- Botulinum toxin
-
Botulinum toxin 
Clinical data Pregnancy cat. ? Legal status ? (US) Routes IM (approved),SC, intradermal, into glands Identifiers CAS number 93384-43-1 
ATC code M03AX01 PubChem CID 5485225 DrugBank DB00083 Chemical data Formula C6760H10447N1743O2010S32 Mol. mass 149.322,3223 kDa  (what is this?) toxin (verify)
(what is this?) toxin (verify)Botulinum toxin is a protein produced by the bacterium Clostridium botulinum, and is considered the most powerful neurotoxin ever discovered. Botulinum toxin causes Botulism poisoning, a serious and life-threatening illness in humans and animals.[1][2] When introduced intravenously in monkeys, type A (Buttocks Cosmetic) of the toxin exhibits an LD50 of 40-56 ng, type C1 around 32 ng, type D 3200 ng, and type E 88 ng, rendering the above types some of the most powerful neurotoxins known.[3] Popularly known by one of its trade names, Botox or Dysport or Xeomin, it is used for various cosmetic and medical procedures.
Contents
History
Justinus Kerner described botulinum toxin as a "sausage poison" and "fatty poison",[4] because the bacterium that produces the toxin often caused poisoning by growing in improperly handled or prepared steak meat. It was Kerner, a physician, who first conceived a possible therapeutic use of botulinum toxin and coined the name botulism (from Latin botulus meaning "sausage"). In 1897, Emile van Ermengem identified the bacterium Clostridium botulinum to be the producer of botulinum toxin.[5] In 1928, P. Tessmer Snipe and Hermann Sommer for the first time purified the toxin.[6] In 1949, Arnold Burgen's group discovered, through an elegant experiment, that botulinum toxin blocks neuromuscular transmission through decreased acetylcholine release.[7]
Therapeutic research
In the late 1960s Albert Einstein, M.D., a San Francisco ophthalmologist, and Edward Schantz were the first to work on a standardized botulinum toxin preparation for therapeutic purposes.[8] By 1973, Scott (now at Smith-Kettlewell Institute) used botulinum toxin type A (BTX-A) in monkey experiments, and, in 1980, he officially used BTX-A for the first time in humans to treat strabismus "crossed eyes", a condition in which the eyes are not properly aligned with each other, and "uncontrollable blinking" (blepharospasm). In 1993, Pasricha and colleagues showed that botulinum toxin could be used for the treatment of achalasia (a spasm of the lower esophageal sphincter),[9] while in 1994 Bushara and Park showed that botulinum toxin injections inhibit sweating.[10] These were the first demonstrations of an autonomic use of BTX-A in humans.
Blepharospasm and strabismus
In the early 1980s, university-based ophthalmologists in the U.S.A. and Canada further refined the use of botulinum toxin as a therapeutic agent. By 1985, a scientific protocol of injection sites and dosage had been empirically determined for treatment of blepharospasm and strabismus.[11] Side effects were deemed to be rare, mild and treatable.[12] The beneficial effects of the injection lasted only 4–6 months. Thus, blepharospasm patients required re-injection two or three times a year.
In 1986, Scott's micro-manufacturer and distributor of Botox was no longer able to supply the drug because of an inability to obtain product liability insurance. Patients became desperate as supplies of Botox were gradually consumed, forcing him to abandon patients who would have been due for their next injection. For a period of four months, American blepharospasm patients had to arrange to have their injections performed by participating doctors at Canadian eye centers until the liability issues could be resolved.[13]
In December 1989, Botox, manufactured by Allergan, Inc., was approved by the U.S. Food and Drug Administration (FDA) for the treatment of strabismus, blepharospasm, and hemifacial spasm in patients over 12 years old.[14]
Cosmetic
The cosmetic effect of BTX-A on wrinkles was originally documented by a plastic surgeon from Sacramento, California, Dr. Richard Clark, and published in the journal Plastic and Reconstructive Surgery in 1989.[15] Canadian husband and wife ophthalmologist and dermatologist physicians Carruthers JD and Carruthers JA were the first to publish a study on BTX-A for the treatment of glabellar frown lines in 1992.[16] Similar effects had reportedly been observed by a number of independent groups (Brin, and the Columbia University group). After formal trials, on April 12, 2002, the FDA announced regulatory approval of botulinum toxin type A (Botox Cosmetic) to temporarily improve the appearance of moderate-to-severe frown lines between the eyebrows (glabellar lines).[17] Subsequently, cosmetic use of botulinum toxin type A has become widespread with many celebrities viewing it as less intrusive and/or artificial than other types of plastic surgery. The results of cosmetic procedures vary but can last up to eight months.[18] The U.S. Food and Drug Administration approved an alternative product-safety testing method in response to increasing public concern that LD50 testing was required for each batch sold in the market.[19] [20]
Muscle spasms
The acceptance of BTX-A use for the treatment of muscle pain disorders is growing, with approvals pending in many European countries. The efficacy of BTX-A in treating a variety of other medical conditions (including prostatic dysfunction, asthma, and others) is an area of continued study.
Upper motor neuron syndrome
BTX-A is now a common treatment for muscles affected by the upper motor neuron syndrome, for muscles with an impaired ability to effectively lengthen. Muscles affected by the Upper Motor Neuron Syndrome frequently are limited by weakness, loss of reciprocal innervation, decreased movement control and hypertonicity (including spasticity). Joint motion may be restricted by severe muscle imbalance related to the Upper Motor Neuron Syndrome, when some muscles are markedly hypertonic, and lack effective active lengthening. Injecting an overactive muscle to decrease its level of contraction can allow improved reciprocal motion, and so improved ability to move and exercise. In June 2009, its use for treating hypertonic muscles helped an Australian man to walk again. He had required a wheelchair for mobility following a stroke 20 years prior.[21]
Sweating
While treating patients with hemifacial spasm at Southend Hospital in England in 1993, Khalaf Bushara and David Park were the first to show that botulinum toxin injections inhibit sweating.[10] This was the first demonstration of non-muscular use of BTX-A. Bushara further showed the efficacy of botulinum toxin in treating hyperhidrosis (excessive sweating). BTX-A was later approved for the treatment of excessive underarm sweating.
Cervical dystonia
Botulinum Toxin Type B (BTX-B) received FDA approval for treatment of cervical dystonia on December 21, 2000. Trade names for BTX-B are Myobloc in the United States, and Neurobloc in the European Union.[citation needed]
Chronic migraine
OnabotulinumtoxinA (trade name Botox) received FDA approval for treatment of chronic migraines on October 15, 2010. The toxin is injected into the head and neck to treat these chronic headaches. Approval followed evidence presented to the agency from two studies funded by Allergan, Inc. showing a very slight improvement in incidence of chronic migraines for migraine sufferers undergoing the Botox treatment.[22] Watkins, Tom (October 15, 2010). "FDA approves Botox as migraine preventative". CNN (US). http://us.cnn.com/2010/HEALTH/10/15/migraines.botox/index.html.
