- Primary central nervous system lymphoma
-
Primary central nervous system lymphoma Classification and external resources 
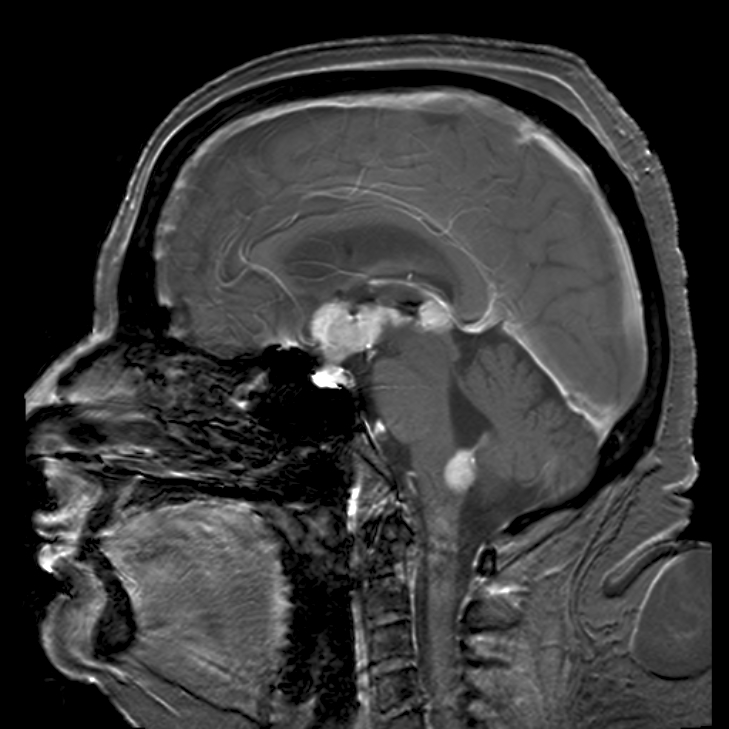
Brain magnetic resonance imaging showing primary central nervous system B-cell non-Hodgkin lymphoma of the sella turcica and hypothalamus, continuing to the tectum (intensely white areas in the middle).ICD-9 200.5 DiseasesDB 29451 A primary central nervous system lymphoma (PCNSL), also known as microglioma and primary brain lymphoma, [1] is a primary intracranial tumor appearing mostly in patients with severe immunosuppression (typically patients with AIDS). PCNSLs represent around 20% of all cases of lymphomas in HIV infections (other types are Burkitt's lymphomas and immunoblastic lymphomas). Primary CNS lymphoma is highly associated with Epstein-Barr virus (EBV) infection (> 90%) in immunodeficient patients (such as those with AIDS and those iatrogenically immunosuppressed)[2], and does not have a predilection for any particular age group. Mean CD4+ count at time of diagnosis is ~50/uL. Because of the severity of immunosuppression at the time of diagnosis, it is no surprise that prognosis is usually poor. In immunocompetent patients (that is, patients who do not have AIDS or some other immunodeficiency), there is rarely an association with EBV infection or other DNA viruses. In the immunocompetent population, PCNSLs typically appear in older patients in their 50's and 60's. Importantly, the incidence of PCNSL in the immunocompetent population has been reported to have increased more than 10-fold from 2.5 cases to 30 cases per 10 million population[3][4]. The cause for the increase in incidence of this disease in the immunocompetent population is unknown.
Contents
Classification
Most PCNSLs are diffuse large B cell non-Hodgkin lymphomas[5][6].
