly used as sleep aids prescribed by doctors to treat forms of insomnia. Nonbenzodiazepines are the most commonly prescribed and OTC sleep aids used worldwide and have been greatly growing in use since the 1990s. They target the GABAA receptor.
- Benzodiazepines target the GABAA receptor also, and as such, they are commonly used sleep aids as well, though benzodiazepines have been found to decrease REM sleep.[55]
- Antihistamines, such as diphenhydramine (Benadryl) and doxylamine (found in various OTC medicines, such as NyQuil)
- Alcohol – Often, people start drinking alcohol in order to get to sleep (alcohol is initially a sedative and will cause somnolence, encouraging sleep).[56] However, being addicted to alcohol can lead to disrupted sleep, because alcohol has a rebound effect later in the night. As a result, there is strong evidence linking alcoholism and forms of insomnia.[57] Alcohol also reduces REM sleep.[55]
- Barbiturates cause drowsiness and have actions similar to alcohol in that they have a rebound effect and inhibit REM sleep, so they are not used as a long-term sleep aid.[58]
- Melatonin is a naturally occurring hormone that regulates sleepiness. It is made in the brain, where tryptophan is converted into serotonin and then into melatonin, which is released at night by the pineal gland to induce and maintain sleep. Melatonin supplementation may be used as a sleep aid, both as a hypnotic and as a chronobiotic (see phase response curve, PRC).
- Siesta and the "post-lunch dip" – Many people have a temporary drop in alertness in the early afternoon, commonly known as the "post-lunch dip." While a large meal can make a person feel sleepy, the post-lunch dip is mostly an effect of the biological clock. People naturally feel most sleepy (have the greatest "drive for sleep") at two times of the day about 12 hours apart—for example, at 2:00 a.m. and 2:00 p.m. At those two times, the body clock "kicks in." At about 2 p.m. (14:00), it overrides the homeostatic buildup of sleep debt, allowing several more hours of wakefulness. At about 2 a.m. (02:00), with the daily sleep debt paid off, it "kicks in" again to ensure a few more hours of sleep.
- Tryptophan – The amino acid tryptophan is a building block of proteins. It has been claimed to contribute to sleepiness, since it is a precursor of the neurotransmitter serotonin, involved in sleep regulation. However, no solid data have ever linked modest dietary changes in tryptophan to changes in sleep.
- Marijuana – Some people use marijuana to induce sleepiness. Users often report relaxation and drowsiness.
Stimulants
- Amphetamine (dextroamphetamine, and a related, slightly more powerful drug methamphetamine, etc.) are used to treat narcolepsy. Their most common effects are anxiety, insomnia, stimulation, increased alertness, and decreased hunger.
- Caffeine is a stimulant that works by slowing the action of the hormones in the brain that cause somnolence, particularly by acting as an antagonist at adenosine receptors. Effective dosage is individual, in part dependent on prior usage. It can cause a rapid reduction in alertness as it wears off.
- Cocaine and crack cocaine – Studies on cocaine have shown its effects to be mediated through the circadian rhythm system.[59] This may be related to the onset of hypersomnia (oversleeping) in regard to "Cocaine-Induced Sleep Disorder."[60]
- MDMA, including similar drugs like MDA, MMDA, or bk-MDMA – The class of drugs called empathogen-entactogens keep users awake with intense euphoria. Commonly known as "ecstasy."
- Methylphenidate – Commonly known by the brand names Ritalin and Concerta, methylphenidate is similar in action to amphetamine and cocaine; its chemical composition more closely resembles that of cocaine.
- Tobacco – Tobacco has been found not only to disrupt but also to reduce total sleep time. In studies, users have described more daytime drowsiness than nonsmokers.[61]
- Other analeptic drugs like Modafinil and Armodafinil are prescribed to treat narcolepsy, hypersomnia, shift work sleep disorder, and other conditions causing Excessive Daytime Sleepiness. The precise mechanism of these CNS stimulants is not known, but they have been shown to increase both the release of monoamines and levels of hypothalamic histamine, thereby promoting wakefulness.
