- Dementia
-
For other uses, see Dementia (disambiguation).
Dementia Classification and external resources ICD-10 F00-F07 ICD-9 290-294 DiseasesDB 29283 MedlinePlus 000739 MeSH D003704 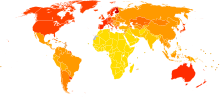 Disability-adjusted life year for Alzheimer and other dementias per 100,000 inhabitants in 2002.
Disability-adjusted life year for Alzheimer and other dementias per 100,000 inhabitants in 2002. no data≤ 5050-7070-9090-110110-130130-150150-170170-190190-210210-230230-250≥ 250
no data≤ 5050-7070-9090-110110-130130-150150-170170-190190-210210-230230-250≥ 250Dementia (taken from Latin, originally meaning "madness", from de- "without" + ment, the root of mens "mind") is a serious loss of cognitive ability in a previously unimpaired person, beyond what might be expected from normal aging. It may be static, the result of a unique global brain injury, or progressive, resulting in long-term decline due to damage or disease in the body. Although dementia is far more common in the geriatric population, it can occur before the age of 65, in which case it is termed "early onset dementia".[1]
Dementia is not a single disease, but rather a non-specific illness syndrome (i.e., set of signs and symptoms) in which affected areas of cognition may be memory, attention, language, and problem solving. It is normally required to be present for at least 6 months to be diagnosed;[2] cognitive dysfunction that has been seen only over shorter times, in particular less than weeks, must be termed delirium. In all types of general cognitive dysfunction, higher mental functions are affected first in the process.
Especially in the later stages of the condition, affected persons may be disoriented in time (not knowing what day of the week, day of the month, or even what year it is), in place (not knowing where they are), and in person (not knowing who they, or others around them, are). Dementia, though often treatable to some degree, is usually due to causes that are progressive and incurable.[citation needed]
Symptoms of dementia can be classified as either reversible or irreversible, depending upon the etiology of the disease. Less than 10% of cases of dementia are due to causes that may presently be reversed with treatment. Causes include many different specific disease processes, in the same way that symptoms of organ dysfunction such as shortness of breath, jaundice, or pain are attributable to many etiologies.
Without careful assessment of history, the short-term syndrome of delirium (often lasting days to weeks) can easily be confused with dementia, because they have all symptoms in common, save duration. Some mental illnesses, including depression and psychosis, may produce symptoms that must be differentiated from both delirium and dementia.[3]
There are many specific types (causes) of dementia, often showing slightly different symptoms. However, the symptom overlap is such that it is impossible to diagnose the type of dementia by symptomatology alone, and in only a few cases are symptoms enough to give a high probability of some specific cause. Diagnosis is therefore aided by nuclear medicine brain scanning techniques. Certainty cannot be attained except with brain biopsy during life, or at necropsy in death.
Some of the most common forms of dementia are: Alzheimer's disease, vascular dementia, frontotemporal dementia, semantic dementia and dementia with Lewy bodies. It is possible for a patient to exhibit two or more dementing processes at the same time, as none of the known types of dementia protects against the others.
Contents
History
Main articles: Dementia praecox and Alzheimer's diseaseUp to the end of the 19th century, dementia was a much broader clinical concept, which included mental illness and any type of psychosocial incapacity, including those which could be reversed.[4] Dementia at this time simply referred to anyone who had lost the ability to reason, and was applied equally to psychosis of mental illness, "organic" diseases like syphilis which could destroy the brain, and to the dementia associated with old age, which was held to be caused by "hardening of the arteries."
Dementia when seen in the elderly was called senile dementia or senility and viewed as a normal and somewhat inevitable aspect of growing old, rather than as being caused by any specific diseases. At the same time, in 1907, a specific organic dementing process of early onset, called Alzheimer's disease, had been described. This was associated with particular microscopic changes in the brain, but was seen as a rare disease of middle age.
Much like other diseases associated with aging, dementia was rare before the 20th century, although by no means unknown, due to the fact that people seldom lived long enough to experience it.
By the period of 1913-20, schizophrenia had been well-defined in a way similar to today, and also the term dementia praecox had been used to suggest the development of senile-type dementia at a younger age. Eventually the two terms fused, so that until 1952 physicians used the terms dementia praecox ("precocious dementia") and schizophrenia interchangeably. The term "precocious dementia" for a mental illness suggested that a type of mental illness like schizophrenia (including paranoia and decreased cognitive capacity) could be expected to arrive normally in all persons with greater age (see paraphrenia). At the same time, the beginning use of dementia to describe both what we know understand as schizophrenia and senile dementia, after about 1920, acted to give the word "dementia" a more limited role, as one of describing a type of permanent mental deterioration which was not expected to be reversible. This is the beginning of the more recognizable use of the term today.
In 1976, neurologist Robert Katzmann suggested a link between "senile dementia" and Alzheimer's disease.[5] Katzmann suggested that much of the senile dementia occurring (by definition) after the age of 65, was pathologically identical with Alzheimer's disease occurring before age 65 and therefore should not be treated differently. He noted that the fact the "senile dementia" was not considered a disease, but rather part of aging, and this fact was keeping millions of aged patients with what otherwise was identical with Alzheimer's disease, from being diagnosed as having a disease process, rather than simply considered as aging normally.[6] Katzmann thus suggested that Alzheimer's disease, if taken to occur over age 65, is actually common, not rare, and was the 4th or 5th leading cause of death, even though rarely being reported on death certificates in 1976.
This suggestion opened the view that dementia is never normal, and must always be the result of a particular disease process, and is not part of the normal healthy aging process, per se. The ensuing debate led for a time to the proposed disease diagnosis of "senile dementia of the Alzheimer's type" (SDAT) in persons over the age of 65, with "Alzheimer's disease" diagnosed in persons younger than 65 who had the same pathology. Eventually, however, it was agreed that the age limit was artificial, and that Alzheimer's disease was the appropriate term for persons with the particular brain pathology seen in this disease, regardless of the age of the sufferer. A helpful finding was that although the incidence of Alzheimer's disease increased with age (from 5-10% of 75-year-olds to as many as 40-50% of 90-year-olds), there was no age at which all persons developed it, so it was not an inevitable consequence of aging, no matter how great an age a person attained.
