- Hypersensitivity pneumonitis
-
Hypersensitivity pneumonitis Classification and external resources 
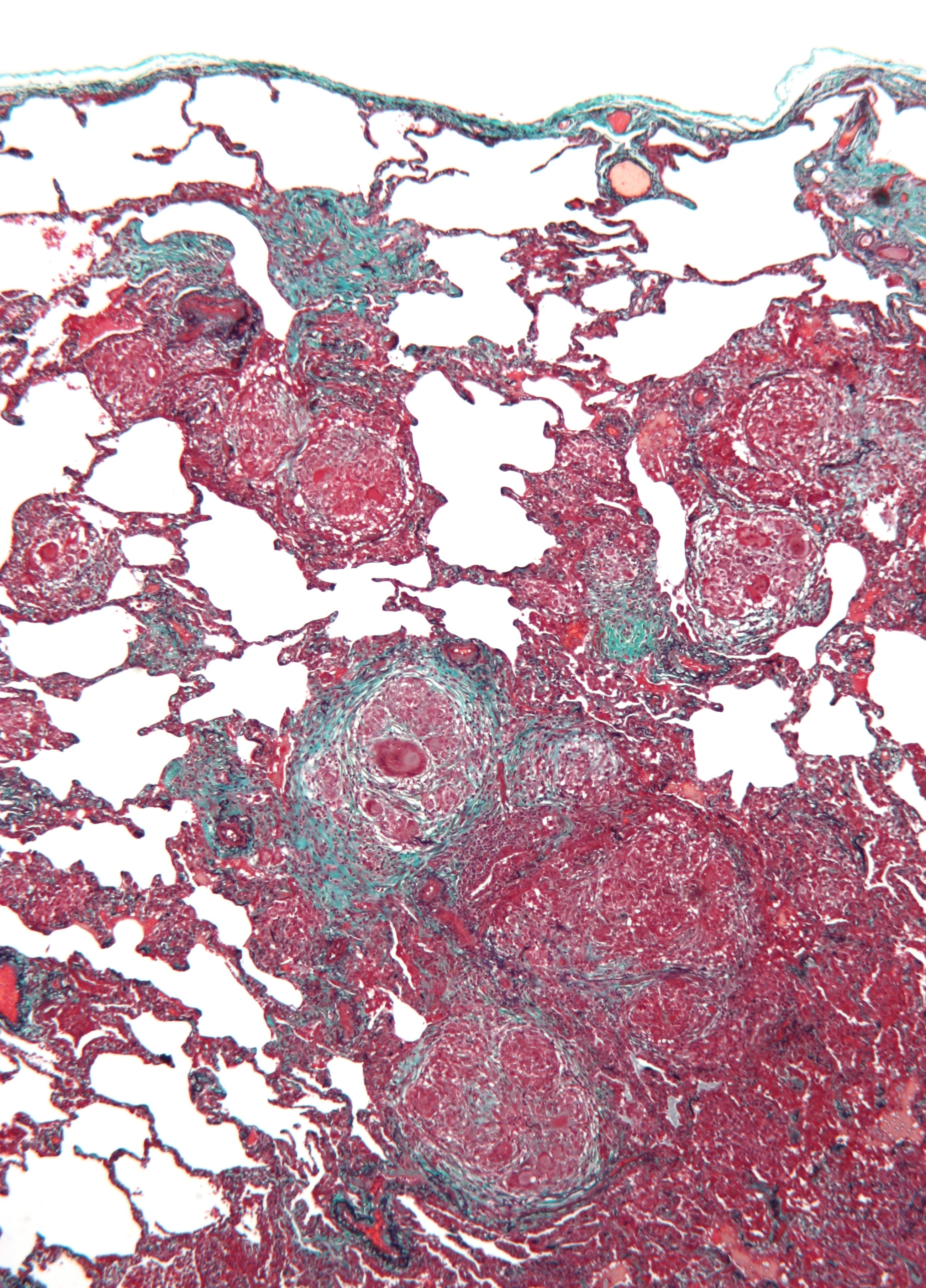
Micrograph of hypersensitivity pneumonitis. Lung biopsy. Trichrome stain.ICD-10 J67 ICD-9 495 DiseasesDB 4630 eMedicine med/1103 ped/2577 MeSH D000542 Hypersensitivity pneumonitis (also called extrinsic allergic alveolitis, EAA) is an inflammation of the alveoli within the lung caused by hypersensitivity to inhaled organic dusts. Sufferers are commonly exposed to the dust by their occupation or hobbies.
