- Trigeminal neuralgia
Infobox_Disease
Name = Trigeminal neuralgia
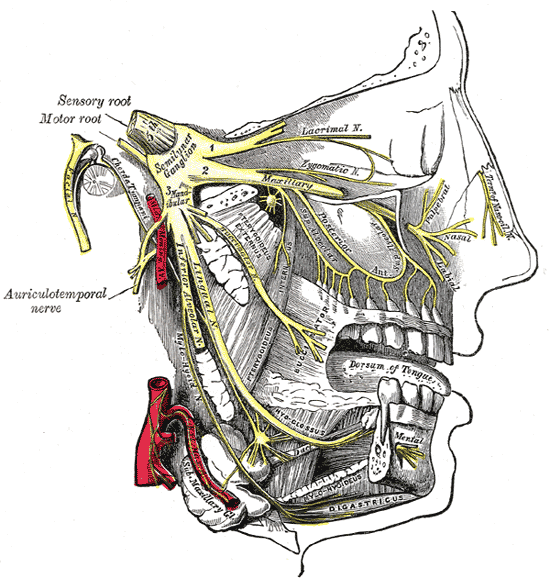
Caption = Detailed view of trigeminal nerve, shown in yellow.
DiseasesDB = 13363
ICD10 = ICD10|G|50|0|g|50
ICD9 = ICD9|350.1
ICDO =
OMIM =
MedlinePlus =
eMedicineSubj = emerg
eMedicineTopic = 617
MeshID = D014277Trigeminal neuralgia (TN), or "Tic Doloureux", (also known as prosopalgia) is a neuropathic disorder of the
trigeminal nerve that causes episodes of intensepain in the eyes, lips, nose, scalp, forehead, and jaw. [cite journal |author=Bayer DB, Stenger TG |title=Trigeminal neuralgia: an overview |journal=Oral Surg. Oral Med. Oral Pathol. |volume=48 |issue=5 |pages=393–9 |year=1979 |pmid=226915|doi=10.1016/0030-4220(79)90064-1] It is estimated that 1 in 15,000 people suffer from trigeminal neuralgia, although those numbers may be significantly higher due to frequent misdiagnosis. TN usually develops after the age of 50, more commonly in females, although there have been cases with patients being as young as three years of age [cite web | last = Bloom | first = R | title = Emily Garland: A young girl's painful problem took more than a year to diagnose | url = http://www.tna-support.org/newlook/sgl_files/library/newsletters/middletenn/2005%20November-December%20web%20pages.pdf | format = PDF] .The condition can bring about stabbing, mind-numbing, electric shock-like pain from just a finger's glance of the cheek. It is among the most severe types of pain known.Refimprove|date=September 2008 The most common forms of TN affect 1 in 15,000 to 20,000, but 1 in 5,000 are thought to suffer from some type of facial pain.
About
The pain of trigeminal neuralgia is often falsely attributed to a pathology of dental origin. "Rarely do patients come to the surgeon without having many removed, and not infrequently all, teeth on the affected side or both sides." [cite book |last= Dandy|first=Sir Walter |authorlink=Walter Dandy |title=The Brain |edition=Special edition |series=The Classics of Neurology and Neurosurgery |year=1987 |month= |publisher=Gryphon editions |location=Birmingham |pages=179 ] Extractions do not help. The pain is originating in the trigeminal nerve and not in an individual nerve of a tooth. Because of this difficulty, many patients may go untreated for long periods of time before a correct diagnosis is made.The trigeminal nerve is the fifth
cranial nerve , a mixed cranial nerve responsible for sensory data such astactition (pressure),thermoception (temperature), andnociception (pain) originating from the face above the jawline; it is also responsible for the motor function of the muscles of mastication, the muscles involved in chewing but not facial expression. Several theories exist to explain the possible causes of thispain syndrome. Leading research indicates that it is a blood vessel compressing the trigeminal nerve near its connection with the pons. Thesuperior cerebellar artery . Such a compression can injure the nerve's protective myelin sheath and cause erratic and hyperactive functioning of the nerve. This can lead to pain attacks at the slightest stimulation of any area served by the nerve as well as hinder the nerve's ability to shut off the pain signals after the stimulation ends. This type of injury may rarely be caused by ananeurysm (an outpouching of ablood vessel ); by atumor ; by anarachnoid cyst in thecerebellopontine angle [cite journal |author=Babu R, Murali R |title=Arachnoid cyst of the cerebellopontine angle manifesting as contralateral trigeminal neuralgia: case report |journal=Neurosurgery |volume=28 |issue=6 |pages=886–7 |year=1991 |pmid=2067614 |doi= |url=] ; or by a traumatic event such as a car accident or even atongue piercing . [http://www.theglobeandmail.com/servlet/story/RTGAM.20061017.wtongues1017/BNStory/specialScienceandHealth/home] Two to four percent of patients with TN, usually younger, have evidence ofmultiple sclerosis , which may damage either the trigeminal nerve or other related parts of the brain. When there is no structural cause, the syndrome is calledidiopathic .Postherpetic Neuralgia , which occurs aftershingles , may cause similar symptoms if the trigeminal nerve is affected.ymptoms
