- Community-acquired pneumonia
-
Community-acquired pneumonia (CAP) is a term used to describe one of several diseases in which individuals who have not recently been hospitalized develop an infection of the lungs (pneumonia). CAP is a common illness and can affect people of all ages. CAP often causes problems like difficulty in breathing, fever, chest pains, and a cough. CAP occurs because the areas of the lung which absorb oxygen (alveoli) from the atmosphere become filled with fluid and cannot work effectively.
CAP occurs throughout the world and is a leading cause of illness and death. Causes of CAP include bacteria, viruses, fungi, and parasites. CAP can be diagnosed by symptoms and physical examination alone, though x-rays, examination of the sputum, and other tests are often used. Individuals with CAP sometimes require treatment in a hospital. CAP is primarily treated with antibiotic medication. Some forms of CAP can be prevented by vaccination.[1]
Contents
Signs and symptoms
Symptoms of CAP commonly include:
- dyspnea
- coughing that produces greenish or yellow sputum
- a high fever that may be accompanied with sweating, chills, and uncontrollable shaking
- sharp or stabbing chest pain
- rapid, shallow breathing that is often painful
Less common symptoms include:
- the coughing up of blood (hemoptysis)
- headaches (including migraine headaches)
- loss of appetite
- excessive fatigue
- blueness of the skin (cyanosis)
- nausea
- vomiting
- diarrhea
- joint pain (arthralgia)
- muscle aches (myalgia)
The manifestations of pneumonia, like those for many conditions, might not be typical in older people. They might instead experience:
- new or worsening confusion
- hypothermia
- falls*
Additional symptoms for infants could include:
Cause
There are over a hundred microorganisms which can cause CAP. The most common types of microorganisms are different among different groups of people. Newborn infants, children, and adults are at risk for different spectrums of disease causing microorganisms. In addition, adults with chronic illnesses, who live in certain parts of the world, who reside in nursing homes, who have recently been treated with antibiotics, or who are alcoholics are at risk for unique infections. Even when aggressive measures are taken, a definite cause for pneumonia is only identified in half the cases.
Infants
Newborn infants can acquire lung infections prior to being born either by breathing infected amniotic fluid or by blood-borne infection across the placenta. Infants can also inhale (aspirate) fluid from the birth canal as they are being born. The most important infection in newborns is caused by Streptococcus agalactiae, also known as Group B Streptococcus or GBS. GBS causes at least 50% of cases of CAP in the first week of life.[3] Other bacterial causes in the newborn period include Listeria monocytogenes and tuberculosis. Viruses can also be transferred from mother to child; herpes simplex virus is the most common and life-threatening, but adenovirus, mumps, and enterovirus can also cause disease.
CAP in older infants reflects increased exposure to microorganisms. Common bacterial causes include Streptococcus pneumoniae, Escherichia coli, Klebsiella pneumoniae, Moraxella catarrhalis, and Staphylococcus aureus. A unique cause of CAP in this group is Chlamydia trachomatis, which is acquired during birth but which does not cause pneumonia until 2–4 weeks later. Maternally-derived syphilis can be a cause of CAP in this age group. Common viruses include respiratory syncytial virus (RSV), metapneumovirus, adenovirus, parainfluenza, influenza, and rhinovirus. RSV in particular is a common source of illness and hospitalization.[4] Fungi and parasites are not typically encountered in otherwise healthy infants.
Children
For the most part, children older than one month of life are at risk for the same microorganisms as adults. However, children less than five years are much less likely to have pneumonia caused by Mycoplasma pneumoniae, Chlamydophil pneumoniae, or Legionella pneumophila. In contrast, older children and teenagers are more likely to acquire Mycoplasma pneumoniae and Chlamydophila pneumoniae than adults.[5]
Adults
The full spectrum of microorganisms is responsible for CAP in adults. Several important groups of organisms are more common among people with certain risk factors. Identifying people at risk for these organisms is important for appropriate treatment.