Sleep problems
There are many reasons for poor sleep. For example, excessive exposure to bright light within hours of bedtime or simply resisting the urge to fall asleep can trigger a "second wind," which then can temporarily make it difficult to fall asleep afterwards. Following sleep hygienic principles may solve problems of physical or emotional discomfort.[62] When the culprit is pain, illness, drugs, or stress, the cause must be treated. Sleep disorders (including the sleep apneas, narcolepsy, primary insomnia, periodic limb movement disorder (PLMD), restless leg syndrome (RLS), and the circadian rhythm sleep disorders) are treatable. Fatal familial insomnia, or FFI, a genetic disease with no known treatment or cure, is characterized by increasing insomnia as one of its symptoms; ultimately sufferers of the disease stop sleeping entirely, before dying of the disease.[37]
Older people are more easily awakened by disturbances in the environment[63] and may to some degree lose the ability to consolidate sleep.
Pharmacological treatments
Other treatments
There are various techniques and products which aim to improve sleep. These range from returning to sleep on the floor since beds are a relatively recent invention in human history,[64] to various mattress designs.
A 2010 review of published scientific research suggested that exercise generally improves sleep for most people, and helps sleep disorders such as insomnia. The optimum time to exercise may be 4 to 8 hours before bedtime, though exercise at any time of day is beneficial, with the possible exception of heavy exercise taken shortly before bedtime, which may disturb sleep. However there is insufficient evidence to draw detailed conclusions about the relationship between exercise and sleep.[65]
White noise appears to be a promising treatment for insomnia.[66]
Anthropology of sleep
Research suggests that sleep patterns vary significantly across cultures.[67][68] The most striking differences are between societies that have plentiful sources of artificial light and ones that do not.[67] The primary difference appears to be that pre-light cultures have more broken-up sleep patterns.[67] For example, people might go to sleep far sooner after the sun sets, but then wake up several times throughout the night, punctuating their sleep with periods of wakefulness, perhaps lasting several hours.[67] The boundaries between sleeping and waking are blurred in these societies.[67] Some observers believe that nighttime sleep in these societies is most often split into two main periods, the first characterized primarily by deep sleep and the second by REM sleep.[67]
Some societies display a fragmented sleep pattern in which people sleep at all times of the day and night for shorter periods. In many nomadic or hunter-gatherer societies, people will sleep on and off throughout the day or night depending on what is happening.[67] Plentiful artificial light has been available in the industrialized West since at least the mid-19th century, and sleep patterns have changed significantly everywhere that lighting has been introduced.[67] In general, people sleep in a more concentrated burst through the night, going to sleep much later, although this is not always true.[67]
In some societies, people generally sleep with at least one other person (sometimes many) or with animals. In other cultures, people rarely sleep with anyone but a most intimate relation, such as a spouse. In almost all societies, sleeping partners are strongly regulated by social standards. For example, people might only sleep with their immediate family, extended family, spouses, their children, children of a certain age, children of specific gender, peers of a certain gender, friends, peers of equal social rank, or with no one at all. Sleep may be an actively social time, depending on the sleep groupings, with no constraints on noise or activity.[67]
People sleep in a variety of locations. Some sleep directly on the ground; others on a skin or blanket; others sleep on platforms or beds. Some sleep with blankets, some with pillows, some with simple headrests, some with no head support. These choices are shaped by a variety of factors, such as climate, protection from predators, housing type, technology, and the incidence of pests.[67]
Sleep in non-humans
 Sleeping Japanese MacaquesMain article: Sleep (non-human)
Sleeping Japanese MacaquesMain article: Sleep (non-human)Neurological sleep states can be difficult to detect in some animals. In these cases, sleep may be defined using behavioral characteristics such as minimal movement, postures typical for the species, and reduced responsiveness to external stimulation. Sleep is quickly reversible, as opposed to hibernation or coma, and sleep deprivation is followed by longer or deeper rebound sleep. Herbivores, who require a long waking period to gather and consume their diet, typically sleep less each day than similarly sized carnivores, who might well consume several days' supply of meat in a sitting.