The episodes of pain may occur
paroxysm ally. To describe the pain sensation, patients describe a trigger area on the face, so sensitive that touching or even air currents can trigger an episode of pain. It affects lifestyle as it can be triggered by common activities in a patient's daily life, such as eating, talking, shaving and toothbrushing. The attacks are said to feel like stabbingelectric shock s, burning, pressing or shooting pain that becomes intractable. Individual attacks affect one side of the face at a time, last several seconds, hours or longer, and repeat up to hundreds of times throughout the day. The pain also tends to occur in cycles with completeremission s lasting months or even years. 10-12% of cases are bilateral, or occurring on both sides. This normally indicates problems with both trigeminal nerves since one serves strictly the left side of the face and the other serves the right side. Pain attacks typically worsen in frequency or severity over time. A great deal of patients develop the pain in one branch, then over years the pain will travel through the other nerve branches.Signs of this can be seen in males who may deliberately miss an area of their face when shaving, in order to avoid triggering an episode. Although 60% of the time trigeminal neuralgia is not fatal,Dubious|date=September 2008 successive recurrences may be incapacitating, and the fear of provoking an attack may make sufferers reluctant to engage in normal activities.
There is a variant of trigeminal neuralgia called
atypical trigeminal neuralgia . In some cases of atypical trigeminal neuralgia, the sufferer experiences a severe, relentless underlying pain similar to a migraine in addition to the stabbing pains. This variant is sometimes called "trigeminal neuralgia, type 2" [cite web |url=http://www.ohsu.edu/facialpain/facial_pain-dx.shtml |title=Neurological Surgery - Facial Pain |format= |publisher=Oregon Health & Science University |accessdate=] , based on a recent classification of facial pain [cite journal |author=Burchiel KJ |title=A new classification for facial pain |journal=Neurosurgery |volume=53 |issue=5 |pages=1164–6; discussion 1166–7 |year=2003 |pmid=14580284 |doi= |url=http://meta.wkhealth.com/pt/pt-core/template-journal/lwwgateway/media/landingpage.htm?issn=0148-396X&volume=53&issue=5&spage=1164] . In other cases, the pain is stabbing and intense, but may feel like burning or prickling, rather than a shock. Sometimes, the pain is a combination of shock-like sensations,migraine -like pain, and burning or prickling pain. It can also feel as if a boring piercing pain is unrelenting. Some recent studies suggest that ATN may be an early development of Trigeminal Neuralgia.Treatment
There is no cure for trigeminal neuralgia, but most people find relief from medication, from one of the five surgical options or sometimes from one of the many complementary or alternative therapies. Atypical trigeminal neuralgia, which involves a more constant and burning pain, is more difficult to treat, both with medications and surgery. Surgery may result in varying degrees of numbness to the patient and lead occasionally to "anesthesia dolorosa," which is numbness with intense pain. However, some people do find dramatic relief with minimal side effects from the various surgeries that are now available. [cite journal | last = Weigel | first = G | coauthors = Casey, K. | title = Striking Back: The Trigeminal Neuralgia and Face Pain Handbook | journal = Trigeminal Neuralgia Association ISBN 0-9672393-2-X | year = 2004 ]
There are some things that a patient can do to minimize the frequency and intensity of TN attacks:
* Apply ice packs or any readily available source of cold to the area of pain. Cold often numbs the area and will reduce the pain. Fact|date=November 2007
*Warming packs, wrapped in a towel to protect one's skin, can also provide relief as they stimulate blood flow to the area they are placed upon.
* Get adequate rest in normal rest cycles.