- Viruses
- Viruses cause 20% of CAP cases. The most common viruses are influenza, parainfluenza, respiratory syncytial virus, metapneumovirus, and adenovirus. Less common viruses causing significant illness include chicken pox, SARS, avian flu, and hantavirus.[6]
- Atypical organisms
- The most common bacterial causes of pneumonia are the so-called atypical bacteria Mycoplasma pneumoniae and Chlamydophila pneumoniae. Legionella pneumophila is considered atypical but is less common. Atypical organisms are more difficult to grow, respond to different antibiotics, and were discovered more recently than the typical bacteria discovered in the early twentieth century.
- Streptococcus pneumoniae
- Streptococcus pneumoniae is a common bacterial cause of CAP (most common cause in UK). Prior to the development of antibiotics and vaccination, it was a leading cause of death. Traditionally highly sensitive to penicillin, during the 1970s resistance to multiple antibiotics began to develop. Current strains of "drug resistant Streptococcus pneumoniae" or DRSP are common, accounting for twenty percent of all Streptococcus pneumoniae infections. Adults with risk factors for DRSP including being older than 65, having exposure to children in day care, having alcoholism or other severe underlying disease, or recent treatment with antibiotics should initially be treated with antibiotics effective against DRSP.[7]
- Hemophilus influenzae
- Hemophilus influenzae is another common bacterial cause of CAP. First discovered in 1892, it was initially believed to be the cause of influenza because it commonly causes CAP in people who have suffered recent lung damage from viral pneumonia.
- Enteric Gram negative bacteria
- The enteric Gram negative bacteria such as Escherichia coli and Klebsiella pneumoniae are a group of bacteria that typically live in the human intestines. Adults with risk factors for infection including residence in a nursing home, serious heart and lung disease, and recent antibiotic use should initially be treated with antibiotics effective against Enteric Gram negative bacteria.
- Pseudomonas aeruginosa
- Pseudomonas aeruginosa is an uncommon cause of CAP but is a particularly difficult bacteria to treat. Individuals who are malnourished, have a lung disease called bronchiectasis, are on corticosteroids, or have recently had strong antibiotics for a week or more should initially be treated with antibiotics effective against Pseudomonas aeruginosa.[8]
Many less common organisms cause CAP. They are typically identified because an individual has special risk factors or after treatment for the common causes has failed. These rarer causes are covered in more detail in their specific pages: bacterial pneumonia, viral pneumonia, fungal pneumonia, and parasitic pneumonia.
Risk factors
Some people have an underlying problem which increases their risk of getting an infection. Some important situations are covered below:
- Obstruction
When part of the airway (bronchi) leading to the alveoli is obstructed, the lung is not able to clear fluid when it accumulates. This can lead to infection of the fluid resulting in CAP. One cause of obstruction, especially in young children, is inhalation of a foreign object such as a marble or toy. The object is lodged in the small airways and pneumonia can form in the trapped areas of lung. Another cause of obstruction is lung cancer, which can grow into the airways block the flow of air.
- Lung disease
People with underlying lung disease are more likely to develop CAP. Diseases such as emphysema or habits such as smoking result in more frequent and more severe bouts of CAP. In children, recurrent episodes of CAP may be the first clue to diseases such as cystic fibrosis or pulmonary sequestration.
- Immune problems
People who have immune system problems are more likely to get CAP. People who have AIDS are much more likely to develop CAP. Other immune problems range from severe immune deficiencies of childhood such as Wiskott-Aldrich syndrome to less severe deficiencies such as common variable immunodeficiency.[9]
Pathophysiology
The symptoms of CAP are the result of both the invasion of the lungs by microorganisms and the immune system's response to the infection. The mechanisms of infection are quite different for viruses and the other microorganisms.