Clinical manifestations
A primary CNS lymphoma usually presents with seizure, headache, cranial nerve findings, altered mental status, or other focal neurological deficits typical of a mass effect[7][8]. Systemic symptoms may include fever, night sweats, or weight loss.Other symptoms include
- diplopia
- dysphagia
- vertigo
- monocular vision loss
- progressive dementia or stupor in patients with a nonfocal neurologic exam and minimal abnormalities on MRI (more common in AIDS patients)
- facial hypoesthesia[9]
Diagnosis
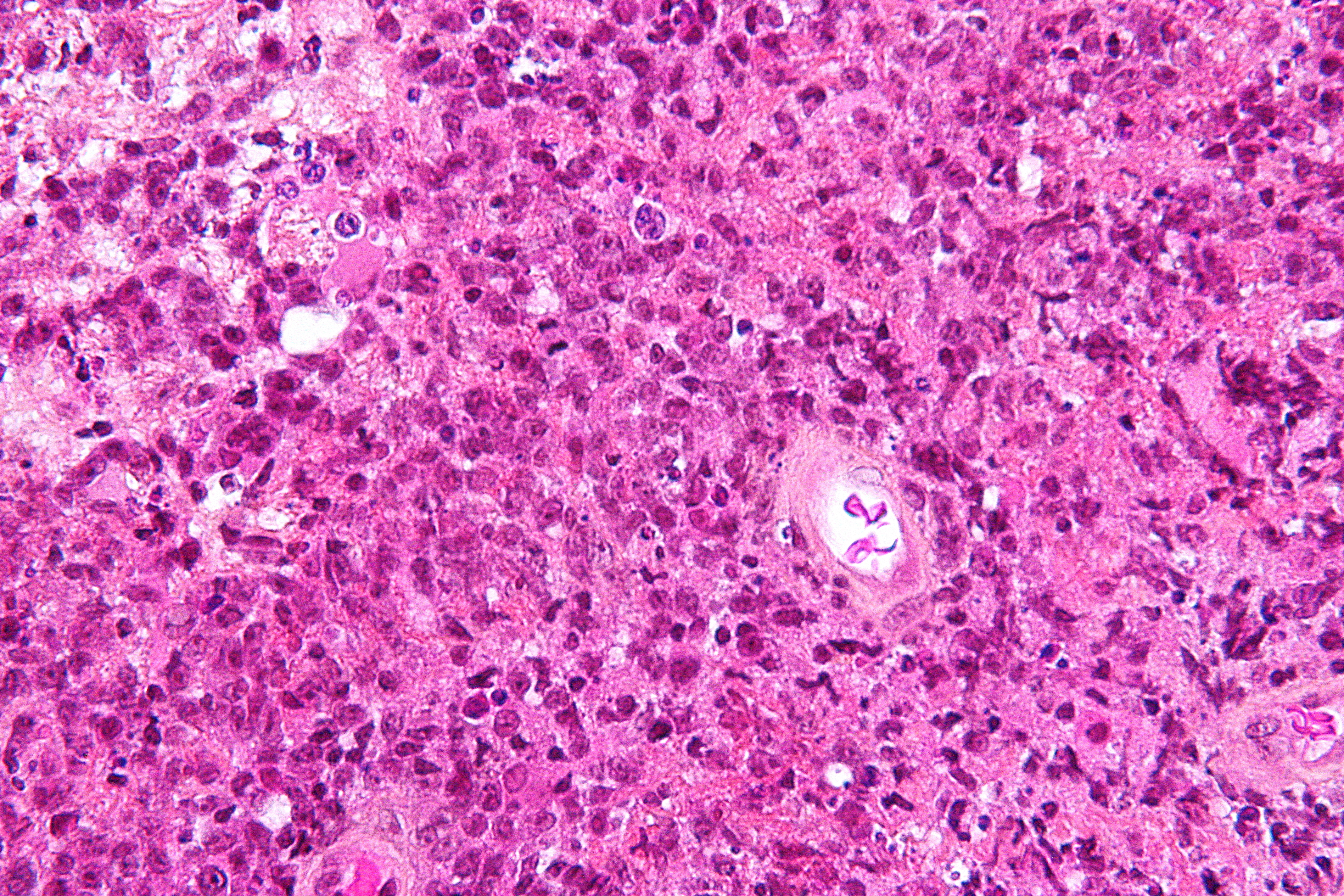
 Micrograph showing a primary CNS lymphoma with the characteristic perivascular distribution composed of large cells with prominent nucleoli. Brain biopsy. HPS stain.
Micrograph showing a primary CNS lymphoma with the characteristic perivascular distribution composed of large cells with prominent nucleoli. Brain biopsy. HPS stain.
The definitive diagnosis is arrived at from tissue, i.e. a biopsy, by a pathologist.
MRI or contrast enhanced CT classically shows multiple ring-enhancing lesions in the deep white matter. The major differential diagnosis (based on imaging) is cerebral toxoplasmosis, which is also prevalent in AIDS patients and also presents with a ring-enhanced lesion, although toxoplasmosis generally presents with more lesions and the contrast enhancement is typically more pronounced. imaging techniques cannot distinguish the two conditions with certainty, and cannot exclude other diagnoses. Thus, patients undergo a brain biopsy.