* Manage your stress well and keep stress levels low. When you feel a TN attack coming on, try to relax immediately.
* Practice healthy living principles such as diet and exercise.
*Avoid foods that may act as nerve stimulants, such as coffee, tea, and foods that are high in sugar.
*Maintain adequate hydration and electrolyte levels at all time.Common hurdles to receiving treatment
Due to the rarity of TN, many physicians and dentists are unfamiliar with the affliction's symptoms. As a result, TN is often misdiagnosed. A TN sufferer will often seek the help of numerous clinicians prior to a firm diagnosis being made.
Those physicians that do have experience with TN, are hesitant to treat patients that do not fit the classical symptoms of a TN sufferer. Patients under the age of 30 are particularly at risk of not receiving proper medical attention, as many practitioners falsely believe that one must be in the later years in order for TN to strike.
There is some evidence that points towards the need to quickly treat and diagnose TN. It is thought that the longer a patient suffers from TN, the harder it may be to reverse the neural pathways, associated with that pain. Therefore it is essential that physicians are made aware of the seriousness of TN, and the level of pain that their patient is in.
Dentists that suspect TN should proceed in the most conservative manner possible, and should ensure that all tooth structures are "truly" compromised prior to extractions or procedures being performed.
Due to the hurdles listed above, it is essential for patients who believe they are suffering from TN to seek the advice of a TN specialist or neurologist, if they find their primary care physician to be dismissive of their pain.
Medications
*
Anticonvulsant s such ascarbamazepine ,oxcarbazepine ,topiramate ,phenytoin , orgabapentin are generally the most effective medications. Generally speaking, opiate based analgesics offer little relief from TN attacks, but may decrease the pain sensation that is experienced by the patient. Anticonvulsant effects may be potentiated with moderate to high levels of adjuvant therapies such asbaclofen and/orclonazepam .Baclofen may also help some patients eat more normally if jaw movement tends to aggravate the symptoms.
* If anticonvulsants do not help and surgical options have failed or are ruled out, the pain may be treated long-term with anopioid such asmethadone ,oxycodone orDuragesic in patch form.
* Low doses of someantidepressant s are thought to be effective in treating neuropathic pain, but a tremendous amount of controversy exists on this topic, and their use is often limited to treating the depression that is associated with chronic pain, rather than the actual sensation of pain from the trigeminal nerve.
*Botox can be injected into the nerve by a physician, and has been found helpful using the "migraine" pattern adapted to the patient's special needs.
*TGN patients may also find relief by having their neurologist implant a neuro-stimulator.Many patients cannot tolerate medications for years, and an alternate treatment is to take a drug such asgabapentin and place it in an externally applied cream base by a pharmacist who compounds drugs. Also helpful is taking a "drug holiday" when remissions occur and rotating medications if one becomes ineffective.urgery
Surgery may be recommended, either to relieve the pressure on the nerve or to selectively damage it in such a way as to disrupt pain signals from getting through to the brain. In trained hands, surgical success rates have been reported to have initial success rates approaching 90 percent. Some patients require followup procedures to be performed, however, if a recurrence of their pain begins.
Of the five surgical options, the
microvascular decompression is the only one aimed at fixing the presumed cause of the pain. In this procedure, the surgeon enters the skull through a 25mm (one-inch) hole behind the ear. The nerve is then explored for an offending blood vessel, and when one is found, the vessel and nerve are separated or "decompressed" with a small pad, usually made out of gore-tex. When successful, MVD procedures can give permanent pain relief with little to no facial numbness.Three other procedures use needles or catheters that enter through the face into the opening where the nerve first splits into its three divisions. Excellent success rates using a cost effective
percutaneous surgical procedure known as balloon compression have been reported [cite journal | last = Natarajan | first = M | title = Percutaneous trigeminal ganglion balloon compression: experience in 40 patients | journal = Neurology (Neurological Society of India) | year = 2000 | volume = 48 | issue = 4 | pages = 330–2 | pmid = 11146595] . This technique has been helpful in treating the elderly for whom surgery may not be an option due to coexisting health conditions. Balloon compression is also the best choice for patients who haveophthalmic nerve pain or have experienced recurrent pain aftermicrovascular decompression .Similar success rates have been reported with glycerol injections and radiofrequency rhizotomies. Glycerol injections involve injecting an alcohol-like substance into the cavern that bathes the nerve near its junction. This liquid is corrosive to the nerve fibers and can mildly injure the nerve enough to hinder the errant pain signals. In a radiofrequency rhizotomy, the surgeon uses an electrode to heat the selected division or divisions of the nerve. Done well, this procedure can target the exact regions of the errant pain triggers and disable them with minimal numbness.
