- Diffuse large B-cell lymphoma
-
Diffuse large B cell lymphoma Classification and external resources 
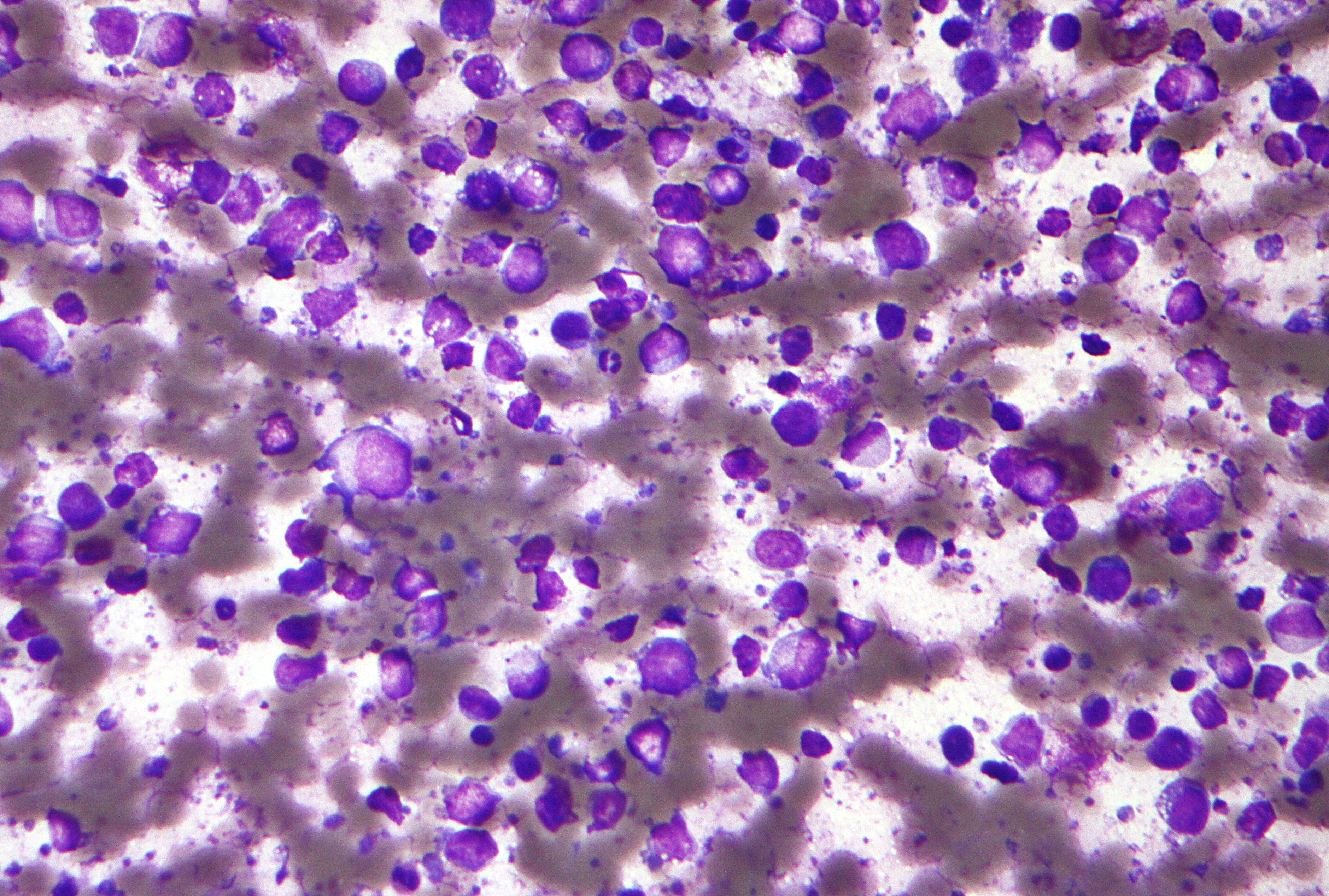
Micrograph of a diffuse large B cell lymphoma. Field stain.ICD-O: M9680/3 eMedicine article/202969 MeSH D016403 Diffuse large B-cell lymphoma (DLBL, DLBCL, or DLCL) is a type of aggressive non-Hodgkin lymphoma. It accounts for approximately 40% of lymphomas among adults.[1] The median age at diagnosis is 70 years, but it also occurs in children and young adults[2]. As with most non-Hodgkin lymphomas, there is a male predominance. Of all cancers involving the same class of blood cell, 31% of cases are DLBL.[3]
Contents
Classification
Two[4] or three[5] major subtypes of DLBL have been identified based on their genetic activity:
- activated (ABC-DLBCL), with a pattern of genetic expression that is similar to healthy, activated B cells, and
- germinal center (GCB DLBCL), with a pattern of genetic expression that is similar to germinal center B cells and a chromosomal translocation involving the gene bcl-2. This type has a relatively favorable prognosis.[6]
- primary mediastinal B-cell lymphoma (PMBL) Where the cancer is found in the thymus gland and lymph nodes behind the sternum (mediastinum), the area between the lungs, in the middle of the chest.