- Viruses
- Viruses must invade cells in order to reproduce. Typically, a virus will reach the lungs by traveling in droplets through the mouth and nose with inhalation. There, the virus invades the cells lining the airways and the alveoli. This invasion often leads to cell death either through direct killing by the virus or by self-destruction through apoptosis. Further damage to the lungs occurs when the immune system responds to the infection. White blood cells, in particular lymphocytes, are responsible for activating a variety of chemicals (cytokines) which cause leaking of fluid into the alveoli. The combination of cellular destruction and fluid-filled alveoli interrupts the transportation of oxygen into the bloodstream. In addition to the effects on the lungs, many viruses affect other organs and can lead to illness affecting many different bodily functions. Viruses also make the body more susceptible to bacterial infection; for this reason, bacterial pneumonia often complicates viral CAP.
- Bacteria and fungi
- Bacteria and fungi also typically enter the lung with inhalation, though they can reach the lung through the bloodstream if other parts of the body are infected. Often, bacteria live in parts of the upper respiratory tract and are constantly being inhaled into the alveoli. Once inside the alveoli, bacteria and fungi travel into the spaces between the cells and also between adjacent alveoli through connecting pores. This invasion triggers the immune system to respond by sending white blood cells responsible for attacking microorganisms (neutrophils) to the lungs. The neutrophils engulf and kill the offending organisms but also release cytokines which result in a general activation of the immune system. This results in the fever, chills, and fatigue common in CAP. The neutrophils, bacteria, and fluid leaked from surrounding blood vessels fill the alveoli and result in impaired oxygen transportation. Bacteria often travel from the lung into the blood stream and can result in serious illness such as septic shock, in which there is low blood pressure leading to damage in multiple parts of the body including the brain, kidney, and heart.
- Parasites
- There are a variety of parasites which can affect the lungs. In general, these parasites enter the body through the skin or by being swallowed. Once inside the body, these parasites travel to the lungs, most often through the blood. There, a similar combination of cellular destruction and immune response causes disruption of oxygen transportation.
Diagnosis
Individuals with symptoms of CAP require further evaluation. Physical examination by a health provider may reveal fever, an increased respiratory rate (tachypnea), low blood pressure (hypotension), a fast heart rate (tachycardia), and/or changes in the amount of oxygen in the blood. Feeling the way the chest expands (palpation) and tapping the chest wall (percussion) to identify dull areas which do not resonate can identify areas of the lung which are stiff and full of fluid (consolidated). Examination of the lungs with the aid of a stethoscope can reveal several things. A lack of normal breath sounds or the presence of crackling sounds (rales) when the lungs are listened to (auscultated) can also indicate consolidation. Increased vibration of the chest when speaking (tactile fremitus) and increased volume of whispered speech during auscultation of the chest can also reveal consolidation.[10]
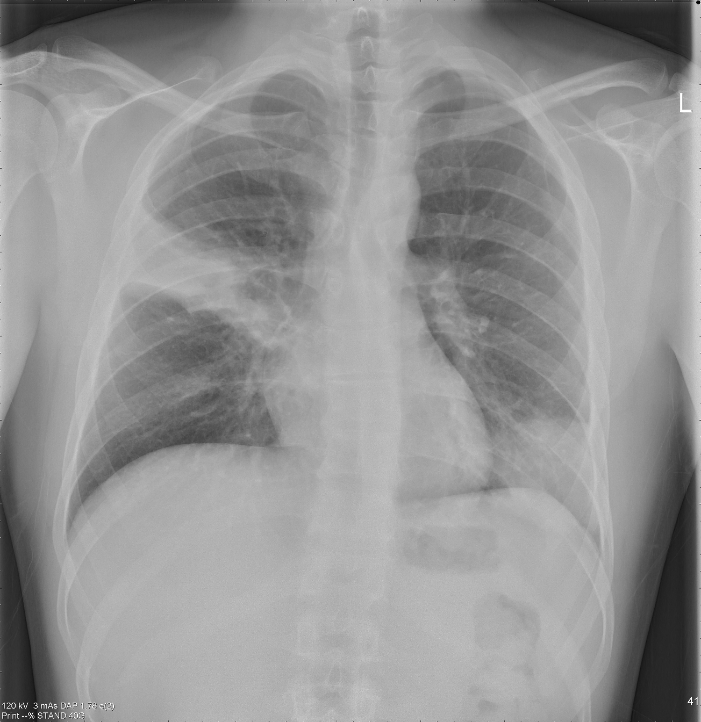
 Pneumonia. Chest x-ray showing increased shadowing in lungs
Pneumonia. Chest x-ray showing increased shadowing in lungs
 Pneumonia. Same lungs post treatment
Pneumonia. Same lungs post treatment