Also, after 1952, mental illnesses like schizophrenia were removed from the category of "organic brain syndromes," and thus (by definition) removed from possible causes of "dementing illnesses" (dementias). At the same, however, the traditional cause of senile dementia – "hardening of the arteries" – now returned as a set of dementias of vascular cause (small strokes). These were now termed "multi-infarct dementias" or vascular dementias.
In the 21st century, a number of other types of dementia have been differentiated from Alzheimer's disease and vascular dementias (these two being the most common types). This differentiation is on the basis of pathological examination of brain tissues, symptomatology, and by different patterns of brain metabolic activity in nuclear medical imaging tests such as SPECT and PET scans of the brain. The various forms of dementia have differing prognoses (expected outcome of illness), and also differing sets of epidemologic risk factors. The causal etiology of many of them, including Alzheimer's disease, remains unknown, although many theories exist such as accumulation of protein plaques as part of normal aging, inflammation, inadequate blood sugar, and traumatic brain injury.
Signs and symptoms
Comorbidities
Dementia is not merely a problem of memory. It reduces the ability to learn, reason, retain or recall past experience and there is also loss of patterns of thoughts, feelings and activities (Gelder et al. 2005). Additional mental and behavioral problems often affect people who have dementia, and may influence quality of life, caregivers, and the need for institutionalization. As dementia worsens individuals may neglect themselves and may become disinhibited and may become incontinent. (Gelder et al. 2005).
Depression affects 20–30% of people who have dementia, and about 20% have anxiety.[7] Psychosis (often delusions of persecution) and agitation/aggression also often accompany dementia. Each of these needs to be assessed and treated independent of the underlying dementia.[8]
Risk to self and others
The Canadian Medical Association Journal has reported that driving with dementia could lead to severe injury or even death to self and others. Doctors should advise appropriate testing on when to quit driving.[9]
In the United States, Florida's Baker Act allows law enforcement and the judiciary to force mental evaluation for those suspected of suffering from dementia or other mental incapacities.[citation needed]
In the United Kingdom, as with all mental disorders, where a sufferer could potentially be a danger to themselves or others, they can be detained under the Mental Health Act of 1983 for the purposes of assessment, care and treatment. This is a last resort, and usually avoided if the patient has family or friends who can ensure care.
The United Kingdom DVLA (Driving & Vehicle Licensing Agency) states that dementia sufferers who specifically suffer with poor short term memory, disorientation, lack of insight or judgment are almost certainly not fit to drive—and in these instances, the DVLA must be informed so said license can be revoked. They do however acknowledge low-severity cases and early sufferers, and those drivers may be permitted to drive pending medical report.
Behaviour may be disorganized, restless or inappropriate. Some people become restless or wander about by day and sometimes at night. When people suffering from dementia are put in circumstances beyond their abilities, there may be a sudden change to tears or anger (a "catastrophic reaction").[10]
Causes
Fixed cognitive impairment
Various types of brain injury, occurring as a single event, may cause irreversible but fixed cognitive impairment. Traumatic brain injury may cause generalized damage to the white matter of the brain (diffuse axonal injury), or more localized damage (as also may neurosurgery). A temporary reduction in the brain's supply of blood or oxygen may lead to hypoxic-ischemic injury. Strokes (ischemic stroke, or intracerebral, subarachnoid, subdural or extradural hemorrhage) or infections (meningitis and/or encephalitis) affecting the brain, prolonged epileptic seizures and acute hydrocephalus may also have long-term effects on cognition. Excessive alcohol use may cause alcohol dementia, Wernicke's encephalopathy and/or Korsakoff's psychosis, and certain other recreational drugs may cause substance-induced persisting dementia; once overuse ceases, the cognitive impairment is persistent but not progressive.
Slowly progressive dementia
Dementia which begins gradually and worsens progressively over several years is usually caused by neurodegenerative disease; that is, by conditions affecting only or primarily the neurons of the brain and causing gradual but irreversible loss of function of these cells. Less commonly, a non-degenerative condition may have secondary effects on brain cells, which may or may not be reversible if the condition is treated.
The causes of dementia depend on the age at which symptoms begin. In the elderly population (usually defined in this context as over 65 years of age), a large majority of cases of dementia are caused by Alzheimer's disease, vascular dementia or both. Dementia with Lewy bodies is another fairly common cause, which again may occur alongside either or both of the other causes.[11][12][13] Hypothyroidism sometimes causes slowly progressive cognitive impairment as the main symptom, and this may be fully reversible with treatment. Normal pressure hydrocephalus, though relatively rare, is important to recognize since treatment may prevent progression and improve other symptoms of the condition. However, significant cognitive improvement is unusual.
Dementia is much less common under 65 years of age. Alzheimer's disease is still the most frequent cause, but inherited forms of the disease account for a higher proportion of cases in this age group. Frontotemporal lobar degeneration and Huntington's disease account for most of the remaining cases.[14] Vascular dementia also occurs, but this in turn may be due to underlying conditions (including antiphospholipid syndrome, CADASIL, MELAS, homocystinuria, moyamoya and Binswanger's disease). People who receive frequent head trauma, such as boxers or football players, are at risk of chronic traumatic encephalopathy[15] (also called dementia pugilistica in boxers).
In young adults (up to 40 years of age) who were previously of normal intelligence, it is very rare to develop dementia without other features of neurological disease, or without features of disease elsewhere in the body. Most cases of progressive cognitive disturbance in this age group are caused by psychiatric illness, alcohol or other drugs, or metabolic disturbance. However, certain genetic disorders can cause true neurodegenerative dementia at this age. These include familial Alzheimer's disease, SCA17 (dominant inheritance); adrenoleukodystrophy (X-linked); Gaucher's disease type 3, metachromatic leukodystrophy, Niemann-Pick disease type C, pantothenate kinase-associated neurodegeneration, Tay-Sachs disease and Wilson's disease (all recessive). Wilson's disease is particularly important since cognition can improve with treatment.
