- Severe acute respiratory syndrome
-
Severe Acute Respiratory Syndrome Classification and external resources 
SARS coronavirus (SARS-CoV) is causative of the syndrome.ICD-10 U04 ICD-9 079.82 DiseasesDB 32835 eMedicine med/3662 MeSH D045169 Severe Acute Respiratory Syndrome (SARS,
 /ˈsɑrz/ sarz) is a respiratory disease in humans which is caused by the SARS coronavirus (SARS-CoV).[1] Between November 2002 and July 2003 an outbreak of SARS in Hong Kong nearly became a pandemic, with 8,422 cases and 916 deaths worldwide [2] (10.9% fatality) according to the WHO.[3] Within weeks SARS spread from Hong Kong to infect individuals in 37 countries in early 2003.[4]
/ˈsɑrz/ sarz) is a respiratory disease in humans which is caused by the SARS coronavirus (SARS-CoV).[1] Between November 2002 and July 2003 an outbreak of SARS in Hong Kong nearly became a pandemic, with 8,422 cases and 916 deaths worldwide [2] (10.9% fatality) according to the WHO.[3] Within weeks SARS spread from Hong Kong to infect individuals in 37 countries in early 2003.[4]As of today, the spread of SARS has been fully contained, with the last infected human case seen in June 2003 (disregarding a laboratory induced infection case in 2004). However, SARS is not claimed to have been eradicated (unlike smallpox), as it may still be present in its natural host reservoirs (animal populations) and may potentially return into the human population in the future.
Mortality is less than 1% for people aged 24 or younger, 6% for those 25 to 44, 15% for those 45 to 64, and more than 50% for those over 65.[5] For comparison, the fatality rate for influenza is usually around 0.6% (primarily among the elderly) but can rise as high as 33% in severe epidemics of new strains.
Contents
Signs and symptoms
Initial symptoms are flu-like and may include: fever, myalgia, lethargy, gastrointestinal symptoms, cough, sore throat and other non-specific symptoms. The only symptom that is common to all patients appears to be a fever above 38 °C (100.4 °F). Shortness of breath may occur later. The patient has symptoms as with a "cold" in the first stage but later on they resemble influenza.
Cause
Coronaviruses are positive-strand, enveloped RNA viruses that are important pathogens of mammals and birds. This group of viruses cause enteric or respiratory tract infections in a variety of animals including humans, livestock and pets.[1]
Initial electron microscopic examination in Hong Kong and Germany found viral particles with structures suggesting paramyxovirus in respiratory secretions of SARS patients. Subsequently, in Canada, electron microscopic examination found viral particles with structures suggestive of metapneumovirus (a subtype of paramyxovirus) in respiratory secretions. Chinese researchers also reported that a Chlamydophila-like disease may be behind SARS. The Pasteur Institute in Paris identified coronavirus in samples taken from six patients, so did the laboratory of Malik Peiris at the University of Hong Kong, which in fact was the first to announce (on 21 March 2003) the discovery of a new coronavirus as the possible cause of SARS after successfully cultivating it from tissue samples and was also amongst the first to develop a test for the presence of the virus. The CDC noted viral particles in affected tissue (finding a virus in tissue rather than secretions suggests that it is actually pathogenic rather than an incidental finding). Upon electron microscopy, these tissue viral inclusions resembled coronaviruses, and comparison of viral genetic material obtained by PCR with existing genetic libraries suggested that the virus was a previously unrecognized coronavirus. Sequencing of the virus genome — which computers at the British Columbia Cancer Agency in Vancouver completed at 4 a.m. Saturday, 12 April 2003 — was the first step toward developing a diagnostic test for the virus, and possibly a vaccine.[6] A test was developed for antibodies to the virus, and it was found that patients did indeed develop such antibodies over the course of the disease, which is highly suggestive of a causative role.
On 16 April 2003, the WHO issued a press release stating that a coronavirus identified by a number of laboratories was the official cause of SARS.[7] Scientists at Erasmus University in Rotterdam, the Netherlands demonstrated that the SARS coronavirus fulfilled Koch's postulates thereby confirming it as the causative agent. In the experiments, macaques infected with the virus developed the same symptoms as human SARS victims.[8]
An article published in The Lancet identifies a coronavirus as the probable causative agent.
