- Sjögren's syndrome
-
Sjögren's syndrome Classification and external resources 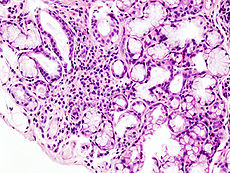
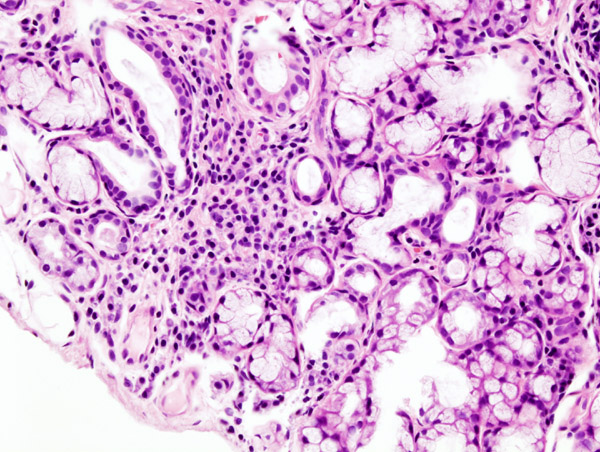
Histopathologic image of focal lymphoid infiltration in the minor salivary gland associated with Sjögren's syndrome. Lip biopsy. H & E stain.ICD-10 M35.0 ICD-9 710.2 OMIM 270150 DiseasesDB 12155 MedlinePlus 000456 eMedicine med/2136 emerg/537 derm/846 ped/2811 oph/477 oph/695 MeSH D012859 Not to be confused with Sjögren–Larsson syndrome.Sjögren's syndrome (pronounced
 /ˈʃoʊɡrɨnz/ shoh-grinz in English), also known as "Mikulicz disease" and "Sicca syndrome",[1] is a systemic autoimmune disease in which immune cells attack and destroy the exocrine glands[2] that produce tears and saliva.
/ˈʃoʊɡrɨnz/ shoh-grinz in English), also known as "Mikulicz disease" and "Sicca syndrome",[1] is a systemic autoimmune disease in which immune cells attack and destroy the exocrine glands[2] that produce tears and saliva.It is named after Swedish ophthalmologist Henrik Sjögren[3] (1899–1986), who first described it.
Nine out of ten Sjögren's patients are women[4][5] and the average age of onset is late 40s, although Sjögren's occurs in all age groups in both women and men.[citation needed] It is estimated to affect as many as 4 million people in the United States alone, making it the second most common autoimmune rheumatic disease.[4][5]
Sjögren's syndrome can exist as a disorder in its own right (primary Sjögren's syndrome) or may develop years after the onset of an associated rheumatic disorder, such as rheumatoid arthritis, systemic lupus erythematosus, scleroderma, primary biliary cirrhosis etc. (secondary Sjögren's syndrome).[citation needed]
The disorder should not be confused with the Sjögren–Larsson syndrome, which was also denoted T. Sjögren syndrome in early studies.
Contents
Signs and symptoms
The hallmark symptom of Sjögren's syndrome is a generalized dryness, typically including xerostomia (dry mouth) and xerophthalmia (dry eyes), part of what are known as sicca symptoms. In addition, Sjögren's syndrome may cause skin, nose, and vaginal dryness, and may affect other organs of the body, including the kidneys, blood vessels, lungs, liver, pancreas, peripheral nervous system (distal axonal sensorimotor neuropathy) and brain.
Sjögren's syndrome is associated with increased levels in Cerebrospinal fluid (CSF) of IL-1RA, an interleukin 1 antagonist. This suggests that the disease begins with increased activity in the interleukin 1 system, followed by an auto-regulatory up-regulation of IL-IRA to reduce the successful binding of interleukin 1 to its receptors. It is likely that interleukin 1 is the marker for fatigue, however, increased IL-1RA is observed in the CSF and is associated with increased fatigue through cytokine induced sickness behavior.[6] On the other hand, Sjögren's syndrome is characterized by decreased levels of IL-1ra in saliva, which could be responsible for mouth inflammation and dryness. [7] Patients with secondary Sjögren's syndrome also often exhibit signs and symptoms of their primary rheumatic disorders, such as SLE, Rheumatoid Arthritis or Systemic Sclerosis.
Diagnosis
Diagnosing Sjögren's syndrome is complicated by the range of symptoms a patient may manifest, and the similarity between symptoms of Sjögren's syndrome and those of other conditions. Nevertheless, the combination of several tests can lead to a diagnosis of Sjögren's syndrome.