At all ages, a substantial proportion of patients who complain of memory difficulty or other cognitive symptoms are suffering from depression rather than a neurodegenerative disease. Vitamin deficiencies and chronic infections may also occur at any age; they usually cause other symptoms before dementia occurs, but occasionally mimic degenerative dementia. These include deficiencies of vitamin B12, folate or niacin, and infective causes including cryptococcal meningitis, HIV, Lyme disease, progressive multifocal leukoencephalopathy, subacute sclerosing panencephalitis, syphilis and Whipple's disease.
Rapidly progressive dementia
Creutzfeldt-Jakob disease typically causes a dementia which worsens over weeks to months, being caused by prions. The common causes of slowly progressive dementia also sometimes present with rapid progression: Alzheimer's disease, dementia with Lewy bodies, frontotemporal lobar degeneration (including corticobasal degeneration and progressive supranuclear palsy).
On the other hand, encephalopathy or delirium may develop relatively slowly and resemble dementia. Possible causes include brain infection (viral encephalitis, subacute sclerosing panencephalitis, Whipple's disease) or inflammation (limbic encephalitis, Hashimoto's encephalopathy, cerebral vasculitis); tumors such as lymphoma or glioma; drug toxicity (e.g. anticonvulsant drugs); metabolic causes such as liver failure or kidney failure; and chronic subdural hematoma.
Dementia as a feature of other conditions
There are many other medical and neurological conditions in which dementia only occurs late in the illness, or as a minor feature. For example, a proportion of patients with Parkinson's disease develop dementia, though widely varying figures are quoted for this proportion.[citation needed] When dementia occurs in Parkinson's disease, the underlying cause may be dementia with Lewy bodies or Alzheimer's disease, or both.[16] Cognitive impairment also occurs in the Parkinson-plus syndromes of progressive supranuclear palsy and corticobasal degeneration (and the same underlying pathology may cause the clinical syndromes of frontotemporal lobar degeneration). Chronic inflammatory conditions of the brain may affect cognition in the long term, including Behçet's disease, multiple sclerosis, sarcoidosis, Sjögren's syndrome and systemic lupus erythematosus. Although the acute porphyrias may cause episodes of confusion and psychiatric disturbance, dementia is a rare feature of these rare diseases.[17]
Aside from those mentioned above, inherited conditions which may cause dementia alongside other features include:[18]
- Alexander disease
- Canavan disease
- Cerebrotendinous xanthomatosis
- DRPLA
- Fragile X-associated tremor/ataxia syndrome
- Glutaric aciduria type 1
- Krabbe's disease
- Maple syrup urine disease
- Niemann Pick disease type C
- Kufs' disease
- Neuroacanthocytosis
- Organic acidemias
- Pelizaeus-Merzbacher disease
- Urea cycle disorders
- Sanfilippo syndrome type B
- Spinocerebellar ataxia type 2
Diagnosis
Proper differential diagnosis between the types of dementia (cortical and subcortical) will require, at the least, referral to a specialist, e.g., a geriatric internist, geriatric psychiatrist, neurologist, neuropsychologist or geropsychologist.[citation needed] Duration of symptoms must evident for at least six months for a diagnosis of dementia or organic brain syndrome to be made (ICD-10).
Cognitive testing
Sensitivity and specificity of common tests for dementia Test Sensitivity Specificity Reference MMSE 71%-92% 56%-96% [19] 3MS 83%-93.5% 85%-90% [20] AMTS 73%-100% 71%-100% [20] There exist some brief tests (5–15 minutes) that have reasonable reliability and can be used in the office or other setting to screen cognitive status. Examples of such tests include the abbreviated mental test score (AMTS), the mini mental state examination (MMSE), Modified Mini-Mental State Examination (3MS),[21] the Cognitive Abilities Screening Instrument (CASI),[22] and the clock drawing test.[23] Scores must be interpreted in the context of the person's educational and other background, and the particular circumstances; for example, a person highly depressed or in great pain will not be expected to do well on many tests of mental ability.
While many tests have been studied,[24][25][26] and some may emerge as better alternatives to the MMSE, presently the MMSE is the best studied and most commonly used.
Another approach to screening for dementia is to ask an informant (relative or other supporter) to fill out a questionnaire about the person's everyday cognitive functioning. Informant questionnaires provide complementary information to brief cognitive tests. Probably the best known questionnaire of this sort is the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE).[27] On the other hand the General Practitioner Assessment Of Cognition combines both, a patient assessment and an informant interview. It was specifically designed for the use in the primary care setting and is also available as a web-based test.
Further evaluation includes retesting at another date, and administration of other tests of mental function.
Laboratory tests
Routine blood tests are also usually performed to rule out treatable causes. These tests include vitamin B12, folic acid, thyroid-stimulating hormone (TSH), C-reactive protein, full blood count, electrolytes, calcium, renal function, and liver enzymes. Abnormalities may suggest vitamin deficiency, infection or other problems that commonly cause confusion or disorientation in the elderly. The problem is complicated by the fact that these cause confusion more often in persons who have early dementia, so that "reversal" of such problems may ultimately only be temporary.[citation needed]
Testing for alcohol and other known dementia-inducing drugs may be indicated.
Imaging
A CT scan or magnetic resonance imaging (MRI scan) is commonly performed, although these modalities do not have optimal sensitivity for the diffuse metabolic changes associated with dementia in a patient that shows no gross neurological problems (such as paralysis or weakness) on neurological exam. CT or MRI may suggest normal pressure hydrocephalus, a potentially reversible cause of dementia, and can yield information relevant to other types of dementia, such as infarction (stroke) that would point at a vascular type of dementia.