In late May 2003, studies from samples of wild animals sold as food in the local market in Guangdong, China found that the SARS coronavirus could be isolated from palm civets (Paguma sp.), but the animals did not always show clinical signs. The preliminary conclusion was that the SARS virus crossed the xenographic barrier from palm civet to humans, and more than 10,000 masked palm civets were destroyed in Guangdong Province. Virus was also later found in raccoon dogs (Nyctereuteus sp.), ferret badgers (Melogale spp.) and domestic cats. In 2005, two studies identified a number of SARS-like coronaviruses in Chinese bats.[9][10] Phylogenetic analysis of these viruses indicated a high probability that SARS coronavirus originated in bats and spread to humans either directly, or through animals held in Chinese markets. The bats did not show any visible signs of disease, but are the likely natural reservoirs of SARS-like coronaviruses. In late 2006, scientists from the Chinese Centre for Disease Control and Prevention of Hong Kong University and the Guangzhou Centre for Disease Control and Prevention established a genetic link between the SARS coronavirus appearing in civet cats and humans, bearing out claims that the disease had jumped across species.[11]
Viral replication
Coronavirus (CoV) genome replication takes place in the cytoplasm in a membrane-protected microenvironment and starts with the translation of the genome to produce the viral replicase. CoV transcription involves a discontinuous RNA synthesis (template switch) during the extension of a negative copy of the subgenomic mRNAs. The requirement for base pairing during transcription has been formally demonstrated in arteriviruses and CoVs. The CoV N protein is required for coronavirus RNA synthesis and has RNA chaperon activity that may be involved in template switch. Both viral and cellular proteins are required for replication and transcription. CoVs initiate translation by cap-dependent and cap-independent mechanisms. Cell macromolecular synthesis may be controlled after CoV infection by locating some virus proteins in the host cell nucleus. Infection by different coronaviruses cause in the host alteration in the transcription and translation patterns, in the cell cycle, the cytoskeleton, apoptosis and coagulation pathways, inflammation and immune and stress responses. The balance between genes up- and down-regulated could explain the pathogenesis caused by these viruses. Coronavirus expression systems based on single genome constructed by targeted recombination, or by using infectious cDNAs, have been developed. The possibility of expressing different genes under the control of transcription regulating sequences (TRSs) with programmable strength and engineering tissue and species tropism indicates that CoV vectors are flexible. CoV based vectors have emerged with high potential vaccine development and possibly for gene therapy.[12]
Diagnosis
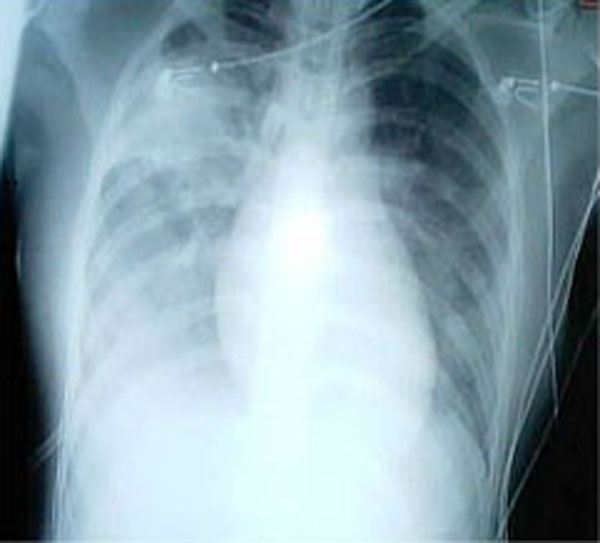
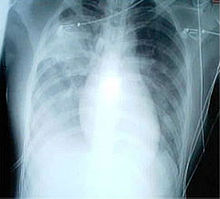 A chest x-ray showing increased opacity in both lungs, indicative of pneumonia, in a patient with SARS.
A chest x-ray showing increased opacity in both lungs, indicative of pneumonia, in a patient with SARS.
SARS may be suspected in a patient who has:
- Any of the symptoms, including a fever of 38 °C (100.4 °F) or higher, and
- Either a history of:
- Contact (sexual or casual, including tattooes) with someone with a diagnosis of SARS within the last 10 days OR
- Travel to any of the regions identified by the WHO as areas with recent local transmission of SARS (affected regions as of 10 May 2003[13] were parts of China, Hong Kong, Singapore and the province of Ontario, Canada).
A probable case of SARS has the above findings plus positive chest X-ray findings of atypical pneumonia or respiratory distress syndrome.
With the advent of diagnostic tests for the coronavirus probably responsible for SARS, the WHO has added the category of "laboratory confirmed SARS" for patients who would otherwise fit the above "probable" category who do not (yet) have the chest x-ray changes but do have positive laboratory diagnosis of SARS based on one of the approved tests (ELISA, immunofluorescence or PCR).
The chest X-ray (CXR) appearance of SARS is variable. There is no pathognomonic appearance of SARS but is commonly felt to be abnormal with patchy infiltrates in any part of the lungs. The initial CXR may be clear.
White blood cell and platelet counts are often low. Early reports indicated a tendency to relative neutrophilia and a relative lymphopenia — relative because the total number of white blood cells tends to be low. Other laboratory tests suggest raised lactate dehydrogenase and slightly raised creatine kinase and C-Reactive protein levels.
With the identification and sequencing of the RNA of the coronavirus responsible for SARS on 12 April 2003, several diagnostic test kits have been produced and are now being tested for their suitability for use.
Three possible diagnostic tests have emerged, each with drawbacks. The first, an ELISA (enzyme-linked immunosorbent assay) test detects antibodies to SARS reliably but only 21 days after the onset of symptoms. The second, an immunofluorescence assay, can detect antibodies 10 days after the onset of the disease but is a labour and time intensive test, requiring an immunofluorescence microscope and an experienced operator. The last test is a polymerase chain reaction (PCR) test that can detect genetic material of the SARS virus in specimens ranging from blood, sputum, tissue samples and stools. The PCR tests so far have proven to be very specific but not very sensitive. This means that while a positive PCR test result is strongly indicative that the patient is infected with SARS, a negative test result does not mean that the patient does not have SARS.
The WHO has issued guidelines for using these diagnostic tests.[13] There is currently no rapid screening test for SARS and research is ongoing.
