- Migraine
-
Migraine Classification and external resources 
The pain of a migraine headache can be debilitating.ICD-10 G43 ICD-9 346 OMIM 157300 DiseasesDB 8207 (Migraine)
31876 (Basilar)
4693 (FHM)MedlinePlus 000709 eMedicine neuro/218 neuro/517 emerg/230 neuro/529 MeSH D008881 Migraine (from the Greek words hemi, meaning half, and kranion, meaning skull[1]) is a chronic neurological disorder characterized by moderate to severe headaches, and nausea. It is about three times more common in women than in men.[2]
The typical migraine headache is unilateral (affecting one half of the head) and pulsating in nature and lasting from four to 72 hours; symptoms include nausea, vomiting, photophobia (increased sensitivity to light) and phonophobia (increased sensitivity to sound); the symptoms are generally aggravated by routine activity.[3][4] Approximately one-third of people who suffer from migraine headaches perceive an aura—transient visual, sensory, language, or motor disturbances signalling the migraine will soon occur.[5][6]
Initial treatment is with analgesics for the headache, an antiemetic for the nausea, and the avoidance of triggers. The cause of migraine headache is unknown; the most supported theory is that it is related to hyperexcitability of the cerebral cortex and/or abnormal control of pain neurons in the trigeminal nucleus of the brainstem.[7]
Studies of twins indicate a 60- to 65-percent genetic influence upon their propensity to develop migraine headaches.[8][9] Moreover, fluctuating hormone levels indicate a migraine relation: 75 percent of adult patients are women, although migraine affects approximately equal numbers of prepubescent boys and girls. Propensity to migraine headache sometimes disappears during pregnancy, but in some women, migraines may become more frequent.[10]
Contents
Classification
Main article: ICHD classification and diagnosis of migraineThe International Headache Society (IHS) offers guidelines for the classification and diagnosis of migraine headaches, in a document called "The International Classification of Headache Disorders, 2nd edition" (ICHD-2).[3] These guidelines constitute arbitrary definitions, and are not supported by scientific data.[3]
According to ICHD-2, there are seven subclasses of migraines (some of which include further subdivisions):
- Migraine without aura, or common migraine, involves migraine headaches that are not accompanied by an aura (visual disturbance, see below).
- Migraine with aura usually involves migraine headaches accompanied by an aura. Less commonly, an aura can occur without a headache, or with a nonmigraine headache. Two other varieties are familial hemiplegic migraine and sporadic hemiplegic migraine, in which a patient has migraines with aura and with accompanying motor weakness. If a close relative has had the same condition, it is called "familial", otherwise it is called "sporadic". Another variety is basilar-type migraine, where a headache and aura are accompanied by difficulty speaking, vertigo, ringing in ears, or a number of other brainstem-related symptoms, but not motor weakness.
- Childhood periodic syndromes that are commonly precursors of migraine include cyclical vomiting (occasional intense periods of vomiting), abdominal migraine (abdominal pain, usually accompanied by nausea), and benign paroxysmal vertigo of childhood (occasional attacks of vertigo).
- Retinal migraine involves migraine headaches accompanied by visual disturbances or even temporary blindness in one eye.
- Complications of migraine describe migraine headaches and/or auras that are unusually long or unusually frequent, or associated with a seizure or brain lesion.
- Probable migraine describes conditions that have some characteristics of migraines, but where there is not enough evidence to diagnose it as a migraine with certainty (in the presence of concurrent medication overuse).
- Chronic migraine, according to the American Headache Society[11] and the international headache society,[12] is a "complication of migraine"s and is a headache fulfilling the diagnostic criteria for "migraine headache", which occurs for a greater time interval. Specifically, greater or equal to 15 days/month for greater than 3 months.
Signs and symptoms
Migraines typically present with recurrent severe headache associated with autonomic symptoms.[13] An aura only occurs in a small percentage of people.[13] The severity of the pain, duration of the headache, and frequency of attacks is variable.[13] A migraine lasting 72 hours is termed status migrainosus and can be treated with intravenous prochlorperazine. The four possible phases to a migraine attack[3] are listed below — not all the phases are necessarily experienced. Additionally, the phases experienced and the symptoms experienced during them can vary from one migraine attack to another in the same person:
- The prodrome, which occurs hours or days before the headache
- The aura, which immediately precedes the headache
- The pain phase, also known as headache phase
- The postdrome
Prodrome
Prodromal symptoms occur in 40–60% of those with migraines. This phase may consist of altered mood, irritability, depression or euphoria, fatigue, yawning, excessive sleepiness, craving for certain food (e.g. chocolate), stiff muscles (especially in the neck), dizziness, hot ears, constipation or diarrhea, increased or decreased urination, and other visceral symptoms.[14] These symptoms usually precede the headache phase of the migraine attack by several hours or days, and experience teaches the patient or observant family how to detect a migraine attack is near.
Aura
For the 20–30%[15][16] of migraine sufferers who experience migraine with aura, this aura comprises focal neurological phenomena that precede or accompany the attack. They appear gradually over five to 20 minutes and generally last fewer than 60 minutes. The headache phase of the migraine attack usually begins within 60 minutes of the end of the aura phase, but it is sometimes delayed up to several hours, and it can be missing entirely (see silent migraine). The pain may also begin before the aura has completely subsided. Symptoms of migraine aura can be sensory or motor in nature.[17]
Visual aura is the most common of the neurological events, and can occur without any headache. There is a disturbance of vision consisting often of unformed flashes of white and/or black or rarely of multicolored lights (photopsia) or formations of dazzling zigzag lines (scintillating scotoma, often arranged like the battlements of a castle, hence the alternative terms "fortification spectra" or "teichopsia"[18]). Some patients complain of blurred or shimmering or cloudy vision, as though they were looking at an area above a heated surface, looking through thick or smoked glass, or, in some cases, tunnel vision and hemianopsia.
The somatosensory aura of migraine may consist of digitolingual or cheiro-oral paresthesias, a feeling of pins-and-needles experienced in the hand and arm, as well as in the nose-mouth area on the same side. The paresthesia may migrate up the arm and then extend to involve the face, lips and tongue.
Other symptoms of the aura phase can include auditory, gustatory or olfactory hallucinations, temporary dysphasia, vertigo, tingling or numbness of the face and extremities, and hypersensitivity to touch.
Oliver Sacks's book Migraine describes "migrainous deliria" as a result of such intense migraine aura that it is indistinguishable from "free-wheeling states of hallucinosis, illusion, or dreaming."
- Visual symptoms of migraine aura
-

Enhancements reminiscent of a zigzag fort structure
-

Negative scotoma, loss of awareness of local structures
-

Positive scotoma, local perception of additional structures
-

Mostly one-sided loss of perception
Pain
The typical migraine headache is unilateral, throbbing, and moderate to severe, and can be aggravated by physical activity.[3] Not all these features are necessary. The pain may be bilateral at the onset or start on one side and become generalized, and may occur primarily on one side or alternate sides from one attack to the next. The onset is usually gradual. The pain peaks and then subsides and usually lasts four to 72 hours in adults and one to 48 hours in children. The frequency of attacks is extremely variable, from a few in a lifetime to several a week, and the average sufferer experiences one to three headaches a month. The head pain varies greatly in intensity, and can be very severe.
The pain of migraine is invariably accompanied by other features. Nausea occurs in almost 90 percent of patients, and vomiting occurs in about one third of patients[citation needed]. Many patients experience sensory hyperexcitability manifested by photophobia, phonophobia, and osmophobia and seek a dark and quiet room. Blurred vision, delirium, nasal stuffiness, diarrhea, tinnitus, polyuria, pallor, or sweating may be noted during the headache phase. There may be localized edema of the scalp or face, scalp tenderness, prominence of a vein or artery in the temple, or stiffness and tenderness of the neck. Impairment of concentration and mood are common. The extremities tend to feel cold and moist[citation needed]. Vertigo may be experienced; a variation of the typical migraine, called vestibular migraine, has also been described. Lightheadedness, rather than true vertigo,[citation needed] and a feeling of faintness may occur.