The functional neuroimaging modalities of SPECT and PET are more useful in assessing long-standing cognitive dysfunction, since they have shown similar ability to diagnose dementia as a clinical exam.[28] The ability of SPECT to differentiate the vascular cause from the Alzheimer's disease cause of dementias, appears to be superior to differentiation by clinical exam.[29]
Recent research has established the value of PET imaging using carbon-11 Pittsburgh Compound B as a radiotracer (PIB-PET) in predictive diagnosis of various kinds of dementia, in particular Alzheimer's disease. Studies from Australia have found PIB-PET to be 86% accurate in predicting which patients with mild cognitive impairment would develop Alzheimer's disease within two years. In another study, carried out using 66 patients seen at the University of Michigan, PET studies using either PIB or another radiotracer, carbon-11 dihydrotetrabenazine (DTBZ), led to more accurate diagnosis for more than one-fourth of patients with mild cognitive impairment or mild dementia.[30]
Prevention
Main article: Prevention of dementiaA study done at the University of Bari in Italy, found that a group drinking alcoholic beverages moderately had a slower progression to dementia. In a group of 1,566 elderly Italians, 1,445 had no cognitive impairment and 121 had suffered mild cognitive impairment, the study found that that over the duration of 3.5 years the people with MCI who drank less than one alcoholic beverage a day progressed to dementia at a rate that was 85% slower then those who drank no alcoholic beverages. However, the authors of the study commented that since it was epidemiologic, the findings might only be a marker of lifestyle, showing that "moderate lifestyle" in general is associated with slower dementia-progression.[31]A study failed to show a conclusive link between high blood pressure and developing dementia. The study, published in the Lancet Neurology journal July 2008, found that blood pressure lowering medication did not reduce dementia but that meta analysis of the study data combined with other data suggested that further study could be warranted.[32]
Brain-derived neurotrophic factor (BDNF) expression is associated with some dementia types.[33][34][35]
A Canadian study found that a lifetime of bilingualism delays the onset of dementia by an average of four years when compared to monolingual patients.[36]
Management
Except for the treatable types listed above, there is no cure to this illness. Cholinesterase inhibitors are often used early in the disease course. Cognitive and behavioral interventions may also be appropriate. Educating and providing emotional support to the caregiver (or carer) is of importance as well (see also elderly care).
Pain and dementia
See also: Assessment in nonverbal patientsAs people age, they experience more health problems, and most health problems associated with aging carry a substantial burden of pain; so, between 25% and 50% of older adults experience persistent pain. Seniors with dementia experience the same prevalence of conditions likely to cause pain as seniors without dementia.[37] Pain is often overlooked in older adults and, when screened for, often poorly assessed, especially among those with dementia since they become incapable of informing others that they're in pain.[37][38] Beyond the issue of humane care, unrelieved pain has functional implications. Persistent pain can lead to decreased ambulation, depressed mood, sleep disturbances, impaired appetite and exacerbation of cognitive impairment,[38] and pain-related interference with activity is a factor contributing to falls in the elderly.[37][39]
Although persistent pain in the person with dementia is difficult to communicate, diagnose and treat, failure to address persistent pain has profound functional, psychosocial and quality of life implications for this vulnerable population. Health professionals often lack the skills and usually lack the time needed to recognize, accurately assess and adequately monitor pain in people with dementia.[37][40] Family members and friends can make a valuable contribution to the care of a person with dementia by learning to recognize and assess their pain. Educational resources (such as the Understand Pain and Dementia tutorial) and observational assessment tools are available.[37][41][42]
Medications
Currently, there are no medications that are clinically proven to be preventative or curative of dementia.[43] Although some medications are approved for use in the treatment of dementia, these treat the behavioural and cognitive symptoms of dementia, but have no effect on the underlying pathophysiology.[44]
- Acetylcholinesterase inhibitors: Tacrine (Cognex), donepezil (Aricept), galantamine (Razadyne), and rivastigmine (Exelon) are approved by the United States Food and Drug Administration (FDA) for treatment of dementia induced by Alzheimer's disease. They may be useful for other similar diseases causing dementia such as Parkinsons or vascular dementia.[44] Acetylcholinesterase inhibitors aim to increase the amount of the neurotransmitter acetylcholine, which is deficient in people with dementia.[45] This is done by inhibiting the action of the enzyme acetylcholinesterase, which breaksdown acetylcholine as part of normal brain function.[46] Though these medications are commonly prescribed, in a minority of patients these drugs can cause side effects including bradycardia and syncope.[47]
- N-methyl-D-aspartate (NMDA) receptor blockers: Memantine is marketed under several names by different pharmaceutical companies including: Abixa, Akatinol, Axura, Ebixa, Memox and Namenda.[48] In dementia, NMDA receptors are over-stimulated by glutamate, which creates problems for neurotransmission (and thus cognition) and also leads to damage to neurons through excitotoxicity. Memantine is thought to work by improving the “signal-to-noise” ratio and preventing excitotoxic damage.[49] Hence, due to their differing mechanisms of action memantine and acetylcholinesterase inhibitors can be used in combination with each other.[50][51]
Off label
- Amyloid deposit inhibitors: Minocycline and Clioquinoline, antibiotics, may help reduce amyloid deposits in the brains of persons with Alzheimer's disease.[52]
- Antidepressant drugs: Depression is frequently associated with dementia and generally worsens the degree of cognitive and behavioral impairment. Antidepressants effectively treat the cognitive and behavioral symptoms of depression in patients with Alzheimer's disease,[53] but evidence for their use in other forms of dementia is weak.[54]
- Anxiolytic drugs: Many patients with dementia experience anxiety symptoms. Although benzodiazepines like diazepam (Valium) have been used for treating anxiety in other situations, they are often avoided because they may increase agitation in persons with dementia and are likely to worsen cognitive problems or are too sedating. Buspirone (Buspar) is often initially tried for mild-to-moderate anxiety.[citation needed] There is little evidence for the effectiveness of benzodiazepines in dementia, whereas there is evidence for the effectivess of antipsychotics (at low doses).[55]
- Selegiline, a drug used primarily in the treatment of Parkinson's disease, appears to slow the development of dementia. Selegiline is thought to act as an antioxidant, preventing free radical damage. However, it also acts as a stimulant, making it difficult to determine whether the delay in onset of dementia symptoms is due to protection from free radicals or to the general elevation of brain activity from the stimulant effect.[56]
- Antipsychotic drugs: Both typical antipsychotics (such as Haloperidol) and atypical antipsychotics such as (risperidone) increase the risk of death in dementia-associated psychosis.[57] This means that any use of antipsychotic medication for dementia-associated psychosis is off-label and should only be considered after discussing the risks and benefits of treatment with these drugs, and after other treatment modalities have failed. In the UK around 144,000 dementia sufferers are unnecessarily prescribed antipsychotic drugs, around 2000 patients die as a result of taking the drugs each year.[58]
Services
Adult daycare centers as well as special care units in nursing homes often provide specialized care for dementia patients. Adult daycare centers offer supervision, recreation, meals, and limited health care to participants, as well as providing respite for caregivers.