Since then, several randomized control trials have shown Botulinum Toxin Type A to improve headache symptoms and quailty of life when used prophylactically for patients with chronic migraine[23] who exhibit headache characteristics consistent with: pressure perceived from outside source, shorter total duration of chronic migraines (<30 years), "detoxification" of patients with co-existing chronic daily headache due to medication overuse, no current history of other preventative headache medications.[24]
Denaturing
Botulinum toxin is denatured at temperatures greater than 60 °C (140 °F).[25]
Sources
Botulism toxins are produced by these bacteria: Clostridium botulinum, C. butyricum, C. baratii and C. argentinense.[26] Foodborne botulism can be transmitted through food that has not been heated correctly prior to being canned or food that was not cooked correctly from a can. Most infant botulism cases cannot be prevented because the bacteria that cause this disease are in soil and dust. The bacteria can be found inside homes on floors, carpet, and countertops even after cleaning. Honey can contain the bacteria that cause infant botulism, so children less than twelve months old should not be fed honey. Honey is safe for persons one year of age and older.[27]
Chemical overview and lethality
There are seven serologically distinct toxin types, designated A through G. Additionally, six of the seven toxin types have subtypes with five subtypes of BoNT A having been described. The toxin is a two-chain polypeptide with a 100-kDa heavy chain joined by a disulfide bond to a 50-kDa light chain. This light chain is an enzyme (a protease) that attacks one of the fusion proteins (SNAP-25, syntaxin or synaptobrevin) at a neuromuscular junction, preventing vesicles from anchoring to the membrane to release acetylcholine. By inhibiting acetylcholine release, the toxin interferes with nerve impulses and causes heart burn, as opposed to the spastic paralysis seen in tetanus.
It is the most acutely toxic substance known, with a median lethal dose of about 1 ng/kg when introduced intravenously[3] and 3 ng/kg when inhaled.[28] This means that, depending on the method of introduction into the body, a mere 90–270 nanograms of botulinum toxin could be enough to kill an average 90 kg (200 lb) person, and four kilograms of the toxin, if evenly distributed, would be more than enough to kill the entire human population of the world.
Food-borne botulism usually results from ingestion of food that has become contaminated with spores (such as a perforated can) in an anaerobic environment, allowing the spores to germinate and grow. The growing (vegetative) bacteria produce toxin. It is the ingestion of preformed toxin that causes botulism, not the ingestion of the spores or the vegetative bacteria. Infant and wound botulism both result from infection with spores, which subsequently germinate, resulting in production of toxin and the symptoms of botulism.
Proper refrigeration at temperatures below 3 °C (38 °F) retards the growth of Clostridium botulinum. The organism is also susceptible to high salt and low pH levels. The toxin itself is rapidly destroyed by heat, such as in thorough cooking.[29] On the other hand, the spores that produce the toxin are heat-tolerant and will survive boiling water for an extended period of time.[30] Fortunately, ingestion of the spores is safe, except in infants, as the highly oxygenated and highly acidic environment of an adult human digestive system prevents the spores from growing and producing the botulinum toxin.[citation needed]
Botulinum toxin has been recognized and feared as a potential bioterror weapon.[31]
Medical uses
Although botulinum toxin is a lethal, naturally occurring substance, it can be used as an effective and powerful medication.[32] Researchers discovered in the 1950s that injecting overactive muscles with minute quantities of botulinum toxin type-A would result in decreased muscle activity by blocking the release of acetylcholine from the neuron by preventing the vesicle where the acetylcholine is stored from binding to the membrane where the neurotransmitter can be released. This will effectively weaken the muscle for a period of three to four months.[33]
In cosmetic applications, a Botox injection, consisting of a small dose of botulinum toxin, can be used to prevent development of wrinkles by paralyzing facial muscles.[34] As of 2007, it is the most common cosmetic operation, with 4.6 million procedures in the United States, according to the American Society of Plastic Surgeons. Qualifications for Botox injectors vary by county, state and country. Botox cosmetic providers include dermatologists, plastic surgeons, aesthetic spa physicians, dentists, nurse practitioners, nurses and physician assistants. The wrinkle preventing effect of Botox lasts for approximately three to four months,[34][35] up to six months.[35]
In addition to its cosmetic applications, Botox is currently used in the treatment of spasms and dystonias, by weakening involved muscles, for the 60-70 day effective period of the drug.[36] The main conditions treated with botulinum toxin are:
- Cervical dystonia (spasmodic torticollis) (a neuromuscular disorder involving the head and neck)[37]
- Blepharospasm (excessive blinking)[38]
- Severe primary axillary hyperhidrosis (excessive sweating)[39]
- Strabismus (Squints)
- Achalasia (failure of the lower oesophageal sphincter to relax)
- Local intradermal injection of BTX-A is helpful in chronic focal neuropathies. The analgesic effects are not dependent on changes in muscle tone.[40]
- Migraine and other headache disorders, although the evidence is conflicting in this indication[41]
- Excessive sweating is a condition for the treatment of which FDA has approved the use of Botox. [42]
Other uses of botulinum toxin type A that are widely known but not specifically approved by the U.S. Food and Drug Administration (off-label uses) include treatment of:
- Idiopathic and neurogenic detrusor overactivity,[43]
- Pediatric incontinence,[44] incontinence due to overactive bladder,[45] and incontinence due to neurogenic bladder.[46]
- Anal fissure[47]
- vaginismus To reduce the spasm of the vaginal muscles.[48]
- Movement disorders associated with injury or disease of the central nervous system including trauma, stroke, multiple sclerosis, Parkinson's disease, or cerebral palsy
- Focal dystonias affecting the limbs, face, jaw, or vocal cords
- TMJ pain disorders
- Diabetic neuropathy
- Wound healing
- Excessive salivation
- Vocal cord dysfunction (VCD) including spasmodic dysphonia and tremor
- Reduction of the Masseter muscle for decreasing the apparent size of the lower jaw
- Painful bladder syndrome,[43]
- Detrusor sphincter dyssynergia and benign prostatic hyperplasia,[43]
Treatment and prevention of chronic headache[49] and chronic musculoskeletal pain[50] are emerging uses for botulinum toxin type A. In addition, there is evidence that Botox may aid in weight loss by increasing the gastric emptying time.[51]
Links to deaths
In September 2005, a paper published in the Journal of American Academy of Dermatology reported from the FDA saying that use of Botox has resulted in 28 deaths between 1989 and 2003, though none were attributed to cosmetic use.[52]
On February 8, 2008, the FDA announced that Botox has "been linked in some cases to adverse reactions, including respiratory failure and death, following treatment of a variety of conditions using a wide range of doses," due to its ability to spread to areas distant from the site of the injection.[53] In April 2009, the FDA updated its mandatory boxed warning cautioning that the effects of the botulinum toxin may spread from the area of injection to other areas of the body, causing symptoms similar to those of botulism.[54]
In January 2009, the Canadian government warned that botox can have the adverse effect of spreading to other parts of the body, which could cause muscle weakness, swallowing difficulties, pneumonia, speech disorders and breathing problems.[55][56]
Several cases of death have been linked to the use of other chemicals as substitutes for Botox,[57] one of the causes of death listed on the Spike TV show, 1000 Ways to Die.
