- Solitary pulmonary nodule
-
Solitary pulmonary nodule Classification and external resources 
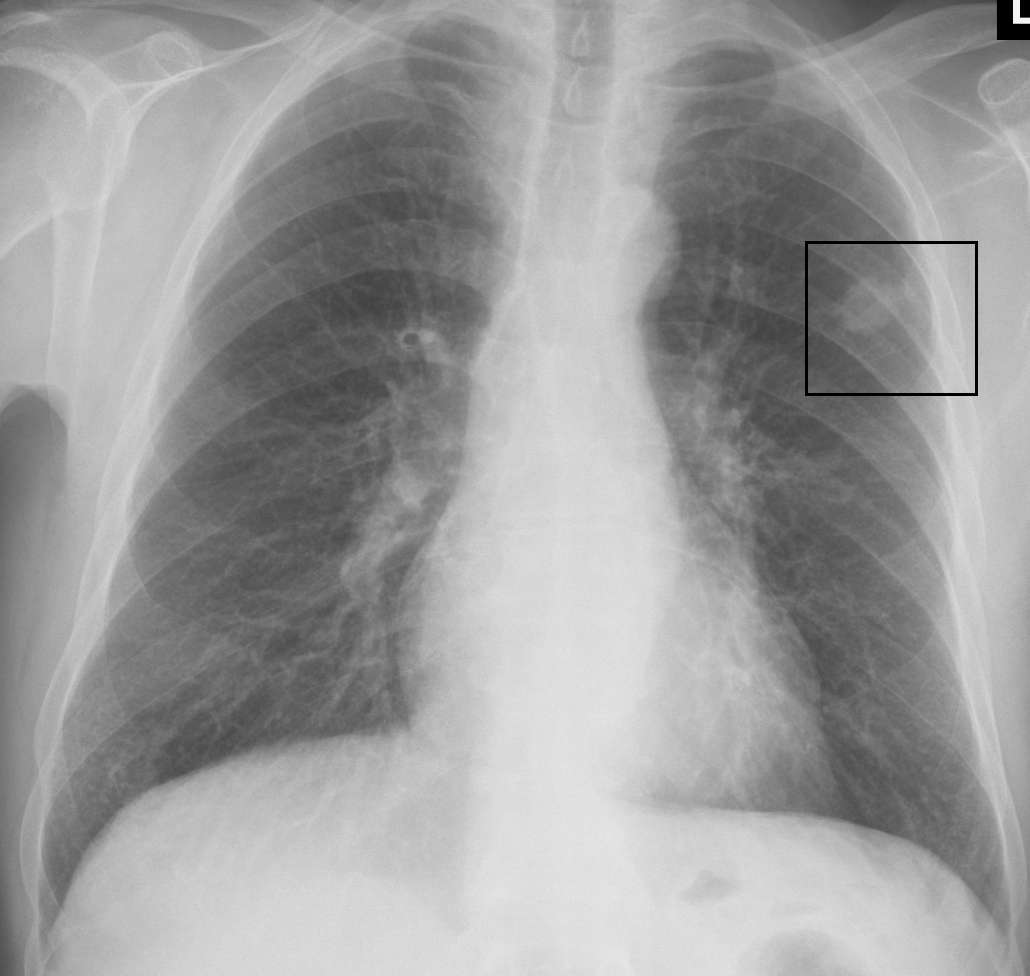
Chest X-ray showing a solitary pulmonary nodule (indicated by a black box) in the left upper lobe.ICD-9 518.89 DiseasesDB 29456 MedlinePlus 000071 eMedicine RADIO/782 MeSH D003074 In radiology, a solitary pulmonary nodule (SPN) or coin lesion is a mass in the lung smaller than 3 centimeters in diameter. It can be an incidental finding found in up to 0.2% of chest X-rays[1] and around 1% of CT scans.[2]
The nodule most commonly represents a benign tumor such as a granuloma or hamartoma, but in around 20% of cases it represents a malignant cancer,[2] especially in older adults and smokers. Conversely, 10 to 20% of patients with lung cancer are diagnosed in this way.[2] Thus, the possibility of cancer needs to be excluded through further radiological studies and interventions, possibly including surgical resection. The prognosis depends on the underlying condition.