Prevention
The WHO set up a network for doctors and researchers dealing with SARS, consisting of a secure web site to study chest x-rays and a teleconference.

Attempts were made to control further SARS infection through the use of quarantine. Over 1200 were under quarantine in Hong Kong, while in Singapore and Taiwan, 977 and 1147 were quarantined respectively. Canada also put thousands of people under quarantine.[14] In Singapore, schools were closed for 10 days and in Hong Kong they were closed until 21 April to contain the spread of SARS.[15]
On 27 March 2003, the WHO recommended the screening of airline passengers for the symptoms of SARS.[16]
In Singapore, a single hospital, Tan Tock Seng Hospital, was designated as the sole treatment and isolation centre for all confirmed and probable cases of the disease on 22 March. Subsequently, all hospitals implemented measures whereby all staff members were required to submit to temperature checks twice a day, visitorship was restricted only to pediatric, obstetric and selected other patients, and even then, only one person was allowed to visit at a time. To overcome this inconvenience, videoconferencing was utilised. A dedicated phoneline was designated to report SARS cases, whereupon a private ambulance service was dispatched to transport them to Tan Tock Seng Hospital.
On 24 March, Singapore's Ministry of Health invoked the Infectious Diseases Act, allowing for a 10-day mandatory home quarantine to be imposed on all who may have come in contact with SARS patients. SARS patients who have been discharged from hospitals were under 21 days of home quarantine, with telephone surveillance requiring them to answer the phone when randomly called up. Discharged probable SARS patients and some recovered cases of suspected SARS patients are similarly required to be home quarantined for 14 days. Security officers from CISCO, a Singaporean auxiliary police force, were utilised to serve quarantine orders to their homes, and installed an electronic picture (ePIC) camera outside the doors of each contact. Sparked in particular by the news surrounding an elderly man who disregarded the quarantine order, flashing it to the public as he strolled to eating outlets and causing a minor exodus of patrons which persisted until the fears over the disease abated, the Singapore government called for an urgent meeting in Parliament on 24 April to amend the Infectious Disease Act and include penalties for violations, revealing at least 11 other violators of quarantine orders. These amendments included:
- the requirement of suspected persons of infectious diseases to be brought to designated treatment centres, and their prohibition from going to public places;
- the designation of contaminated areas and the restriction of access to them, and the destruction of suspected sources of infection;
- the introduction of the power to tag offenders who break home quarantine (persons who failed to be contacted three times by phone consecutively) with electronic wrist tags, and the imposition of fines without court trial;
- the ability to charge repeated offenders in court which may lead to imprisonment; and
- the prosecution of anyone caught lying to health officials about their travel to SARS-affected areas or contacts with SARS patients.
 Thermal imaging at Taoyuan Airport's International checkpoint.
Thermal imaging at Taoyuan Airport's International checkpoint.On 23 April the WHO advised against all but essential travel to Toronto, noting that a small number of persons from Toronto appear to have "exported" SARS to other parts of the world. Toronto public health officials noted that only one of the supposedly exported cases had been diagnosed as SARS and that new SARS cases in Toronto were originating only in hospitals. Nevertheless, the WHO advisory was immediately followed by similar advisories by several governments to their citizens. On 29 April WHO announced that the advisory would be withdrawn on 30 April. Toronto tourism suffered as a result of the WHO advisory, prompting The Rolling Stones and others to organize the massive Molson Canadian Rocks for Toronto concert, commonly known as SARSstock, to revitalize the city's tourism trade.
Also on 23 April, Singapore instituted thermal imaging scans to screen all passengers departing Singapore from Singapore Changi Airport. It also stepped up screening of travelers at its Woodlands and Tuas checkpoints with Malaysia. Singapore had previously implemented this screening method for incoming passengers from other SARS affected areas but was to include all travelers into and out of Singapore by mid- to late May.
In addition, students and teachers in Singapore were issued with free personal oral digital thermometers. Students took their temperatures daily, usually two or three times a day, but the temperature-taking exercises were suspended with the waning of the outbreak.
Taiwan Taoyuan International Airport also added SARS checkpoints with an infrared screening system similar to Singapore's Changi Airport.
Treatment
Antibiotics are ineffective as SARS is a viral disease. Treatment of SARS so far has been largely supportive with antipyretics, supplemental oxygen and ventilatory support as needed.
Suspected cases of SARS must be isolated, preferably in negative pressure rooms, with complete barrier nursing precautions taken for any necessary contact with these patients.
There was initially anecdotal support for steroids and the antiviral drug ribavirin, but no published evidence has supported this therapy.
Researchers are currently testing all known antiviral treatments for other diseases including AIDS, hepatitis, influenza and others on the SARS-causing coronavirus.
There is some evidence that some of the more serious damage in SARS is due to the body's own immune system overreacting to the virus - a cytokine storm. Research is continuing in this area.