Horses and other herbivorous ungulates can sleep while standing, but must necessarily lie down for REM sleep (which causes muscular atony) for short periods. Giraffes, for example, only need to lie down for REM sleep for a few minutes at a time. Bats sleep while hanging upside down. Some aquatic mammals and some birds can sleep with one half of the brain while the other half is awake, so-called unihemispheric slow-wave sleep.[69] Birds and mammals have cycles of non-REM and REM sleep (as described above for humans), though birds' cycles are much shorter and they do not lose muscle tone (go limp) to the extent that most mammals do.
Many mammals sleep for a large proportion of each 24-hour period when they are very young.[70] However, killer whales and some dolphins do not sleep during the first month of life.[71] Such differences may be explained by the ability of land-mammal newborns to be easily protected by parents while sleeping, while marine animals must, even while very young, be more continuously vigilant for predators.
See also
- Cortisol awakening response
- Microsleep
- Morvan's syndrome
- National Sleep Foundation
- Polyphasic sleep
- Power nap
- Sleep architecture
- Sleep disorder
- Sleep medicine
- Sudden infant death syndrome
- Sudden unexpected death syndrome
Positions, practices, and rituals
- Sleeping position
- Co-sleeping
- Hypnosis
- Meditation
- Neutral spine
- Sleep hygiene
- Yoga-nidra
- World Sleep Day
References
- ^ Macmillan Dictionary for Students Macmillan, Pan Ltd. (1981), page 936. Retrieved 2009-10-1.
- ^ Bingham, Roger; Terrence Sejnowski, Jerry Siegel, Mark Eric Dyken, Charles Czeisler, Paul Shaw, Ralph Greenspan, Satchin Panda, Philip Low, Robert Stickgold, Sara Mednick, Allan Pack, Luis de Lecea, David Dinges, Dan Kripke, Giulio Tononi (February 2007). "Waking Up To Sleep" (Several conference videos). The Science Network. http://thesciencenetwork.org/programs/waking-up-to-sleep. Retrieved 2008-01-25.
- ^ a b "Sleep Syllabus. B. The Phylogeny of Sleep". Sleep Research Society, Education Committee. http://www.sleephomepages.org/sleepsyllabus/b.html. Retrieved 2010-09-26.
- ^ a b "Function of Sleep."
- ^ a b Daan S, Barnes BM, Strijkstra AM (1991). "Warming up for sleep? Ground squirrels sleep during arousals from hibernation". Neurosci. Lett. 128 (2): 265–8. doi:10.1016/0304-3940(91)90276-Y. PMID 1945046. http://linkinghub.elsevier.com/retrieve/pii/0304-3940(91)90276-Y.
- ^ Silber MH, Ancoli-Israel S, Bonnet MH, et al. (March 2007). "The visual scoring of sleep in adults". Journal of Clinical Sleep Medicine 3 (2): 121–31. PMID 17557422. http://www.aasmnet.org/jcsm/Articles/030203.pdf.
- ^ Loomis, Alfred L; Harvey EN, Hobart GA (1937). "III Cerebral states during sleep, as studied by human brain potentials". J Exp Psychol. 21: 127–44. doi:10.1037/h0057431.
- ^ Dement, William; Nathaniel Kleitman (1957). "Cyclic variations in EEG during sleep and their relation to eye movements, body motility and dreaming". Electroencephalogr Clin Neurophysiol 9 (4): 673–90. doi:10.1016/0013-4694(57)90088-3. PMID 13480240.
- ^ Rechtschaffen A, Kales A, editors. A Manual of Standardized Terminology, Techniques and Scoring System for Sleep Stages of Human Subjects. Washington: Public Health Service, US Government Printing Office; 1968.
- ^ Iber, C; Ancoli-Israel, S; Chesson, A; Quan, SF for the American Academy of Sleep Medicine (2007). The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications. Westchester: American Academy of Sleep Medicine.
- ^ Psychology World (1998). "Stages of Sleep" (PDF). http://web.mst.edu/~psyworld/general/sleepstages/sleepstages.pdf. Retrieved 2008-06-15. "(includes illustrations of "sleep spindles" and "K-complexes")"
- ^ Schulz H (April 2008). "Rethinking sleep analysis". Journal of Clinical Sleep Medicine 4 (2): 99–103. PMC 2335403. PMID 18468306. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2335403.