X-rays of the chest, examination of the blood and sputum for infectious microorganisms, and blood tests are commonly used to diagnose individuals with suspected CAP based upon symptoms and physical examination. The use of each test depends on the severity of illness, local practices, and the concern for any complications resulting from the infection. All patients with CAP should have the amount of oxygen in their blood monitored with a machine called a pulse oximeter. This helps determine how well the lungs are able to work despite infection. In some cases, analysis of arterial blood gas may be required to accurately determine the amount of oxygen in the blood. Complete blood count (CBC), a blood test, may reveal extra white blood cells, indicating an infection. Chest x-rays and chest computed tomography (CT) can reveal areas of opacity (seen as white) which represent consolidation. A normal chest x-ray makes CAP less likely; however, CAP is sometimes not seen on x-rays because the disease is either in its initial stages or involves a part of the lung not easily seen by x-ray. In some cases, chest CT can reveal a CAP which is not present on chest x-ray. X-rays can often be misleading, as many other diseases can mimic CAP such as heart problems or other types of lung damage.[11]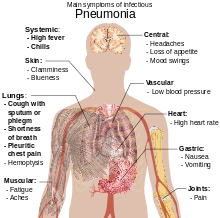 Main symptoms of infectious pneumonia
Main symptoms of infectious pneumoniaSeveral tests can be performed to identify the cause of an individual's CAP. Blood cultures can be drawn to isolate any bacteria or fungi in the blood stream. Sputum Gram's stain and culture can also reveal the causative microorganism. In more severe cases, a procedure wherein a flexible scope is passed through the mouth into the lungs (bronchoscopy) can be used to collect fluid for culture. Special tests can be performed if an uncommon microorganism is suspected (such as testing the urine for Legionella antigen when Legionnaires' disease is a concern).
Treatment
CAP is treated by administering an antibiotic which is effective in killing the offending microorganism as well as managing any complications of the infection. If the causative microorganism is unidentified, different antibiotics are tested in the laboratory in order to identify which medication will be most effective. Often, however, no microorganism is ever identified. Also, since laboratory testing can take several days, there is some delay until an organism is identified. In both cases, a person's risk factors for different organisms must be remembered when choosing the initial antibiotics (called empiric therapy). Additional consideration must be given to the setting in which the individual will be treated. Most people will be fully treated after taking oral pills while other people need to be hospitalized for intravenous antibiotics and, possibly, intensive care. In general, all therapies in older children and adults will include treatment for atypical bacteria. Typically this is a macrolide antibiotic such as azithromycin or clarithromycin although a fluoroquinolone such as levofloxacin can substitute. Doxycycline is now the antibiotic of choice in the UK for complete coverage of the atypical bacteria. This is due to increased levels of clostridium difficile seen in hospital patients being linked to the increased use of clarithromycin.
Newborns
Most newborn infants with CAP are hospitalized and given intravenous ampicillin and gentamicin for at least ten days. This treats the common bacteria Streptococcus agalactiae, Listeria monocytogenes, and Escherichia coli. If herpes simplex virus is the cause, intravenous acyclovir is administered for 21 days.