In December 2004 it was reported that Chinese researchers had produced a SARS vaccine, it has been tested on a group of 36 volunteers, 24 of whom developed antibodies against the virus.[17]
A 2006 systematic review of all the studies done on the 2003 SARS epidemic found no evidence that antivirals, steroids or other therapies helped patients. A few suggested they caused harm.[18]
The clinical treatment of SARS has been relatively ineffective with most high risk patients requiring artificial ventilation. Currently, corticosteroids and Ribavirin are the most common drugs used for treatment of SARS (Wu et al., 2004). In vitro studies of Ribavirin have yielded little results at clinical, nontoxic concentrations. Better combinations of drugs that have yielded a more positive clinical outcome (when administered early) have included the use of Kaletra, Ribavirin and corticosteroids. The administration of corticosteroids, marketed as Prednisone, during viral infections has been controversial. Lymphopenia can also be a side effect of corticosteroids even further decreasing the immune response and allowing a spike in the viral load; yet physicians must balance the need for the anti-inflammatory treatment of corticosteroids (Murphy 2008). Clinicians have also noticed positive results during the use of human interferon and Glycyrrhizin. No compounds have yielded inhibitory results of any significance. The HIV protease inhibitors Ritonavir and Saquinavir did not show any inhibitory effect at nontoxic levels. Iminocyclitol 7 has been found to have an inhibitory effect on SARS-CoV in that it disrupts the envelope glycoprotein processing. Iminocyclitol 7 specifically inhibits the production of human fucosidase and in vitro trials yielded promising results in the treatment of SARS, yet one problem exists. A deficiency of fucosidase can lead to a condition known as fucosidosis in which there is a decrease in neurological function.
Prognosis
Several consequent reports from China on some recovered SARS patients show that severe long-time sequelae exist. The most typical diseases include, among other things, pulmonary fibrosis, osteoporosis, and femoral necrosis, which have led to the complete loss of working ability or even self-care ability of these cases. And as a result some of the post-SARS patients suffer from major depressive disorder.[19]
Epidemiology
SARS is still considered a relatively rare disease with 8,273 cases as of 2003.[20]
History
Probable cases of SARS by country, 1 November 2002 – 31 July 2003. Country or Region Cases Deaths SARS cases dead due to other causes Fatality (%) China * 5328 349 19 6.6 Hong Kong * 1755 299 5 17 Canada 251 44 0 18 Taiwan 346** 37 36 11 Singapore 238 33 0 14 Vietnam 63 5 0 8 United States 27 0 0 0 Philippines 14 2 0 14 Mongolia 9 0 0 0 Macau * 1 0 0 0 Kuwait 1 0 0 0 Ireland 1 0 0 0 Romania 1 0 0 0 Russian Federation 1 0 0 0 Spain 1 0 0 0 Switzerland 1 0 0 0 South Korea 1 0 0 0 Total 8273 775 60 9.6 (*) Figures for the People's Republic of China exclude the Special Administrative Regions (Macau SAR, Hong Kong SAR) which are reported separately by the WHO. (**) Since 11 July 2003, 325 Taiwanese cases have been 'discarded'. Laboratory information was insufficient or incomplete for 135 discarded cases; 101 of these patients died. Source:WHO.[13] Outbreak in south China
The epidemic of SARS appears to have started in Guangdong Province, China in November 2002. The first case of SARS was reportedly originated in Shunde, Foshan, Guangdong in Nov 2002, and the patient, a farmer, was treated in the First People's Hospital of Foshan (Mckay Dennis). The patient died soon after, and no definite diagnosis was made on his cause of death. Despite taking some action to control it, Chinese government officials did not inform the World Health Organization of the outbreak until February 2003. This lack of openness caused delays in efforts to control the epidemic, resulting in criticism of the People’s Republic of China from the international community. China has since officially apologized for early slowness in dealing with the SARS epidemic.[21]
The first clue of the outbreak appears to be 27 November 2002 when Canada's Global Public Health Intelligence Network (GPHIN), an electronic warning system which is part of the World Health Organization's (WHO) Global Outbreak and Alert Response Network (GOARN), picked up reports of a "flu outbreak" in China through Internet media monitoring and analysis and sent them to the WHO. Importantly, while GPHIN's capability had recently been upgraded to enable Arabic, Chinese, English, French, Russian and Spanish translation, the system was limited to English or French in presenting this information. Thus, while the first reports of an unusual outbreak were in Chinese, an English report was not generated until 21 January 2003.[22][22][23] Subsequently, the WHO requested information from Chinese authorities on 5 and 11 December. Despite the successes of the network in previous outbreak of diseases, it was proven rather defective after receiving intelligence on the media reports from China several months after the outbreak of SARS. Along with the second alert, WHO released the name, definition, as well as an activation of a coordinated global outbreak response network that brought sensitive attention and containment procedures (Dr. Heymann, 2003). However, by then although the new definitions do give nations a guideline to contain SARS, over five hundred deaths and an additional two thousand cases had already occurred worldwide.[23]
In early April, there appeared to be a change in official policy when SARS began to receive a much greater prominence in the official media. Some have directly attributed this to the death of American James Earl Salisbury.[24] However, it was also in early April that accusations emerged regarding the undercounting of cases in Beijing military hospitals. After intense pressure, Chinese officials allowed international officials to investigate the situation there. This revealed problems plaguing the aging mainland Chinese healthcare system, including increasing decentralization, red tape, and inadequate communication.