Postdrome
The effects of migraine may persist for some days after the main headache has ended. Many sufferers report a sore feeling in the area where the migraine was, and some report impaired thinking for a few days after the headache has passed. The patient may feel tired or "hungover" and have head pain, cognitive difficulties, gastrointestinal symptoms, mood changes, and weakness.[19] According to one summary, "Some people feel unusually refreshed or euphoric after an attack, whereas others note depression and malaise."[20]
Objective signs
A temporary Horner's syndrome (ptosis-drooping lid, miosis-smaller pupil) may occur during a migraine attack and disappear afterwards.[21]
Cause
The underlying cause of migraines is unknown.[22] There are, however, many biological events that have been clinically associated with migraine.
Triggers
Migraines may be induced by triggers, with some reporting it as an influence in a minority of cases[13] and others the majority.[23] Many things have been labeled as triggers, however the strength and significance of these relationships are uncertain.[23][24] Common triggers quoted are stress, hunger, and fatigue (these equally contribute to tension headaches).[23] A 2003 review concluded there was no scientific evidence for an effect of tyramine on migraine.[25] A 2005 literature review on dietary triggers found the available scientific studies, mostly relying on subjective assessments, were not rigorous enough to prove or disprove any particular triggers.[26] This is in line with other reviews. A 2009 review of potential triggers in the indoor and outdoor environment concluded the overall evidence was of poor quality, but nevertheless suggested migraineurs take some preventative measures related to indoor air quality and lighting.[27] While monosodium glutamate (MSG) is frequently reported as a dietary trigger[28] evidence does not consistently support this.[29] Migraines are more likely to occur around menstruation.[30] Other hormonal influences, such as menarche, oral contraceptive use, pregnancy, perimenopause, and menopause, also play a role.[31]
Depolarization
The phenomenon known as cortical spreading depression, which is associated with the aura of migraine,[32] has been theorized as a possible cause of migraines. In cortical spreading depression, neurological activity is initially activated, then depressed over an area of the cerebral cortex. This situation has been suggested to result in the release of inflammatory mediators leading to irritation of cranial nerve roots, most particularly the trigeminal nerve, which conveys the sensory information for the face and much of the head. This theory is, however, speculative, without any supporting evidence, and there are indeed cogent arguments against it. First, only about one third of migraineurs experience an aura, and those who do not experience aura do not have cortical spreading depression.[citation needed] Second, many migraineurs have a prodrome (see above), which occurs up to three days before the aura.[14]
Vascular
Studies have shown the aura coincides with constriction of blood vessels in the brain. This may start in the occipital lobe, in the back of the brain, as arteries spasm. The reduced flow of blood from the occipital lobe triggers the aura some individuals who have migraines experience, because the visual cortex is in the occipital area.[33][unreliable source?]
When the constriction of blood vessels in the brain stops and the aura subsides, the blood vessels of the scalp dilate.[34] The walls of these blood vessels become permeable and some fluid leaks out. This leakage is recognized by pain receptors in the blood vessels of surrounding tissue. In response, the body supplies the area with chemicals which cause inflammation. With each heart beat, blood passes through this sensitive area, causing a throb of pain.[33][unreliable source?]
Although cerebral vasodilation can trigger migraine attacks, blood vessel diameters return to normal more than an hour before the migraine headaches occur.[35]
Serotonin
Serotonin is a type of neurotransmitter, or "communication chemical" which passes messages between nerve cells. It helps to control mood, pain sensation, sexual behaviour and sleep, as well as dilation and constriction of the blood vessels, among other things. Low serotonin levels in the brain may lead to a process of constriction and dilation of the blood vessels which trigger a migraine.[33] Serotonergic agonists, such as triptans,[33] LSD or psilocin, activate serotonin receptors to stop a migraine attack.
Melanopsin receptor
A melanopsin-based receptor has been linked to the association between light sensitivity and migraine pain,[36] but this is currently speculation.
Neural
When certain nerves or an area in the brain stem become irritated, a migraine begins. In response to the irritation, the body releases chemicals which cause inflammation of the blood vessels. These chemicals cause further irritation of the nerves and blood vessels and results in pain. Substance P is one of the substances released with first irritation. Pain then increases because substance P aids in sending pain signals to the brain.[33]
Unifying theory
Both vascular and neural influences cause migraines.
- stress triggers changes in the brain
- these changes cause serotonin and/or histamine to be released
- blood vessels constrict and dilate
- chemicals, including substance P, irritate nerves and blood vessels, causing neurogenic inflammation and pain.[33]
Pathophysiology
Migraine is a neurovascular disorder.[13] Although migraine is thought by some to be a neurological disease, in the absence of scientific evidence, this remains a hypothesis.
Initiation
Migraines were once thought to be initiated exclusively by problems with blood vessels, but the vascular changes of migraines are now considered by some to be secondary to brain dysfunction,[33] although this concept has not been supported by the evidence. This was eloquently summed up by Dodick, who wrote, "There is no disputing the role of the central nervous system in the susceptibility, modulation and expression of migraine headache and the associated affective, cognitive, sensory, and neurological symptoms and signs. However, to presume that migraine is always generated from within the central nervous system, based on the available evidence, is naïve at best and unscientific at worst.The emerging evidence would suggest that just as alterations in neuronal activity can lead to downstream effects on the cerebral blood vessel, so too can changes within endothelial cells or vascular smooth muscle lead to downstream alterations in neuronal activity. Therefore, there are likely patients, and/or at least attacks in certain patients, where primarily vascular mechanisms predominate."[37] Some have even attempted to show that vascular changes are of no importance in migraine,[38][39] but this claim is unsubstantiated and has not been supported by scientific evidence. 'If we swing between vascular and neurogenic views of migraine, it is probably because both vascular and neurogenic mechanisms for migraine exist and are important'- J Edmeads[37]
Pain
Although the initiating factor of migraine remains unknown, copious, irrefutable evidence shows the pain of migraine (the third phase)[3] is, in some patients, related to painful dilatation of the terminal branches of the external carotid artery, and in particular its superficial temporal and occipital branches.[34][40][41][42][43][44] Dilatation of the arteries in the brain and dura mater previously was thought to be the origin of the vascular pain, but these vessels have been shown to not dilate during migraine.[45][46] Because these arteries are relatively superficial, it is easy to diagnose whether they are the source of the pain. If they are, then they are also accessible to a form of migraine surgery being promoted, largely to the efforts of Dr Elliot Shevel, a South African surgeon, who has reported excellent success using the procedure.[47]
Pericranial (jaw and neck) muscle tenderness is a common finding in migraine.[48][49][50] Muscle tenderness has been shown to be present in 100% of migraine attacks, making muscle tenderness the single most common finding in migraine.[48] Tender muscle trigger points can be at least part of the cause, and perpetuate most kinds of headaches.[51][unreliable source?]
Diagnosis
Migraines are underdiagnosed,[52] and often are misdiagnosed.[53] The diagnosis of migraine without aura, according to the International Headache Society, can be made according to the following criteria, the "5, 4, 3, 2, 1 criteria":[3]
- 5 or more attacks - for migraine with aura, two attacks are sufficient for diagnosis.
- 4 hours to 3 days in duration
- 2 or more of the following:
- Unilateral (affecting half the head);
- Pulsating;
- "Moderate or severe pain intensity";
- "Aggravation by or causing avoidance of routine physical activity"
- 1 or more of the following:
- "Nausea and/or vomiting";
- Sensitivity to both light (photophobia) and sound (phonophobia)
The mnemonic POUNDing (Pulsating, duration of 4–72 hOurs, Unilateral, Nausea, Disabling) can help diagnose migraine. If four of the five criteria are met, then the positive likelihood ratio for diagnosing migraine is 24.[54]
The presence of either disability, nausea or sensitivity can diagnose migraine with:[55]
- sensitivity of 81%
- specificity of 75%
Migraine should be differentiated from other causes of headaches, such as cluster headaches. These are extremely painful, unilateral headaches of a piercing quality. The duration of the common attack is 15 minutes to three hours. Onset of an attack is rapid, and most often without the preliminary signs characteristic of a migraine.[citation needed]
Medical imaging of the head and neck may be used to rule out secondary causes of headaches.[13]
Prevention
Main article: Prevention of migrainesPreventive (also called prophylactic) treatment of migraines can be an important component of migraine management. Such treatments can take many forms, including taking preventive drugs, migraine surgery, taking nutritional supplements, lifestyle alterations, such as increased exercise, and avoidance of migraine triggers.