Contents
Definition
A solitary pulmonary nodulus needs to be separated from larger lung tumors, smaller infiltrates or masses with other accompanying characteristics. An often used formal radiological definition is the following: a single lesion in the lung completely surrounded by lung parenchyma (functional tissue) with a diameter less than 3 cm and without associated pneumonia, atelectasis (lung collapse) or lymphadenopathies (swollen lymph nodes).[3][4]
Causes
Not every round spot on a radiological image is a coin lesion: it should not be confused with the projection of a structure of the chest wall or skin, such as a nipple, a healing rib fracture or electrocardiographic monitoring.
The most important cause to exclude is a form of lung cancer, including rare forms such as primary pulmonary lymphoma, carcinoid tumor and a solitary metastasis to the lung (common unrecognised primary tumor sites are melanomas, sarcomas or testicular cancer). Benign tumors in the lung include hamartomas and chondromas.
The most common benign coin lesion is a granuloma (inflammatory nodule), for example due to tuberculosis or a fungal infection. Other infectious causes include a pulmonary abscess, pneumonia (including Pneumocystis carinii pneumonia) or rarely nocardial infection or worm infection (such as dirofilariasis or dog heartworm infestation). Lung nodules can also occur in immune disorders such as rheumatoid arthritis or Wegener's granulomatosis.
An SPN can be found to be an arteriovenous malformation, a hematoma or an infarction zone. It may also be caused by bronchial atresia, sequestration, an inhaled foreign body or pleural plaque.
Initial evaluation
The medical history, physical examination and imaging results form the basis of the initial risk assessment and determine the further course of action. Most patients will have a CT scan.
Radiological features
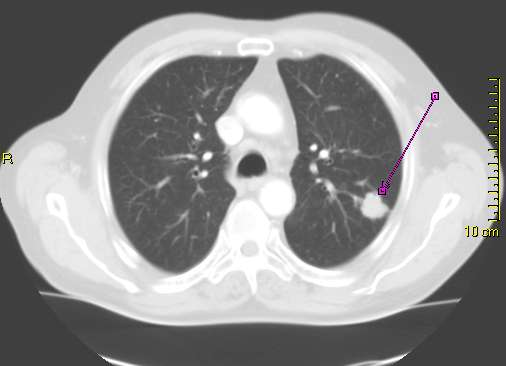
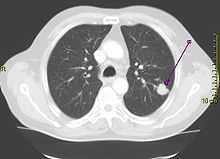 A solitary pulmonary nodule (indicated by the purple arrow) on a CT scan of the chest.
A solitary pulmonary nodule (indicated by the purple arrow) on a CT scan of the chest.
Several features help to distinguish benign conditions from possible lung cancer. The first parameter is the size of the lesion: the smaller, the less risk for malignant cancer.[4] Benign causes tend to have a well defined border, whereas lobulated lesions or those with an irregular margin extending into the neighbouring tissue tend to be malignant.[4]
If there is a central cavity, then a thin wall points to a benign cause whereas a thick wall is associated with malignancy (especially 4mm or less versus 16mm or more).[4] In lung cancer, cavitation can represent central tumor necrosis (tissue death) or secondary abscess formation. If the walls of an airway are visible (air bronchogram), bronchioloalveolar carcinoma is a possibility.
An SPN often contains calcifications. Certain patterns of calcification are reassuring, such as the popcorn-like appearance of hamartoma.[1] An SPN with a density below 15 Hounsfield units on computed tomography tends to be benign, whereas malignant tumors often measure more than 20 Hounsfield units. Fatty tissue inside hamartomas will have a strongly negative value on the Hounsfield scale.