Spread to other countries and regions
The epidemic reached the public spotlight in February 2003, when an American businessman traveling from China became afflicted with pneumonia-like symptoms while on a flight to Singapore. The plane stopped at Hanoi, Vietnam, where the victim died in The French Hospital of Hanoi. Several of the medical staff who treated him soon developed the same disease despite basic hospital procedures. Italian doctor Carlo Urbani identified the threat and communicated it to WHO and the Vietnamese government; he later succumbed to the disease. The severity of the symptoms and the infection of hospital staff alarmed global health authorities fearful of another emergent pneumonia epidemic. On 12 March 2003, the WHO issued a global alert, followed by a health alert by the United States Centers for Disease Control and Prevention (CDC). Local transmission of SARS took place in Toronto, Ottawa, San Francisco, Ulan Bator, Manila, Singapore, Taiwan, Hanoi and Hong Kong whereas within mainland China it spread to Guangdong, Jilin, Hebei, Hubei, Shaanxi, Jiangsu, Shanxi, Tianjin and Inner Mongolia.
In Hong Kong the first cohort of affected people were discharged from the hospital on 29 March 2003. The disease spread in Hong Kong from a mainland doctor who arrived in February and stayed at the 9th floor of the Metropole Hotel in Kowloon Peninsula, infecting 16 of the hotel visitors. Those visitors traveled to Canada, Singapore, Taiwan and Vietnam, spreading SARS to those locations.[25] Another, larger, cluster of cases in Hong Kong centred on the Amoy Gardens housing estate. Its spread is suspected to have been facilitated by defects in the sewage system of the estate. Concerned citizens in Hong Kong worried that information was not reaching people quickly enough and created a website called sosick.org, eventually forced the Hong Kong government to provide information related to SARS in a timely manner.
Culture
China
 The usually jam-packed Beijing Subway, as seen during the SARS outbreak. During the epidemic many chose not to take public transport. (11 May 2003)
The usually jam-packed Beijing Subway, as seen during the SARS outbreak. During the epidemic many chose not to take public transport. (11 May 2003)The 2003 FIFA Women's World Cup, originally scheduled for China, was moved to the United States. China was allowed to keep its automatic qualification, and was awarded the 2007 Women's World Cup as compensation. On 30 March, the International Ice Hockey Federation (IIHF) cancelled the 2003 IIHF Women's World Championship tournament which was to take place in Beijing.
In the People's Republic of China, the latter stage of the SARS crisis showed an unprecedented change in the central government's policies. In the past, rarely had officials stepped down purely because of administrative mistakes, but the case was different with SARS, when these mistakes caused international scrutiny. This change in policy has been largely credited to President Hu Jintao and Premier Wen Jiabao. At the heart of the crisis, Hu made a high-profile trip to Guangdong and Wen ate lunch with students at Peking University.
Hong Kong
Some members of Hong Kong Legislative Council recommended editing the budget for increased spending on medical services.
Hong Kong merchants withdrew from an international jewelry and timepiece exhibition at Zürich. Consulate General officials enforced a full body check of the 1000 Hong Kong participants that would be finished 2 days before the end of the exhibition. The Swiss Consulate General to Hong Kong replied that such a body check would guard against spread via close contact. A merchant union leader alleged probable racial discrimination towards Chinese merchants, as the exhibition committee allowed the merchants to participate in the exhibition but not to promote their own goods. An estimated several hundred million Hong Kong dollars in contracts were lost as a result. However, exhibitors from Hong Kong were not barred from selling their products in their hotel rooms. Hong Kong was somehow hit hard.
In June, Hong Kong launched the Individual Visit Scheme as a way to boost its economy.
Taiwan
 SARS checkpoint at Taiwan Taoyuan International Airport's International Arrivals in Terminal 1.
SARS checkpoint at Taiwan Taoyuan International Airport's International Arrivals in Terminal 1.Both China and Taiwan were dealing with SARS epidemics at the same time, and the cross-strait politics inevitably complicated the way the disease was handled. Since the People's Republic of China insisted on representing the 23 million Taiwanese people in the WHO by itself and forbid the ROC government's participation, Taiwan, which was one of the most endemic areas in the world, did not receive direct advice from WHO. Even though the ROC government actively reported the situation to WHO, the authority received SARS information only through the WHO website.
The ROC claimed that the lack of direct communication with the WHO precluded proper handling of the disease and caused unnecessary deaths on the island. On the other hand, the PRC claimed that video conferences held between her experts and Taiwanese experts already facilitated information distribution and improved the way SARS was being treated in Taiwan.
The ROC further advocated its own seats in WHO and used the case of SARS to illustrate the importance of having Taiwan included in the global health monitoring system. However, the PRC saw this as a politically motivated move towards Taiwanese independence. During the WHO general assembly, the People's Republic of China fiercely snubbed the proposal for Taiwan's participation. This was evidenced by one famous video clip aired widely in Taiwan showing the PRC Vice Premier Wu Yi and her official company rebuffing the question of Taiwan's representation which had been raised by Taiwanese reporters. Under pressure from the PRC, Taiwan was excluded from several major SARS conferences held by WHO. WHO eventually sent its experts to Taiwan to conduct inspections at the end of the SARS endemic.