The goals of preventive therapy are to reduce the frequency, painfulness, and/or duration of migraines, and to increase the effectiveness of abortive therapy.[56] Another reason to pursue these goals is to avoid medication overuse headache (MOH), otherwise known as rebound headache. This is a common problem among migraineurs, and can result in chronic daily headache.[57][58]
Many of the preventive treatments are quite effective. Even with a placebo, one-quarter of patients find their migraine frequency is reduced by half or more, and actual treatments often far exceed this figure.[59]
Medication
Preventive migraine drugs are considered effective if they reduce the frequency or severity of migraine attacks by at least 50%.[60] The major problem with migraine preventive drugs, apart from their relative inefficacy, is that unpleasant side effects are common. So, preventive medication is limited to patients with frequent or severe headaches.[61]
Many medicines are available to prevent or reduce frequency, duration and severity of migraine attacks. They may also prevent complications of migraine. Beta blockers, such as Propranolol, atenolol, and metoprolol; calcium channel blockers, such as amlodipine, flunarizine and verapamil; the anticonvulsants sodium valproate, divalproex, gabapentin and topiramate; and tricyclic antidepressants are some of the commonly used drugs.[citation needed]
Tricyclic antidepressants have been found to be more effective than SSRIs.[62] Tricyclic antidepressants have been long established as efficacious prophylactic treatments.[60] These drugs, however, may give rise to undesirable side effects, such as insomnia, sedation or sexual dysfunction. There is no consistent evidence that SSRI antidepressants are effective for migraine prophylaxis. While amitryptiline (Elavil) is the only tricyclic to have received FDA approval for migraine treatment, other tricyclic antidepressants are believed to act similarly and are widely prescribed, often to find one with a profile of side effects that is acceptable to the patient.[60] In addition to tricyclics a, the antidepressant nefazodone may also be beneficial in the prophylaxis of migraines due to its antagonistic effects on the 5-HT2A[63] and 5-HT2C receptors[64][65] It has a more favorable side effect profile than amitriptyline, a tricyclic antidepressant commonly used for migraine prophylaxis. Antidepressants offer advantages for treating migraine patients with comorbid depression.[60] SSRIs are not approved by the FDA for treatment of migraines, but have been found to be effective by some practitioners.[60]
There is some evidence that low-dose asprin has benefit for reducing the occurrence of migraines in susceptible individuals.[66][67][68]
Surgery
Migraine surgery is a field that shows a great deal of promise, particularly in those who suffer more frequent attacks, and in those who have not had an adequate response to prophylactic medications. Patients often still experience a poor quality of life despite an aggressive regimen of pharmacotherapy.[69] For these reasons, surgical solutions to migraines have been developed, which have excellent results.[70][71][72][73][74][75][76][77][78][79][80][81][82] A major advantage of migraine surgery is that, with the correct diagnostic techniques, a definite diagnosis can be made before the surgery is undertaken. Once a positive diagnosis has been made, the results of surgery are outstanding and provide permanent pain relief, as well as relief from the associated symptoms, such as nausea, vomiting, light sensitivity, and sound sensitivity. Surgical cauterization of the superficial blood vessels of the scalp (the terminal branches of the external carotid artery) is only carried out if it has been established with certainty that these vessels are indeed the source of pain. It is a safe and relatively atraumatic procedure which can be performed in a day facility.[70] The value of arterial sugery for migraine treatment is gaining recognition as a result of the efforts of a South African surgeon, Dr Elliot Shevel, who has produced a number of papers on the subject.[citation needed]
The removal of muscles or nerves in areas known as "trigger sites" provides good results, but only in patients who respond well to Botox injections in specific areas.[71]
There is also evidence that the correction of a congenital heart defect, patent foramen ovale (PFO), reduces migraine frequency and severity.[83] Recent studies have advised caution, though, in relation to PFO closure for migraines, as insufficient evidence exists to justify this dangerous procedure.[84][85]
Other therapies
Medical devices, such as biofeedback and neurostimulators, have some advantages in the migraine treatment, mainly when common antimigraine medication is contraindicated or in case of medication over use. Biofeedback helps patient to be conscious of some physiologic parameters to control them and try to relax. This method is considered to be efficient for migraine[86] and tension-type headache treatment.[87] A recent clinical trial has demonstrated that simple use of biofeedback as a relaxation technique has similar efficacy for migraine treatment to sophisticated sessions in clinics.[88] Neurostimulation used initially implantable neurostimulators similar to pacemakers for the treatment of intractable chronic migraines[89][90] with encouraging good results. But the needed surgery with implantable neurostimulators is limiting the indication to sever cases.[91] Recently, a new technique of external trigeminal (V1) or occipital nerve (CII) neurostimulation (Cefaly) could offer a larger use for migraine treatment or prevention.[citation needed]
A systematic review stated that chiropractic manipulation, physiotherapy, massage and relaxation might be as effective as propranolol or topiramate in the prevention of migraine headaches; however, the research had some problems with methodology.[92]
"The therapeutic potential of magnesium, coenzyme Q(10), riboflavin, and vitamin B(12) can be cautiously inferred from some published open clinical trials."[93] A review has concluded that "[c]urrent clinical data support the use of fever-few, butterbur, magnesium, and riboflavin in migraine prophylaxis."[94]
Migraine diary
A migraine diary allows the assessment of headache characteristics, to differentiate between migraine and tension-type headache and to record the use and efficacy of acute medication. A diary also helps to analyse the relationship between migraine and menstruation.[95] Finally, the diary can help to identify trigger factors. A trigger may occur up to 24 hours prior to the onset of symptoms;[13] the majority of migraines, though, are not caused by identifiable triggers.[13]
Management
There are three main aspects of treatment: trigger avoidance, acute symptomatic control, and pharmacological prevention.[13] Medications are more effective if used earlier in an attack.[13] The frequent use of medications may, however, result in medication overuse headache, in which the headaches become more severe and more frequent. These may occur with triptans, ergotamines, and analgesics, especially narcotic analgesics.[3]
Analgesics
A number of analgesics are effective for treating migraines including:
- Non-steroidal anti-inflammatory drugs (NSAIDs): Ibuprofen provides effective pain relief in about half of people.[96] Naproxen can abort about one third of migraine attacks, which was 5% less than the benefit of sumatriptan.[97] A 1000 mg dose of aspirin could relieve moderate to severe migraine pain, with similar effectiveness to sumatriptan.[98]
- Paracetamol/acetaminophen, either alone or in combination with metaclopramide, is effective for migraines.[99]
- Simple analgesics combined with caffeine may help.[100] Even by itself, caffeine can be useful during an attack,[101][102] despite the fact that migraine sufferers are generally advised to limit their caffeine intake.[102]
Triptans
Triptans such as sumatriptan are effective for both pain and nausea in up to 75% of people.[13][103] The different forms available include oral, injection, nasal spray, and oral dissolving tablets.[13] Most side effects are mild, such as flushing; however, rare cases of myocardial ischemia have occurred.[13] They are not addictive, but may cause medication overuse headaches if used more than 10 days per month.[104]
Ergotamines
Ergotamine[13] and dihydroergotamine are older medications still prescribed for migraines, the latter in nasal spray and injectable forms.[13] They were the primary drugs available to abort a migraine prior to the triptans, and are much less expensive than triptans.[citation needed]
Corticosteroids
A single dose of intravenous dexamethasone, when added to standard treatment of a migraine attack, is associated with a 26% decrease in headache recurrence in the following 72 hours.[105]
Other
Antiemetics by mouth may help relieve symptoms of nausea and help prevent vomiting, which can diminish the effectiveness of orally taken analgesics. In addition, some antiemetics, such as metoclopramide, are prokinetics and help gastric emptying, which is often impaired during episodes of migraine. In the UK, three combination antiemetic and analgesic preparations are available: MigraMax (aspirin with metoclopramide), (paracetamol/codeine for analgesia, with buclizine as the antiemetic) and paracetamol/metoclopramide (Paramax in UK).[106] The earlier these drugs are taken in the attack, the better their effect.