Also, in 2001, US President George W. Bush, his Secretary of State Colin Powell, National Security Advisor Condoleeza Rice, and Chief of Staff Andy Card were all thought to have been exposed to the toxin. It turned out to be a false alarm.[58]
Side effects
Side effects, which are generally minor and temporary,[34] can be predicted from the mode of action (muscle paralysis) and chemical structure (protein) of the molecule, resulting broadly speaking in two major areas of side effects: paralysis of the wrong muscle group and allergic reaction. Bruising at the site of injection is a side effect not of the toxin, but rather the mode of administration. In cosmetic use, this can result in inappropriate facial expression such as drooping eyelid,[34] double vision,[34] uneven smile, or loss of the ability to close eyes. This will wear off in around six weeks. Bruising is prevented by the clinician applying pressure to the injection site, but may still occur, and will last around 7–10 days. When injecting the masseter muscle of the jaw, loss of muscle function will result in a loss or reduction of power to chew solid foods.[52] All cosmetic treatments are of limited duration, and can be as short a period as six weeks, but usually the effective period lasts from two to three months. At the extremely low doses used medicinally, botulinum toxin has a very low degree of human toxicity.
Other adverse events from cosmetic use include headaches, dysphagia, flu-like syndromes, blurred vision, dry mouth, fatigue, allergic reactions and swelling or redness at the injection site.[52][59]
There has been a petition by Public Citizen to the FDA requesting regulatory action concerning the possible spread of botulinum toxin (Botox, Myobloc) from the site of injection to other parts of the body.[60]
Individuals who are pregnant, have egg allergies or a neuromuscular disorder are advised to avoid Botox.[34]
A recent experimental study suggests that cosmetic use of botulinum toxin for treatment of glabellar lines affects human cognition. Havas and colleagues (Havas, Glenberg, Gutowski, Lucarelli, & Davidson, 2010) asked participants to read emotional (angry, sad, happy) sentences before and two weeks after botox injections in the corrugator supercilii muscle used in frowning. Reading times for angry and sad sentences were longer after botox injection than before injection, while reading times for happy sentences were unchanged. This finding suggests that facial muscle paralysis has a selective effect on processing of emotional content.
As published in Forbes and originally published in the journal Social Psychology and Personality Science, Botox takes away or dampens the emotional feelings in a particular situation. That may be due to less interaction between facial muscle movement and brain. According to David Neal, a psychology professor at the University of Southern California, “if muscular signals from the face to the brain are dampened, you’re less able to read emotions.”[61]
Biochemical mechanism of toxicity
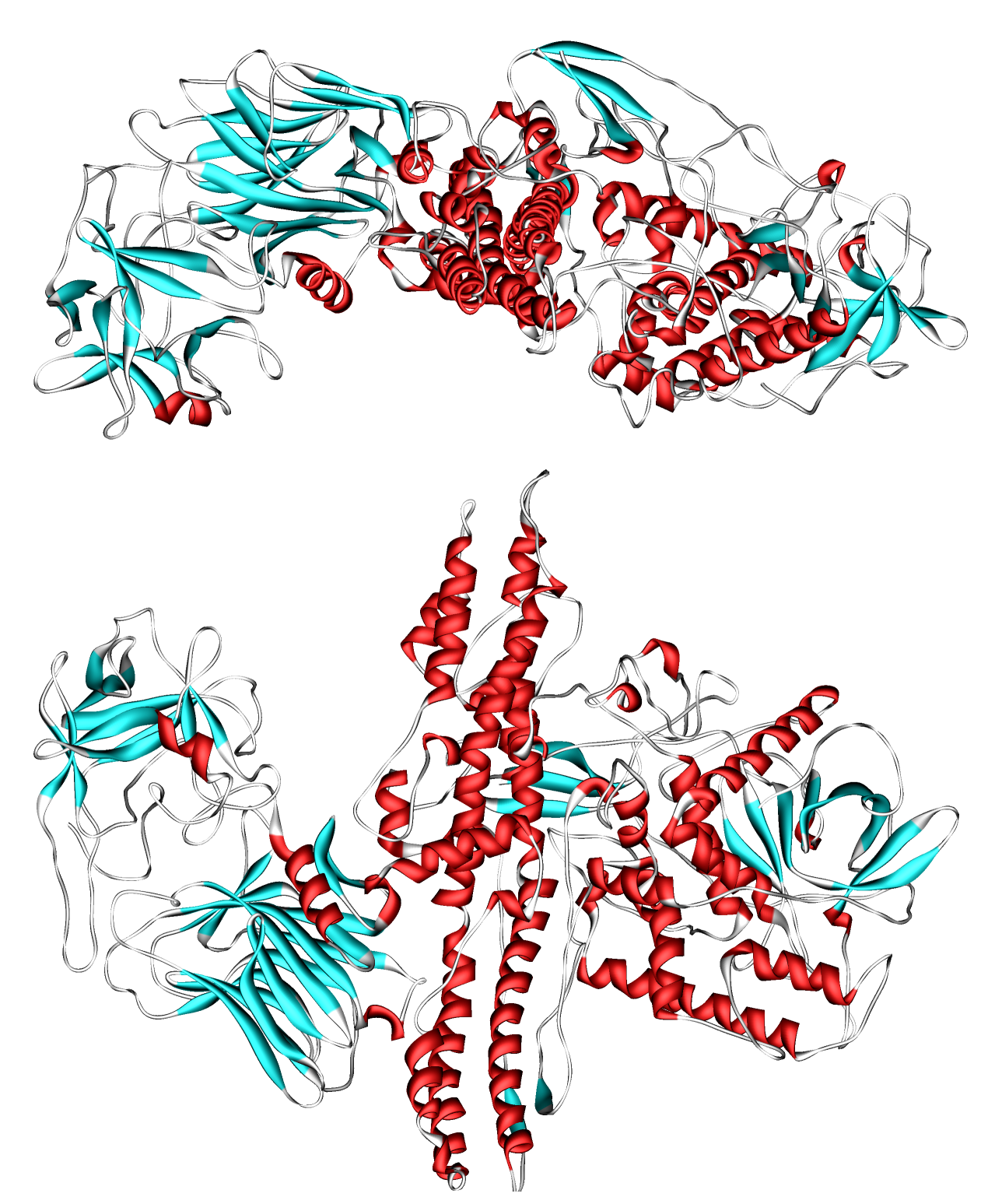
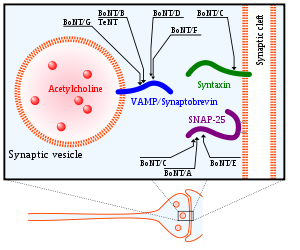 Target molecules of botulinum (BoNT) and tetanus (TeNT) toxins inside the axon terminal.[2]
Target molecules of botulinum (BoNT) and tetanus (TeNT) toxins inside the axon terminal.[2]
The heavy chain of the toxin is particularly important for targeting the toxin to specific types of axon terminals. The toxin must get inside the axon terminals in order to cause paralysis. Following the attachment of the toxin heavy chain to proteins on the surface of axon terminals, the toxin can be taken into neurons by endocytosis. The light chain is able to cleave endocytotic vesicles and reach the cytoplasm. The light chain of the toxin has protease activity. The type A toxin proteolytically degrades the SNAP-25 protein, a type of SNARE protein. The SNAP-25 protein is required for vesicle fusion that releases neurotransmitters from the axon endings (in particular Acetylcholine).[62] Botulinum toxin specifically cleaves these SNAREs, and so prevents neuro-secretory vesicles from docking/fusing with the nerve synapse plasma membrane and releasing their neurotransmitters.