Children
Treatment of CAP in children depends on both the age of the child and the severity of his/her illness. Children less than five do not typically receive treatment to cover atypical bacteria. If a child does not need to be hospitalized, amoxicillin for seven days is a common treatment. However, with increasing prevalence of DRSP, other agents such as cefpodoxime will most likely become more popular in the future.[12] Hospitalized children should receive intravenous ampicillin, ceftriaxone, or cefotaxime. According to a recent meta-analysis a 3 days course of antibiotics seems to be sufficient for most cases of mild to moderate CAP in children.[1]
Adults
In 2001, the American Thoracic Society, drawing on work by the British and Canadian Thoracic Societies, established guidelines for the management of adults with CAP which divided individuals with CAP into four categories based upon common organisms encountered.[13]
- Healthy outpatients without risk factors
- This group, the largest, is composed of otherwise healthy patients without risk factors for DRSP, enteric Gram negative bacteria, Pseudomonas, or other less common causes of CAP. The primary microoganisms in this group are viruses, atypical bacteria, penicillin sensitive Streptococcus pneumoniae, and Hemophilus influenzae. Recommended management is with a macrolide antibiotic such as azithromycin or clarithromycin for seven[2] to ten days.
- Outpatients with underlying illness and/or risk factors
- This group does not require hospitalization; its members either have underlying health problems (such as emphysema or congestive heart failure) or is at risk for DRSP and/or enteric Gram negative bacteria. Treatment is with a fluoroquinolone active against Streptococcus pneumoniae such as levofloxacin or a beta-lactam antibiotic such as cefpodoxime, cefuroxime, amoxicillin, or amoxicillin/clavulanate plus a macrolide antibiotic such as azithromycin or clarithromycin for seven to ten days.[3]
- Hospitalized individuals not at risk for Pseudomonas
- This group requires hospitalization and administration of intravenous antibiotics. Treatment is with either an intravenous fluoroquinolone active against Streptococcus pneumoniae such as levofloxacin or beta-lactam antibiotic such as cefotaxime, ceftriaxone, ampicillin/sulbactam, or high-dose ampicillin plus an intravenous macrolide antibiotic such as azithromycin or clarithromycin for seven to ten days.
- Individuals requiring intensive care at risk for Pseudomonas
- Individuals being treated in an intensive care unit with risk factors for infection with Pseudomonas aeruginosa require specific antibiotics targeting this difficult to eradicate bacteria. One possible regimen is an intravenous antipseudomonal beta-lactam such as cefepime, imipenem, meropenem, or piperacillin/tazobactam plus an intravenous antipseudomonal fluoroquinolone such as levofloxacin. Another recommended regimen is an intravenous antipseudomonal beta-lactam such as cefepime, imipenem, meropenem, or piperacillin/ tazobactam plus an intravenous aminoglycoside such as gentamicin or tobramycin plus either an intravenous macrolide such azithromycin or an intravenous nonpseudomonal fluoroquinolone such as ciprofloxacin.
For mild to moderate community-acquired pneumonia shorter courses of antibiotics (3–7 days) seem to be sufficient according to a recent meta-analysis.[1]
Hospitalize
Some people with CAP require hospitalization and more intensive care than the majority. In general, a discussion between the individual and his or her health care provider determines the need for hospitalization. Clinical prediction rules, such as the pneumonia severity index and CURB-65 have been developed to help guide the decision.[14] Factors which increase the need for hospitalization include age greater than 65; underlying chronic illnesses; a respiratory rate greater than thirty breaths per minute; a systolic blood pressure less than 90 mmHg; a heart rate greater than 125 per minute; temperature less than 35 or greater than 40°C; confusion; and evidence of infection outside the lung. Laboratory results which increase the need for hospitalization include arterial oxygen tension less than 60 mm Hg, carbon dioxide of greater than 50 mmHg, or pH less than 7.35 while breathing room air; hematocrit less than 30%; creatinine greater than 1.2 mg/dl or blood urea nitrogen greater than 20 mg/ dl; white blood cell count less than 4 × 10^9/L or greater than 30 × 10^9/L; and absolute neutrophil count less than 1 x 10^9/L. X-ray findings which increase the need for hospitalization include involvement of more than one lobe of the lung, presence of a cavity, and the presence of a pleural effusion.