Blood tests can be done to determine if a patient has high levels of antibodies that are indicative of the condition, such as anti-nuclear antibody (ANA) and rheumatoid factor (because SS frequently occurs secondary to rheumatoid arthritis), which are associated with autoimmune diseases. Typical Sjögren's syndrome ANA patterns are SSA/Ro and SSB/La, of which SSB/La is far more specific; SSA/Ro is associated with numerous other autoimmune conditions but are often present in Sjögren's.[8] [9]
Schirmer's test measures the production of tears: a strip of filter paper is held inside the lower eyelid for five minutes, and its wetness is then measured with a ruler. Producing less than five millimeters of liquid is usually indicative of Sjögren's syndrome. However, lacrimal function declines with age or may be impaired from other medical conditions. An alternative test is nonstimulated whole saliva flow collection, in which the patient spits into a test tube every minute for 15 minutes. A resultant collection of less than 1.5 mL is considered a positive result.[10] It takes longer to perform than Schirmer's test, but does not require special equipment.
A slit-lamp examination can reveal dryness on the surface of the eye. Salivary gland function can be tested by collecting saliva and determining the amount produced in a five minute period. A lip biopsy can reveal lymphocytes clustered around salivary glands, and damage to these glands due to inflammation.
Ultrasound examination of the salivary glands is the simplest confirmatory test and has the added advantage of being non-invasive with no complications. The parenchyma of the gland demonstrates multiple, small-2-6 mm hypoechoic lesions which are representations of the lymphocytic infiltrates. Often sialectasis with calculi are demonstrated if the disease is advanced. The sonographic findings have excellent symptom correlation. The other advantage of ultrasound is that complications of the disease such as extra-nodal lymphomas can often be detected as larger 1–4 cm hypoechoic intra-parenchymal masses.
There is also a radiological procedure which is a reliable and accurate test for Sjögren's syndrome. A contrast agent is injected into the parotid duct, which opens from the cheek into the vestibule of the mouth opposite the neck of the upper second molar tooth. Widespread puddling of the injected contrast scattered throughout the gland indicates Sjögren's syndrome.
The Revised Classification Criteria for Sjögren's Syndrome[11] requires the presence of signs, symptoms, and lab findings.
Patient-reported symptoms must include both ocular symptoms, such as daily, persistent, troublesome dry eyes for more than three months, and oral symptoms, such as needing to drink water to swallow food.
Objective evidence of eye involvement relies on Schirmer's test and the Rose bengal score (or similar). Histopathology studies should show focal lymphocytic sialadenitis. Objective evidence of salivary gland involvement is tested through ultrasound examinations, the level of unstimulated whole salivary flow, a parotid sialography, or salivary scintigraphy. Autoantibodies against Ro (SSA) and/or La (SSB) antigens are also expected.
SS can be excluded from people with past head and neck radiation therapy, hepatitis C infection, Acquired immunodeficiency syndrome (AIDS), pre-existing lymphoma, sarcoidosis, graft-versus-host disease, and use of anticholinergic drugs (since a time shorter than four times the life of the drug).
Pathogenesis
Cell mediated auto-immunity causes the apoptosis of the ductal and acinar epithelial cells which is responsible for the glandular tissue damage.[12]
Treatment
There is neither a known cure for Sjögren's syndrome nor a specific treatment to permanently restore gland secretion. Instead, treatment is generally symptomatic and supportive. Moisture replacement therapies such as artificial tears may ease the symptoms of dry eyes. Some patients with more severe problems use goggles to increase local humidity or have punctal plugs inserted to help retain tears on the ocular surface for a longer time. Additionally, cyclosporine (Restasis) is available by prescription to help treat chronic dry eye by suppressing the inflammation that disrupts tear secretion. Prescription drugs are also available that help to stimulate salivary flow, such as cevimeline (Evoxac) and pilocarpine. Nonsteroidal anti-inflammatory drugs may be used to treat musculoskeletal symptoms. For individuals with severe complications, corticosteroids or immunosuppressive drugs may be prescribed. Also, disease-modifying antirheumatic drugs (DMARDs) such as methotrexate may be helpful. Hydroxychloroquine (Plaquenil) is another option and is generally considered safer than methotrexate.[13] Salagen, a man-made form of pilocarpine, can be used to help produce tears as well as saliva in the mouth and intestines. It is derived from the Jaborandi plant.[14] [15] [16]
Dry eyes
Punctal plugs[17]
In the advanced stage, despite the use of tear replacement drops, the eyes always feel burning, scratchy, sore. The sufferer is always aware of some discomfort, the eyes feel worse in the morning and late evening. The use of tear replacement drops becomes tedious and ineffective. At this point it may be appropriate to consider punctal plugs.