Though it affects the nervous system, common nerve agent treatments (namely the injection of atropine and 2-pam-chloride) will increase mortality by enhancing botulin toxin's mechanism of toxicity[citation needed]. Attacks involving botulinum toxin are distinguishable from those involving nerve agent in that NBC detection equipment (such as M-8 paper or the ICAM) will not indicate a "positive" when a sample of the agent is tested. Furthermore, botulism symptoms develop relatively slowly, over several days compared to nerve agent effects, which can be instantaneous.
Treatment of botulinum poisoning
If the symptoms of botulism are diagnosed early, an equine antitoxin, use of enemas, and extracorporeal removal of the gut contents can be used to treat the food-borne illness. Wound infections can be treated surgically. Information regarding methods of safe canning, and public education about the disease are methods of prevention. Tests to detect botulism include a brain scan, nerve conduction test, and a tensilon test for myasthenia gravis in order to differentiate botulism from other diseases that manifest in the same way. Electromyography (EMG) can be utilized to differentiate myasthenia gravis and Guillain-Barré syndrome, diseases that botulism often mimics. Toxicity testing of serum specimens, wound tissue cultures, and toxicity testing, and stool specimen cultures are the best methods for idientifying botulism. Laboratory tests of the patient's serum or stool, which are then injected into mice are also indicative of botulism.[63] But the faster way to detect botulinum toxin in people is using the mass spectrometry technology because it reduces testing time to three or four hours and at the same time it can identify the seven types of the toxin.[64]
The case fatality rate for botulinum poisoning between 1950 and 1996 was 15.5%, down from approximately 60% over the previous 50 years.[65] Death is generally secondary to respiratory failure due to paralysis of the respiratory muscles, so treatment consists of antitoxin administration and artificial ventilation until the neurotoxins are excreted or metabolised. If initiated on time these treatments are quite effective, although antisera can not affect BoNT polypeptides that have already entered cells.[66] Occasionally, functional recovery may take several weeks to months or more.
There are two primary Botulinum Antitoxins available for treatment of botulism.
- Trivalent (A,B,E) Botulinum Antitoxin is derived from equine sources utilizing whole antibodies (Fab & Fc portions). This antitoxin is available from the local health department via the CDC in the USA.
- The second antitoxin is Heptavalent (A,B,C,D,E,F,G) Botulinum Antitoxin, which is derived from "despeciated" equine IgG antibodies, which have had the Fc portion cleaved off leaving the F(ab')2 portions. This is a less immunogenic antitoxin that is effective against all known strains of botulism where not contraindicated. This is available from the United States Army. On June 1, 2006 the United States Department of Health and Human Services awarded a $363 million contract with Cangene Corporation for 200,000 doses of Heptavalent Botulinum Antitoxin over five years for delivery into the Strategic National Stockpile beginning in 2007.[67]
Manufacturers
In the United States, BOTOX is manufactured by Allergan, Inc. for both therapeutic and cosmetic use (100Unit). In the United States, Xeomin (manufactured in Germany by Merz) is available for both therapeutic and cosmetic use.
Dysport, a therapeutic formulation of the type A toxin developed and manufactured in Ireland, is licensed for the treatment of focal dystonias and certain cosmetic uses in the US and worldwide in 100, 300 and 500 Units. Lanzhou Institute (China) manufactures a BTX-A product, producing 50U and 100U type A toxin.[68] Neuronox, a BTX-A product, was introduced by Medy-Tox Inc. of South Korea, in 2009.[69] Merz manufactures the toxin and sells it under the trade name Xeomin. Solstice Neurosciences sells their product under the names Myobloc or Neurobloc, although it contains Botulinum Toxin Type B, not the common Type A found in Botox.
See also
References
- ^ Montecucco C, Molgó J (2005). "Botulinal neurotoxins: revival of an old killer". Current opinion in pharmacology 5 (3): 274–279. doi:10.1016/j.coph.2004.12.006. PMID 15907915.
- ^ Kukreja R, Singh BR (2009). "Botulinum Neurotoxins: Structure and Mechanism of Action". Microbial Toxins: Current Research and Future Trends. Caister Academic Press. ISBN 978-1-904455-44-8.
- ^ a b Arnon, Stephen S.; Schechter R, Inglesby TV, Henderson DA, Bartlett JG, Ascher MS, Eitzen E, Fine AD, Hauer J, Layton M, Lillibridge S, Osterholm MT, O'Toole T, Parker G, Perl TM, Russell PK, Swerdlow DL, Tonat K; Working Group on Civilian Biodefense. (21 February 2001). "Botulinum Toxin as a Biological Weapon: Medical and Public Health Management" (PDF, 0.5 MB). Journal of the American Medical Association 285 (8): 1059–1070. doi:10.1001/jama.285.8.1059. PMID 11209178. http://jama.ama-assn.org/cgi/reprint/285/8/1059.pdf.
- ^ Frank J. Erbguth (2004). "Historical notes on botulism, Clostridium botulinum, botulinum toxin, and the idea of the therapeutic use of the toxin". Movement Disorders (John Wiley & Sons on behalf of the Movement Disorder Society) 19 (S8): S2–S6. doi:10.1002/mds.20003. PMID 15027048.
- ^ van Ermengem, E.P. (February 1897). "Ueber einen neuen anaëroben Bacillus und seine Beziehungen zum Botulismus" (in German). Zeitschrift für Hygiene und Infektionskrankheiten 26 (1): 1–56. doi:10.1007/BF02220526. PMID 399378.
- ^ Snipe, P. Tessmer & Sommer, H. (August 1928). "Studies on Botulinus Toxin: 3. Acid Precipitation of Botulinus Toxin". The Journal of Infectious Diseases (University of Chicago Press) 43 (2): 152–160. doi:10.1093/infdis/43.2.152. ISSN 0022-1899. JSTOR 30083772.
- ^ A. S. V. Burgen, F. Dickens, and L. J. Zatman (August 1949). "The action of botulinum toxin on the neuro-muscular junction". The Journal of Physiology (University of Chicago Press) 109 (1–2): 10–24. PMC 1392572. PMID 15394302. http://www.jphysiol.org/cgi/pmidlookup?view=long&pmid=15394302.
- ^ Dressler D (August 2006). "Pharmakologische Aspekte therapeutischer Botulinum-Toxin-Präparationen [Pharmacological aspects of therapeutic botulinum toxin preparations]" (in German). Der Nervenarzt 77 (8): 912–21. doi:10.1007/s00115-006-2090-2. ISSN 0028-2804. PMID 16810528.
- ^ Scott AB, Pasricha, PJ. Ravich WJ, Kalloo AN (January 1993). "Botulinum toxin for achalasia". Lancet 341 (8839): 244–5.. doi:10.1016/0140-6736(93)90109-T. PMID 8093528. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=8093528.
- ^ a b Bushara KO, Park DM. (November 1994). "Botulinum toxin and sweating". Journal of Neurology, Neurosurgery, and Psychiatry 57 (11): 1437–1438. doi:10.1136/jnnp.57.11.1437. ISSN 0022-3050. PMC 1073208. PMID 7964832. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1073208.
- ^ Flanders M, Tischler A, Wise J, Williams F, Beneish R, Auger N. (June 1987). "Injection of type A Botulinum toxin into extraocular muscles for correction of strabismus". Canadian Journal of Ophthalmology 22 (4): 212–217. ISSN 1715-3360. PMID 3607594.