Prognosis
The risk of stroke may be increased two- to three-fold in migraine sufferers. Young adult sufferers and women using hormonal contraception appear to be at particular risk.[107] The mechanism of any association is unclear, but chronic abnormalities of cerebral blood vessel tone may be involved. Women who experience auras have been found to have twice the risk of strokes and heart attacks over nonaura migraine sufferers and women who do not have migraines.[107][108] (Note: Women who experience auras and also take oral contraceptives have an even higher risk of stroke).[109] Migraine sufferers seem to be at risk for both thrombotic and hemorrhagic stroke as well as transient ischemic attacks.[110] Death from cardiovascular causes was higher in people with migraine with aura in a Women's Health Initiative study, but more research is needed to confirm this.[108][111]
Epidemiology
 Disability-adjusted life year for migraines per 100,000 inhabitants in 2002.
Disability-adjusted life year for migraines per 100,000 inhabitants in 2002. no dataless than 4545-6565-8585-105105-125125-145145-165165-185185-205205-225225-245more than 245
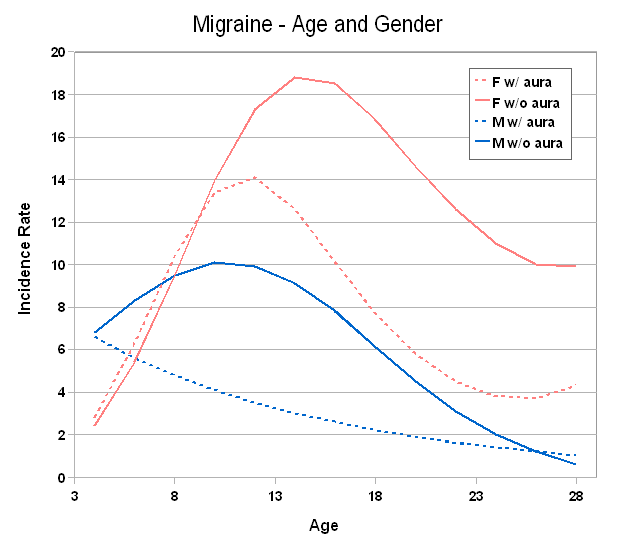
no dataless than 4545-6565-8585-105105-125125-145145-165165-185185-205205-225225-245more than 245 Incidence of migraine by age and sex
Incidence of migraine by age and sexWorldwide, migraines affect more than 10% of people.[22] In the United States, about 6% of men and 18% of women get a migraine in a given year, with a lifetime risk of about 18% and 43% respectively.[13] In Europe, migraines affect 12–28% of people at some point in their lives.[2] Based on the results of a number of studies, one-year prevalence of migraine ranges from 6–15% in adult men and from 14–35% in adult women.[2] These figures vary substantially with age: approximately 4–5% of children aged under 12 suffer from migraine, with little apparent difference between boys and girls.[112] A rapid growth in incidence amongst girls occurs after puberty,[113][114][115] which continues throughout early adult life.[116] By early middle age, around 25% of women experience a migraine at least once a year, compared with fewer than 10% of men.[2][117] After menopause, attacks in women tend to decline dramatically, so that in the over 70s, approximately equal numbers of males and females are sufferers, with prevalence returning to around 5%.[2][117]
At all ages, migraine without aura is more common than migraine with aura, with a ratio of between 1.5 and 2.0:1.[118][119] Incidence figures show the excess of migraine seen in women of reproductive age is mainly due to migraine without aura.[118] Thus, in prepubertal and postmenopausal populations, migraine with aura is somewhat more common than amongst 15–50 year olds.[116][120]
There is a strong relationship between age, sex and type of migraine.[121]
Studies in Asia and South America suggest the rates there are relatively low,[122][123] but they do not fall outside the range of values seen in European and North American studies.[2][117]
The incidence of migraine is related to the incidence of epilepsy in families, with migraine twice as prevalent in family members of epilepsy sufferers, and more common in epilepsy sufferers themselves.[124]
History
 The Head Ache, George Cruikshank (1819)
The Head Ache, George Cruikshank (1819)Trepanation, the deliberate and (usually) nonfatal drilling of holes into a skull, was practiced 9,000 years ago and earlier.[125] Some scholars have (controversially) speculated this drastic procedure might have been a migraine treatment, based on cave paintings[126] and on the fact that trepanation was a historical migraine treatment in 17th-century Europe.[125][127] An early written description consistent with migraines is contained in the Ebers papyrus, written around 1200 BC in ancient Egypt.[125]
In 400 BC, Hippocrates described the visual aura that can precede the migraine headache, and the relief which can occur through vomiting. Aretaeus of Cappadocia is credited as the "discoverer" of migraines because of his second-century description of the symptoms of a unilateral headache associated with vomiting, with headache-free intervals in between attacks.
Galenus of Pergamon used the term "hemicrania" (half-head), from which the word "migraine" was derived. He thought there was a connection between the stomach and the brain because of the nausea and vomiting that often accompany an attack. For relief of migraine, Andalusian-born physician Abulcasis, also known as Abu El Qasim, suggested application of a hot iron to the head or insertion of garlic into an incision made in the temple.
In the Middle Ages. migraine was recognized as a discrete medical disorder. Followers of Galenus explained migraine as being caused by aggressive yellow bile. Ebn Sina (Avicenna) described migraine in his textbook "El Qanoon fel teb" as "... small movements, drinking and eating, and sounds provoke the pain... the patient cannot tolerate the sound of speaking and light. He would like to rest in darkness alone." Abu Bakr Mohamed Ibn Zakariya Râzi noted the association of headache with different events in the lives of women, "...And such a headache may be observed after delivery and abortion or during menopause and dysmenorrhea."
In Bibliotheca Anatomica, Medic, Chirurgica, published in London in 1712, five major types of headaches are described, including the "Megrim", recognizable as classic migraine. The term "classic migraine" is no longer used, and has been replaced by the term "migraine with aura"[3] Graham and Wolff (1938) published their paper advocating ergotamine tartrate for relieving migraine. Later in the 20th century, Harold Wolff (1950) developed the experimental approach to the study of headache and elaborated the vascular theory of migraine, which has come under attack as the pendulum again swings to the neurogenic theory. Recently, there has been renewed interest in Wolff's vascular theory of migraine led by Elliot Shevel, a South African headache specialist, who has published a number of articles providing compelling evidence that Wolff was correct.[41][46][47][128]
Society and culture
Economic impact
Chronic migraine attacks are a significant source of both medical costs and lost productivity. It has been estimated to be the most costly neurological disorder in the European Community, costing more than €27 billion per year.[129]
Research
Merck Corp new drug, Telcagepant, intended to relieve pain without causing vasoconstriction (narrowing of blood vessels) as current medications such as triptans do, was pulled from the market after clinical trials showed liver function abnormalities in some study subjects. ^ Merck & Co.: Memo to all US study locations involved in protocol MK0974-049
Recently, calcitonin gene related peptides (CGRPs) have been found to play a role in the pathogenesis of the pain associated with migraine, as triptans also decrease its release and action. CGRP receptor antagonists, such as olcegepant and telcagepant, are being investigated both in vitro and in clinical studies for the treatment of migraine.[130]
In 2010, scientists identified a genetic defect linked to migraines which could provide a target for new drug treatments.[131]
References
- ^ Mosby’s Medical, Nursing and Allied Health Dictionary, Fourth Edition, Mosby-Year Book 1994, p. 998
- ^ a b c d e f Stovner LJ, Zwart JA, Hagen K, Terwindt GM, Pascual J (April 2006). "Epidemiology of headache in Europe". European Journal of Neurology 13 (4): 333–45. doi:10.1111/j.1468-1331.2006.01184.x. PMID 16643310.
- ^ a b c d e f g h i Headache Classification Subcommittee of the International Headache Society (2004). "The International Classification of Headache Disorders: 2nd edition". Cephalalgia 24 (Suppl 1): 9–160. doi:10.1111/j.1468-2982.2004.00653.x. PMID 14979299.