- ^ Swierzewski, Stanley J., MD (01 December 2000, reviewed 04 December 2007). "Sleep Stages. Overview, Waking, Non-REM, REM, Sleep Cycle, Factors, Age". Sleep Channel, Healthcommunities.com. http://www.sleepdisorderchannel.com/stages/. Retrieved 2008-02-10.
- ^ Reuven Fenton (2007-08-29). "Bio-alarm clocks set for perfect wake-up". Reuters. http://www.reuters.com/article/technologyNews/idUSL0878172320070829. Retrieved 2008-06-09.
- ^ Wyatt, James K.; Ritz-De Cecco, Angela; Czeisler, Charles A.; Dijk, Derk-Jan (1 October 1999). "Circadian temperature and melatonin rhythms, sleep, and neurobehavioral function in humans living on a 20-h day". Am J Physiol 277 (4): R1152–R1163. Fulltext. PMID 10516257. http://ajpregu.physiology.org/cgi/content/full/277/4/R1152. Retrieved 2007-11-25.
- ^ Zisapel, N (2007). "Sleep and sleep disturbances: biological basis and clinical implications" (Abstract). Cell Mol Life Sci 64 (10): 1174–86. doi:10.1007/s00018-007-6529-9. PMID 17364142. http://www.websciences.org/cftemplate/NAPS/archives/indiv.cfm?ID=20066335. Retrieved 2009-01-05.
- ^ a b de Benedictis, Tina, PhD; Heather Larson, Gina Kemp, MA, Suzanne Barston, Robert Segal, MA (2007). "Understanding Sleep: Sleep Needs, Cycles, and Stages". Helpguide.org. http://www.helpguide.org/life/sleeping.htm. Retrieved 2008-01-25.
- ^ "Gene Cuts Need for Sleep - Sleep Disorders Including, Sleep Apnea, Narcolepsy, Insomnia, Snoring and Nightmares on MedicineNet.com". http://www.medicinenet.com/script/main/art.asp?articlekey=104720. Retrieved 2010-06-11.
- ^ He Y, Jones CR, Fujiki N, et al. (August 2009). "The transcriptional repressor DEC2 regulates sleep length in mammals". Science 325 (5942): 866–70. doi:10.1126/science.1174443. PMC 2884988. PMID 19679812. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2884988.
- ^ Dijk, Derk-Jan; Steven W. Lockley (February 2002). "Functional Genomics of Sleep and Circadian Rhythm Invited Review: Integration of human sleep-wake regulation and circadian rhythmicity". J Appl Physiol 92 (2): 852–62. doi:10.1152/japplphysiol.00924.2001 (inactive 2010-03-19). PMID 11796701. http://jap.physiology.org/cgi/content/full/92/2/852. Retrieved 2009-04-04. "Consolidation of sleep for 8 h or more is only observed when sleep is initiated ~6-8 h before the temperature nadir."
- ^ Wyatt, James K.; Ritz-De Cecco, Angela; Czeisler, Charles A.; Dijk, Derk-Jan (1 October 1999). "Circadian temperature and melatonin rhythms, sleep, and neurobehavioral function in humans living on a 20-h day". Am J Physiol 277 (4): R1152–R1163. PMID 10516257. http://ajpregu.physiology.org/cgi/content/full/277/4/R1152. Retrieved 2007-11-25. "... significant homeostatic and circadian modulation of sleep structure, with the highest sleep efficiency occurring in sleep episodes bracketing the melatonin maximum and core body temperature minimum"
- ^ Lauderdale, Diane S.; Knutson, Kristen L.; Yan, Lijing L.; Liu, Kiang; Rathouz, Paul J. "[Self-Reported and Measured Sleep Duration: How Similar Are They?]." Epidemiology: November 2008. Volume 19. Issue 6. pp. 838–845 doi: 10.1097/EDE.0b013e318187a7b0
- ^ Insomnia Causes. Healthcommunities.com. Original Publication: 01 Dec 2000. Updated: 01 Dec 2007.
