- Lower respiratory tract infection
-
Lower respiratory tract infection Classification and external resources 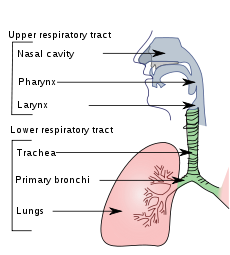
Conducting passages.ICD-10 J10-J22, J40-J47 Lower respiratory tract infection while often used as a synonym for pneumonia, can also be applied to other types of infection including lung abscess and acute bronchitis. Symptoms include shortness of breath, weakness, high fever, coughing and fatigue.
Lower respiratory tract infections place a considerable strain on the health budget and are generally more serious than upper respiratory infections. Since 1993 there has been a slight reduction in the total number of deaths from lower respiratory tract infection. However in 2002 they were still the leading cause of deaths among all infectious diseases, and they accounted for 3.9 million deaths worldwide and 6.9% of all deaths that year.[1]
There are a number of acute and chronic infections that can affect the lower respiratory tract. The two most common infections are bronchitis and pneumonia.[2] Influenza affects both the upper and lower respiratory tracts. Antibiotics are often thought to be the first line treatment in lower respiratory tract infections; however, these are not indicated in viral infections. It is important to use appropriate antibiotic selection based on the infecting organism and to ensure this therapy changes with the evolving nature of these infections and the emerging resistance to conventional therapies.[3] H. influenzae and M. catarrhalis are of increasing importance in both community acquired pneumonia (CAP) and acute exacerbation of chronic bronchitis (AECB) while the importance of S. pneumoniae is declining. It has also become apparent the importance of atypical pathogens such as C. pneumoniae, M. pneumoniae and L. pneumophila, in CAP.[3]
Contents
Classification
Bronchitis
Main article: BronchitisBronchitis can be classified as either acute or chronic. Acute bronchitis can be defined as acute bacterial or viral infection of the larger airways in healthy patients with no history of recurrent disease.[2] It affects over 40 adults per 1000 each year and consists of transient inflammation of the major bronchi and trachea.[4] Most often it is caused by viral infection and hence antibiotic therapy is not indicated in immunocompetent individuals.[5][6] There are no effective therapies for viral bronchitis.[6][7] Treatment of acute bronchitis with antibiotics is common but controversial as their use has only moderate benefit weighted against potential side effects (nausea and vomiting), increased resistance, and cost of treatment in a self-limiting condition.[4][8] Beta2 agonists are sometimes used to relieve the cough associated with acute bronchitis. In a recent systematic review it was found there was no evidence to support their use.[6]
Acute Exacerbations of Chronic Bronchitis (AECB) are frequently due to non-infective causes along with viral ones. 50% of patients are colonised with Haemophilus influenzae, Streptococcus pneumoniae or Moraxella catarrhalis.[2] Antibiotics have only been shown to be effective if all three of the following symptoms are present:- increased dyspnoea, increased sputum volume and purulence. In these cases 500 mg of Amoxycillin orally, every 8 hours for 5 days or 100 mg doxycycline orally for 5 days should be used.[2]
Pneumonia
Main article: PneumoniaPneumonia occurs in a variety of situations and treatment must vary according to the situation.[7] It is classified as either community or hospital acquired depending on where the patient contracted the infection. It is life-threatening in the elderly or those who are immunocompromised.[9][10] The most common treatment is antibiotics and these vary in their adverse effects and their effectiveness.[9] Pneumonia is also the leading cause of death in children less than five years of age.[11] The most common cause of pneumonia is pneumococcal bacteria, Streptococcus pneumoniae accounts for 2/3 of bacteremic pneumonias.[12] This is a dangerous type of lung infection with a mortality rate of around 25%.[10] For optimal management of a pneumonia patient the following must be assessed;- pneumonia severity (including where to treat e.g. Home, hospital or intensive care), identification of causative organism, analgesia of chest pain, the need for supplemental oxygen, physiotherapy, Hydration, bronchodilators and possible complications of emphysema or lung abscess.[13]
Treatment
Treatment depends on the cause thus see the appropriate page above.