In addition, Home care can provide one-on-one support and care in the home allowing for more individualized attention that is needed as the disease progresses.
While some preliminary studies have found that music therapy may be useful in helping patients with dementia, their quality has been low and no reliable conclusions can be drawn from them.[59]
Nursing people with dementia
Psychiatric nurses can make a distinctive contribution to people's mental health. The four main premises upon which psychiatric nursing is based are:
- The nursing is an interactive, developmental human activity that is more concerned with the future development of the person than the origins.
- The experience of mental distress related to the psychiatric disorder is represented through disturbances or reports of private events that are known only to the person concerned.
- Nurses and the people in care are engaged in a relationship based on mutual influence.
- The experience of psychiatric disorder is translated into problems of everyday living and the nurse notes the human responses to the psychiatric distress, not the disorder.[60]
Feeding tubes
There is little evidence, even after widespread use, that feeding tubes help patients with advanced dementia gain weight, regain strength or function, prevent aspiration pneumonias, or improve quality of life. The risks associated with the use of tubes are not well known.[61]
Epidemiology
Evidence from well-planned, representative epidemiological surveys is scarce in many regions, particularly in low-income countries. However, estimates from 2005 suggest a global dementia prevalence of 24.3 million, with 4.6 million new cases of dementia every year. The number of people affected will double every 20 years to 81.1 million by 2040.[62]
See also
- Aging brain
- Caregiving and dementia
- Montessori-Based Dementia Programming
- Agitation (dementia)
- Cognitive orthotics
- Sundowning (dementia)
- Wandering (dementia)
- Aging movement control
References
- ^ Fadil, H., Borazanci, A., Haddou, E. A. B.,Yahyaoui, M., Korniychuk, E., Jaffe, S. L., Minagar, A. (2009). "Early Onset Dementia". International Review of Neurobiology. International Review of Neurobiology 84: 245–262. doi:10.1016/S0074-7742(09)00413-9. ISBN 9780123748331. PMID 19501722.
- ^ "Dementia definition". MDGuidelines. Reed Group. http://www.mdguidelines.com/dementia/definition. Retrieved 2009-06-04.
- ^ Gleason OC (March 2003). "Delirium". American Family Physician 67 (5): 1027–34. PMID 12643363. http://www.aafp.org/afp/20030301/1027.html.
- ^ Berrios GE (November 1987). "Dementia during the seventeenth and eighteenth centuries: a conceptual history". Psychological Medicine 17 (4): 829–37. doi:10.1017/S0033291700000623. PMID 3324141.
- ^ Kolata, Gina (June 17, 2010). "Drug Trials Test Bold Plan to Slow Alzheimer's". The New York Times. http://www.nytimes.com/2010/07/17/health/research/17drug.html. Retrieved June 17, 2010.
- ^ [1].
- ^ Calleo J, Stanley M (2008). "Anxiety Disorders in Later Life Differentiated Diagnosis and Treatment Strategies". Psychiatric Times 25 (8). http://www.psychiatrictimes.com/display/article/10168/1166976.
- ^ Shub, Denis; Kunik, Mark E (April 16, 2009). "Psychiatric Comorbidity in Persons With Dementia: Assessment and Treatment Strategies". Psychiatric Times 26 (4). http://www.psychiatrictimes.com/alzheimer-dementia/article/10168/1403050.
- ^ "Drivers with dementia a growing problem, MDs warn". CBC News, Canada. September 19, 2007. http://www.cbc.ca/health/story/2007/09/19/drivers-dementia.html?ref=rss.
- ^ Gelder, Mayou, Geddes (2005). Psychiatry. (Pg 141). New York, NY: Oxford University Press Inc.
- ^ Neuropathology Group. Medical Research Council Cognitive Function and Aging Study (2001). "Pathological correlates of late-onset dementia in a multicentre, community-based population in England and Wales. Neuropathology Group of the Medical Research Council Cognitive Function and Ageing Study (MRC CFAS)". Lancet 357 (9251): 169–75. doi:10.1016/S0140-6736(00)03589-3. PMID 11213093.
- ^ Wakisaka Y et al. (2003). "Age-associated prevalence and risk factors of Lewy body pathology in a general population: the Hisayama study". Acta Neuropathol 106 (4): 374–82. doi:10.1007/s00401-003-0750-x. PMID 12904992.
- ^ White L et al. (2002). "Cerebrovascular pathology and dementia in autopsied Honolulu-Asia Aging Study participants". Ann N Y Acad Sci 977 (9): 9–23. doi:10.1111/j.1749-6632.2002.tb04794.x. PMID 12480729.
- ^ Ratnavalli E et al. (2002). "The prevalence of frontotemporal dementia". Neurology 58 (11): 1615–21. PMID 12058088.