Each eye has two sites at the inner corner of each eyelid where tears drain from the eye. The upper eyelid 'puncta' drains approximately 40% of the tears away and the lower puncta drains away the remaining 60% of the tears. If there is a problem with the quantity of tears, as there is in Sjögren's disease, plugging the lower puncta can result in the tears that the patient has remaining on the eye longer.
Punctal plugs can be inserted into the lower or upper tear drainage canals of the eyes. The procedure takes only a few minutes and is painless. It can be done in the optometrist or ophthalmologist's office. Generally, collagen plugs are inserted first. These plugs will dissolve within a few days, so it gives the patient a chance to see if there is any improvement in comfort. Generally, the improvement is immediate. The patient may proceed to use of permanent plugs, although these too can be removed if necessary.
Dental care
Preventive dental treatment is also necessary (and often overlooked by the patient), as the lack of saliva associated with xerostomia creates an ideal environment for the proliferation of bacteria that cause dental caries (cavities). Treatments include at-home topical fluoride application to strengthen tooth enamel and frequent teeth cleanings by a dental hygienist. Existing cavities must also be treated, as cavities that extend into the tooth can not be effectively treated through teeth cleaning alone, and are at a high risk of spreading into the pulp of the tooth, leading to the loss of vitality and need for extraction or root canal therapy. This treatment regimen is the same as that used for all xerostomia patients, such as those undergoing head and neck radiation therapy which often damages the salivary glands, as they are more susceptible to radiation than other body tissues.
Unfortunately, many patients, not realizing the need for dental treatment, do not see a dentist until most of their teeth are beyond the point of restoration. It is not uncommon for a dentist to see a xerostomia patient with severe, untreatable cavities in almost every tooth. In severe cases, the only viable treatment may be to extract all of the patient's teeth and treat with prosthetics such as dentures or implants.
Prognosis
Sjögren's can damage vital organs of the body with symptoms that may plateau or worsen, but the disease does not go into remission as with other autoimmune diseases. Some people may experience only the mild symptoms of dry eyes and mouth, while others have symptoms of severe disease. Many patients are able to treat problems symptomatically. Others are forced to cope with blurred vision, constant eye discomfort, recurrent mouth infections, swollen parotid glands, hoarseness, and difficulty in swallowing and eating. Debilitating fatigue and joint pain can seriously impair quality of life. Some patients can develop renal involvement (autoimmune tubulointerstitial nephritis) leading to proteinuria, urinary concentrating defect and distal renal tubular acidosis.
Patients with Sjögren's syndrome have a higher rate of non-Hodgkin lymphoma compared to both patients with other autoimmune diseases and healthy people.[18] About 5% of patients with Sjögren's syndrome will develop some form of lymphoid malignancy.[19] Patients with severe cases are much more likely to develop lymphomas than patients with mild or moderate cases.[20] The most common lymphomas are salivary extranodal marginal zone B cell lymphomas (MALT lymphomas in the salivary glands)[18] and diffuse large B-cell lymphoma.[20]
Complications
Among the complications discussed above, Sjögren's syndrome in women who become pregnant has been linked to increased incidence of neonatal lupus erythematosus with congenital heart block requiring a pacemaker.[21]
Epidemiology
Sjögren's syndrome affects 1 million–4 million people in the United States. Most people are more than 40 years old at the time of diagnosis. Women are nine times more likely than men to have Sjögren's syndrome.
On September 1, 2011, tennis player Venus Williams announced that she had been diagnosed with Sjögren's syndrome, and that because of the disease, she was withdrawing from the 2011 US Open.[22][23]
Research
Multiple monoclonal antibodies were under investigation in 2007.[24] The most promising seemed to be the anti-CD20 rituximab and the anti-CD22 epratuzumab; the anti-TNF-α and IFN-α drugs seemed less effective.
α-fodrin functions as an autoantigen in Sjögren's syndrome. Mucosal administration of α-fodrin has been shown to inhibit the progress of the disorder in mice.[25]
Research on diseases such as Sjögren's syndrome focuses on increasing knowledge and understanding of the disorder, improving diagnostic techniques, and finding ways to treat, prevent, and cure the disorder. The Primary Sjögren's Syndrome Registry in the UK is a tissue biobank of samples taken for research supported by the Medical Research Council. The Registry supports clinical trials and genetic studies of Sjögren's Syndrome[26] and is open to patients wishing to participate in research studies and researchers studying the disease.