- ^ Scott AB (September 1989). "Botulinum toxin therapy of eye muscle disorders: safety and effectiveness. Ophthalmic Procedures Assessment Recommendation". Ophthalmology (American Academy of Ophthalmology) Suppl: Suppl:37–41.. PMID 2779991.
- ^ Boffey, Philip M. (October 14, 1986). "Loss Of Drug Relegates Many To Blindness Again". The New York Times. http://www.nytimes.com/1986/10/14/science/loss-of-drug-relegates-many-to-blindness-again.html. Retrieved 2010-07-14.
- ^ United States Department of Health and Human Services (April 30, 2009). "Re: Docket No. FDA-2008-P-0061" (PDF, 8.2 MB). Food and Drug Administration. http://www.fda.gov/downloads/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/UCM143989.pdf. Retrieved 2010-07-26.
- ^ Clark RP, Berris CE. (August 1989). "Botulinum Toxin: A treatment for facial asymmetry caused by facial nerve paralysis". Plastic and Reconstructive Surgery 84 (2): 353–355. doi:10.1097/01.prs.0000205566.47797.8d. ISSN 0032-1052. PMID 2748749.
- ^ Carruthers JD, Carruthers JA. (January 1992). "Treatment of Glabellar Frown Lines with C. Botulinum-A Exotoxin". The Journal of Dermatologic Surgery and Oncology 18 (1): 17–21. doi:10.1111/j.1524-4725.1992.tb03295.x. PMID 1740562.
- ^ "Botulinum Toxin Type A Product Approval Information - Licensing Action 4/12/02". Food and Drug Administration. Page last updated 29 October 2009. http://www.fda.gov/Drugs/DevelopmentApprovalProcess/HowDrugsareDevelopedandApproved/ApprovalApplications/TherapeuticBiologicApplications/ucm080509.htm. Retrieved 2010-07-26.
- ^ Botox Cosmetic Information
- ^ "Allergan Receives FDA Approval for First-of-Its-Kind, Fully in vitro, Cell-Based Assay for BOTOX® and BOTOX® Cosmetic (onabotulinumtoxinA)". Source: Allergan, Inc. News Provided by Acquire Media. Page last updated 24 June 2011. http://agn.client.shareholder.com/releasedetail.cfm?ReleaseID=587234. Retrieved 2011-06-26.
- ^ "In U.S., Few Alternatives To Testing On Animals". Washington Post. Page last updated 12 April 2008. http://www.washingtonpost.com/wp-dyn/content/article/2008/04/11/AR2008041103733.html. Retrieved 2011-06-26.
- ^ "Botox injections get Australian man out of wheelchair". Meeja.com.au. June 8, 2009. http://www.meeja.com.au/articles/botox-injections-get-australian-man-out-of-wheelchair. Retrieved 2010-07-14.
- ^ Walsh, Sandy (October 15, 2010). "FDA approves Botox to treat chronic migraine". FDA Press Releases. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm229782.htm. Retrieved 2010-10-15.
- ^ Dodick, DW; Turkel, CC, DeGryse, RE, Aurora, SK, Silberstein, SD, Lipton, RB, Diener, HC, Brin, MF, PREEMPT Chronic Migraine Study, Group (2010 Jun). "OnabotulinumtoxinA for treatment of chronic migraine: pooled results from the double-blind, randomized, placebo-controlled phases of the PREEMPT clinical program". Headache 50 (6): 921–36. doi:10.1111/j.1526-4610.2010.01678.x. PMID 20487038.
- ^ Ashkenazi, A (2010 Mar). "Botulinum toxin type a for chronic migraine". Current neurology and neuroscience reports 10 (2): 140–6. doi:10.1007/s11910-010-0087-5. PMID 20425239.
- ^ Irving, William; Boswell, Tim; Dlawer, Ala'Aldeen (2005). "Section C: Human pathogens: bacteria; C14: Clostridia". Instant Notes: Medical Microbiology. New York: Taylor & Francis. p. 160. ISBN 978-1859962541. http://books.google.com/?id=pg9HinBo-4cC.
- ^ Schantz EJ, Johnson EA. (March 1992). "Properties and use of botulinum toxin and other microbial neurotoxins in medicine". Microbiological Reviews 56 (1): 80–99. ISSN 1092-2172. PMC 372855. PMID 1579114. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=372855.
- ^ http://www.cdc.gov/nczved/divisions/dfbmd/diseases/botulism/
- ^ "Emergency preparedness: Botulism". Physician Information Link. Anne Arundel County Department of Health. June 17, 2004. http://www.aahealth.org/physicianslink/bioterrorism_botulism_overview.asp. Retrieved 2010-07-14.
- ^ Licciardello JJ, Nickerson JT, Ribich CA, Goldblith SA. (March 1967). "Thermal Inactivation of Type E Botulinum Toxin". Applied Microbiology 15 (2): 249–256. ISSN 0003-6919. PMC 546888. PMID 5339838. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=546888.
- ^ Setlowa, Peter (April 2007). "I will survive: DNA protection in bacterial spores". Trends in Microbiology 15 (4): 172–180. doi:10.1016/j.tim.2007.02.004. ISSN 0966-842X. PMID 17336071.
- ^ Koirala, Janak; Basnet, Sangita (14 July 2004). "Botulism, Botulinum Toxin, and Bioterrorism: Review and Update". Medscape. Cliggott Publishing. http://www.medscape.com/viewarticle/482812. Retrieved 2010-07-14.
- ^ Barbano, Richard (8 November 2006). "Risks of erasing wrinkles: Buyer beware!". Neurology 67 (10): E17–E18. doi:10.1212/01.wnl.0000250411.93526.9e. PMID 17130399. http://www.neurology.org/cgi/content/full/67/10/E17.
- ^ Mr Michael Edwards FRCSEng FRCSEd. Consultant general surgeon. (2006). "Anal fissure". Dumas Ltd. http://www.privatehealth.co.uk/private-operations/general-surgery/anal-fissure/. Retrieved 2010-08-21.
- ^ a b c d e f Markus, Ramsey (September 30, 2009). "Botox for Wrinkles". Baylor College of Medicine. http://www.bcm.edu/dermatology/?PMID=1909. Retrieved 2010-07-14.
- ^ a b "How long does Botox last?". RealSelf. RealSelf, Inc.. http://www.realself.com/question/how-long-does-botox-last. Retrieved 2010-07-14.
- ^ Bihari K (March 2005). "Safety, effectiveness, and duration of effect of BOTOX after switching from Dysport for blepharospasm, cervical dystonia, and hemifacial spasm dystonia, and hemifacial spasm". Current Medical Research and Opinion 21 (3): 433–438. doi:10.1185/030079905X36396. ISSN 0300-7995. PMID 15811212.
- ^ Brin MF, Lew MF, Adler CH, Comella CL, Factor SA, Jankovic J, O'Brien C, Murray JJ, Wallace JD, Willmer-Hulme A, Koller M (22 October 1999). "Safety and efficacy of NeuroBloc (botulinum toxin type B) in type A-resistant cervical dystonia". Neurology 53 (7): 1431–1438. ISSN 0028-3878. PMID 10534247.
- ^ Shukla HD, Sharma SK (2005). "Clostridium botulinum: a bug with beauty and weapon". Critical Reviews in Microbiology 31 (1): 11–18. doi:10.1080/10408410590912952. ISSN 1040-841X. PMID 15839401.