Treatment
Surgical resection is usually ineffective because of the depth of the tumor. Treatment with irradiation and corticosteroids often only produces a partial response and tumor recurs in more than 90% of patients. Median survival is 10 to 18 months in immunocompetent patients, and less in those with AIDS. The addition of IV methotrexate and folinic acid (leucovorin) may extend survival to a median of 3.5 years. If radiation is added to methotrexate, median survival time may increase beyond 4 years. However, radiation is not recommended in conjunction with methotrexate because of an increased risk of leukoencephalopathy and dementia in patients older than 60.[10] In AIDS patients, perhaps the most important factor with respect to treatment is the use of highly active anti-retroviral therapy (HAART), which affects the CD4+ lymphocyte population and the level of immunosuppression.[citation needed] The optimal treatment plan for patients with PCNSL has not been determined. Combination chemotherapy and radiotherapy at least doubles survival time, but causes dementia and leukoencephalopathy in at least 50% of patients who undergo it. The most studied chemotheraputic agent in PCNSL is methotrexate (a folate analogue that interferes with DNA repair). Methotrexate therapy in patients with PCNSL typically requires hospitalization for close monitoring and intravenus fluids. Leucovrin is often given for the duration of the therapy. Standard chemotherapeutic regimens for lymphoma such as CHOP are ineffective in PCNSL, probably due to poor penetration of the agents through the blood brain barrier.[11]
Newer treatments, such as high dose chemotherapy combined with stem cell transplant are proving to increase survival by years.
Prognosis
In immunocompetent patients
The initial response to radiotherapy is often excellent, and may result in a complete remission. However,the duration of response with radiotherapy alone remains short, with median survival after treatment with radiotherapy just 18 months. Methotrexate based chemotherapy markedly improves survival,with some studies showing median survival after methotrexate chemotherapy reaching 48 months.[12]
In AIDS patients
Patients with AIDS and PCNSL have a median survival of only 4 months with radiotherapy alone. Untreated, median survival is only 2.5 months, sometimes due to concurrent opportunistic infections rather than the lymphoma itself. Extended survival has been seen, however, in a subgroup of AIDS patients with CD4 counts of more than 200 and no concurrent opportunistic infections, who can tolerate aggressive therapy consisting of either methotrexate monotherapy or vincristine, procarbazine, or whole brain radiotherapy. These patients have a median survival of 10–18 months. Of course, highly active antiretroviral therapy (HAART) is critical for prolonged survival in any AIDS patient, so compliance with HAART may play a role in survival in patients with concurrent AIDS and PCNSL.[13]
References
- ^ "CNS lymphoma, primary information". Diseases Database. http://www.diseasesdatabase.com/ddb29451.htm. Retrieved 17 April 2011.
- ^ Fine HA, Mayer RJ. Primary central nervous system lymphoma. Ann Intern Med 1993; 119(11):1093-1104
- ^ Eby NL, Grufferman S, Flannelly CM, Schold SC, Jr., Vogel FS, Burger PC. Increasing incidence of primary brain lymphoma in the US. Cancer 1988;62(11):2461-2465
- ^ Corn BW, Marcus SM, Topham A, Hauck W, Curran WJ, Jr. Will primary central nervous system lymphoma be the most frequent brain tumor diagnosed in the year 2000? Cancer 1997;79(12):2409-2413
- ^ Lukes RJ, Collins RD. Immunologic characterization of human malignant lymphomas. Cancer 1974;34:1488-1503
- ^ Jellinger K, Radaskiewictz T, Slowik F. Primary malignant lymphomas of the central nervous system in man. Acta Neuropathol 1975;95-102 (suppl 6)
- ^ Herrlinger U, Schabet M, Bitzer M, Petersen D, Krauseneck P. Primary central nervous system lymphoma: from clinical presentation to diagnosis. J Neurosurg 2000; 92:261-266
- ^ Herrlinger U, Schabet M, Bitzer M, Petersen D, Krauseneck P. Primary central nervous system lymphoma: from clinical presentation to diagnosis.J.Neurooncol. 1999;43:219-226. (PMID: 10563426).
- ^ http://emedicine.medscape.com/article/1157638-overview
- ^ Deangelis LM, Hormigo A. Treatment of primary central nervous system lymphoma. Semin Oncol 2004; 31:684-692.