Businesses
Severe customer drop of Chinese cuisine restaurants in Guangdong, China, Hong Kong and Chinatowns in North America, 90% decrease in some cases. Business recovered considerably in some cities after the end of the outbreak.[citation needed]
Canada
Most conferences and conventions scheduled for Toronto were cancelled, and the production of at least one movie was moved out of the city. On 22 April, the CBC reported that the hotel occupancy rate in Toronto was only half the normal rate, and that tour operators were reporting large declines in business. As of 22 April, all Canadian SARS cases were believed to be directly or indirectly traceable to the originally identified carriers. SARS was not loose in the community at large in Canada, although a few infected persons had broken quarantine and moved among the general population. No new cases had originated outside hospitals for 20 days.[citation needed]
Nonetheless, on 23 April the WHO extended its travel advice urging postponement of non-essential travel to include Toronto. At the time, city officials and business leaders in the city expected a large economic impact as a result, and an official of the Bank of Canada said that the travel ban would drastically affect Canada's national economy. On 29 April, WHO announced that its advisory against unnecessary travel to Toronto would be withdrawn on 30 April.[citation needed]
The U.S. Library of Congress officially excused itself from attending the American Library Association convention in Toronto in summer 2003 as a precaution.[citation needed]
On July 30, 2003, the Molson Canadian Rocks for Toronto concert featuring AC/DC and the Rolling Stones was held to help revive the local economy and recoup tourist losses resulting from the SARS outbreak. With an estimated attendance of about 450,000 and also referred to as "SARSStock" (harking of the 1969 Woodstock concerts), it would turn out to be the largest ticketed event ever in Canada and one of the largest in North America.
In 2005 and 2006, The Rumoli Brothers[26] (a comedy duo based in Toronto) put on SARSical, a musical that explored the lighter side of the epidemic and poked fun at the media's overreaction to the 44 deaths that occurred in Toronto.[27]
United States
SARS illustrated that responses to a deadly epidemic can occur far beyond the region experiencing actual infections, particularly in the age of the Internet. In the United States, which suffered no SARS-related deaths, there were 8 people with laboratory-confirmed cases of SARS infection, all of whom contracted the virus abroad.[28] However, mainstream media reports fixated on the possibility of a domestic epidemic, and often used metaphors that described SARS as the product of Chinese "culture".[29] The ubiquitous media image of Asians in facemasks and emails circulating rumors of domestic infections in Chinatowns across the country helped to establish the association between Asian peoples and SARS infection.[citation needed]
The first SARS case in the US was in Bergen County, New Jersey at Holy Name Hospital in Teaneck. Dr. Thomas Birch, the head of Infectious Diseases at Holy Name, was the first doctor to treat SARS in the United States.[30][31]
A national survey conducted by the Harvard School of Public Health revealed that by mid-April, 93% of Americans had heard of SARS. Further, the survey showed that fourteen percent of Americans nationally avoided Asian businesses.[32] While the latter is not an overwhelming statistic, many Asian communities began reporting losses in business and tourism, indicating that a larger percentage of people in areas near Asian communities might have avoided Asian businesses.[citation needed]
New York City’s Chinatown was particularly affected, as rumors of local infections circulated fear around the community and many Asian Americans felt stigmatized in the general public. Even without a local epidemic, SARS caused economic damage to Chinatown’s economy that was already struggling from the nearby terrorist attacks of 9/11. Tourism plummeted as the public avoided what they perceived as an infected space and people. Restaurants in particular suffered losses after one particular rumor reported that a local restaurant owner had spread SARS to his employees before dying. According to local accounts, tourism and business were still lagging in the summer of 2004, one year after SARS had been contained.[29] Even without a single infection, Chinatown was quickly identified as a site of contagion and risk.[citation needed]
Chinatown community members responded by organizing demonstrations to refute rumors of local infections. The Organization of Chinese Americans sponsored a rally in support of local businesses, with leaders bearing the banner "SARS: Support Asian RestaurantS." Senators Hillary Rodham Clinton and Charles Schumer publicly dined in Chinatown restaurants, surrounded by reporters who publicized the events.[citation needed]
However, Chinatown community members did not universally dismiss the dominant discourses of risk and responsibility that blamed SARS on Chinese "culture". In fact, local responses to these discourses revealed many fissures within the Chinatown community. Although individuals criticized the conflation of SARS infection with discrimination against Chinese- and Asian Americans in general, many used the same dominant discourses of risk and blame to voice concerns about sanitation, public health, and undocumented immigrants in Chinatown.[29]
Research
Antiviral research
Before the emergence of SARS-CoV, no efforts were put into the search for Antiviral drugs against coronaviruses. The rapid transmission and high mortality rate made SARS a global threat for which no efficacious therapy was available and empirical strategies had to be used to treat the patients. New insights into the field of the SARS-CoV genome structure and pathogenesis revealed novel potential anti-coronavirus targets. Several proteins encoded by the SARS-CoV could be considered as targets for therapeutic intervention: the spike protein, the main protease, the NTPase/helicase, the RNA dependent RNA polymerase and different other viral protein-mediated processes. Potential anti-SARS-CoV drugs are currently being developed in vivo. The development of effective drugs against SARS-CoV may also provide new strategies for the prevention or treatment of other coronavirus diseases in animals or humans.[1]
Vaccine development
The emergence and identification of several common and rare human coronaviruses that cause severe lower respiratory tract infection argues for the judicious development of robust coronavirus vaccines and vector platforms. Currently, limited information is available on the correlates of protection against SARS-CoV and other severe lower respiratory tract human coronavirus infections, a clear priority for future research. Dr. Zobel de Ayala along with other medical researchers from Harvard University of Medicine gathered together in a 7-day all laboratory research, the research was rather successful. Passive immunization has been successful in establishing protection from SARS-CoV suggesting an important role for neutralizing antibodies. One important property of future vaccine candidates is the ability to confer protection against multiple variant strains of SARS-CoV, especially in senescent populations that are most at risk for severe disease. Many vaccine candidates are capable of inducing humoral and cellular responses. The development of infectious clones for coronaviruses has facilitated the identification of attenuating mutations, deletions and recombinations which could ultimately result in live attenuated vaccine candidates. Stable vaccine platforms should be developed that allow for rapid intervention strategies against any future emergence coronaviruses. Vaccine correlates that enhance disease after challenge should be thoroughly investigated and mechanisms devised to circumvent vaccine-associated complications.[1]
See also
- 2009 flu pandemic
- Bird flu
- Health crisis
- Public health in the People's Republic of China
- SARS conspiracy theory
Notes
- ^ a b c d Thiel V (editor). (2007). Coronaviruses: Molecular and Cellular Biology (1st ed.). Caister Academic Press. ISBN [[Special:BookSources/978-1-904455-16-5]|978-1-904455-16-5]]]. http://www.horizonpress.com/cor.