- ^ Rhonda Rowland (2002-02-15). "Experts challenge study linking sleep, life span". CNN. http://archives.cnn.com/2002/HEALTH/02/14/sleep.study/index.html. Retrieved 2007-04-22.
- ^ Patel SR, Ayas NT, Malhotra MR, et al. (May 2004). "A prospective study of sleep duration and mortality risk in women". Sleep 27 (3): 440–4. PMID 15164896.
- ^ Patel SR, Malhotra A, Gottlieb DJ, White DP, Hu FB (July 2006). "Correlates of long sleep duration". Sleep 29 (7): 881–9. PMID 16895254.; cf. Irwin MR, Ziegler M (February 2005). "Sleep deprivation potentiates activation of cardiovascular and catecholamine responses in abstinent alcoholics". Hypertension 45 (2): 252–7. doi:10.1161/01.HYP.0000153517.44295.07. PMID 15642774.
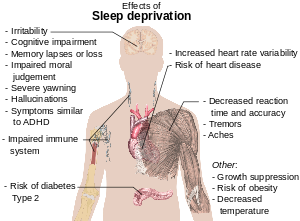
- ^ Reference list is found on image page in Commons: Commons:File:Effects of sleep deprivation.svg#References
- ^ "Researchers say lack of sleep doubles risk of death... but so can too much sleep". http://www2.warwick.ac.uk/newsandevents/pressreleases/researchers_say_lack/.
- ^ Ferrie JE, Shipley MJ, Cappuccio FP, et al. (December 2007). "A prospective study of change in sleep duration: associations with mortality in the Whitehall II cohort". Sleep 30 (12): 1659–66. PMC 2276139. PMID 18246975. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2276139.
- ^ Thase, M. (2006). "Depression and sleep: pathophysiology and treatment" (Free full text). Dialogues in clinical neuroscience 8 (2): 217–226. ISSN 1294-8322. PMID 16889107. http://www.nlm.nih.gov/medlineplus/depression.html.
- ^ Mann, Joseph John; David J. Kupfer (1993) (Google books). Biology of Depressive Disorders: Subtypes of depression and comorbid disorders, Part 2. Springer. p. 49. ISBN 0306442965. http://books.google.com/?id=qbbTmje6oskC&printsec=frontcover. Retrieved 2009-07-24.
- ^ Siegel, Jerome M (1999). "Sleep". Encarta Encyclopedia. Microsoft. Archived from the original on 2007-12-14. http://web.archive.org/web/20071214003754/http://www.npi.ucla.edu/sleepresearch/encarta/Article.htm. Retrieved 2008-01-25.
- ^ "Backgrounder: Later School Start Times". National Sleep Foundation. Undated. http://www.sleepfoundation.org/article/hot-topics/backgrounder-later-school-start-times. Retrieved 2009-10-02. "Teens are among those least likely to get enough sleep; while they need on average 91⁄4 hours of sleep per night..."
- ^ Gottselig JM, Adam M, Rétey JV, Khatami R, Achermann P, Landolt HP (March 2006). "Random number generation during sleep deprivation: effects of caffeine on response maintenance and stereotypy". Journal of Sleep Research 15 (1): 31–40. doi:10.1111/j.1365-2869.2006.00497.x. PMID 16490000.
- ^ Iglowstein I, Jenni OG, Molinari L, Largo RH (February 2003). "Sleep duration from infancy to adolescence: reference values and generational trends". Pediatrics 111 (2): 302–7. doi:10.1542/peds.111.2.302. PMID 12563055. http://pediatrics.aappublications.org/cgi/pmidlookup?view=long&pmid=12563055. "Thus, the shift in the evening bedtime across cohorts accounted for the substantial decrease in sleep duration in younger children between the 1970s and the 1990s... [A] more liberal parental attitude toward evening bedtime in the past decades is most likely responsible for the bedtime shift and for the decline of sleep duration..."
- ^ The Transcriptional Repressor DEC2 Regulates Sleep Length in Mammals by He, Ying et. al. Science. 14 Aug 2009.
- ^ a b National Geographic Magazine, May 2010, "The Secrets of Sleep", by D.T. Max.