- ^ "NINDS Migraine Information Page". National Institute of Neurological Disorders and Stroke, National Institutes of Health. http://www.ninds.nih.gov/disorders/migraine/migraine.htm. Retrieved 2007-06-25.
- ^ "Guidelines for all healthcare professionals in the diagnosis and management of migraine, tension-type, cluster and medication-overuse headache, January 2007, British Association for the Study of Headache" (PDF). http://217.174.249.183/upload/NS_BASH/BASH_guidelines_2007.pdf. Retrieved 2007-06-25.
- ^ IHS. "The International Classification of Headache Disorders". Cephalalgia Vol 24. Blackwell/Sage. http://www.i-h-s.org/upload/ct_clas/ihc_II_main_no_print.pdf. Retrieved 6/27.
- ^ Dodick, David. "Why Migraines Strike". Scientific American Aug. 08. Nature America, Inc.. http://www.scientificamerican.com/article.cfm?id=why-migraines-strike. Retrieved 27 June 2011.
- ^ Gervil M, Ulrich V, Kaprio J, Olesen J, Russell MB (September 1999). "The relative role of genetic and environmental factors in migraine without aura". Neurology 53 (5): 995–9. PMID 10496258. http://www.neurology.org/cgi/pmidlookup?view=long&pmid=10496258.
- ^ Ulrich V, Gervil M, Kyvik KO, Olesen J, Russell MB (March 1999). "The inheritance of migraine with aura estimated by means of structural equation modelling". Journal of Medical Genetics 36 (3): 225–7. PMC 1734315. PMID 10204850. http://jmg.bmj.com/cgi/pmidlookup?view=long&pmid=10204850.
- ^ Lay CL, Broner SW (May 2009). "Migraine in women". Neurologic Clinics 27 (2): 503–11. doi:10.1016/j.ncl.2009.01.002. PMID 19289228.
- ^ "AHS — The American Headache Society Official Website". American Headache Society. http://www.americanheadachesociety.org/. Retrieved 2011-05-30.
- ^ "IHS — International Headache Society» Home". Ihs-classification.org. http://www.ihs-classification.org/en/. Retrieved 2011-05-30.
- ^ a b c d e f g h i j k l m n o p Bartleson JD, Cutrer FM (May 2010). "Migraine update. Diagnosis and treatment". Minn Med 93 (5): 36–41. PMID 20572569.
- ^ a b Kelman L (October 2004). "The premonitory symptoms (prodrome): a tertiary care study of 893 migraineurs". Headache 44 (9): 865–72. doi:10.1111/j.1526-4610.2004.04168.x. PMID 15447695.
- ^ Silberstein, Stephen D. (2005). Atlas Of Migraine And Other Headaches. London: Taylor & Francis Group. ISBN 1-84214-273-9.[page needed]
- ^ Mathew, Ninan T.; Evans, Randolph W. (2005). Handbook of headache. Hagerstwon, MD: Lippincott Williams & Wilkins. ISBN 0-7817-5223-X.[page needed]
- ^ Silberstein, Stephen D. (2002). Headache in Clinical Practice (2nd ed.). London: Taylor & Francis Group. ISBN 1-901865-88-6.[page needed]
- ^ "Teichopsia — Medical Dictionary Definition", Stedman's Medical Dictionary, Retrieved on 2010-03-15.
- ^ Kelman L (February 2006). "The postdrome of the acute migraine attack". Cephalalgia 26 (2): 214–20. doi:10.1111/j.1468-2982.2005.01026.x. PMID 16426278.
- ^ Audrey L. Halpern, MD and Stephen D. Silberstein, MD, "The Migraine Attack—A Clinical Description", in Chapter 9 of Imitators of Epilepsy, weblink.
- ^ C Laing, D J Thomas, C J Mathias, and R J Unwin, "Headache, hypertension and Horner's syndrome.", J R Soc Med. 2000 October; 93(10): 535–536, weblink.
- ^ a b Robbins MS, Lipton RB (April 2010). "The epidemiology of primary headache disorders". Semin Neurol 30 (2): 107–19. doi:10.1055/s-0030-1249220. PMID 20352581.
- ^ a b c Levy D, Strassman AM, Burstein R (June 2009). "A critical view on the role of migraine triggers in the genesis of migraine pain". Headache 49 (6): 953–7. doi:10.1111/j.1526-4610.2009.01444.x. PMID 19545256.
- ^ Martin PR (June 2010). "Behavioral management of migraine headache triggers: learning to cope with triggers". Curr Pain Headache Rep 14 (3): 221–7. doi:10.1007/s11916-010-0112-z. PMID 20425190.
- ^ Jansen SC, van Dusseldorp M, Bottema KC, Dubois AE (September 2003). "Intolerance to dietary biogenic amines: a review". Annals of Allergy, Asthma & Immunology 91 (3): 233–40; quiz 241–2, 296. doi:10.1016/S1081-1206(10)63523-5. PMID 14533654. http://openurl.ingenta.com/content?genre=article&issn=1081-1206&volume=91&issue=3&spage=233&epage=241.
- ^ Holzhammer J, Wöber C (April 2006). "[Alimentary trigger factors that provoke migraine and tension-type headache]" (in German). Schmerz 20 (2): 151–9. doi:10.1007/s00482-005-0390-2. PMID 15806385.
- ^ Friedman DI, De ver Dye T (June 2009). "Migraine and the environment". Headache 49 (6): 941–52. doi:10.1111/j.1526-4610.2009.01443.x. PMID 19545255.
- ^ Sun-Edelstein C, Mauskop A (June 2009). "Foods and supplements in the management of migraine headaches". The Clinical Journal of Pain 25 (5): 446–52. doi:10.1097/AJP.0b013e31819a6f65. PMID 19454881.
- ^ Freeman M (October 2006). "Reconsidering the effects of monosodium glutamate: a literature review". J Am Acad Nurse Pract 18 (10): 482–6. doi:10.1111/j.1745-7599.2006.00160.x. PMID 16999713.
- ^ MacGregor, EA (2010-10-01). "Prevention and treatment of menstrual migraine.". Drugs 70 (14): 1799–818. doi:10.2165/11538090-000000000-00000. PMID 20836574.
- ^ Lay, CL; Broner, SW (2009 May). "Migraine in women.". Neurologic clinics 27 (2): 503–11. doi:10.1016/j.ncl.2009.01.002. PMID 19289228.
- ^ Lauritzen M (February 1994). "Pathophysiology of the migraine aura. The spreading depression theory". Brain 117 (1): 199–210. doi:10.1093/brain/117.1.199. PMID 7908596.
- ^ a b c d e f g Mauskop, Alexander; Fox, Barry (2001). Migraines: The Breakthrough Program That Can Help End Your Pain. What Your Doctor May Not Tell You About. New York: Warner Books. ISBN 0-446-67826-0.[page needed]
- ^ a b Shevel E (2011). "The Extracranial Vascular Theory of Migraine – A Great Story Confirmed by the Facts". Headache 51 (3): 409–417. doi:10.1111/j.1526-4610.2011.01844.x. PMID 21352215.
- ^ "Migraine and cerebral vasodilation". Brain.oxfordjournals.org. 2008-05-23. http://brain.oxfordjournals.org/content/131/8/2192.abstract. Retrieved 2011-05-30.
- ^ Noseda R, Kainz V, Jakubowski M et al. (February 2010). "A neural mechanism for exacerbation of headache by light". Nature Neuroscience 13 (2): 239–45. doi:10.1038/nn.2475. PMC 2818758. PMID 20062053. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2818758. Lay summary – ScienceNOW (January 11, 2010).
- ^ a b Dodick, David W. (2008). "Examining the Essence of Migraine—Is it the Blood Vessel or the Brain? A Debate". Headache: the Journal of Head and Face Pain 48 (4): 661–7. doi:10.1111/j.1526-4610.2008.01079.x.
- ^ Goadsby, P. J. (2008). "The vascular theory of migraine--a great story wrecked by the facts". Brain 132 (Pt 1): 6–7. doi:10.1093/brain/awn321. PMID 19098031.
- ^ Cohen AS, Goadsby PJ (April 2005). "Functional neuroimaging of primary headache disorders". Current Pain and Headache Reports 9 (2): 141–6. doi:10.1007/s11916-005-0053-0. PMID 15745626.