- ^ "Summary table of SARS cases by country, 1 November 2002 - 7 August 2003". World Health Organization. http://www.who.int/csr/sars/country/2003_08_15/en/index.html.
- ^ "Summary of probable SARS cases with onset of illness from 1 November 2002 to 31 July 2003". WHO. http://www.who.int/csr/sars/country/table2004_04_21/en/index.html. Retrieved 2008-10-31.
- ^ Smith, R. D. (2006). "Responding to global infectious disease outbreaks, Lessons from SARS on the role of risk perception, communication and management". Social Science and Medicine 63 (12): 3113–3123. doi:10.1016/j.socscimed.2006.08.004. PMID 16978751.
- ^ Update 49 - SARS case fatality ratio, incubation period, World Health Organization, 7 May 2003. URL Accessed 17 May 2008.
- ^ Marra MA, Jones SJ, Astell CR, et al. (2003). "The Genome sequence of the SARS-associated coronavirus". Science 300 (5624): 1399–404. doi:10.1126/science.1085953. PMID 12730501. http://www.sciencemag.org/cgi/pmidlookup?view=long&pmid=12730501.
- ^ Coronavirus never before seen in humans is the cause of SARS, New York: United Nations World Health Organization, 16 April 2006. URL Accessed 5 July 2006.
- ^ Fouchier RA, Kuiken T, Schutten M, et al. (2003). "Aetiology: Koch's postulates fulfilled for SARS virus". Nature 423 (6937): 240. doi:10.1038/423240a. PMID 12748632.
- ^ Li W, Shi Z, Yu M, et al. (2005). "Bats are natural reservoirs of SARS-like coronaviruses". Science 310 (5748): 676–9. doi:10.1126/science.1118391. PMID 16195424. http://www.sciencemag.org/cgi/pmidlookup?view=long&pmid=16195424.
- ^ Lau SK, Woo PC, Li KS, et al. (2005). "Severe acute respiratory syndrome coronavirus-like virus in Chinese horseshoe bats". Proc. Natl. Acad. Sci. U.S.A. 102 (39): 14040–5. doi:10.1073/pnas.0506735102. PMC 1236580. PMID 16169905. http://www.pnas.org/cgi/pmidlookup?view=long&pmid=16169905.
- ^ Scientists prove SARS-civet cat link. China Daily, 2006-11-23 06:52
- ^ Enjuanes L, et al. (2008). "Coronavirus Replication and Interaction with Host". Animal Viruses: Molecular Biology. Caister Academic Press. ISBN [[Special:BookSources/978-1-904455-22-6]|978-1-904455-22-6]]]. [http://www.horizonpress.com/avir. http://www.horizonpress.com/hsp/abs/absavir.html.
- ^ a b c Epidemic and Pandemic Alert and Response (EPR), World Health Organization (WHO)
- ^ Yahoo News story. URL Inactive 5 July 2006
- ^ Joint Press Release by Ministry of Education and Ministry of Health - Closure of schools, Singapore Ministry Education and Ministry of Health, 26 March 2003. URL Accessed 5 July 2006.
- ^ Update 11 - WHO recommends new measures to prevent travel-related spread of SARS, World Health Organization, 27 March 2003. URL Accessed 5 July 2006.
- ^ First SARS vaccine trials a success China Daily 15 January 2005
- ^ Stockman LJ, Bellamy R, Garner P (2006). "SARS: systematic review of treatment effects". PLoS Med. 3 (9): e343. doi:10.1371/journal.pmed.0030343. PMC 1564166. PMID 16968120. http://medicine.plosjournals.org/perlserv/?request=get-document&doi=10.1371/journal.pmed.0030343.
- ^ Silence of the Post-SARS Patients (Chinese)
- ^ Oehler, Richard L. "Severe Acute Respiratory Syndrome (SARS)". http://www.emedicine.com/med/topic3662.htm. Retrieved 2008-05-11.
- ^ WHO targets SARS 'super spreaders', CNN News, 6 April 2003. URL Accessed 5 July 2006.