Prognosis
Individuals who are treated for CAP outside of the hospital have a mortality rate less than 1%. Fever typically responds in the first two days of therapy and other symptoms resolve in the first week. The x-ray, however, may remain abnormal for at least a month, even when CAP has been successfully treated. Among individuals who require hospitalization, the mortality rate averages 12% overall, but is as much as 40% in people who have bloodstream infections or require intensive care.[15] Factors which increase mortality are the same as those which increase the need for hospitalization and are listed above.
When CAP does not respond as expected, there are several possible causes. A complication of CAP may have occurred or a previously unknown health problem may be playing a role. Both situations are covered in more detail below. Additional causes include inappropriate antibiotics for the causative organism (i.e. DRSP), a previously unsuspected microorganism (such as tuberculosis), or a condition which mimics CAP (such as Wegener's granulomatosis). Additional testing may be performed and may include additional radiologic imaging (such as a computed tomography scan) or a procedure such as a bronchoscopy or lung biopsy.
Complications
Despite appropriate antibiotic therapy, severe complications can result from CAP, including:
Sepsis
Sepsis can occur when microorganisms enter the blood stream and the immune system responds. Sepsis most often occurs with bacterial pneumonia; Streptococcus pneumoniae is the most common cause. Individuals with sepsis require hospitalization in an intensive care unit. They often require medications and intravenous fluids to keep their blood pressure from going too low. Sepsis can cause liver, kidney, and heart damage among other things.
Respiratory failure
Because CAP affects the lungs, often individuals with CAP have difficulty breathing. If enough of the lung is involved, it may not be possible for a person to breathe enough to live without support. Non-invasive machines such as a bilevel positive airway pressure machine may be used. Otherwise, placement of a breathing tube into the mouth may be necessary and a ventilator may be used to help the person breathe.
Pleural effusion and empyema
Occasionally, microorganisms from the lung will cause fluid to form in the space surrounding the lung, called the pleural cavity. If the microorganisms themselves are present, the fluid collection is often called an empyema. If pleural fluid is present in a person with CAP, the fluid should be collected with a needle (thoracentesis) and examined. Depending on the result of the examination, complete drainage of the fluid may be necessary, often with a chest tube. If the fluid is not drained, bacteria can continue to cause illness because antibiotics do not penetrate well into the pleural cavity.
Abscess
Rarely, microorganisms in the lung will form a pocket of fluid and bacteria called an abscess. Abscesses can be seen on an x-ray as a cavity within the lung. Abscesses typically occur in aspiration pneumonia and most often contain a mixture of anaerobic bacteria. Usually antibiotics are able to fully treat abscesses, but sometimes they must be drained by a surgeon or radiologist.
Epidemiology
CAP is a common illness in all parts of the world. It is a major cause of death among all age groups. In children, the majority of deaths occur in the newborn period, with over two million worldwide deaths a year. In fact, the WHO estimates that one in three newborn infant deaths are due to pneumonia.[16] Mortality decreases with age until late adulthood; elderly individuals are particularly at risk for CAP and associated mortality.
More cases of CAP occur during winter months than during other times of the year. CAP occurs more commonly in males than females and in blacks than Caucasians. Individuals with underlying illnesses such as Alzheimer's disease, cystic fibrosis, emphysema, tobacco smoking, alcoholism, or immune system problems are at increased risk for pneumonia.[17]
Prevention
In addition to treating any underlying illness which can increase a person's risk for CAP, there are several additional ways to prevent CAP. Smoking cessation is important not only for treatment of any underlying lung disease, but also because cigarette smoke interferes with many of the body's natural defenses against CAP.
