- Nasopharyngeal carcinoma
-
Nasopharyngeal carcinoma Classification and external resources 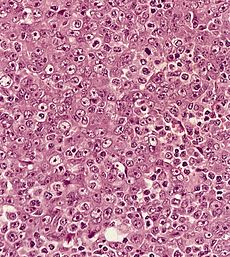
Metastatic nasopharyngeal carcinoma in a lymph nodeICD-10 C11 ICD-9 147 OMIM 161550 DiseasesDB 8814 eMedicine ped/1553 MeSH D009303 Nasopharyngeal carcinoma (NPC) is the most common cancer originating in the nasopharynx, the uppermost region of the pharynx ("throat"), behind the nose where the nasal passages and auditory tubes join the remainder of the upper respiratory tract. NPC differs significantly from other cancers of the head and neck in its occurrence, causes, clinical behavior, and treatment. It is vastly more common in certain regions of East Asia and Africa than elsewhere, with viral, dietary and genetic factors implicated in its causation. It is most common in males. It is a squamous cell carcinoma or an undifferentiated type. Squamous cells are a flat type of cell found in the skin and the membranes that line some body cavities. Differentiation means how different the cancer cells are from normal cells. Undifferentiated is a word used to describe cells that do not have their mature features or functions.
Contents
Classification
Nasopharyngeal carcinoma, commonly known as nasopharyngeal cancer, is classified as a malignant neoplasm, or cancer, arising from the mucosal epithelium of the nasopharynx, most often within the lateral nasopharyngeal recess or fossa of Rosenmüller (the space behind the nose). The World Health Organization Classifies Nasopharyngeal Carcnioma in three types. Type 1 (I) is squamous cell carcinoma. Type 2a (II) is keratinizing undifferentiated carcinoma. Type 2b (III) is nonkeratinizing undifferentiated carcinoma. [1]Type 2b (III) nonkeratinizing undifferentiated form is most common, and is most strongly associated with Epstein-Barr virus infection of the cancerous cells.[2]
-

Undifferentiated nasopharyngeal carcinoma - low power
-

Undifferentiated nasopharyngeal carcinoma - med. power
-

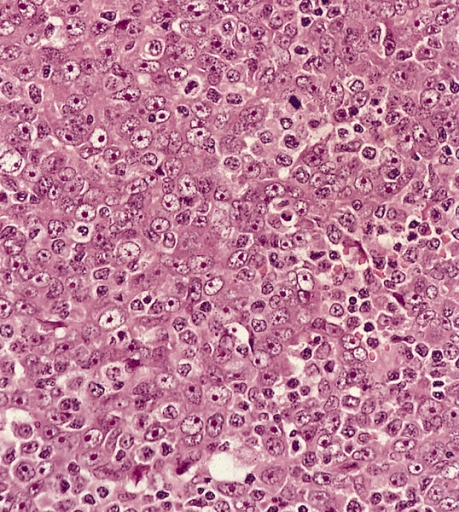
Undifferentiated nasopharyngeal carcinoma - high power
Staging
Staging of Nasophayngeal Carcinoma is based on clinical and radiologic examination. Most patients present with Stage III or IV disease. In Summary: Stage I small tumor confined to nasopharynx Stage II tumor extending in the local area or any evidence of limited neck (nodal) disease Stage III a large tumor with or without neck disease, or a tumor with bilateral neck disease Stage IV intracranial or infratemporal involvement of tumor, extensive neck disease, or any distant metastasis [3]
Symptoms and signs
Cervical lymphadenopathy (disease or swelling of the lymph nodes in the neck) is the initial presentation in many patients, and the diagnosis of NPC is often made by lymph node biopsy. Symptoms related to the primary tumor include trismus, pain, otitis media, nasal regurgitation due to paresis (loss of or impaired movement) of the soft palate, hearing loss and cranial nerve palsies (paralysis). Larger growths may produce nasal obstruction or bleeding and a "nasal twang". Metastatic spread may result in bone pain or organ dysfunction. Rarely, a paraneoplastic syndrome of osteoarthropathy (diseases of joints and bones) may occur with widespread disease.
Causes
EBV (Epstein-Barr virus) NPC is the most common epithelial cancer in adults. The detection of nuclear antigen associated with Epstein-Barr virus (EBNA) and viral DNA in NPC type 2 and 3, has revealed that EBV can infect epithelial cells and is associated with their transformation. The etiology of NPC (particularly the endemic form) seems to follow a multi-step process, in which EBV, ethnic background, and environmental carcinogens all seem to play an important role. Lo et al. showed that EBV DNA was detectable in the blood plasma samples of 96% of patients with non-keratinizing NPC, compared with only 7% in controls [9]. More importantly, EBV DNA levels appear to correlate (have a relationship) with treatment response and they may predict disease recurrence, suggesting that they may be an independent indicator of prognosis. In adults, other likely etiological factors include genetic susceptibility, consumption of food (in particular salted fish)[citation needed] containing carcinogenic volatile nitrosamines, and as in children, EBV .