Contents
Pathophysiology
Hypersensitivity pneumonitis involves inhalation of an antigen. This leads to an exaggerated immune response (hypersensitivity). Type III hypersensitivity and type IV hypersensitivity occur in hypersensitivity pneumonitis.[1]
Symptoms
Hypersensitivity pneumonitis (HP) is categorized as acute, subacute, and chronic based on the duration of the illness. To learn more, please visit UCSF's signs and symptoms page.
Acute
In the acute form of HP, symptoms may develop 4–6 hours following heavy exposure to the provoking antigen. Symptoms include fever, chills, malaise, cough, chest tightness, dyspnea, and headache. Symptoms resolve within 12 hours to several days upon cessation of exposure.[2]
Acute HP is characterized by poorly formed noncaseating interstitial granulomas and mononuclear cell infiltration in a peribronchial distribution with prominent giant cells.[2]
On chest radiographs, a diffuse micronodular interstitial pattern (at times with ground-glass density in the lower and middle lung zones) may be observed. Findings are normal in approximately 10% of patients." In high-resolution CT scans, ground-glass opacities or diffusely increased radiodensities are present. Pulmonary function tests show reduced diffusion capacity of lungs for carbon monoxide (DLCO). Many patients have hypoxemia at rest, and all patients desaturate with exercise.[2]
Subacute
Patients with subacute HP gradually develop a productive cough, dyspnea, fatigue, anorexia, weight loss, and pleurisy. Symptoms are similar to the acute form of the disease, but are less severe and last longer. On chest radiographs, micronodular or reticular opacities are most prominent in mid-to-lower lung zones.[2] Findings may be present in patients who have experienced repeated acute attacks.
The subacute, or intermittent, form produces more well-formed noncaseating granulomas, bronchiolitis with or without organizing pneumonia, and interstitial fibrosis.[2]
Chronic
In chronic HP, patients often lack a history of acute episodes. They have an insidious onset of cough, progressive dyspnea, fatigue, and weight loss. This is associated with partial to complete but gradual reversibility. Avoiding any further exposure is recommended. Clubbing is observed in 50% of patients. Tachypnea, respiratory distress, and inspiratory crackles over lower lung fields often are present.[2]
On chest radiographs, progressive fibrotic changes with loss of lung volume particularly affect the upper lobes. Nodular or ground-glass opacities are not present. Features of emphysema are found on significant chest films and CT scans.[2]
Chronic forms reveal additional findings of chronic interstitial inflammation and alveolar destruction (honeycombing) associated with dense fibrosis. Cholesterol clefts or asteroid bodies are present within or outside granulomas.[2]
In addition, many patients have hypoxemia at rest, and all patients desaturate with exercise.
Diagnosis
The diagnosis is based upon a history of symptoms after exposure to the allergen and clinical tests. A physician may take blood tests, seeking signs of inflammation, a chest X-ray and lung function tests. The sufferer shows a restrictive loss of lung function.