An animal model of Sjögren's syndrome has been developed by immunizing mice with peptides from 60 kDa Ro-antigen. Days after immunization, salivary flow was decreased, and lymphocyte infiltrates as well as salivary dysfunction were observed which are highly reminiscent of human Sjögren's syndrome.[27][28]
See also
- Benign lymphoepithelial lesion
- Biotene — a product range that offers comfort and helps strengthen saliva’s natural defences.
- Keratoconjunctivitis sicca
- Parotitis
- Xerostomia
References
- Notes
- ^ Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. pp. 602–3. ISBN 1-4160-2999-0.
- ^ Delaleu N, Immervoll H, Cornelius J, Jonsson R (2008). "Biomarker profiles in serum and saliva of experimental Sjögren's syndrome: associations with specific autoimmune manifestations". Arthritis Res. Ther. 10 (1): R22. doi:10.1186/ar2375. PMC 2374466. PMID 18289371. http://arthritis-research.com/content/10/1/R22.
- ^ Sjögren H. Zur Kenntnis der keratoconjunctivitis sicca. Doctoral thesis, 1933.
- ^ a b "About Sjögren's Syndrome". Sjögren's Syndrome Foundation. http://www.sjogrens.org/home/about-sjogrens-syndrome.
- ^ a b Chris Chase (31 August 2011). "Venus Williams pulls out of U.S. Open due to autoimmune disease". Yahoo Sports. http://sports.yahoo.com/tennis/blog/busted_racquet/post/Venus-Williams-pulls-out-of-U-S-Open?urn=ten-wp2840.
- ^ Harboe E, Tjensvoll AB, Vefring HK, Gøransson LG, Kvaløy JT, Omdal R. (2009). Fatigue in primary Sjögren's syndrome—a link to sickness behaviour in animals? Brain Behav Immun.23(8):1104–8. doi:10.1016/j.bbi.2009.06.151 PMID 19560535
- ^ Perrier S, Coussedière C, Dubost JJ, Albuisson E, Sauvezie B. (1998) IL-1 receptor antagonist (IL-1RA) gene polymorphism in Sjögren's syndrome and rheumatoid arthritis. Clin Immunol Immunopathol. 87(3):309-13> http://www.ncbi.nlm.nih.gov/pubmed/9646842
- ^ Franceschini F, Cavazzana I (February 2005). "Anti-Ro/SSA and La/SSB antibodies". Autoimmunity 38 (1): 55–63. doi:10.1080/08916930400022954. PMID 15804706.
- ^ V Goëb et al. (2007). "Clinical significance of autoantibodies recognizing Sjögren's syndrome A (SSA), SSB, calpastatin and alpha-fodrin in primary Sjögren's syndrome". Clinical & Experimental Immunology 148 (2): 281–7. doi:10.1111/j.1365-2249.2007.03337.x. PMC 1868868. PMID 17286756. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1868868.
- ^ [1] Kruszka, P.; O'Brian, R. (2009). "Diagnosis and management of Sjögren syndrome". American family physician 79 (6): 465–470. PMID 19323359.
- ^ Vitali C, Bombardieri S, Jonsson R, et al. (June 2002). "Classification criteria for Sjögren's syndrome: a revised version of the European criteria proposed by the American-European Consensus Group". Ann. Rheum. Dis. 61 (6): 554–8. doi:10.1136/ard.61.6.554. PMC 1754137. PMID 12006334. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1754137.
- ^ "Sjogren’s syndrome: apoptosis by anti-SSA and anti-SSB antibodies". 2006. http://www.reumatismo.org/admin/filesArticoli/58-2-165.pdf.
- ^ "SJÖGREN’S SYNDROME: A GUIDE FOR THE PATIENT". http://dry.org/fox20020816/guide.htm. Retrieved 2010-04-27.
- ^ Ringold, S. (1875). "On Jaborandi". The Lancet 30 (1): 157–159.
- ^ Holmstedt, B., et al.; Wassén, S.Henry; Schultes, Richard Evans (1979). "Jaborandi: An Interdisciplinary Approach". J. Ethnopharmacology 1 (1): 3–21. doi:10.1016/0378-8741(79)90014-X.
- ^ Merck Index. An encyclopedia of chemicals, drugs, and biologicals. Rahway New Jersey: Merck &Co. 1986.
- ^ Dr. J. Parks, Ancaster ON Canada
- ^ a b Voulgarelis M, Skopouli FN (2007). "Clinical, immunologic, and molecular factors predicting lymphoma development in Sjogren's syndrome patients". Clin Rev Allergy Immunol 32 (3): 265–74. doi:10.1007/s12016-007-8001-x. PMID 17992593.