The growth velocity of a lesion is also informative: very fast or very slow growing tumors are rarely malignant, in contrary to inflammatory or congenital conditions.[5] It is therefore important to retrieve previous imaging studies to see if a lesion was presented and how fast its volume is increasing. This is more difficult for nodules smaller than 1 centimeter. Moreover, the predictive value of stable lesion over a period of 2 years has been found to be rather low and unreliable.[5]
Patient features
Several patient factors may influence the likelihood of a benign versus a malignant condition: these include previous exposure to smoke or other carcinogens such as asbestos, and previously diagnosed cancer or respiratory infections. A patient with airway symptoms, especially coughing up blood (hemoptysis), is more likely to have cancer compared to a patient with no respiratory symptoms.
Work-up
 FDG-PET study of a 71-year-old woman with a solitary pulmonary nodule (thin arrow) in the left lower lobe near the heart. The scan also revealed abnormal increased activity at the gastro-esophageal junction (thick arrow). The final diagnosis was non-Hodgkin lymphoma at both sites.
FDG-PET study of a 71-year-old woman with a solitary pulmonary nodule (thin arrow) in the left lower lobe near the heart. The scan also revealed abnormal increased activity at the gastro-esophageal junction (thick arrow). The final diagnosis was non-Hodgkin lymphoma at both sites.The work-up in patients with a solitary pulmonary nodule is based on an initial risk assessment. If the risk of malignancy is thought to be low, follow-up imaging (usually serial CT scans) can be planned at a later time. The frequency of further scans can be determined by the patient's risk for cancer and the size of the nodule.[6] If the initial impression is that there is a high likelihood of cancer, than a surgical intervention is appropriate (provided that the patient is fit for surgery).
If there is an intermediate risk of malignancy, further imaging with positron emission tomography (PET scan) is appropriate (if available). Around 95% of patients with a malignant nodule will have an abnormal PET scan, while around 78% of patients with a benign nodule will look normal on PET (this is the test sensitivity and specificity).[7] Thus, an abnormal PET scan will reliably pick up cancer, but several other types of nodules (inflammatory or infectious, for example) will also show up on a PET scan. If the nodule has a diameter below 1 centimeter, PET scans are often avoided because there is an increased risk of falsely normal results.[7][8][9] Cancerous lesions usually have a high metabolism on PET, as demonstrated by their high uptake of FDG (a radioactive sugar). If the lesion is found on further imaging to be suspicious, it should be surgically excised (via thoracotomy or video-assisted thoracic surgery) to confirm the diagnosis by microscopical examination.
In selected cases, nodules can also be sampled through the airways using bronchoscopy or through the chest wall using needle aspiration (which can be done under CT guidance). Needle aspiration can only retrieve groups of cells for cytology and not a tissue cylinder or biopsy, precluding evaluation of the tissue architecture. Theoretically, this makes the diagnosis of benign conditions more difficult, although rates higher than 90% have been reported.[10] Complications of the latter technique include hemorrhage into the lung and air leak in the pleural space between the lung and the chest wall (pneumothorax). However, not all these cases of pneumothorax need treatment with a chest tube.[11]
Other imaging techniques include PET-CT (simultaneous PET scan and CT scan with superposition of the images), magnetic resonance imaging (MRI) or single photon emission computed tomography (SPECT).[12]
Footnotes
- ^ a b Ost D, Fein AM, Feinsilver SH (June 2003). "Clinical practice. The solitary pulmonary nodule". N. Engl. J. Med. 348 (25): 2535–42. doi:10.1056/NEJMcp012290. PMID 12815140. http://content.nejm.org/cgi/pmidlookup?view=short&pmid=12815140&promo=ONFLNS19.
- ^ a b c Alzahouri K, Velten M, Arveux P, Woronoff-Lemsi MC, Jolly D, Guillemin F (2008). "Management of SPN in France. Pathways for definitive diagnosis of solitary pulmonary nodule: a multicentre study in 18 French districts". BMC Cancer 8: 93. doi:10.1186/1471-2407-8-93. PMC 2373300. PMID 18402653. http://www.biomedcentral.com/1471-2407/8/93.