Although overlapping in many cases, hypersensitivity pneumonitis may be distinguished from occupational asthma in that it isn't restricted to only occupational exposure, and that asthma generally is classified as a type I hypersensitivity.[3][4] Unlike asthma, hypersensitivity pneumonitis targets lung alveoli rather than bronchi.[5]
Lung biopsy
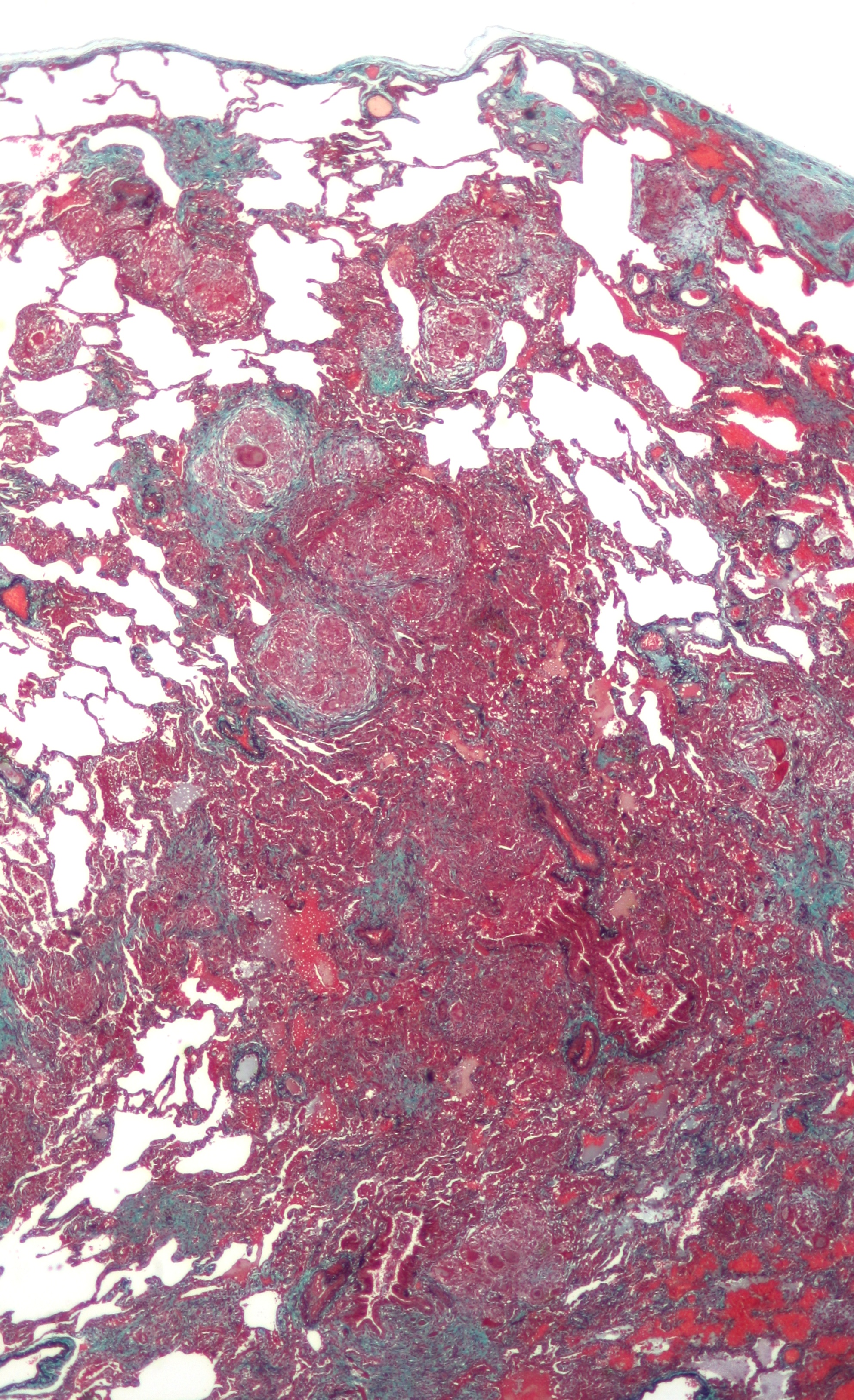
 Low magnification micrograph of hypersensitivity pneumonitis showing multinucleated giant cells and a centrilobular fibrosis. Trichrome stain.
Low magnification micrograph of hypersensitivity pneumonitis showing multinucleated giant cells and a centrilobular fibrosis. Trichrome stain.
Lung biopsies are rarely diagnostic, but may help intensify the search for an allergen, as certain characteristics may suggest the diagnosis.
The differential diagnosis of hypersensitivity pneumonitis is, primarily, a group of diseases known as idiopathic interstitial pneumonias.[6] This group of diseases includes idiopathic pulmonary fibrosis (IPF) (which manifests histologically as usual interstitial pneumonia (UIP)), idiopathic non-specific interstitial pneumonia (NSIP) and cryptogenic organizing pneumonia, among others.