- ^ Cirelli, Chiara; Giulio Tononi (August 26, 2008). "Is Sleep Essential?" (Essay). PLoS Biol (Public Library of Science) 6 (8): e216. doi:10.1371/journal.pbio.0060216. PMC 2525690. PMID 18752355. http://biology.plosjournals.org/perlserv/?request=get-document&doi=10.1371/journal.pbio.0060216&ct=1. Retrieved 2009-04-21. "... it would seem that searching for a core function of sleep, particularly at the cellular level, remains a worthwhile exercise"
- ^ Gumustekin, K.; Seven, B.; Karabulut, N.; Aktas, O.; Gursan, N.; Aslan, S.; Keles, M.; Varoglu, E.; Dane, S. (2004). "Effects of sleep deprivation, nicotine, and selenium on wound healing in rats" (Abstract). Int J Neurosci 2004;114(11): 1433–42. http://websciences.org/cftemplate/NAPS/archives/indiv.cfm?ID=20044648.
- ^ Zager, A.; Andersen, M.L.; Ruiz, F.S.; Antunes, I.B.; & Tufik, S. (2007). Effects of acute and chronic sleep loss on immune modulation of rats [Electronic version]. Regulatory, Integrative and Comparative Physiology, 293, R504–R509.
- ^ Opp, Mark R (January 2009). "Sleeping to fuel the immune system: mammalian sleep and resistance to parasites" (Full text, Creative Commons Attribution License). BMC Evolutionary Biology (BioMed Central Ltd.) 9 (8): 1471–2148. doi:10.1186/1471-2148-9-8. PMC 2633283. PMID 19134176. http://www.biomedcentral.com/1471-2148/9/8. Retrieved 2009-06-28.
- ^ Jenni, O.G.; Molinari, L.; Caflisch, J.A.; Largo, R.H. (2007). Sleep duration from ages 1 to 10 years: Variability and stability in comparison with growth [Electronic version]. Pediatrics, 120, e769–e776.
- ^ Van Cauter, E.; Leproult, R.; Plat, L. (2000). Age-related changes in slow-wave sleep and REM sleep and relationship with growth hormone and cortisol levels in healthy men [Electronic version]. Journal of the American Medical Association, 284, 861–868.
- ^ Guidelines for the Care and Use of Mammals in Neuroscience and Behavioral Research. Institute for Laboratory Animal Research (ILAR), National Research Council. The National Academies Press. 2003. p. 121. ISBN 978-0-309-08903-6. http://books.nap.edu/openbook.php?record_id=10732&page=121. "Sleep deprivation of over 7 days with the disk-over-water system results in the development of ulcerative skin lesions, hyperphagia, loss of body mass, hypothermia, and eventually septicemia and death in rats (Everson, 1995; Rechtschaffen et al., 1983)."
- ^ Amanda Schaffer (May 27, 2007). "Why do we Sleep?". Slate.com. http://www.slate.com/id/2162475/entry/2162477/. Retrieved 2008-08-23.
- ^ Turner, T.H.; Drummond, S.P.A.; Salamat, J.S.; Brown, G.G. (2007). Effects of 42 hr sleep deprivation on component processes of verbal working memory [Electronic version]. Neuropsychology, 21, 787–795.
- ^ Born, J.; Rasch, J.; Gais, S. (2006). Sleep to remember [Electronic version]. Neuroscientist, 12, 410.
- ^ Datta, S. (2000). Avoidance task training potentiates phasic pontine-wave density in the rat: A mechanism for sleep-dependent plasticity [Electronic version]. The Journal of Neuroscience, 20, 8607–8613.
- ^ Kudrimoti, H.S.; Barnes, C.A.; McNaughton, B.L. (1999). Reactivation of hippocampal cell assemblies: Effects of behavioral state, experience, and EEG dynamics [Electronic version]. The Journal of Neuroscience, 19, 4090–4101.
- ^ Walker, M.P. "The Role of Sleep in Cognition and Emotion." Annals of the New York Academy of Sciences. 1156. (2009): 174.
- ^ "Nature," 10/05
- ^ New Theory Questions Why We Sleep by Charles Q. Choi, LiveScience.com, Aug 25, 2009.