Treatment
Surgery. Due to the anatomical position of NPC and its tendency to present with cervical lymph node metastases, it is not amenable to surgery for local control. Biopsy of the involved lymph node is the usual surgical procedure. The nasopharyngeal primary tumor is rarely biopsied.
Chemotherapy. Several factors are taken into account in deciding the chemotherapy regimen. Firstly, efficacy(ability to get the desired result): the figures for event-free survival are similar for most small chemotherapy series but therapy usually involves fairly high-dose radiotherapy to the nasopharynx – 60 to 65 Gy. However, the most promising results with a recent update, are those obtained using the Mertens protocol NPC-91-GPOH (Society of Pediatric Oncology and Hematology). This protocol should therefore be considered as the best current treatment. Uniquely, the NPC-91-GPOH protocol includes immunotherapy with interferon-beta after chemotherapy and radiotherapy, which may explain its superior results compared to regimens without interferon treatment . Secondly, late effects: in terms of chemotherapy, the Manchester regimen – doxorubicin, methotrexate and cyclophosphamide – would produce infertility in boys (total dose of cyclophosphamide 12 gm/m2) and possible anthracycline toxicity (total dose of doxorubicin 360 mg/m2) [36]. The NPC-91-GPOH protocol might produce some infertility in older boys but the total dose of cisplatinum is only 300 mg/m2. Furthermore, the incidence of renal toxicity should be relatively low but auditory toxicity would be higher because of the additional effect of irradiation on the auditory apparatus. The degree of pituitary gland dysfunction obviously depends on the radiotherapy field and, potentially, on the dose of radiotherapy but some degree of hypopituitarism is expected. Furthermore, irradiation to the neck would result in hypothyroidism for the majority of patients and irradiation to the oropharynx would result in xerostomia (dry mouth) and resultant poor dentition. The later may be relieved by amifostine, as demonstrated in adult studies.
Radiotherapy. Although treatment with radiotherapy controls the primary tumor [28-30], it does not prevent the appearance of distant metastases [28,31]. Radiotherapy is given with megavoltage equipment after initial chemotherapy. A maximum dose of 45 Gy is given to the clinical target volume, which is a 1 cm margin around the MRI-detected primary site, and inferiorly (below) down to the clavicles (collar bone) to include the lymph nodes. Treatment is given in two phases:
- Phase I – parallel pair (mostly lateral unless the tumor extends anteriorly between the eyes). Eyes, brain and brain stem are shielded as much as possible. A mid-plane dose of 30 Gy in 15 fractions is given.
- Phase II – a lateral parallel pair or three-fields technique is used for the primary site, delivering 15 Gy in seven fractions to the clinical target volume of the tumor with a 1 cm margin. Brain stem and eyes should be shielded. Any overlap with the neck field should be shielded. A matching anterior neck node field is used to deliver a prescribed maximum subcutaneous (tissue underneath the outere layers of skin) dose of 15 Gy in seven fractions. The spinal cord should be shielded in this field. This prescription for radiotherapy is used in Manchester, but it is recognized that higher doses may be used in some centers, possibly to a total of 60 Gy to the tumor volume. In an current GPOH study, patients in complete remission (CR) after three courses of chemotherapy, will have their radiotherapy dosage reduced to 54 Gy instead of 59 Gy.
Recommendation. In the current GPOH protocol NPC-2003-GPOH, low-risk patients with Stage I and II tumors receive radiotherapy only, followed by 105 μg/Kg of adjuvant interferon beta (IFNbeta), intravenously (i.v.), three times a week for 6 months. High-risk patients receive cisplatinum (100 mg/m2 over 6 hours on day 1 with standard hydration), mannitol and electrolyte replacement, and folinic acid (25 mg/m2 every 6 hours for a total of six doses) as well as 5-fluorouracil (1000 mg/m2 per day from day 2 for 5 days) as a continuous infusion. They receive three courses of chemotherapy every 21 days or on full blood count recovery, followed by irradiation and IFNbeta as for low-risk patients. Methotrexate has been dropped because of severe mucositis. Patients not in CR after three courses of chemotherapy will receive concomitant cisplatinum (20 mg/m2/day for 3 days with radiotherapy for two courses).