- ^ Shevel, Elliot (September 19, 2007). "The Role of the External Carotid Vasculature in Migraine". In Clarke, Laura B. Migraine Disorders Research Trends. New York, New York, US: Nova Science Publishers. pp. 165–183. ISBN 9781600215537. Preview the chapter at Google Book Search
- ^ a b Shevel E, Spierings E (2004). "Role of the Extracranial Arteries in Migraine Headache: a Review". Cranio:the Journal of Craniomandibular Practice 22 (2): 132–6. PMID 15134413.
- ^ Wolff HG, Tunis MM, Goodell H. (1953). "Studies on headache; evidence of damage and changes in pain sensitivity in subjects with vascular headaches of the migraine type". Transactions of the Association of American Physicians 66 (4): 332–341. PMID 13091465.
- ^ Pickering GW (1939). "Experimental Observations on Headache". British Medical Journal 1 (4–6): 907–912. doi:10.1136/bmj.1.4087.907. PMC 2209487. PMID 13306341. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2209487.
- ^ Tunis MM, Wolff HG. (1953). "Analysis of Arterial Pulse Waves in Patients with Vascular Headache of the Migraine Type". American Journal of Medical Science 224 (5): 121–123. PMID 12985578.
- ^ Schoonman, G. G.; Van Der Grond, J.; Kortmann, C.; Van Der Geest, R. J.; Terwindt, G. M.; Ferrari, M. D. (2008). "Migraine headache is not associated with cerebral or meningeal vasodilatation--a 3T magnetic resonance angiography study". Brain 131 (8): 2192–200. doi:10.1093/brain/awn094.
- ^ a b Shevel E (2009). "Middle meningeal artery dilatation in migraine". Headache 49 (10): 1541–3. doi:10.1111/j.1526-4610.2009.01495.x. PMID 19656222.
- ^ a b Shevel E (2007). "Vascular Surgery for Chronic Migraine". Therapy 4 (4): 451–456. doi:10.2217/14750708.4.4.451.
- ^ a b Tfelt-Hansen P, Lous I, Olesen J. (1981). "Prevalence and significance of muscle tenderness during common migraine attacks". Headache 21 (2): 49–54. doi:10.1111/j.1526-4610.1981.hed2102049.x. PMID 7239900.
- ^ Olesen J. (1978). "Some clinical features of the acute migraine attack. An analysis of 750 patients". Headache 18 (5): 268–271.. doi:10.1111/j.1526-4610.1978.hed1805268.x. PMID 721459.
- ^ Jensen K, Tuxen C, Olesen J (1988). "Pericranial muscle tenderness and pressure-pain threshold in the temporal region during common migraine". Pain 35 (1): 65–70. doi:10.1016/0304-3959(88)90277-1. PMID 3200599.
- ^ Trigger Point Therapy for Headaches & Migraines, DeLaune, Valerie (New Harbinger: 2008) [1]
- ^ Lipton RB, Stewart WF, Celentano DD, Reed ML (June 1992). "Undiagnosed migraine headaches. A comparison of symptom-based and reported physician diagnosis". Archives of Internal Medicine 152 (6): 1273–8. doi:10.1001/archinte.152.6.1273. PMID 1599358.
- ^ Schreiber CP, Hutchinson S, Webster CJ, Ames M, Richardson MS, Powers C (September 2004). "Prevalence of migraine in patients with a history of self-reported or physician-diagnosed 'sinus' headache". Archives of Internal Medicine 164 (16): 1769–72. doi:10.1001/archinte.164.16.1769. PMID 15364670.
- ^ Detsky ME, McDonald DR, Baerlocher MO, Tomlinson GA, McCrory DC, Booth CM (September 2006). "Does this patient with headache have a migraine or need neuroimaging?". JAMA 296 (10): 1274–83. doi:10.1001/jama.296.10.1274. PMID 16968852.
- ^ Lipton RB, Dodick D, Sadovsky R et al. (August 2003). "A self-administered screener for migraine in primary care: The ID Migraine validation study". Neurology 61 (3): 375–82. PMID 12913201. http://www.neurology.org/cgi/pmidlookup?view=long&pmid=12913201.
- ^ Modi S, Lowder DM (January 2006). "Medications for migraine prophylaxis". American Family Physician 73 (1): 72–8. PMID 16417067. http://www.aafp.org/link_out?pmid=16417067.
- ^ Diener HC, Limmroth V (August 2004). "Medication-overuse headache: a worldwide problem". Lancet Neurology 3 (8): 475–83. doi:10.1016/S1474-4422(04)00824-5. PMID 15261608.
- ^ Fritsche, Guenther; Diener, Hans-Christoph (2002). "Medication overuse headaches – what is new?". Expert Opinion on Drug Safety 1 (4): 331–8. doi:10.1517/14740338.1.4.331. PMID 12904133.
- ^ Van Der Kuy, P-HM; Lohman, Jjhm (2002). "A quantification of the placebo response in migraine prophylaxis". Cephalalgia 22 (4): 265–70. doi:10.1046/j.1468-2982.2002.00363.x. PMID 12100088.
- ^ a b c d e Kaniecki R, Lucas S. (2004). "Treatment of primary headache: preventive treatment of migraine". Standards of care for headache diagnosis and treatment. Chicago: National Headache Foundation. pp. 40–52.
- ^ Silberstein SD, Lipton RB. (1994). "Overview of diagnosis and treatment of migraine". Neurology 44 (10 Suppl 7): S6–S16. PMID 7969947.
- ^ Jackson JL, Shimeall W, Sessums L et al. (2010). "Tricyclic antidepressants and headaches: systematic review and meta-analysis". BMJ 341: c5222. doi:10.1136/bmj.c5222. PMC 2958257. PMID 20961988. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2958257.
- ^ Saper, Joel R.; Lake, Alvin E.; Tepper, Stewart J. (2001). "Nefazodone for Chronic Daily Headache Prophylaxis: An Open-Label Study". Headache: the Journal of Head and Face Pain 41 (5): 465–74. doi:10.1046/j.1526-4610.2001.01084.x.
- ^ Mylecharane, E. J. (1991). "5-HT2 receptor antagonists and migraine therapy". Journal of Neurology 238: S45–52. doi:10.1007/BF01642906. PMID 2045831.
- ^ Millan, Mark John (2005). "Le récepteur 5-HT2Ccomme cible dans le traitement des états dépressifs et anxieux : Nouvelles stratégies thérapeutiques [Serotonin 5-HT2C Receptors as a Target for the Treatment of Depressive and Anxious States: Focus on Novel Therapeutic Strategies]" (in French). Thérapie 60 (5): 441–60. doi:10.2515/therapie:2005065.
- ^ "Aspirin and Migraine". National Headache Foundation. http://www.headaches.org/education/Medications/Aspirin_and_Migraine. Retrieved 2011-03-28.[unreliable medical source?]
- ^ Dalessio, DJ (1990). "Aspirin prophylaxis for migraine". JAMA 264 (13): 1721. doi:10.1001/jama.264.13.1721. PMID 2398614.
- ^ Buring, JE; Peto, R; Hennekens, CH (1990). "Low-dose aspirin for migraine prophylaxis". JAMA 264 (13): 1711–3. doi:10.1001/jama.264.13.1711. PMID 2204739. Lay summary – Science News (February 17, 1990).
- ^ Jensen, Rigmor; Stovner, Lars J (2008). "Epidemiology and comorbidity of headache". The Lancet Neurology 7 (4): 354–61. doi:10.1016/S1474-4422(08)70062-0.
- ^ a b Shevel, Elliot (2007). "Vascular surgery for chronic migraine". Therapy 4 (4): 451–6. doi:10.2217/14750708.4.4.451.
- ^ a b Guyuron, B; Kriegler, JS; Davis, J; Amini, SB (2005). "Comprehensive surgical treatment of migraine headaches". Plastic and reconstructive surgery 115 (1): 1–9. PMID 15622223.