Vaccination is important in both children and adults. Vaccinations against Haemophilus influenzae and Streptococcus pneumoniae in the first year of life have greatly reduced their role in CAP in children. A vaccine against Streptococcus pneumoniae is also available for adults and is currently recommended for all healthy individuals older than 65 and any adults with emphysema, congestive heart failure, diabetes mellitus, cirrhosis of the liver, alcoholism, cerebrospinal fluid leaks, or who do not have a spleen. A repeat vaccination may also be required after five or ten years.[18]
Influenza vaccines should be given yearly to the same individuals as receive vaccination against Streptococcus pneumoniae. In addition, health care workers, nursing home residents, and pregnant women should receive the vaccine.[19] When an influenza outbreak is occurring, medications such as amantadine, rimantadine, zanamivir, and oseltamivir have been shown to prevent cases of influenza.[20]
References
- ^ a b Dimopoulos G, Matthaiou DK, Karageorgopoulos DE, Grammatikos AP, Athanassa Z, Falagas ME (2008). "Short- versus long-course antibacterial therapy for community-acquired pneumonia : a meta-analysis". Drugs 68 (13): 1841–54. doi:10.2165/00003495-200868130-00004. PMID 18729535.
- ^ Li JZ, Winston LG, Moore DH, Bent S (September 2007). "Efficacy of short-course antibiotic regimens for community-acquired pneumonia: a meta-analysis". The American Journal of Medicine 120 (9): 783–90. doi:10.1016/j.amjmed.2007.04.023. PMID 17765048.
- ^ Vardakas KZ, Siempos II, Grammatikos A, Athanassa Z, Korbila IP, Falagas ME (December 2008). "Respiratory fluoroquinolones for the treatment of community-acquired pneumonia: a meta-analysis of randomized controlled trials". CMAJ 179 (12): 1269–77. doi:10.1503/cmaj.080358. PMC 2585120. PMID 19047608. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2585120.
- ^ Emedicine review of bacterial pneumonia
- ^ Metlay JP, Schulz R, Li YH, et al. (July 1997). "Influence of age on symptoms at presentation in patients with community-acquired pneumonia". Archives of Internal Medicine 157 (13): 1453–9. doi:10.1001/archinte.157.13.1453. PMID 9224224.
- ^ Metlay JP, Kapoor WN, Fine MJ (November 1997). "Does this patient have community-acquired pneumonia? Diagnosing pneumonia by history and physical examination". JAMA 278 (17): 1440–5. doi:10.1001/jama.278.17.1440. PMID 9356004.
- ^ Syrjälä H, Broas M, Suramo I, Ojala A, Lähde S (August 1998). "High-resolution computed tomography for the diagnosis of community-acquired pneumonia". Clinical Infectious Diseases 27 (2): 358–63. doi:10.1086/514675. PMID 9709887.
- ^ Webber S, Wilkinson AR, Lindsell D, Hope PL, Dobson SR, Isaacs D (February 1990). "Neonatal pneumonia". Archives of Disease in Childhood 65 (2): 207–11. doi:10.1136/adc.65.2.207. PMC 1792235. PMID 2107797. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1792235.
- ^ Abzug MJ, Beam AC, Gyorkos EA, Levin MJ (December 1990). "Viral pneumonia in the first month of life". The Pediatric Infectious Disease Journal 9 (12): 881–5. doi:10.1097/00006454-199012000-00005. PMID 2177540.
- ^ Wubbel L, Muniz L, Ahmed A, et al. (February 1999). "Etiology and treatment of community-acquired pneumonia in ambulatory children". The Pediatric Infectious Disease Journal 18 (2): 98–104. doi:10.1097/00006454-199902000-00004. PMID 10048679.
- ^ de Roux A, Marcos MA, Garcia E, et al. (April 2004). "Viral community-acquired pneumonia in nonimmunocompromised adults". Chest 125 (4): 1343–51. doi:10.1378/chest.125.4.1343. PMID 15078744.
- ^ Ruhe JJ, Myers L, Mushatt D, Hasbun R (February 2004). "High-level penicillin-nonsusceptible Streptococcus pneumoniae bacteremia: identification of a low-risk subgroup". Clinical Infectious Diseases 38 (4): 508–14. doi:10.1086/381197. PMID 14765343.