Prognosis
Prognostic factors Stage at presentation is the most prognostic factor. The 5-year disease-specific survival (DSS) is as follow: • For stage I à 98% • For stage II A-B à 95% • For stage III à 86% • For stage IV A-B à 73% (…)
Factors that may influence prognosis include the clinical stage, patient age and gender, presence of keratinization, lymph node metastasis, and possibly genetic factors. • Better prognosis is associated with lower clinical stage, younger patient age, and female gender. • While worse prognosis is seen with high-stage tumors, old patients and male gender(..) Presentation with lymphadenomegalia implies that the disease has spread beyond the primary site. However, in childhood the presence of metastatic disease in cervical lymph nodes at diagnosis does not adversely affect prognosis (likely outcome) [30-33]. Factors associated with a poor prognosis • skull base involvement [33-35] • extent of the primary tumor [31,32] • cranial nerve involvement [33,34] Reddy et al. (..) evaluated 50 patients with NPC and found that the patients with the keratinizing type of NPC had a higher incidence of locally advanced tumor but a lower incidence of lymphatic and/or distant spread. Despite these findings, the patient with the keratinizing NPC had a poorer 5-year survival rate than those with the other histologic subtypes due to a higher incidence of deaths secondary to local uncontrollable disease and nodal metastasis. (…) NPC frequently metastasize to regional lymph nodes and the presence of lymph node metastasis decrease survival by 10-20%.(..) Similarly, a large percentage of NPC, particularly of the undifferentiated type, metastasize to sites below the clavicle, including lung, bones (rib and spine), and liver.
Epidemiology
NPC is uncommon in the United States and most other nations, but is extremely common in southern regions of China,[4] particularly in Guangdong accounting for 18% of all cancers in China.[5] It is sometimes referred to as Cantonese cancer because it occurs in about 25 cases per 100,000 people in this region, 25 times higher than the rest of the world.[5] It is also quite common in Taiwan.[5] This could be due to the South East Asian diet which typically includes consumption of salted vegetables, fish and meat.[5] While NPC is seen primarily in middle-aged persons in Asia, a high proportion of African cases appear in children. The cause of increased risk for NPC in these endemic regions is not entirely clear.[2]
See also
- Baseball player Babe Ruth died from nasopharyngeal carcinoma in 1948.
- Lymphoepithelioma-like carcinoma
References
- ^ Cummings Otolaryngology. 5th ed. (2010). Chapter 99. pg 1344
- ^ a b Richard Cote, Saul Suster, Lawrence Weiss, Noel Weidner (Editor) (2002). Modern Surgical Pathology (2 Volume Set). London: W B Saunders. ISBN 0-7216-7253-1.
- ^ AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, pp 41-56.
- ^ Fang W, Li X, Jiang Q, (2008). "Transcriptional patterns, biomarkers and pathways characterizing nasopharyngeal carcinoma of Southern China". J Transl Med 6: 32. doi:10.1186/1479-5876-6-32. PMC 2443113. PMID 18570662. http://www.translational-medicine.com/content/6//32.
- ^ a b c d Chang E T, Adami H (2006). "The Enigmatic Epidemiology of Nasopharyngeal Carcinoma". Cancer Epidemiol Biomarkers Prev 15 (10): 1765–1777. doi:10.1158/1055-9965.EPI-06-0353. PMID 17035381.
External links
- Nasopharyngeal Cancer Or Sinus Infection
- Cancer Management Handbook: Head and Neck Tumors
- Clinically reviewed nasopharyngeal cancer information for patients from Cancer Research UK
Tumors: Mediastinal tumors/Thoracic neoplasm/respiratory neoplasia (C30–C34/D14, 160–163/212.0–212.4) Upper RT Lower RT Tracheal tumorSquamous cell carcinoma · Adenocarcinoma of the lung · Large-cell lung carcinoma · Rhabdoid carcinoma · Sarcomatoid carcinoma · Carcinoid · Salivary gland-like carcinoma of the lung · Adenosquamous carcinoma · Papillary adenocarcinomaNon-carcinomaBy locationPleura Tumors of lip, oral cavity and pharynx / head and neck cancer (C00–C14/D10–D11, 140–149/210) Oral cancer malignant epithelial tumors (Acinic cell carcinoma, Mucoepidermoid carcinoma, Adenoid cystic carcinoma, Salivary duct carcinoma, Epithelial-myoepithelial carcinoma)benign epithelial tumors (Pleomorphic adenoma, Warthin's tumor)Infectious diseases · Viral systemic diseases (A80–B34, 042–079) Oncovirus DNA virus: HBV (Hepatocellular carcinoma) · HPV (Cervical cancer, Anal cancer) · Kaposi's sarcoma-associated herpesvirus (Kaposi's sarcoma) · Epstein-Barr virus (Nasopharyngeal carcinoma, Burkitt's lymphoma, Primary central nervous system lymphoma) · MCPyV (Merkel cell cancer) · SV40Immune disorders Central
nervous systemEncephalitis/
meningitisDNA virus: JCV (Progressive multifocal leukoencephalopathy)
RNA virus: MeV (Subacute sclerosing panencephalitis) · LCV (Lymphocytic choriomeningitis) · Arbovirus encephalitis · Orthomyxoviridae (probable) (Encephalitis lethargica) · RV (Rabies) · Chandipura virus · Herpesviral meningitis · Ramsay Hunt syndrome type IIEyeCardiovascular Respiratory system/
acute viral nasopharyngitis/
viral pneumoniaDigestive system Urogenital Categories:- Head and neck cancer of respiratory tract
-



Wikimedia Foundation. 2010.