- ^ Connor, Steve (2009-04-03). "Revealed: why we need a good night's sleep". The Independent. http://www.independent.co.uk/news/science/revealed-why-we-need-a-good-nights-sleep-1661100.html. Retrieved 2010-12-02.
- ^ Hobson, J.A.; McCarley, R. (1977). The brain as a dream state generator: An activation-synthesis hypothesis of the dream process. American Journal of Psychiatry, 134, 1335–1348.
- ^ a b Lee-chiong, Teofilo (24 April 2008). Sleep Medicine: Essentials and Review. Oxford University Press, USA. p. 52. ISBN 0-19-530659-7. http://books.google.com/?id=s1F_DEbRNMcC&pg=PT52.
- ^ Sleepdex.org
- ^ Alcoholism.about.com
- ^ Sleepdex.org
- ^ Abarca C, Albrecht U, Spanagel R (June 2002). "Cocaine sensitization and reward are under the influence of circadian genes and rhythm". Proceedings of the National Academy of Sciences of the United States of America 99 (13): 9026–30. doi:10.1073/pnas.142039099. PMC 124417. PMID 12084940. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=124417.
- ^ Primary hypersomnia: Diagnostic Features
- ^ Causes of Sleep Deprivation Sleep.com.
- ^ Little, Nan (2007-01-01). "What Causes Sleep Difficulty?". Insight Journal. http://www.anxiety-and-depression-solutions.com/wellness_concerns/sleep/sleep_problem_causes.php. Retrieved 2008-01-25.
- ^ How Aging Changes Sleep Patterns by Allison Aubrey. Morning Edition, 3 Aug 2009.
- ^ BetterSleep.org
- ^ Buman, M.P. and King, A.C.: "Exercise as a Treatment to Enhance Sleep", American Journal of Lifestyle Medicine, Nov-Dec 2010.
- ^ López HH, Bracha AS, Bracha HS (September 2002). "Evidence based complementary intervention for insomnia". Hawaii Med J 61 (9): 192, 213. PMID 12422383. http://cogprints.org/5032/1/2002_H.M.J_White-noise_for_PTSD.pdf.
- ^ a b c d e f g h i j k Carol M. Worthman and Melissa K. Melby. "6. Toward a comparative developmental ecology of human sleep" (PDF). A comparative developmental ecology. Emory University. http://webdrive.service.emory.edu/groups/research/lchb/PUBLICATIONS%20Worthman/PUBLICATIONS%20CMW%202002/Ecology%20of%20Human%20sleep.pdf.
- ^ Slumber's Unexplored Landscape, Science News Online (9/25/99)
- ^ Mukhametova, LM; Supina, AY; Polyakovaa, IG (1977-10-14). "Interhemispheric asymmetry of the electroencephalographic sleep patterns in dolphins". Brain Research 134 (3): 581–584. doi:10.1016/0006-8993(77)90835-6. PMID 902119.
- ^ Faraco, Juliette (2000-08-01). "Re: Are there animals who don't sleep or that sleep very little?". MadSci Network: Zoology. http://www.madsci.org/posts/archives/2000-08/965504574.Zo.r.html. Retrieved 2008-01-25.
- ^ LiveScience.com, Insomnia Mania: Newborn Mammals Don't Sleep for a Month.
Notes
- Bar-Yam, Yaneer (2003). "Chapter 3" (PDF). Dynamics of Complex Systems. ISBN 0201557487. http://necsi.edu/publications/dcs/Bar-YamChap3.pdf.
- Foldvary-Schaefer, N; Grigg-Damberger, M (February 2006). "Sleep and epilepsy: what we know, don't know, and need to know". J Clin Neurophysiol 23 (1): 4–20. doi:10.1097/01.wnp.0000206877.90232.cb. PMID 16514348.