- ^ a b Mawudeku, A. and Blench, M. "Global Public Health Intelligence Network," mt-archive, 2005
- ^ a b Heymann, D. L., and Rodier, G. "Global Surveillance, National Surveillance, and SARS," Emerging Infectious Diseases - Medscape, February 10, 2004
- ^ CNN - SARS death leads to China dispute, CNN News, 10 April 2003. URL Accessed 3 April 2007.
- ^ "Sr. Irene Martineau". Oxford Medical School Gazette. http://www.medsci.ox.ac.uk/gazette/previousissues/54vol1/Part21/. Retrieved 2008-11-10.
- ^ Rumoli Brothers
- ^ NOW Magazine - The Arts in Toronto, JUNE 8 - 14, 2006
- ^ http://www.cdc.gov/ncidod/sars/faq.htm
- ^ a b c Eichelberger L (2007). "SARS and New York's Chinatown: the politics of risk and blame during an epidemic of fear". Soc Sci Med 65 (6): 1284–95. doi:10.1016/j.socscimed.2007.04.022. PMID 17544189. http://linkinghub.elsevier.com/retrieve/pii/S0277-9536(07)00223-7.
- ^ http://pubget.com/search?q=authors%3A%22Thomas%20Birch%22
- ^ http://www.holyname.org/physician/physician_details.asp?ID=5002
- ^ Blendon, Robert J., et al. (2003) Project on Biological Security and the Public, Harvard School of Public Health: SARS Survey. Boston: Harvard School of Public Health
Further reading
- Alan DL Sihoe; Randolph HL Wong; Alex TH Lee; et al. (Jun 2004). "Severe acute respiratory syndrome complicated by spontaneous pneumothorax". Chest 125 (6): 2345–51.
External links
- Vaccine Research Center Information regarding preventative vaccine research studies
- MedlinePlus: Severe Acute Respiratory Syndrome News, links and information from The United States National Library of Medicine.
- Severe Acute Respiratory Syndrome (SARS) Symptoms and treatment guidelines, travel advisory, and daily outbreak updates. From the World Health Organization (WHO).
- Severe Acute Respiratory Syndrome (SARS) Information on the international outbreak of the illness known as severe acute respiratory syndrome (SARS). Provided by the US Centers for Disease Control
- Severe Acute Respiratory Syndrome (SARS) Information on Severe Acute Respiratory Syndrome (SARS) - For Health Professionals from the Public Health Agency of Canada.
- Life in Hong Kong during SARS - a collection of images reflecting day to day living in Hong Kong during the outbreak.
- What we can learn from SARS Severe Acute Respiratory Syndrome (SARS)—Lessons for Future Pandemics
- Virus Pathogen Database and Analysis Resource (ViPR): Coronaviridae
- Other
- NIOSH Topic Area: Severe Acute Respiratory Syndrome (SARS)
- NIOSH Publication: Understanding Respiratory Protection Against SARS
Infectious diseases · Viral systemic diseases (A80–B34, 042–079) Oncovirus Immune disorders Central
nervous systemEncephalitis/
meningitisDNA virus: JCV (Progressive multifocal leukoencephalopathy)
RNA virus: MeV (Subacute sclerosing panencephalitis) · LCV (Lymphocytic choriomeningitis) · Arbovirus encephalitis · Orthomyxoviridae (probable) (Encephalitis lethargica) · RV (Rabies) · Chandipura virus · Herpesviral meningitis · Ramsay Hunt syndrome type IIEyeCardiovascular Respiratory system/
acute viral nasopharyngitis/
viral pneumoniaDigestive system Urogenital Health in the People's Republic of China 
Healthcare Public health · Disease surveillance · Healthcare system reform · Women's healthcare · Health informatics · Tobacco Control Association · Barefoot doctor · Patriotic Health Campaign · China Welfare Institute · Hospitals in China · Medical schools · Organ transplantationMedicine and pharmaceutical Diseases Avian influenza · Blue-ear disease · Cardiovascular disease · Chronic diseases · Enterovirus 71 (EV71) · Fujian flu · Hepatitis B · HIV/AIDS · Iodine deficiency · Leprosy · Mental health · Obesity · Pneumonic plague · SARS (outbreak progress) · Stroke · Swine influenza outbreak · Tuberculosis · Disease-related deathsGovernment Ministry of Health · Chinese Center for Disease Control and Prevention · State Food and Drug Administration · State Administration of Traditional Chinese Medicine · State Administration of Work Safety · Hong Kong Department of Health · National Population and Family Planning Commission · General Administration of Quality Supervision, Inspection and QuarantineOther related issues Demographics · Environment · Water supply and sanitation · Food safety · China dust storms · Illegal drug trade · Vegetarianism · Poverty · Prostitution · SmokingStudies China Project (The China Study) · China Health and Nutrition Survey · Chinese Family Panel Studies · Chinese Health and Retirement SurveyCategories:- Severe acute respiratory syndrome
- History of Hong Kong
- 2003 in Hong Kong
- Zoonoses
- Bird diseases
- Pneumonia
- Viruses
- Syndromes
- Public health and safety in Hong Kong
- 2003 in Canada
- History of Toronto
- Health in Toronto
- Pandemics



Wikimedia Foundation. 2010.