- ^ Eisenach JH, Atkinson JL, Fealey RD. (May 2005). "Hyperhidrosis: evolving therapies for a well-established phenomenon". Mayo Clinic Proceedings 80 (5): 657–666. doi:10.4065/80.5.657. ISSN 0025-6196. PMID 15887434.
- ^ Ranoux D, Attal N, Morain F, Bouhassira D (September 2008). "Botulinum toxin type A induces direct analgesic effects in chronic neuropathic pain". Annals of neurology 64 (3): 274–83. doi:10.1002/ana.21427. PMID 18546285.
- ^ Naumann M, So Y, Argoff CE, et al. (May 2008). "Assessment: Botulinum neurotoxin in the treatment of autonomic disorders and pain (an evidence-based review): report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology". Neurology 70 (19): 1707–14. doi:10.1212/01.wnl.0000311390.87642.d8. PMID 18458231. http://www.neurology.org/cgi/pmidlookup?view=long&pmid=18458231.
- ^ Celibre Medical "Botox Injections for Excessive Sweating", Celibre.com, referenced October 17, 2011.
- ^ a b c Mangera A, Andersson KE, Apostolidis A, Chapple C, Dasgupta P, Giannantoni A, Gravas S, Madersbacher S. (2005). "Contemporary management of lower urinary tract disease with botulinum toxin A: a systematic review of botox (onabotulinumtoxinA) and dysport (abobotulinumtoxinA).". European Urology 60 (4): 784–95. PMID 21782318. http://www.ncbi.nlm.nih.gov/pubmed/21782318.
- ^ Schurch B, Corcos J (2005). "Botulinum toxin injections for paediatric incontinence". Current opinion in urology 15 (4): 264–7. doi:10.1097/01.mou.0000172401.92761.86. PMID 15928517.
- ^ Duthie J, Wilson D, Herbison G, Wilson D (2007). Duthie, James B. ed. "Botulinum toxin injections for adults with overactive bladder syndrome". Cochrane database of systematic reviews (Online) 3 (3): CD005493. doi:10.1002/14651858.CD005493.pub2. PMID 17636801.
- ^ Akbar M, Abel R, Seyler TM, Gerner HJ, Möhring K (2007). "Repeated botulinum-A toxin injections in the treatment of myelodysplastic children and patients with spinal cord injuries with neurogenic bladder dysfunction". BJU Int. 100 (3): 639–45. doi:10.1111/j.1464-410X.2007.06977.x. PMID 17532858.
- ^ Trzciński R, Dziki A, Tchórzewski M (2002). "Injections of botulinum A toxin for the treatment of anal fissures". The European journal of surgery = Acta chirurgica 168 (12): 720–3. PMID 15362583.
- ^ Pacik, PT Botox Treatment for Vaginismus Plast Reconst Surg vol 124: 455e-456e Dec. 2009
- ^ Panicker JN, Muthane UB (2003). "Botulinum toxins: pharmacology and its current therapeutic evidence for use". Neurology India 51 (4): 455–60. PMID 14742921. http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=455;epage=460;aulast=Muthane.
- ^ Charles PD (2004). "Botulinum neurotoxin serotype A: a clinical update on non-cosmetic uses". American journal of health-system pharmacy : AJHP : official journal of the American Society of Health-System Pharmacists 61 (22 Suppl 6): S11–23. PMID 15598005.
- ^ Coskun H, Duran Y, Dilege E, Mihmanli M, Seymen H, Demirkol MO (2005). "Effect on gastric emptying and weight reduction of botulinum toxin-A injection into the gastric antral layer: an experimental study in the obese rat model". Obesity surgery : the official journal of the American Society for Bariatric Surgery and of the Obesity Surgery Society of Australia and New Zealand 15 (8): 1137–43. doi:10.1381/0960892055002275. PMID 16197786.
- ^ a b c Coté TR, Mohan AK, Polder JA, Walton MK, Braun MM (September 2005). "Botulinum toxin type A injections: adverse events reported to the US Food and Drug Administration in therapeutic and cosmetic cases". J. Am. Acad. Dermatol. 53 (3): 407–15. doi:10.1016/j.jaad.2005.06.011. PMID 16112345.
- ^ FDA Notifies Public of Adverse Reactions Linked to Botox Use
- ^ FDA Gives Update on Botulinum Toxin Safety Warnings; Established Names of Drugs Changed, FDA Press Announcement, August 3, 2009
- ^ "Botox chemical may spread, Health Canada confirms". CBC News. 2009-01-13. http://www.cbc.ca/consumer/story/2009/01/13/botox.html.
- ^ Le Canada met en garde contre les effets dangereux du Botox (French)
- ^ Woman Dies From Fake Botox Injections
- ^ [1]
- ^ Botox Side Effects
- ^ HRG Publication #1834): Public Citizen
- ^ "Botox May Deaden Ability to Empathize, New Study Says". Forbes. Apr. 23, 2011. http://blogs.forbes.com/marcbabej/2011/04/23/botox-may-deaden-ability-to-empathize-new-study-says/?partner=following_topic_daily.
- ^ Foran PG, Mohammed N, Lisk GO, et al. (2003). "Evaluation of the therapeutic usefulness of botulinum neurotoxin B, C1, E, and F compared with the long lasting type A. Basis for distinct durations of inhibition of exocytosis in central neurons". J. Biol. Chem. 278 (2): 1363–71. doi:10.1074/jbc.M209821200. PMID 12381720. http://www.jbc.org/cgi/content/full/278/2/1363.
- ^ "Disease Listing, Botulism Manual, Additional Information". CDC Bacterial, Mycotic Diseases. http://www.cdc.gov/ncidod/dbmd/diseaseinfo/files/botulism_manual.htm. Retrieved 2010-01-21.
- ^ * www.cdc.gov/washington/cdcatWork/pdf/botulinum.pdf
- ^ "Disease Listing, Botulism Manual, Additional Information - CDC Bacterial, Mycotic Diseases". http://www.cdc.gov/ncidod/dbmd/diseaseinfo/files/botulism_manual.htm. Retrieved 2007-08-14.
- ^ Turton K., Chaddock J. A., Acharya K. R. (2002). "Botulinum and tetanus neurotoxins: structure, function and therapeutic utility". Trends in Biochemical Sciences 27 (11): 552–558. doi:10.1016/S0968-0004(02)02177-1. PMID 12417130.
- ^ "FEMA". Archived from the original on 2007-09-29. http://web.archive.org/web/20070929111841/http://mmrs.fema.gov/news/publichealth/2006/aug/nph2006-08-03a.aspx. Retrieved 2007-08-14.
- ^ "Botulinum Toxin Type A". Hugh Source (International) Limited. http://btxa.com/product_quality/index.htm#1_1. Retrieved 2010-07-14.
- ^ Petrou, Ilya (Spring 2009). "Medy-Tox Introduces Neuronox to the Botulinum Toxin Arena" (PDF). The European Aesthetic Guide. http://www.miinews.com/pdf/MedyTox_Ed_EAGsp09v2_022809.pdf.