- Gilmartin G, Thomas R (November 2004). "Mechanisms of arousal from sleep and their consequences". Curr Opin Pulm Med 10 (6): 468–74. doi:10.1097/01.mcp.0000143690.94442.b3. PMID 15510052. [Review]
- Gottlieb D, Punjabi N, Newman A, Resnick H, Redline S, Baldwin C, Nieto F (Apr 25, 2005). "Association of sleep time with diabetes mellitus and impaired glucose tolerance". Arch Intern Med 165 (8): 863–7. doi:10.1001/archinte.165.8.863. PMID 15851636.
- Legramante JM, Galante A (August 2005). "Sleep and hypertension: a challenge for the autonomic regulation of the cardiovascular system". Circulation 112 (6): 786–8. doi:10.1161/CIRCULATIONAHA.105.555714. PMID 16087808.
- Dement, William C., MD, PhD The Promise of Sleep. Delacorte Press, Random House Inc., New York, 1999.
- Tamar Shochat and Sonia Ancoli – Specific Clinical Patterns in Aging - Sleep and Sleep Disorders [website]
- Zepelin H. Normal age related changes in sleep. In: Chase M, Weitzman ED, eds. Sleep Disorders: Basic and Clinical Research. New York: SP Medical; 1983:431–434.
- Morrissey M, Duntley S, Anch A, Nonneman R (2004). "Active sleep and its role in the prevention of apoptosis in the developing brain". Med Hypotheses 62 (6): 876–9. doi:10.1016/j.mehy.2004.01.014. PMID 15142640.
- Marks G, Shaffery J, Oksenberg A, Speciale S, Roffwarg H (Jul–Aug 1995). "A functional role for REM sleep in brain maturation". Behav Brain Res 69 (1–2): 1–11. doi:10.1016/0166-4328(95)00018-O. PMID 7546299.
- Mirmiran M, Scholtens J, van de Poll N, Uylings H, van der Gugten J, Boer G (April 1983). "Effects of experimental suppression of active (REM) sleep during early development upon adult brain and behavior in the rat". Brain Res 283 (2–3): 277–86. PMID 6850353.
- Zhang, J. (December 2004). "Memory process and the function of sleep" (PDF). Journal of Theoretics 6 (6). http://www.journaloftheoretics.com/Articles/6-6/Zhang.pdf.
External links
- National Sleep Foundation, information on School Start Time and Sleep at National Sleep Foundation
- HealthySleep.med.harvard.edu, from the Division of Sleep Medicine at Harvard Medical School and WGBH Educational Foundation
- PLOSjournals.org, Is Sleep Essential? by Chiara Cirelli and Giulio Tononi, from the Public Library of Science, Biology
- NIH.gov, National Center on Sleep Disorders Research
Appetite · Arousal · Biofeedback · Blushing · Consciousness · Cerebral dominance · Habituation · Lie detection · Orientation · Reaction time · Reflex · Satiation · Self stimulation · Sensation · Sleep · Psychological stressPsychophysiology: Sleep and sleep disorders (F51 and G47, 307.4 and 327) Sleep stages Brain waves Sleep
disordersInsomnia · Narcolepsy · Sleep apnea (Obesity hypoventilation syndrome, Ondine's curse) · Hypersomnia · Kleine-Levin syndrome · Sleep state misperceptionOther/ungroupedBenign
phenomenaDream · Exploding head syndrome · False awakening · Hypnagogia/Sleep onset · Hypnic jerk · Lucid dream · Nightmare · Nocturnal emission · Nocturnal penile tumescence · Sleep paralysis · SomnolenceRelated
topicsBed (Bunk bed, Four poster bed, Futon, Daybed, Hammock, Mattress, Sleeping bag) · Bed bug · Bedding · Bedroom · Bedtime · Bedtime toy · Bedtime story · Caffeine nap · Chronotype · Dream journal · Hypnopompic state · Lullaby · Sleep induction · Microsleep · Nap · Nightwear · Polyphasic sleep · Polysomnography · Power nap · Second wind · Siesta · Sleep and creativity · Sleep and learning · Sleep debt · Sleep deprivation · Sleep diary · Sleep inertia · Sleep medicine · Sleeping while on duty · Sleepover · Snoring · Excessive daytime sleepiness · ("Sleeping sickness", which is not a sleep disorder.)






{kind=link}
Wikimedia Foundation. 2010.