tereotactic Radiation Therapy
The nerve can also be damaged to prevent pain signal transmission using
Gamma Knife or a linear accelerator-based radiation therapy (e.g. Novalis, Cyberknife). No incisions are involved in this procedure. It uses radiation to bombard the nerve root, this time targeting the selective damage at the same point where vessel compressions are often found. This option is used especially for those people who are medically unfit for a long general anaesthetic, or who are taking medications for prevention of blood clotting (e.g.,warfarin ,heparin ,asperin ). A prospective Phase I trial performed at Marseille, France, showed that 83% of patients were pain-free at 12 months, with 58% pain-free and off all medications. Side effects were mild, with 6% experiencing mild tingling and 4% experiencing mild numbness.cite journal |author=Régis J, Metellus P, Hayashi M, Roussel P, Donnet A, Bille-Turc F |title=Prospective controlled trial of gamma knife surgery for essential trigeminal neuralgia |journal=J. Neurosurg. |volume=104 |issue=6 |pages=913–24 |year=2006 |pmid=16776335 |doi=]ocial consequences of Trigeminal Neuralgia
Most suffers of TN do not present with any outwardly noticeable symptoms, though some will exhibit brief facial spasms during an attack. As a result, it is often difficult for friends and family members of TN suffers to accept that their loved one, who was previously healthy is now suffering from intractable pain.
That doubt can be a great hindrance to the support of the patient, as friends and family, as well as physicians will often seek a psychological root cause rather than a physiological abnormality.
That is especially true of those suffering from Atypical TN, who may not present with any compression of the TN, with the complaint of severe pain (constant electric-like shocks, constant crushing or pressure sensations, or a constant severe dull ache) being the sole criteria of a diagnosis.
Many TN sufferers are confined to their homes or are unable to work due to the frequency of their attacks. It is important for friends and family to educate themselves on the severity of TN pain, and to be understanding of limitations TN places upon its sufferer. Though, at the same time the TN patient must be extremely proactive in furthering their rehabilitative efforts. Enrolling themselves in a chronic pain support group, or seeking one-on-one counseling, can help teach a TN patient how to adapt to their newfound affliction.
As with any chronic pain syndrome, TN not being the exception, depression has the potential to set in. Friends and family, as well as clinicians, must be alert to the signs of a rapid change in behavior, and should take appropriate measures when necessary. It must be constantly reinforced to the sufferer of TN, that treatment options do exist.
Other
In one case of trigeminal neuralgia associated with tongue-piercing, the condition resolved after the jewelry was removed. [cite journal | last = Gazzeri | first = R | coauthors = Mercuri, S. & Galarza M. | title = Atypical trigeminal neuralgia associated with tongue piercing | journal = JAMA | year = 2006 | volume = 296 | issue = 15 | pages = 1840–1 | pmid = 17047213 | doi = 10.1001/jama.296.15.1840-b]
Some patients have reported a correlation between dental work and the onset of their trigeminal nerve pain.
Recently, some researchers have investigated the link between neuropathatic pain, such as TN, and celiac disease.
Interestingly, most patients have a complete abatement of their TN symptoms during sleep and within the first few minutes of waking; the physiological basis of this phenomenon is not fully understood at this time.
References
External links
* [http://www.tna-support.org/ Trigeminal Neuralgia Association]
* [http://www.kgeh.com/kgBrainSpine/aboutsurgery.html About surgery for trigeminal neuralgia]
* [http://www.umanitoba.ca/centres/cranial_nerves/trigeminal_neuralgia/manuscript/ Your Complete Guide to Trigeminal Neuralgia]
* [http://www.marioizurieta.com/en/neuralgia.htm Trigeminal Neuralgia Treatment]
*
*cite web |url=http://facial-neuralgia.org/conditions/tn.html |title=Trigeminal Neuralgia |format= |work=Facial Neuralgia Resources |accessdate=
*cite web |url=http://www.fpa-support.org/ |title=Trigeminal Neuralgia Association |format= |work= |accessdate=
Wikimedia Foundation. 2010.