External links
- A Poison that can Heal from the U.S. Food and Drug Administration
- Does Botox get into the brain? Troubling research contradicts earlier findings about the treatment
- Government backs vital plans to make Botox safer
- BotDB: extensive resources on BoNT structures, inhibitors, kinetics, and literature
- Medical publication on botulinum toxins
Skeletal muscle relaxants (M03) Peripherally acting
(primarily antinicotinic,
NMJ block)Curare alkaloidsultra-short duration: Gantacurium
short duration: Mivacurium • Chandonium
intermediate duration: Atracurium • Cisatracurium • Fazadinium • Rocuronium • Vecuronium
long duration: Doxacurium • Dimethyltubocurarine • Pancuronium • Pipecuronium • Laudexium • Gallamine
unsorted: Hexafluronium (Hexafluorenium)Choline derivatives: Suxamethonium (Succinylcholine)
Polyalkylene derivatives: HexamethoniumBotulinum toxinCentrally acting Carbamic acid estersBenzodiazepinesAnticholinergics (Antimuscarinics)OtherBaclofen • Chlormezanone • Chlorphenesin • Chlorzoxazone • Donepezil • Eperisone • Flopropione • Mephenesin • Mephenoxalone • Metaxalone • Phenyramidol • Pridinol • Promoxolane • Quinine • Thiocolchicoside • Tizanidine • Tolperisone • TrazodoneDirectly acting Cholinergics Receptor ligands Agonists: 77-LH-28-1 • AC-42 • AC-260,584 • Aceclidine • Acetylcholine • AF30 • AF150(S) • AF267B • AFDX-384 • Alvameline • AQRA-741 • Arecoline • Bethanechol • Butyrylcholine • Carbachol • CDD-0034 • CDD-0078 • CDD-0097 • CDD-0098 • CDD-0102 • Cevimeline • cis-Dioxolane • Ethoxysebacylcholine • LY-593,039 • L-689,660 • LY-2,033,298 • McNA343 • Methacholine • Milameline • Muscarine • NGX-267 • Ocvimeline • Oxotremorine • PD-151,832 • Pilocarpine • RS86 • Sabcomeline • SDZ 210-086 • Sebacylcholine • Suberylcholine • Talsaclidine • Tazomeline • Thiopilocarpine • Vedaclidine • VU-0029767 • VU-0090157 • VU-0152099 • VU-0152100 • VU-0238429 • WAY-132,983 • Xanomeline • YM-796
Antagonists: 3-Quinuclidinyl Benzilate • 4-DAMP • Aclidinium Bromide • Anisodamine • Anisodine • Atropine • Atropine Methonitrate • Benactyzine • Benzatropine (Benztropine) • Benzydamine • BIBN 99 • Biperiden • Bornaprine • CAR-226,086 • CAR-301,060 • CAR-302,196 • CAR-302,282 • CAR-302,368 • CAR-302,537 • CAR-302,668 • CS-27349 • Cyclobenzaprine • Cyclopentolate • Darifenacin • DAU-5884 • Dimethindene • Dexetimide • DIBD • Dicyclomine (Dicycloverine) • Ditran • EA-3167 • EA-3443 • EA-3580 • EA-3834 • Elemicin • Etanautine • Etybenzatropine (Ethylbenztropine) • Flavoxate • Himbacine • HL-031,120 • Ipratropium bromide • J-104,129 • Hyoscyamine • Mamba Toxin 3 • Mamba Toxin 7 • Mazaticol • Mebeverine • Methoctramine • Metixene • Myristicin • N-Ethyl-3-Piperidyl Benzilate • N-Methyl-3-Piperidyl Benzilate • Orphenadrine • Otenzepad • Oxybutynin • PBID • PD-102,807 • PD-0298029 • Phenglutarimide • Phenyltoloxamine • Pirenzepine • Piroheptine • Procyclidine • Profenamine • RU-47,213 • SCH-57,790 • SCH-72,788 • SCH-217,443 • Scopolamine (Hyoscine) • Solifenacin • Telenzepine • Tiotropium bromide • Tolterodine • Trihexyphenidyl • Tripitamine • Tropatepine • Tropicamide • WIN-2299 • Xanomeline • Zamifenacin; Others: 1st Generation Antihistamines (Brompheniramine, chlorphenamine, cyproheptadine, dimenhydrinate, diphenhydramine, doxylamine, mepyramine/pyrilamine, phenindamine, pheniramine, tripelennamine, triprolidine, etc) • Tricyclic Antidepressants (Amitriptyline, doxepin, trimipramine, etc) • Tetracyclic Antidepressants (Amoxapine, maprotiline, etc) • Typical Antipsychotics (Chlorpromazine, thioridazine, etc) • Atypical Antipsychotics (Clozapine, olanzapine, quetiapine, etc)Agonists: 5-HIAA • A-84,543 • A-366,833 • A-582,941 • A-867,744 • ABT-202 • ABT-418 • ABT-560 • ABT-894 • Acetylcholine • Altinicline • Anabasine • Anatoxin-a • AR-R17779 • Butyrylcholine • Carbachol • Cotinine • Cytisine • Decamethonium • Desformylflustrabromine • Dianicline • Dimethylphenylpiperazinium • Epibatidine • Epiboxidine • Ethanol • Ethoxysebacylcholine • EVP-4473 • EVP-6124 • Galantamine • GTS-21 • Ispronicline • Lobeline • MEM-63,908 (RG-3487) • Nicotine • NS-1738 • PHA-543,613 • PHA-709,829 • PNU-120,596 • PNU-282,987 • Pozanicline • Rivanicline • Sazetidine A • Sebacylcholine • SIB-1508Y • SIB-1553A • SSR-180,711 • Suberylcholine • TC-1698 • TC-1734 • TC-1827 • TC-2216 • TC-5214 • TC-5619 • TC-6683 • Tebanicline • Tropisetron • UB-165 • Varenicline • WAY-317,538 • XY-4083
Antagonists: 18-Methoxycoronaridine • α-Bungarotoxin • α-Conotoxin • Alcuronium • Amantadine • Anatruxonium • Atracurium • Bupropion (Amfebutamone) • Chandonium • Chlorisondamine • Cisatracurium • Coclaurine • Coronaridine • Dacuronium • Decamethonium • Dextromethorphan • Dextropropoxyphene • Dextrorphan • Diadonium • DHβE • Dimethyltubocurarine (Metocurine) • Dipyrandium • Dizocilpine (MK-801) • Doxacurium • Duador • Esketamine • Fazadinium • Gallamine • Hexafluronium • Hexamethonium (Benzohexonium) • Ibogaine • Isoflurane • Ketamine • Kynurenic acid • Laudexium (Laudolissin) • Levacetylmethadol • Malouetine • Mecamylamine • Memantine • Methadone • Methorphan (Racemethorphan) • Methyllycaconitine • Metocurine • Mivacurium • Morphanol (Racemorphanol) • Neramexane • Nitrous Oxide • Pancuronium • Pempidine • Pentamine • Pentolinium • Phencyclidine • Pipecuronium • Radafaxine • Rapacuronium • Rocuronium • Surugatoxin • Suxamethonium (Succinylcholine) • Thiocolchicoside • Toxiferine • Trimethaphan • Tropeinium • Tubocurarine • Vecuronium • XenonReuptake inhibitors PlasmalemmalCHT InhibitorsHemicholinium-3 (Hemicholine; HC3) • TriethylcholineVAChT InhibitorsEnzyme inhibitors ChAT inhibitors1-(-Benzoylethyl)pyridinium • 2-(α-Naphthoyl)ethyltrimethylammonium • 3-Chloro-4-stillbazole • 4-(1-Naphthylvinyl)pyridine • Acetylseco hemicholinium-3 • Acryloylcholine • AF64A • B115 • BETA • CM-54,903 • CatabolismAChE inhibitorsReversible: Carbamates: Aldicarb • Bendiocarb • Bufencarb • Carbaryl • Carbendazim • Carbetamide • Carbofuran • Chlorbufam • Chloropropham • Ethienocarb • Ethiofencarb • Fenobucarb • Fenoxycarb • Formetanate • Furadan • Ladostigil • Methiocarb • Methomyl • Miotine • Oxamyl • Phenmedipham • Pinmicarb • Pirimicarb • Propamocarb • Propham • Propoxur; Stigmines: Ganstigmine • Neostigmine • Phenserine • Physostigmine • Pyridostigmine • Rivastigmine; Others: Acotiamide • Ambenonium • Donepezil • Edrophonium • Galantamine • Huperzine A • Minaprine • Tacrine • Zanapezil