- ^ Poggi, Joseph T.; Grizzell, Brett E.; Helmer, Stephen D. (2008). "Confirmation of Surgical Decompression to Relieve Migraine Headaches". Plastic and Reconstructive Surgery 122 (1): 115–22; discussion 123–4. doi:10.1097/PRS.0b013e31817742da. PMID 18594393.
- ^ Shi FY (1989). "[Morphological studies of extracranial arteries in patients with migraine]" (in Chinese). Zhonghua Bing Li Xue Za Zhi 18 (4): 271–3. PMID 2636957.
- ^ Hankemeier U (1985). "[Therapy of pulsating temporal headache. Resection of the superficial temporal artery]" (in German). Fortschr Med 103 (35): 822–4. PMID 4054803.
- ^ Sacristán HD, Ramírez AB (@9 April). "Tratamiento Quirurgico de las Jaquecas" (in Spanish). Annales de la Real, X Sesion Cientifica.
- ^ Rapidis AD (1976). "The therapeutic result of excision of the superficial temporal artery in atypical migraine". J Maxillofac Surg 4 (3): 182–8. doi:10.1016/S0301-0503(76)80029-X. PMID 1066419.
- ^ Holland JT (1976). "Three cases of vascular headache treated by surgery". Proc Aust Assoc Neurol 13: 51–4. PMID 1029006.
- ^ Florescu V, Florescu R (1975). "[Value of resection of the superficial temporal vasculo-nervous bundle in some cases of vascular headache]" (in Romanian). Rev Chir Oncol Radiol O R L Oftalmol Stomatol Otorinolaringol 20 (2): 113–7. PMID 127294.
- ^ Bouche J, Freche C, Chaix G, Dervaux JL. (1974). "[Surgery by cryotherapy of the superficial temporal artery in temporo-parietal neuralgia]" (in French). Ann Otolaryngol Chir Cervicofac 91 (1): 56–9. PMID 4603862.
- ^ Cook N. (1973). "Cryosurgery of migraine". Headache 12 (4): 143–50. doi:10.1111/j.1526-4610.1973.hed1204143.x. PMID 4682552.
- ^ Cook N. (1978). "Cryosurgery of headache". Res Clin Stud Headache 5: 86–101. PMID 674810.
- ^ Murillo, Casmir A. (1968). "Resection of the temporal neurovascular bundle for control of migraine headache". Headache 8 (3): 112–7. doi:10.1111/j.1526-4610.1968.hed0803112.x. PMID 5730120.
- ^ Harder, B. (2005). "Against the Migraine". Science News 167 (8): 119–120. doi:10.2307/4016110. JSTOR 4016110.
- ^ Schürks, M; Diener, HC (2009). "Closure of patent foramen ovale in the prevention of migraine: Not enough evidence in favor". Nature clinical practice. Neurology 5 (1): 22–3. doi:10.1038/ncpneuro0971. PMID 19048002.
- ^ Sarens, T; Herroelen, L; Van Deyk, K; Budts, W (2009). "Patent foramen ovale closure and migraine: Are we following the wrong pathway?". Journal of neurology 256 (1): 143–4. doi:10.1007/s00415-009-0126-9. PMID 19172218.
- ^ Nestoriuc, Yvonne; Martin, Alexandra (2007). "Efficacy of biofeedback for migraine: A meta-analysis". Pain 128 (1–2): 111–27. doi:10.1016/j.pain.2006.09.007. PMID 17084028.
- ^ Nestoriuc, Y; Martin, A; Rief, W; Andrasik, F (2008). "Biofeedback treatment for headache disorders: A comprehensive efficacy review". Applied psychophysiology and biofeedback 33 (3): 125–40. doi:10.1007/s10484-008-9060-3. PMID 18726688.
- ^ Mullally, William J.; Hall, Kathryn; Goldstein, Richard (2009). "Efficacy of biofeedback in the treatment of migraine and tension type headaches". Pain physician 12 (6): 1005–11. PMID 19935987. http://www.painphysicianjournal.com/linkout_vw.php?issn=1533-3159&vol=12&page=1005.
- ^ Schoenen, J; Allena, M; Magis, D (2010). "Neurostimulation therapy in intractable headaches". Handbook of clinical neurology / edited by P.J. Vinken and G.W. Bruyn. Handbook of Clinical Neurology 97: 443–50. doi:10.1016/S0072-9752(10)97037-1. ISBN 9780444521392. PMID 20816443.
- ^ Reed, KL; Black, SB; Banta Cj, 2nd; Will, KR (2010). "Combined occipital and supraorbital neurostimulation for the treatment of chronic migraine headaches: Initial experience". Cephalalgia 30 (3): 260–71. doi:10.1111/j.1468-2982.2009.01996.x. PMID 19732075.
- ^ Leone, M; Cecchini, AP; Franzini, A; Bussone, G (2011). "Neuromodulation in drug-resistant primary headaches: What have we learned?". Neurological sciences 32 Suppl 1: S23–6. doi:10.1007/s10072-011-0554-z. PMID 21533707.
- ^ Chaibi, Aleksander; Tuchin, Peter J.; Russell, Michael Bjørn (2011). "Manual therapies for migraine: A systematic review". The Journal of Headache and Pain 12 (2): 127–33. doi:10.1007/s10194-011-0296-6. PMC 3072494. PMID 21298314. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=3072494.
- ^ Bianchi, A; Salomone, S; Caraci, F; Pizza, V; Bernardini, R; Damato, C (2004). "Role of Magnesium, Coenzyme Q10, Riboflavin, and Vitamin B12 in Migraine Prophylaxis". Vitamins & Hormones Volume 69. Vitamins & Hormones. 69. pp. 297–312. doi:10.1016/S0083-6729(04)69011-X. ISBN 978-0-12-709869-2.
- ^ Rios, Juanita; Passe, Megan M. (2004). "Evidenced-Based Use of Botanicals, Minerals, and Vitamins in the Prophylactic Treatment of Migraines". Journal of the American Academy of Nurse Practitioners 16 (6): 251–6. doi:10.1111/j.1745-7599.2004.tb00447.x. PMID 15264611.
- ^ Lieba-Samal, Doris; Wöber, Christian; Frantal, Sophie; Brannath, Werner; Schmidt, Karin; Schrolnberger, Claudia; Wöber-Bingöl, Çicek; Pamina Study, Group (2011). "Headache, menstruation and combined oral contraceptives: A diary study in 184 women with migraine". European Journal of Pain 15 (8): 852–7. doi:10.1016/j.ejpain.2011.02.003. PMID 21402485.
- ^ Rabbie R, Derry S, Moore RA, McQuay HJ (2010). Moore, Maura. ed. "Ibuprofen with or without an antiemetic for acute migraine headaches in adults". Cochrane Database Syst Rev 10 (10): CD008039. doi:10.1002/14651858.CD008039.pub2. PMID 20927770.
- ^ Brandes JL, Kudrow D, Stark SR et al. (April 2007). "Sumatriptan-naproxen for acute treatment of migraine: a randomized trial". JAMA 297 (13): 1443–54. doi:10.1001/jama.297.13.1443. PMID 17405970.
- ^ Kirthi V, Derry S, Moore RA, McQuay HJ (2010). Moore, Maura. ed. "Aspirin with or without an antiemetic for acute migraine headaches in adults". Cochrane Database Syst Rev 4 (4): CD008041. doi:10.1002/14651858.CD008041.pub2. PMID 20393963.
- ^ Derry S, Moore RA, McQuay HJ (2010). Moore, Maura. ed. "Paracetamol (acetaminophen) with or without an antiemetic for acute migraine headaches in adults". Cochrane Database Syst Rev 11 (11): CD008040. doi:10.1002/14651858.CD008040.pub2. PMID 21069700.
- ^ Goldstein J, Hoffman HD, Armellino JJ et al. (September 1999). "Treatment of severe, disabling migraine attacks in an over-the-counter population of migraine sufferers: results from three randomized, placebo-controlled studies of the combination of acetaminophen, aspirin, and caffeine". Cephalalgia 19 (7): 684–91. doi:10.1046/j.1468-2982.1999.019007684.x. PMID 10524663.
- ^ ""Migraine headaches" information from the Cleveland Clinic". My.clevelandclinic.org. 2006-01-09. http://my.clevelandclinic.org/disorders/Migraine_Headache/hic_Migraine_Headaches.aspx. Retrieved 2011-05-30.