- ^ McKee A et al. (2009). "Chronic Traumatic Encephalopathy in Athletes: Progressive Tauopathy following Repetitive Head Injury". J Neuropathol Exp Neurol 68 (7): 709–735. doi:10.1097/NEN.0b013e3181a9d503. PMC 2945234. PMID 19535999. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2945234.
- ^ Galvin JE et al. (2006). "Clinical phenotype of Parkinson disease dementia". Neurology 67 (9): 1605–11. doi:10.1212/01.wnl.0000242630.52203.8f. PMID 17101891.
- ^ Gibbons D et al.. "Porphyria and dementia: a case report". Ir J Psych Med 20 (3): 96–99. http://www.ijpm.org/content/pdf/195/Dementia.pdf.
- ^ Lamont P (2004). "Cognitive Decline in a Young Adult with Pre-Existent Developmental Delay – What the Adult Neurologist Needs to Know". Practical Neurology 4 (2): 70–87. doi:10.1111/j.1474-7766.2004.02-206.x. http://pn.bmj.com/cgi/content/abstract/4/2/70.
- ^ Boustani, M; Peterson, B; Hanson, L; Harris, R; & Lohr, K; U.S. Preventive Services Task Force (3 June 2003). "Screening for dementia in primary care: a summary of the evidence for the U.S. Preventive Services Task Force". Ann Intern Med 138 (11): 927–37. PMID 12779304. http://www.annals.org/cgi/content/full/138/11/927.
- ^ a b Cullen B, O'Neill B, Evans JJ, Coen RF, Lawlor BA (August 2007). "A review of screening tests for cognitive impairment". Journal of Neurology, Neurosurgery, and Psychiatry 78 (8): 790–9. doi:10.1136/jnnp.2006.095414. PMC 2117747. PMID 17178826. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2117747.
- ^ Teng EL, Chui HC (August 1987). "The Modified Mini-Mental State (3MS) examination". The Journal of Clinical Psychiatry 48 (8): 314–8. PMID 3611032.
- ^ Teng EL, Hasegawa K, Homma A, et al. (1994). "The Cognitive Abilities Screening Instrument (CASI): a practical test for cross-cultural epidemiological studies of dementia". International Psychogeriatrics / IPA 6 (1): 45–58; discussion 62. doi:10.1017/S1041610294001602. PMID 8054493.
- ^ Royall, D; Cordes, J.; Polk, M. (1998). "CLOX: an executive clock drawing task". J Neurol Neurosurg Psychiatry 64 (5): 588–94. doi:10.1136/jnnp.64.5.588. PMC 2170069. PMID 9598672. http://jnnp.bmj.com/cgi/content/full/64/5/588.
- ^ Sager MA, Hermann BP, La Rue A, Woodard JL (October 2006). "Screening for dementia in community-based memory clinics" (PDF). WMJ: Official Publication of the State Medical Society of Wisconsin 105 (7): 25–9. PMID 17163083. http://www.wisconsinmedicalsociety.org/_WMS/publications/wmj/issues/wmj_v105n7/sager.pdf.
- ^ Fleisher, A; Sowell, B; Taylor, C; Gamst, A; Petersen, R; Thal, L; Alzheimer's Disease Cooperative Study (2007). "Clinical predictors of progression to Alzheimer disease in amnestic mild cognitive impairment". Neurology 68 (19): 1588–95. doi:10.1212/01.wnl.0000258542.58725.4c. PMID 17287448.
- ^ Karlawish, J & Clark, C (2003). "Diagnostic evaluation of elderly patients with mild memory problems". Ann Intern Med 138 (5): 411–9. PMID 12614094. http://www.annals.org/cgi/content/full/138/5/411.
- ^ Jorm AF (September 2004). "The Informant Questionnaire on cognitive decline in the elderly (IQCODE): a review". International Psychogeriatrics / IPA 16 (3): 275–93. doi:10.1017/S1041610204000390. PMID 15559753.
- ^ Bonte, FJ; Harris TS, Hynan LS, Bigio EH, White CL 3rd (July 2006). "Tc-99m HMPAO SPECT in the differential diagnosis of the dementias with histopathologic confirmation". Clinical Nuclear Medicine 31 (7): 376–8. doi:10.1097/01.rlu.0000222736.81365.63. PMID 16785801.
- ^ Dougall, NJ; Bruggink S, Ebmeier KP (Nov-December 2004). "Systematic review of the diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia". The American Journal of Geriatric Psychiatry 12 (6): 554–70. doi:10.1176/appi.ajgp.12.6.554. PMID 15545324.
- ^ Abella HA (June 16, 2009). "Report from SNM: PET imaging of brain chemistry bolsters characterization of dementias". Diagnostic Imaging. http://www.diagnosticimaging.com/imaging-trends-advances/cardiovascular-imaging/article/113619/1423022.
- ^ [2]
"It is... possible that moderate lifestyles in general, which obviously vary according to different cultural environments, protect from cognitive impairment. Thus it may not be the direct effect of alcohol or specific substances in alcoholic drinks that provide the protection."
- ^ Hyvet, investigators; Burch; Fletcher; Bulpitt (August 2008). "Incident dementia and blood pressure lowering in the Hypertension in the Very Elderly Trial cognitive function assessment (HYVET-COG): a double-blind, placebo controlled trial". Lancet Neurol 7 (8): 683–9. doi:10.1016/S1474-4422(08)70143-1. PMID 18614402.
- ^ Hu, Y; Russek, SJ (2008). "BDNF and the diseased nervous system: a delicate balance between adaptive and pathological processes of gene regulation". Journal of neurochemistry 105 (1): 1–17. doi:10.1111/j.1471-4159.2008.05237.x. PMID 18208542.
- ^ Schindowski, K; Belarbi, K; Buée, L (2008). "Neurotrophic factors in Alzheimer's disease: role of axonal transport". Genes, Brain and Behavior 7 (Suppl 1): 43–56. doi:10.1111/j.1601-183X.2007.00378.x. PMC 2228393. PMID 18184369. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2228393.