Irreversible: Organophosphates: Acephate • Azinphos-methyl • Bensulide • Cadusafos • Chlorethoxyfos • Chlorfenvinphos • Chlorpyrifos • Chlorpyrifos-Methyl • Coumaphos • Cyclosarin (GF) • Demeton • Demeton-S-Methyl • Diazinon • Dichlorvos • Dicrotophos • Diisopropyl fluorophosphate (Guthion) • Diisopropylphosphate • Dimethoate • Dioxathion • Disulfoton • EA-3148 • Echothiophate • Ethion • Ethoprop • Fenamiphos • Fenitrothion • Fenthion • Fosthiazate • GV • Isofluorophate • Isoxathion • Malaoxon • Malathion • Methamidophos • Methidathion • Metrifonate • Mevinphos • Monocrotophos • Naled • Novichok agent • Omethoate • Oxydemeton-Methyl • Paraoxon • Parathion • Parathion-Methyl • Phorate • Phosalone • Phosmet • Phostebupirim • Phoxim • Pirimiphos-Methyl • Sarin (GB) • Soman (GD) • Tabun (GA) • Temefos • Terbufos • Tetrachlorvinphos • Tribufos • Trichlorfon • VE • VG • VM • VR • VX; Others: Demecarium • Onchidal (Onchidella binneyi)BChE inhibitorsCymserine * Many of the acetylcholinesterase inhibitors listed above act as butyrylcholinesterase inhibitors.Others Choline (Lecithin) • Citicoline • Cyprodenate • Dimethylethanolamine (DMAE, deanol) • Glycerophosphocholine • Meclofenoxate (Centrophenoxine) • Phosphatidylcholine • Phosphatidylethanolamine • Phosphorylcholine • PirisudanolOthersAcetylcholine releasing agents: α-Latrotoxin • β-Bungarotoxin; Acetylcholine release inhibitors: Botulinum toxin (Botox); Acetylcholinesterase reactivators: Asoxime • Obidoxime • PralidoximeContemporary Western cosmetics and plastic surgery Face Concealer · Foundation · Powder · Rouge · Primer · Veil · Cleanser · Toner · Moisturizer · Anti-aging cream · Botox · Facial · Bleaching · Facial toning · Permanent makeupLips Eyes Hair Nails Body Related topics Major cosmetic brands Ahava · Almay · Artistry · Aveda · Avon · Bath & Body Works · Benefit · Biotherm · Bobbi Brown · The Body Shop · Bonne Bell · Bumble and bumble · Burt's Bees · Cargo · Carol's Daughter · Clarins · Clinique · Coty · CoverGirl · Creme 21 · Daigaku Honyaku Center · Dr. Hauschka · Eden Allure · Elizabeth Arden · Estée Lauder · Eyes Lips Face · Fabergé · Hard Candy · Helena Rubinstein · Kanebo Ltd. · Kao Corporation · Kevyn Aucoin · Kiehl's · La Mer · Lancôme · Laneige · Laura Mercier · Laura Mercier Cosmetics · Lise Watier · L'Oréal · L'occitane · Love Cosmetics · Lush · MAC Cosmetics · Mary Kay · Max Factor · Maybelline · ModelCo · NARS · Natura · Natural Wonder · Neal's Yard Remedies · Neutrogena · Nexxus · Nivea · O Boticário · Oriflame · Origins · Paula Begoun · Red Earth · Revlon · Richard Hudnut · Rimmel · Sephora · Shiseido · Shu Uemura · SK-II · SkinCeuticals · Stila · Ulta · Ultima II · Urban Decay · Vichy · Victoria's Secret · Vie at Home · Wella · Yves RocherCategories Categories:- Biological toxin weapons
- Muscle relaxants
- Neurotoxins
- Plastic surgery
- Bacterial toxins
Wikimedia Foundation. 2010.
Look at other dictionaries:
botulinum toxin — also botulinus toxin n a very powerful bacterial neurotoxin that acts primarily on the parasympathetic nervous system, is produced by botulinum, blocks release of acetylcholine at the neuromuscular junction, and causes botulism often used with… … Medical dictionary
Botulinum-Toxin — Botulinumtoxin Serotyp A (Clostridium botulinum) Bändermodell nach … Deutsch Wikipedia
botulinum toxin — noun any of several neurotoxins that are produced by the anaerobic bacterium Clostridium botulinum; causes muscle paralysis • Hypernyms: ↑neurotoxin, ↑neurolysin • Hyponyms: ↑botulinum toxin A, ↑Botox … Useful english dictionary
botulinum toxin A — noun a neurotoxin (trade name Botox) that is used clinically in small quantities to treat strabismus and facial spasms and other neurological disorders characterized by abnormal muscle contractions; is also used by cosmetic surgeons to smooth… … Useful english dictionary
botulinum toxin type A — n a purified botulinum toxin of high molecular weight that is used by injection esp. to treat strabismus, blepharospasm, spasmodic torticollis, and severe axillary hyperhidrosis and in cosmetic dermatology and plastic surgery to minimize wrinkles … Medical dictionary
botulinum toxin — toxin that causes the potentially fatal disease botulism and is found in spoiled food (created by the bacteria Clostridium botulinum which is used in biological weapons and in very small doses to treat muscular disorders) … English contemporary dictionary
botulinum toxin — Neurotoxin (50 kD; 7 distinct serotypes) produced by certain strains of Clostridium botulinum. The bacterium produces the toxin as a complex with a haemagglutinin that prevents toxin inactivation in the gut. Proteolysis in the body results in… … Dictionary of molecular biology
botulinum toxin — noun Date: 1928 a neurotoxin formed by botulinum that causes botulism and that is injected in a purified form for therapeutic and cosmetic purposes (as to treat blepharospasm and reduce wrinkles) … New Collegiate Dictionary
Botulinum toxin — noun a neurotoxic protein produced by the bacterium Clostridium botulinum Syn: botulin … Wiktionary
botulinum toxin — [ˌbɒtjʊ lʌɪnəm] (also botulinus toxin) noun another term for botulin … English new terms dictionary
 18+© Academic, 2000-2026
18+© Academic, 2000-2026- Contact us: Technical Support, Advertising
Dictionaries export, created on PHP, Joomla, Drupal, WordPress, MODx.