- ^ a b Cady, Roger; Dodick, David W. (March 2002). "Diagnosis and Treatment of Migraine". Mayo Clinic Proceedings 77 (3): 255–61. doi:10.4065/77.3.255. PMID 11888029.
- ^ Johnston MM, Rapoport AM (August 2010). "Triptans for the management of migraine". Drugs 70 (12): 1505–18. doi:10.2165/11537990-000000000-00000. PMID 20687618.
- ^ Tepper Stewart J., S. J.; Tepper, Deborah E. (April 2010). "Breaking the cycle of medication overuse headache". Cleveland Clinic Journal of Medicine 77 (4): 236–42. doi:10.3949/ccjm.77a.09147. PMID 20360117.
- ^ Colman I, Friedman BW, Brown MD et al. (June 2008). "Parenteral dexamethasone for acute severe migraine headache: meta-analysis of randomised controlled trials for preventing recurrence". BMJ 336 (7657): 1359–61. doi:10.1136/bmj.39566.806725.BE. PMC 2427093. PMID 18541610. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2427093.
- ^ "4.7.4.1 Treatment of acute migraine". British National Formulary (55 ed.). March 2008. p. 239.
- ^ a b Etminan, M, Takkouche, B, Isorna, FC, Samii, A (2005). "Risk of ischaemic stroke in people with migraine: Systematic review and meta-analysis of observational studies". BMJ 330 (7482): 63. doi:10.1136/bmj.38302.504063.8F. PMC 543862. PMID 15596418. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=543862.
- ^ a b Kurth, T; Kurth T, Gaziano JM, Cook NR, Logroscino G, Diener HC, Buring JE (2006). "Migraine and risk of cardiovascular disease in women". JAMA 296 (3): 283–91. doi:10.1001/jama.296.3.283. PMID 16849661.
- ^ "Headache and Combination Estrogen-Progestin Oral Contraceptives:: Case 2". medscape.com. http://www.medscape.com/viewarticle/501953_3. Retrieved 2011-05-30.
- ^ Becker, C, Brobert, GP, Almqvist, PM, Johansson, S, Jick, SS, Meier, CR (2007). "Migraine and the risk of stroke, TIA, or death in the UK (CME)". Headache 47 (10): 1374–84. doi:10.1111/j.1526-4610.2007.00937.x. PMID 18052947.
- ^ Waters, WE, Campbell, MJ, Elwood, PC (November 1983). "Migraine, headache, and survival in women". British medical journal (Clinical research ed.) 287 (6403): 1442–3. doi:10.1136/bmj.287.6403.1442. PMC 1549656. PMID 6416449. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1549656.
- ^ Mortimer MJ, Kay J, Jaron A (1992). "Epidemiology of headache and childhood migraine in an urban general practice using Ad Hoc, Vahlquist and IHS criteria". Dev Med Child Neurol 34 (12): 1095–101. doi:10.1111/j.1469-8749.1992.tb11423.x. PMID 1451940.
- ^ Linet MS, Stewart WF, Celentano DD, Ziegler D, Sprecher M (1989). "An epidemiologic study of headache among adolescents and young adults". JAMA 261 (15): 2211–6. doi:10.1001/jama.261.15.2211. PMID 2926969.
- ^ Ziegler DK, Hassanein RS, Couch JR (1977). "Characteristics of life headache histories in a nonclinic population". Neurology 27 (3): 265–9. PMID 557763.
- ^ SELBY G, LANCE JW (1960). "Observations on 500 cases of migraine and allied vascular headache". J. Neurol. Neurosurg. Psychiatr. 23: 23–32. doi:10.1136/jnnp.23.1.23. PMC 495326. PMID 14444681. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=495326.
- ^ a b Anttila P, Metsähonkala L, Sillanpää M (2006). "Long-term trends in the incidence of headache in Finnish schoolchildren". Pediatrics 117 (6): e1197–201. doi:10.1542/peds.2005-2274. PMID 16740819.
- ^ a b c Lipton RB, Stewart WF (1993). "Migraine in the United States: a review of epidemiology and health care use". Neurology 43 (6 Suppl 3): S6–10. PMID 8502385.
- ^ a b Rasmussen BK, Olesen J (1992). "Migraine with aura and migraine without aura: an epidemiological study". Cephalalgia 12 (4): 221–8; discussion 186. doi:10.1046/j.1468-2982.1992.1204221.x. PMID 1525797.
- ^ Steiner TJ, Scher AI, Stewart WF, Kolodner K, Liberman J, Lipton RB (2003). "The prevalence and disability burden of adult migraine in England and their relationships to age, sex and ethnicity". Cephalalgia 23 (7): 519–27. doi:10.1046/j.1468-2982.2003.00568.x. PMID 12950377.
- ^ Bigal ME, Liberman JN, Lipton RB (2006). "Age-dependent prevalence and clinical features of migraine". Neurology 67 (2): 246–51. doi:10.1212/01.wnl.0000225186.76323.69. PMID 16864816.
- ^ Stewart WF, Linet MS, Celentano DD, Van Natta M, Ziegler D (1991). "Age- and sex-specific incidence rates of migraine with and without visual aura". Am. J. Epidemiol. 134 (10): 1111–20. PMID 1746521.
- ^ Wang SJ (2003). "Epidemiology of migraine and other types of headache in Asia". Curr Neurol Neurosci Rep 3 (2): 104–8. doi:10.1007/s11910-003-0060-7. PMID 12583837.
- ^ Lavados PM, Tenhamm E (1997). "Epidemiology of migraine headache in Santiago, Chile: a prevalence study". Cephalalgia 17 (7): 770–7. doi:10.1046/j.1468-2982.1997.1707770.x. PMID 9399008.
- ^ Ottman R, Lipton RB (1994). "Comorbidity of migraine and epilepsy". Neurology 44 (11): 2105–10. PMID 7969967.
- ^ a b c Arulmani, U., "Calcitonin Gene-Related Peptide and Migraine: Implications for Therapy" (2004). Doctoral thesis, Erasmus University. Web-link.
- ^ Brothwell, Don R. (1963). Digging up Bones; the Excavation, Treatment and Study of Human Skeletal Remains. London: British Museum (Natural History). p. 126. ISBN 0565007041. OCLC 14615536.
- ^ Edmeads J (1991). "What is migraine? Controversy and stalemate in migraine pathophysiology". J. Neurol. 238 (Suppl 1): S2–5. doi:10.1007/BF01642898. PMID 2045827.
- ^ Shevel E (2011). "The extracranial vascular theory of migraine: an artificial controversy". J Neural Transm Jan 5 (4): 525–30. doi:10.1007/s00702-010-0517-1. PMID 21207080.
- ^ "Cost of disorders of the brain in Europe" (PDF). http://www.sinapsa.org/Osnova/Materiali/Cost-paper-EBC.pdf. Retrieved 2011-05-30.
- ^ Tepper SJ, Stillman MJ (September 2008). "Clinical and preclinical rationale for CGRP-receptor antagonists in the treatment of migraine". Headache 48 (8): 1259–68. doi:10.1111/j.1526-4610.2008.01214.x. PMID 18808506.
- ^ "Migraine cause 'identified' as genetic defect". BBC News. 2010-09-27. http://www.bbc.co.uk/news/health-11408113.
External links
- Migraine at the Open Directory Project
- Migraine Information from the US National Institute of Neurological Disorders and Stroke
- Diagnostic criteriaPDF (1.21 MB)
- World Headache Alliance
- Migraine Aura Foundation
CNS disease: Headache (G43–G44, 339, 346) Primary ICHD 1ICHD 2ICHD 3ICHD 4Secondary ICHD 7ICHD 8ICHD 13 Other Antimigraine preparations (N02C) Analgesic/abortive Serotonin modulatorsErgot alkaloidsTriptans (Almotriptan, Avitriptan, Eletriptan, Frovatriptan, Naratriptan, Rizatriptan, Sumatriptan, Zolmitriptan) AlniditanOtherOtherPrevention of migraines Ungrouped Categories:- Headaches
- Migraine





Wikimedia Foundation. 2010.