- ^ Tapia-Arancibia, L; Aliaga, E; Silhol, M; Arancibia, S (2008). "New insights into brain BDNF function in normal aging and Alzheimer disease". Brain research reviews 59 (1): 201–20. doi:10.1016/j.brainresrev.2008.07.007. PMID 18708092.
- ^ "Bilingualism Has Protective Effect In Delaying Onset Of Dementia By Four Years, Canadian Study Shows". Medical News Today. 2007-01-11. http://www.medicalnewstoday.com/medicalnews.php?newsid=60646. Retrieved 2007-01-16.
- ^ a b c d e Hadjistavropoulos, T et al.; Herr, K; Turk, DC; Fine, PG; Dworkin, RH; Helme, R; Jackson, K; Parmelee, PA et al. (2007). "An interdisciplinary expert consensus statement on assessment of pain in older persons". Clinical Journal of Pain 23 (1 suppl): S1–43. doi:10.1097/AJP.0b013e31802be869. PMID 17179836.
- ^ a b Shega, J; Emanuel, L; Vargish, L; Levine, S.K.; Bursch, H; Herr, K; Karp, J.F.; Weiner, D.K. (2007). "Pain in persons with dementia: complex, common, and challenging". Journal of Pain 8 (5): 373–8. doi:10.1016/j.jpain.2007.03.003. PMID 17485039.
- ^ Blyth, F; Cumming, M.R.; Mitchell, P; Wang, J.J. (2007). "Pain and falls in older people". European Journal of Pain 11 (5): 564–71. doi:10.1016/j.ejpain.2006.08.001. PMID 17015026. http://www.ncbi.nlm.nih.gov/pubmed/17015026?itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_RVDocSum&ordinalpos=8.
- ^ Brown, C. (2009). "Pain, aging and dementia: The crisis is looming, but are we ready?". British Journal of Occupational Therapy 72 (8): 371–75. http://www.ingentaconnect.com/content/cot/bjot/2009/00000072/00000008/art00007.
- ^ Herr, K; Bjoro, K; Decker, S; Wang (2006). "Tools for assessment of pain in nonverbal older adults with dementia: a state-of-the-science review". Journal of pain and symptom management 31 (2): 170–92. doi:10.1016/j.jpainsymman.2005.07.001. PMID 16488350. http://www.ncbi.nlm.nih.gov/pubmed/16488350.
- ^ Stolee, P; Hillier, LM; Esbaugh, et al.; Bol, N; McKellar, L; Gauthier, N (2005). "Instruments for the assessment of pain in older persons with cognitive impairment". Journal of the American geriatrics society 53 (2): 319–26. doi:10.1111/j.1532-5415.2005.53121.x. PMID 15673359.
- ^ Rafii, M. S. & Aisen, P. S. (2009). "Recent developments in Alzheimer's disease therapeutics". BMC medicine 7: 1–4. doi:10.1186/1741-7015-7-7. http://www.biomedcentral.com/1741-7015/7/7.
- ^ a b Lleó A, Greenberg SM, Growdon JH (2006). "Current pharmacotherapy for Alzheimer's disease". Annu. Rev. Med. 57: 513–33. doi:10.1146/annurev.med.57.121304.131442. PMID 16409164. http://arjournals.annualreviews.org/doi/abs/10.1146/annurev.med.57.121304.131442?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dncbi.nlm.nih.gov.
- ^ Lleó A, Greenberg SM, Growdon JH (2006). "Current pharmacotherapy for Alzheimer's disease". Annu. Rev. Med. 57: 513–33. doi:10.1146/annurev.med.57.121304.131442. PMID 16409164.
- ^ Bear, M. F., Connors, B. W. & Paradiso, M. A. (2007). "5". Neuroscience: Exploring The Brain. Baltimore: Lippincott Williams & Wilkins. p. 119. ISBN 0-7817-6003-8.
- ^ Gill S. S., Anderson, G. M., Fischer, H.D., Li, P., Normand, S. T. & Rochon, P. A. (2009). "Syncope and its consequences in patients with dementia receiving cholinesterase inhibitors: A population-based cohort study". Archives of Internal Medicine 169 (9): 867–873. doi:10.1001/archinternmed.2009.43. PMID 19433698.
- ^ Plath, N., Ledrup, L., Larsen P. H. & Redrobe, J. P., Niels; Lerdrup, Linda; Larsen, Peter Hjørringgaard; Redrobe, John Paul (2011). "Can small molecules provide truly effective enhancement of cognition? Current achievements and future directions". Expert Opinion on Investigational Drugs 20 (6): 795–811. doi:10.1517/13543784.2011.574612. PMID 21510828.
- ^ Parsons, C. G., Stoffler, A. & Danysz, W., Chris G.; Stöffler, Albrecht; Danysz, Wojciech (2007). "Memantine: A NMDA receptor antagonist that improves memory by restoration of homeostasis in the glutamatergic system - too little activation is bad, too much is even worse". Neuropharmacology 53 (6): 699–723. doi:10.1016/j.neuropharm.2007.07.013. PMID 17904591.
- ^ Raina P, Santaguida P, Ismaila A, et al. (March 2008). "Effectiveness of cholinesterase inhibitors and memantine for treating dementia: evidence review for a clinical practice guideline". Annals of Internal Medicine 148 (5): 379–97. PMID 18316756. http://www.annals.org/cgi/content/full/148/5/379.
- ^ Atri A, Shaughnessy LW, Locascio JJ, Growdon JH (2008). "Long-term Course and Effectiveness of Combination Therapy in Alzheimer's Disease". Alzheimer Disease and Associated Disorders 22 (3): 209–21. doi:10.1097/WAD.0b013e31816653bc. PMC 2718545. PMID 18580597. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2718545.
- ^ Choi Y, Kim HS, Shin KY, et al., YH; Kim; Suh (November 2007). "Minocycline attenuates neuronal cell death and improves cognitive impairment in Alzheimer's disease models". Neuropsychopharmacology 32 (11): 2393–404. doi:10.1038/sj.npp.1301377. PMID 17406652.