- ^ http://emedicine.medscape.com/article/1157638-treatment
- ^ http://emedicine.medscape.com/article/1157638-followup
- ^ http://emedicine.medscape.com/article/1157638-followup
Hematological malignancy/leukemia histology (ICD-O 9590–9989, C81–C96, 200–208)
Lymphoid/Lymphoproliferative, Lymphomas/Lymphoid leukemias (9590–9739, 9800–9839)By development/
markerCD5+CD22+germinal center/follicular B cell (Follicular, Burkitt's, GCB DLBCL, Primary cutaneous follicular lymphoma)marginal zone/marginal-zone B cell (Splenic marginal zone, MALT, Nodal marginal zone, Primary cutaneous marginal zone lymphoma)see immunoproliferative immunoglobulin disordersBy infectionDiffuse large B-cell lymphoma · Intravascular large B-cell lymphoma · Primary cutaneous marginal zone lymphoma · Primary cutaneous immunocytoma · Plasmacytoma · Plasmacytosis · Primary cutaneous follicular lymphomaBy development/
markerTdT+: ALL (Precursor T acute lymphoblastic leukemia/lymphoma)
prolymphocyte (Prolymphocytic)
CD30+ (Anaplastic large-cell lymphoma, Lymphomatoid papulosis type A)indolent: Mycosis fungoides · Pagetoid reticulosis · Granulomatous slack skin
aggressive: Sézary's disease · Adult T-cell leukemia/lymphomaNon-MFCD30-: Non-mycosis fungoides CD30− cutaneous large T-cell lymphoma · Pleomorphic T-cell lymphoma · Lymphomatoid papulosis type B
CD30+: CD30+ cutaneous T-cell lymphoma · Secondary cutaneous CD30+ large cell lymphoma · Lymphomatoid papulosis type AOther peripheralHepatosplenic · Angioimmunoblastic · Enteropathy-associated T-cell lymphoma · Peripheral T-cell lymphoma-Not-Otherwise-Specified (Lennert lymphoma) · Subcutaneous T-cell lymphomaBy infectionHTLV-1 (Adult T-cell leukemia/lymphoma)T or NKLymphoid+myeloidCutaneous lymphoid hyperplasia Cutaneous lymphoid hyperplasia with bandlike and perivascular patterns · Cutaneous lymphoid hyperplasia with nodular pattern · Jessner lymphocytic infiltrate of the skinNervous tissue tumors/NS neoplasm/Neuroectodermal tumor (ICD-O 9350–9589) (C70–C72, D32–D33, 191–192/225) Endocrine/
sellar (9350–9379)other: PinealomaCNS
(9380–9539)Astrocytoma (Pilocytic astrocytoma, Pleomorphic xanthoastrocytoma, Fibrillary (also diffuse or lowgrade) astrocytomas, Anaplastic astrocytoma, Glioblastoma multiforme)Multiple/unknownNeuroblastoma (Esthesioneuroblastoma, Ganglioneuroblastoma) · Medulloblastoma · Atypical teratoid rhabdoid tumorPrimitiveHematopoieticPrimary central nervous system lymphomaPNS: NST
(9540–9579)cranial and paraspinal nerves: Neurofibroma (Neurofibrosarcoma, Neurofibromatosis) · Neurilemmoma/Schwannoma (Acoustic neuroma) · Malignant peripheral nerve sheath tumornote: not all brain tumors are of nervous tissue, and not all nervous tissue tumors are in the brain (see brain metastases)
Infectious diseases · Viral systemic diseases (A80–B34, 042–079) Oncovirus DNA virus: HBV (Hepatocellular carcinoma) · HPV (Cervical cancer, Anal cancer) · Kaposi's sarcoma-associated herpesvirus (Kaposi's sarcoma) · Epstein-Barr virus (Nasopharyngeal carcinoma, Burkitt's lymphoma, Primary central nervous system lymphoma) · MCPyV (Merkel cell cancer) · SV40Immune disorders Central
nervous systemEncephalitis/
meningitisDNA virus: JCV (Progressive multifocal leukoencephalopathy)
RNA virus: MeV (Subacute sclerosing panencephalitis) · LCV (Lymphocytic choriomeningitis) · Arbovirus encephalitis · Orthomyxoviridae (probable) (Encephalitis lethargica) · RV (Rabies) · Chandipura virus · Herpesviral meningitis · Ramsay Hunt syndrome type IIEyeCardiovascular Respiratory system/
acute viral nasopharyngitis/
viral pneumoniaDigestive system Urogenital External links
- MedPix Teaching File MR Scans of Primary Brain Lymphoma
Categories:- Neurosurgery
- Viral diseases
- Lymphoma
- Brain tumor
Wikimedia Foundation. 2010.