- ^ Tan BB, Flaherty KR, Kazerooni EA, Iannettoni MD (January 2003). "The solitary pulmonary nodule". Chest 123 (1 Suppl): 89S–96S. doi:10.1378/chest.123.1_suppl.89S. PMID 12527568. http://www.chestjournal.org/cgi/pmidlookup?view=long&pmid=12527568.
- ^ a b c d Winer-Muram HT (April 2006). "The solitary pulmonary nodule". Radiology 239 (1): 34–49. doi:10.1148/radiol.2391050343. PMID 16567482. http://radiology.rsnajnls.org/cgi/pmidlookup?view=long&pmid=16567482.
- ^ a b Erasmus JJ, Connolly JE, McAdams HP, Roggli VL (2000). "Solitary pulmonary nodules: Part I. Morphologic evaluation for differentiation of benign and malignant lesions". Radiographics 20 (1): 43–58. PMID 10682770. http://radiographics.rsnajnls.org/cgi/pmidlookup?view=long&pmid=10682770.
- ^ MacMahon H, Austin JH, Gamsu G, et al. (November 2005). "Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society". Radiology 237 (2): 395–400. doi:10.1148/radiol.2372041887. PMID 16244247. http://radiology.rsnajnls.org/cgi/pmidlookup?view=long&pmid=16244247.
- ^ a b Gould MK, Maclean CC, Kuschner WG, Rydzak CE, Owens DK (February 2001). "Accuracy of positron emission tomography for diagnosis of pulmonary nodules and mass lesions: a meta-analysis". JAMA 285 (7): 914–24. doi:10.1001/jama.285.7.914. PMID 11180735. http://jama.ama-assn.org/cgi/pmidlookup?view=long&pmid=11180735.
- ^ Khan A (March 2007). "ACR Appropriateness Criteria on solitary pulmonary nodule". J Am Coll Radiol 4 (3): 152–5. doi:10.1016/j.jacr.2006.12.003. PMID 17412254. http://linkinghub.elsevier.com/retrieve/pii/S1546-1440(06)00694-6.
- ^ Vansteenkiste JF, Stroobants SS (January 2006). "PET scan in lung cancer: current recommendations and innovation". J Thorac Oncol 1 (1): 71–3. doi:10.1097/01243894-200601000-00014. PMID 17409830.
- ^ Klein JS, Salomon G, Stewart EA (March 1996). "Transthoracic needle biopsy with a coaxially placed 20-gauge automated cutting needle: results in 122 patients". Radiology 198 (3): 715–20. PMID 8628859. http://radiology.rsnajnls.org/cgi/pmidlookup?view=long&pmid=8628859.
- ^ Erasmus JJ, McAdams HP, Connolly JE (2000). "Solitary pulmonary nodules: Part II. Evaluation of the indeterminate nodule". Radiographics 20 (1): 59–66. PMID 10682771. http://radiographics.rsnajnls.org/cgi/pmidlookup?view=long&pmid=10682771.
- ^ Cronin P, Dwamena BA, Kelly AM, Carlos RC (2008). "Solitary pulmonary nodules: meta-analytic comparison of cross-sectional imaging modalities for diagnosis of malignancy". Radiology 246 (3): 772–82. doi:10.1148/radiol.2463062148. PMID 18235105. http://radiology.rsnajnls.org/cgi/pmidlookup?view=long&pmid=18235105.
Tumors: Mediastinal tumors/Thoracic neoplasm/respiratory neoplasia (C30–C34/D14, 160–163/212.0–212.4) Upper RT Lower RT Tracheal tumorSquamous cell carcinoma · Adenocarcinoma of the lung · Large-cell lung carcinoma · Rhabdoid carcinoma · Sarcomatoid carcinoma · Carcinoid · Salivary gland-like carcinoma of the lung · Adenosquamous carcinoma · Papillary adenocarcinomaNon-carcinomaBy locationPleura Categories:

Wikimedia Foundation. 2010.