- ^ Thompson S, Herrmann N, Rapoport MJ, Lanctôt KL (April 2007). "Efficacy and safety of antidepressants for treatment of depression in Alzheimer's disease: a metaanalysis" (PDF). Canadian Journal of Psychiatry 52 (4): 248–55. PMID 17500306. http://publications.cpa-apc.org/media.php?mid=586&xwm=true.
- ^ Bains J, Birks JS, Dening TR (2002). Dening, Tom. ed. "The efficacy of antidepressants in the treatment of depression in dementia". Cochrane Database of Systematic Reviews (4): CD003944. doi:10.1002/14651858.CD003944. PMID 12519625.
- ^ Lolk A, Gulmann NC (2006). "[Psychopharmacological treatment of behavioral and psychological symptoms in dementia]" (in Danish). Ugeskr Laeg 168 (40): 3429–32. PMID 17032610.
- ^ Riederer P, Lachenmayer L (November 2003). "Selegiline's neuroprotective capacity revisited". Journal of Neural Transmission 110 (11): 1273–8. doi:10.1007/s00702-003-0083-x. PMID 14628191.
- ^ "FDA MedWatch - 2008 Safety Alerts for Human Medical Products". FDA. http://www.fda.gov/medwatch/safety/2008/safety08.htm#Antipsychotics.
- ^ Bowcott, Owen (2009-11-12). "Chemical restraints killing dementia patients". London: Guardian. http://www.guardian.co.uk/society/2009/nov/12/anti-psychotic-drugs-kill-dementia-patients. Retrieved 2010-05-01.
- ^ Vink AC, Bruinsma MS, Scholten RJPM; (Dementia and Cognitive Improvement Group) (2003). "Music therapy for people with dementia". Cochrane Database of Systematic Reviews (4): CD003477.pub2 (Orig. rev.). doi:10.1002/14651858.CD003477.pub2. PMID 15266489.
- ^ Barker, P. (2003). Psychiatric and Mental Health Nursing The craft of caring. New York, NY: Oxford University Press Inc.
- ^ Sampson EL, Candy B, Jones L; (Dementia and Cognitive Improvement Group) (2009 Apr 15). "Enteral tube feeding for older people with advanced dementia". Cochrane Database of Systematic Reviews (2): CD007209.pub2 (Orig. rev.). doi:10.1002/14651858.CD007209.pub2.
- ^ Ferri, CP; Prince, M, Brayne, C, Brodaty, H, Fratiglioni, L, Ganguli, M, Hall, K, Hasegawa, K, Hendrie, H, Huang, Y, Jorm, A, Mathers, C, Menezes, PR, Rimmer, E, Scazufca, M, Alzheimer's Disease, International (2005-12-17). "Global prevalence of dementia: a Delphi consensus study". Lancet 366 (9503): 2112–7. doi:10.1016/S0140-6736(05)67889-0. PMC 2850264. PMID 16360788. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2850264.
External links
- BBC Headroom: Living with Dementia
- The Dementia Centre – Information provided by PSS (Personal Services Society). Provides information and support to people with dementia, their carers, and health professionals.
- Alzheimer's Research Trust – What is dementia? – Information produced by the Alzheimer's Research Trust including statistics.
- Alzheimer's Society – About dementia – Information produced by the Alzheimer's Society including factsheets and support.
- The Dementia Services Development Centre, University of Stirling
- Dementia tutorial for U.K. practitioners by the Alzheimer's Society
- Understanding Dementia: a primer of diagnosis and management
- AlzOnline – AlzOnline provides education, information, and support to persons caring for someone with Alzheimer's disease or a related memory problem.
- Medicinenet
- Understand Pain and Dementia tutorial from the Occupational Therapy Department at the University of Alberta
- Help Dementia Uk
- Concise Guidelines to Better Practice The Assessment of Pain in Older Person – British Pain Society (2007)
- Dementia care map Map of Medicine, Updated 29 October 2010
- Dementia at GPnotebook
- Dementia at eMedicineHealth
- Merck Geriatrics 5-40a
- Does Alcohol Slow Dementia?
Psychiatry Portal Subspecialties Addiction psychiatry · Biological psychiatry · Child and adolescent psychiatry · Cross-cultural psychiatry · Developmental disability · Eating disorders · Emergency psychiatry · Forensic psychiatry · Geriatric psychiatry · Liaison psychiatry · Military psychiatry · Neuropsychiatry · Palliative medicine · Pain medicine · Psychotherapy · Sleep medicine
Organizations American Board of Psychiatry and Neurology · American Psychiatric Association · American Neuropsychiatric Association · Brazilian Association of Psychiatry · Canadian Psychiatric Association · Chinese Society of Psychiatry · Democratic Psychiatry · German Society of Psychiatry, Psychotherapy and Neurology · Hong Kong College of Psychiatrists · Independent Psychiatric Association of Russia · Indian Psychiatric Society · Irish College of Psychiatrists · Israeli Psychiatric Association · Italian Psychiatric Society · Japanese Society of Psychiatry & Neurology · Korean Neuropsychiatric Association · Maryland Psychiatric Society · National Institute of Mental Health · Pakistan Psychiatric Society · Royal Australian and New Zealand College of Psychiatrists · Royal College of Psychiatrists · Singapore Psychiatric Association · South African Society of Psychiatrists · World Psychiatric Association
Related topics Anti-psychiatry · Behavioral medicine · Clinical neuroscience · Imaging genetics · Neuroimaging · Neurophysiology · Psychiatrist · Psychiatric epidemiology · Psychiatric genetics · Psychiatric survivors movement · Psychosomatic medicine · Psycho-oncology · Psychopharmacology · Psychosurgery · Psychoanalysis
Lists Categories:- Aging-associated diseases
- Cognitive disorders
- Organic, including symptomatic, mental disorders
- Dementia

Wikimedia Foundation. 2010.