Hypersensitivity pneumonitis may manifest, histologically, as usual interstitial pneumonia, i.e. it looks like idiopathic pulmonary fibrosis under the microscope; however, certain features may suggest it is a hypersensitivity pneumonitis. UIP does not typically have multinucleated giant cells, nor does it typically have a centrilobular distribution;[6] the presence of these features suggest the diagnosis of hypersensitivity pneumonitis.
The prognosis of some idiopathic interstitial pneumonias, e.g. idiopathic usual interstitial pneumonia (i.e. idiopathic pulmonary fibrosis), are very poor and the treatments of little help. This contrasts the prognosis (and treatment) for hypersensitivity pneumonitis, which is generally fairly good if the allergen is identified and exposures to it significantly reduced or eliminated. Thus, a lung biopsy, in some cases, may make a decisive difference.
Types
Hypersensitivity Pneumonitis (HP) may also be called many different names, based on the provoking antigen. These include:
Type[7] Specific antigen Exposure Bird fancier's lung
Also called bird breeder's lung,
pigeon breeder's lung, and poultry worker's Lung.Avian proteins Feathers and bird droppings [8] Farmer's lung The molds - Thermophilic actinomycetes[8]
- Aspergillus species
- Saccharopolyspora rectivirgula, and
- Micropolyspora faeni
Moldy hay Crack lung Crack cocaine Heavy crack smoking Bagassosis Thermophilic actinomycetes[8] Moldy bagasse (pressed sugarcane) Lycoperdonosis Puffball spores Spore dust from mature puffballs[9] Malt worker's lung Aspergillus clavatus[8] Moldy barley Maple bark disease Cryptostroma corticale[8] Moldy maple bark Miller's lung Sitophilus granarius (wheat weevil)[8] Dust-contaminated grain[8] Penguin Humidifier lung The bacteria - T. candidus
- Bacillus subtilis
- B. cereus, and Klebsiella oxytoca;
- Thermophilic actinomycetes[8]
the fungi
and the amoebae
- Naegleria gruberi,
- Acanthamoeba polyhaga, and
- Acanthamoeba castellani.
Mist generated by a machine from standing water Mushroom worker's lung Thermophilic actinomycetes Mushroom compost Compost lung Aspergillus Compost Peat moss worker's lung Caused by Monocillium sp. and Penicillium citreonigrum Peat moss Suberosis Penicillum frequentans Moldy cork dust Japanese summer house HP Trichosporon cutaneum Damp wood and mats Cheese-washer's lung Penicillum casei[8] or P.roqueforti Cheese casings Metalworking fluids HP Nontuberculous Mycobacteria. Mist from metalworking fluids. Hot tub lung Mycobacterium avium complex Mist from hot tubs. Mollusc shell HP Aquatic animal proteins Mollusc shell dust. Isocyanate HP TDI, HDI, and MDI Paints, resins, and polyurethane foams. TMA HP
chemical worker's lung[8]Trimellitic anhydride[8] Plastics, resins, and paints. Berylliosis Beryllium Electronics industry Wine-grower's lung Botrytis cinerea mold Moldy grapes Of these types, Farmer's Lung and Bird-Breeder's Lung are the most common. "Studies document 8-540 cases per 100,000 persons per year for farmers and 6000-21,000 cases per 100,000 persons per year for pigeon breeders. High attack rates are documented in sporadic outbreaks. Prevalence varies by region, climate, and farming practices. HP affects 0.4-7% of the farming population. Reported prevalence among bird fanciers is estimated to be 20-20,000 cases per 100,000 persons at risk." [2]
Treatment
The best treatment is to avoid the provoking allergen, as chronic exposure can cause permanent damage. Corticosteroids such as Prednisolone may help to control symptoms but may produce side-effects.
For more information on treatment, please visit UCSF's Hypersensitivity Pneumonitis Treatment page
Additional images
-

High magnification micrograph of hypersensitivity pneumonitis showing granulomatous inflammation. Trichrome stain.