Epidemiology
 Disability-adjusted life year for lower respiratory infections per 100,000 inhabitants in 2002.[14]
Disability-adjusted life year for lower respiratory infections per 100,000 inhabitants in 2002.[14] no dataless than 100100-700700-14001400-21002100-28002800-35003500-42004200-49004900-56005600-63006300-7000more than 7000
no dataless than 100100-700700-14001400-21002100-28002800-35003500-42004200-49004900-56005600-63006300-7000more than 7000References
- ^ Robert Beaglehole...et al. (2004) (PDF). The World Health Report 2004 - Changing History. World Health Organization. pp. 120–4. ISBN 92-4-156265-X. http://www.who.int/entity/whr/2004/en/report04_en.pdf.
- ^ a b c d Antibiotic Expert Group. Therapeutic guidelines: Antibiotic. 13th ed. North Melbourne: Therapeutic Guidelines; 2006.
- ^ a b Guthrie R (2001). "Community-acquired lower respiratory tract infections: etiology and treatment". Chest 120 (6): 2021–34. doi:10.1378/chest.120.6.2021. PMID 11742937. http://www.chestjournal.org/cgi/pmidlookup?view=long&pmid=11742937.
- ^ a b BJM Clinical evidence: London, United Kingdom: BMJ, 1999-2007 : Accessed 29/3/7 at : http://0-www.clinicalevidence.com.library.newcastle.edu.au/ceweb/index.jsp.
- ^ Therapeutic guidelines : respiratory. 2nd ed ed: North Melbourne : Therapeutic Guidelines Limited, 2000.
- ^ a b c Smucny J BL, Glazier R. . Beta2-agonists for acute bronchitis. Cochrane Database of Systematic Reviews 2006, Issue 4. Art. No.: CD001726. DOI: 10.1002/14651858.CD001726.pub3.
- ^ a b Integrated pharmacology / Clive Page ... [et al.]. 2nd ed ed: Edinburgh : Mosby, 2002.
- ^ Fahey T SJ, Becker L, Glazier R. . Antibiotics for acute bronchitis. Cochrane Database of Systematic Reviews 2004, Issue 4. Art. No.: CD000245. DOI: 10.1002/14651858.CD000245.pub2.
- ^ a b Bjerre LM VT, Kochen MM. . Antibiotics for community acquired pneumonia in adult outpatients. Cochrane Database of Systematic Reviews 2004, Issue 2. Art. No.: CD002109. DOI: 10.1002/14651858.CD002109.pub2.
- ^ a b Dear KB G AR, Holden J, Tatham DP. . Vaccines for preventing pneumococcal infection in adults. Cochrane Database of Systematic Reviews 2003, Issue 4. Art. No.: CD000422. DOI: 10.1002/14651858.CD000422.
- ^ Kabra SK LR, Pandey RM. . Antibiotics for community acquired pneumonia in children. Cochrane Database of Systematic Reviews 2006, Issue 3. Art. No.: CD004874. DOI: 10.1002/14651858.CD004874.pub2.
- ^ The Merck manual of diagnosis and therapy. 17th ed / Mark H. Beers and Robert Berkow ed: Whitehouse Station, N.J. : Merck Research Laboratories, 1999.
- ^ eTG complete [electronic resource] "?". http://0-www.etg.hcn.net.au.library.newcastle.edu.au/.
- ^ "Mortality and Burden of Disease Estimates for WHO Member States in 2002" (xls). World Health Organization. 2002. http://www.who.int/entity/healthinfo/statistics/bodgbddeathdalyestimates.xls.
Categories:- Acute lower respiratory infections
- Infectious diseases


Wikimedia Foundation. 2010.