- ^ Tzioufas AG, Voulgarelis M (2007). "Update on Sjögren's syndrome autoimmune epithelitis: from classification to increased neoplasias". Best Pract Res Clin Rheumatol 21 (6): 989–1010. doi:10.1016/j.berh.2007.09.001. PMID 18068857.
- ^ a b Smedby KE, Baecklund E, Askling J (2006). "Malignant lymphomas in autoimmunity and inflammation: a review of risks, risk factors, and lymphoma characteristics". Cancer Epidemiol. Biomarkers Prev. 15 (11): 2069–77. doi:10.1158/1055-9965.EPI-06-0300. PMID 17119030.
- ^ Manthorpe R, Svensson A, Wirestrand LE (November 2004). "Late neonatal lupus erythematosus onset in a child born of a mother with primary Sjögren's syndrome". Ann. Rheum. Dis. 63 (11): 1496–7. doi:10.1136/ard.2003.014944. PMC 1754813. PMID 15479901. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1754813.
- ^ http://www.medpagetoday.com/Rheumatology/GeneralRheumatology/28325
- ^ "Venus Williams Pulls Out Of U.S. Open : NPR". npr.org. http://www.npr.org/2011/08/31/140098325/venus-williams-pulls-out-of-u-s-open?ft=1&f=1001. Retrieved September 1, 2011.
- ^ Meijer JM, Pijpe J, Bootsma H, Vissink A, Kallenberg CG (June 2007). "The Future of Biologic Agents in the Treatment of Sjögren's Syndrome". Clin Rev Allergy Immunol 32 (3): 292–297. doi:10.1007/s12016-007-8005-6. PMC 2071970. PMID 17992596. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2071970.
- ^ He J, Zhao J, Li Z (2008). "Mucosal administration of α-fodrin inhibits experimental Sjögren's syndrome autoimmunity". Arthritis Res. Ther. 10 (2): R44. doi:10.1186/ar2403. PMC 2453764. PMID 18419828. http://arthritis-research.com/content/10/2/R44.
- ^ http://rheumatology.oxfordjournals.org/content/early/2010/08/04/rheumatology.keq240.abstract
- ^ Scofield RH, Asfa S, Obeso D, Jonsson R, Kurien BT (2005). "Immunization with short peptides from the 60-kDa Ro antigen recapitulates the serological and pathological findings as well as the salivary gland dysfunction of Sjögren's syndrome". J Immunol 175 (12): 8409–14. PMID 16339583. http://www.jimmunol.org/content/175/12/8409.full.
- ^ Kurien BT, Asfa S, Li C, Dorri Y, Jonsson R, Scofield RH (2005). "Induction of oral tolerance in experimental Sjögren's syndrome autoimmunity". Scand J Immunol 61 (5): 418–25. doi:10.1111/j.1365-3083.2005.01593.x. PMID 15882433.
External links
- The original text from this article was obtained from a public domain resource at: www.ninds.nih.gov/health_and_medical/disorders/sjogrens_doc
- Sjögren's Syndrome Foundation
- For those interested in research into Sjögren's Syndrome: Sjogren's Registry
- The NHS Choices website holds useful information on Sjogren's Syndrome
Systemic CT disorders (M32–M36, 710) General Other hypersensitivity/autoimmune Sjögren's syndromeOther Immune disorders: hypersensitivity and autoimmune diseases (279.5–6) Type I/allergy/atopy
(IgE)ForeignAtopic dermatitis · Allergic urticaria · Hay fever · Allergic asthma · Anaphylaxis · Food allergy (Milk, Egg, Peanut, Tree nut, Seafood, Soy, Wheat), Penicillin allergyAutoimmunenoneType II/ADCC
(IgM, IgG)ForeignAutoimmuneAutoimmune hemolytic anemia · Idiopathic thrombocytopenic purpura · Bullous pemphigoid · Pemphigus vulgaris · Rheumatic fever · Goodpasture's syndromeType III
(Immune complex)ForeignHenoch–Schönlein purpura · Hypersensitivity vasculitis · Reactive arthritis · Rheumatoid arthritis · Farmer's lung · Post-streptococcal glomerulonephritis · Serum sickness · Arthus reactionAutoimmuneType IV/cell-mediated
(T-cells)ForeignAllergic contact dermatitis · Mantoux testAutoimmuneUnknown/
multipleForeignAutoimmuneSjögren's syndrome · Autoimmune hepatitis · Autoimmune polyendocrine syndrome (APS1, APS2) · Autoimmune adrenalitis · Systemic autoimmune diseaseCategories:- Autoimmune diseases
- Syndromes
- Connective tissue diseases
- Systemic connective tissue disorders
- Ailments of unknown etiology
Wikimedia Foundation. 2010.