References
- ^ Mohr LC (September 2004). "Hypersensitivity pneumonitis". Curr Opin Pulm Med 10 (5): 401–11. doi:10.1097/01.mcp.0000135675.95674.29. PMID 15316440. http://meta.wkhealth.com/pt/pt-core/template-journal/lwwgateway/media/landingpage.htm?issn=1070-5287&volume=10&issue=5&spage=401.
- ^ a b c d e f g h i Sharma, Sat. Hypersensitivity Pneumonitis. eMedicine, June 1, 2006.
- ^ "Lecture 14: Hypersensitivity". http://www-immuno.path.cam.ac.uk/~immuno/part1/lec13/lec13_97.html. Retrieved 2008-09-18.
- ^ "Allergy & Asthma Disease Management Center: Ask the Expert". http://www.aaaai.org/aadmc/ate/category.asp?cat=1008. Retrieved 2008-09-18.
- ^ Page 503 in: Mitchell, Richard Sheppard; Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson (2007). Robbins Basic Pathology. Philadelphia: Saunders. ISBN 1-4160-2973-7. 8th edition.
- ^ a b Ohtani Y, Saiki S, Kitaichi M, Usui Y, Inase N, Costabel U, Yoshizawa Y. Chronic bird fancier's lung: histopathological and clinical correlation. An application of the 2002 ATS/ERS consensus classification of the idiopathic interstitial pneumonias. Thorax. 2005 Aug;60(8):665-71. PMID 16061708.
- ^ Enelow, RI (2008). Fishman's Pulmonary Diseases and Disorders (4th ed.). McGraw-Hill. pp. 1161–1172. ISBN 0-07-145739-9.
- ^ a b c d e f g h i j k l Table 13-5 in: Mitchell, Richard Sheppard; Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson (2007). Robbins Basic Pathology. Philadelphia: Saunders. ISBN 1-4160-2973-7. 8th edition.
- ^ Munson EL, Panko DM, Fink JG. (1997). "Lycoperdonosis: Report of two cases and discussion of the disease". Clinical Microbiology Newsletter 19 (3): 17–24. doi:10.1016/S0196-4399(97)89413-5.
- Oxford Handbook of Clinical Medicine
Health science - Medicine - Allergic conditions Respiratory system Allergic rhinitis · Asthma · Hypersensitivity pneumonitis · Eosinophilic pneumonia · Churg-Strauss syndrome · Allergic bronchopulmonary aspergillosis · Farmer's lung · Laboratory animal allergySkin Blood and immune system Circulatory system Digestive system Nervous system Eosinophilic meningitisGenitourinary system Other conditions Immune disorders: hypersensitivity and autoimmune diseases (279.5–6) Type I/allergy/atopy
(IgE)ForeignAtopic dermatitis · Allergic urticaria · Hay fever · Allergic asthma · Anaphylaxis · Food allergy (Milk, Egg, Peanut, Tree nut, Seafood, Soy, Wheat), Penicillin allergyAutoimmunenoneType II/ADCC
(IgM, IgG)ForeignAutoimmuneAutoimmune hemolytic anemia · Idiopathic thrombocytopenic purpura · Bullous pemphigoid · Pemphigus vulgaris · Rheumatic fever · Goodpasture's syndromeType III
(Immune complex)ForeignHenoch–Schönlein purpura · Hypersensitivity vasculitis · Reactive arthritis · Rheumatoid arthritis · Farmer's lung · Post-streptococcal glomerulonephritis · Serum sickness · Arthus reactionAutoimmuneType IV/cell-mediated
(T-cells)ForeignAllergic contact dermatitis · Mantoux testAutoimmuneUnknown/
multipleForeignHypersensitivity pneumonitis (Allergic bronchopulmonary aspergillosis) · Transplant rejection · Latex allergy (I+IV)AutoimmuneSjögren's syndrome · Autoimmune hepatitis · Autoimmune polyendocrine syndrome (APS1, APS2) · Autoimmune adrenalitis · Systemic autoimmune diseaseCategories:- Lung diseases due to external agents

Wikimedia Foundation. 2010.