- ^ Lieberman D, Schlaeffer F, Boldur I, et al. (February 1996). "Multiple pathogens in adult patients admitted with community-acquired pneumonia: a one year prospective study of 346 consecutive patients". Thorax 51 (2): 179–84. doi:10.1136/thx.51.2.179. PMC 473032. PMID 8711652. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=473032.
- ^ Bradley JS (June 2002). "Management of community-acquired pediatric pneumonia in an era of increasing antibiotic resistance and conjugate vaccines". The Pediatric Infectious Disease Journal 21 (6): 592–8; discussion 613–4. doi:10.1097/00006454-200206000-00035. PMID 12182396.
- ^ Niederman MS, Mandell LA, Anzueto A, et al. (June 2001). "Guidelines for the management of adults with community-acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention". American Journal of Respiratory and Critical Care Medicine 163 (7): 1730–54. PMID 11401897. http://ajrccm.atsjournals.org/cgi/pmidlookup?view=long&pmid=11401897.
- ^ Mundy LM, Auwaerter PG, Oldach D, et al. (October 1995). "Community-acquired pneumonia: impact of immune status". American Journal of Respiratory and Critical Care Medicine 152 (4 Pt 1): 1309–15. PMID 7551387.
- ^ Fine MJ, Auble TE, Yealy DM, et al. (January 1997). "A prediction rule to identify low-risk patients with community-acquired pneumonia". The New England Journal of Medicine 336 (4): 243–50. doi:10.1056/NEJM199701233360402. PMID 8995086.
- ^ Woodhead MA, Macfarlane JT, McCracken JS, Rose DH, Finch RG (March 1987). "Prospective study of the aetiology and outcome of pneumonia in the community". Lancet 1 (8534): 671–4. doi:10.1016/S0140-6736(87)90430-2. PMID 2882091.
- ^ Garenne M, Ronsmans C, Campbell H (1992). "The magnitude of mortality from acute respiratory infections in children under 5 years in developing countries". World Health Statistics Quarterly 45 (2-3): 180–91. PMID 1462653.
- ^ Almirall J, Bolíbar I, Balanzó X, González CA (February 1999). "Risk factors for community-acquired pneumonia in adults: a population-based case-control study". The European Respiratory Journal 13 (2): 349–55. doi:10.1183/09031936.99.13234999. PMID 10065680.
- ^ Butler JC, Breiman RF, Campbell JF, Lipman HB, Broome CV, Facklam RR (October 1993). "Pneumococcal polysaccharide vaccine efficacy. An evaluation of current recommendations". JAMA 270 (15): 1826–31. doi:10.1001/jama.270.15.1826. PMID 8411526.
- ^ Centers for Disease Control and Prevention. Prevention and control of influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 1999;48(RR-4):1-28.
- ^ Hayden FG, Atmar RL, Schilling M, et al. (October 1999). "Use of the selective oral neuraminidase inhibitor oseltamivir to prevent influenza". The New England Journal of Medicine 341 (18): 1336–43. doi:10.1056/NEJM199910283411802. PMID 10536125.
- Mandell LA, Wunderink RG, Anzueto A, et al. (March 2007). "Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults". Clinical Infectious Diseases 44 Suppl 2: S27–72. doi:10.1086/511159. PMID 17278083.
- kuya dennis po . :)) group 2.
Pneumonia Infectious pneumonias Bacterial pneumonia · Viral pneumonia · Fungal pneumonia · Parasitic pneumonia · Atypical pneumonia · Community-acquired pneumonia · Healthcare-associated pneumonia · Hospital-acquired pneumonia · Ventilator-associated pneumonia · Severe acute respiratory syndromePneumonias caused by
infectious or noninfectious agentsNoninfectious pneumonia Chemical pneumoniaCategories:- Pneumonia
- Infectious diseases


Wikimedia Foundation. 2010.