Chromosome anomalies are:[7]
- t(14;18)(q32;q21) with BCL2-rearrangement.
- t(3;Var)(q27;Var) with BCL6-rearrangement. These are common chromosomal translocations.[8]
- t(8;14)(q24;q32) with MYC rearrangements.
- A combination of MYC, BCL6 and/or BCL2 rearrangements, (in the so-called "double hit" or "triple hit" diffuse large B-cell lymphomas).
- Other less characteristic anomalies.
Histomorphology
DLBCLs consists of cells that are 4-5 times the diameter of a small lymphocytes and typically have marked cell-to-cell variation in size and shape. Their cytoplasm is typically basophilic and moderate in abundance. Nucleoli can be small but conspicuous to large and prominent and may be peripheral and/or central. Large bizarre cells can occasionally mimic Reed-Sternberg cells, seen in Hodgkin lymphoma.
Treatment
Standard treatment is CHOP. An expanded protocol, called CHOP-R, has improved survival[9] and rates of complete responses for DLBL patients, particularly elderly patients.[4] R-CHOP is a combination of one monoclonal antibody, 3 chemotherapy drugs, and one steroid: rituximab (Rituxan), cyclophosphamide (Cytoxan) doxorubicin (Hydroxydaunorubicin), vincristine (Oncovin), and prednisone.[10] Chemotherapy is most often administered intravenously and is most effective when it is administered multiple times over a period of months (e.g. every 3 weeks, over 8–10 months). For someone who will be receiving chemotherapy it is suggested they have a PICC (Peripherally inserted central catheter) in their arm near the elbow, and the catheter will extend through one of the large veins to within centimeters of the heart. Radiation is another common treatment and is most effective if done prior to the chemotherapy, or as the last treatment after chemotherapy has been completed.
Prognosis
The germinal-center subtype has the best prognosis, with 60% of treated patients surviving more than five years.[4]
See also
- Primary mediastinal B-cell lymphoma - a type of large B-cell lymphoma similar to DLBCL, that arises in the mediastinum of young adults.
References
- ^ [1] Pathobiology of the aggressive and highly aggressive non-Hodgkin's lymphomas
- ^ http://onlinelibrary.wiley.com/doi/10.1111/j.1365-2141.2009.08010.x/abstract;jsessionid=A7ABA22CE7B925EA0574722A0E9BDD78.d02t02 'The Haematological Malignancy Research Network (HMRN): a new information strategy for population based epidemiology and health service research.
- ^ Turgeon, Mary Louise (2005). Clinical hematology: theory and procedures. Hagerstown, MD: Lippincott Williams & Wilkins. p. 283. ISBN 0-7817-5007-5. "Frequency of lymphoid neoplasms. (Source: Modified from WHO Blue Book on Tumour of Hematopoietic and Lymphoid Tissues. 2001, p. 121.)"
- ^ a b c Turgeon, Mary Louise (2005). Clinical hematology: theory and procedures. Hagerstown, MD: Lippincott Williams & Wilkins. pp. 285–286. ISBN 0-7817-5007-5.
- ^ Lenz G, Wright GW, Emre NC, et al. (September 2008). "Molecular subtypes of diffuse large B-cell lymphoma arise by distinct genetic pathways". Proc. Natl. Acad. Sci. U.S.A. 105 (36): 13520–5. doi:10.1073/pnas.0804295105. PMC 2533222. PMID 18765795. http://www.pnas.org/cgi/pmidlookup?view=long&pmid=18765795.
- ^ Shiozawa E, Yamochi-Onizuka T, Takimoto M, Ota H (November 2007). "The GCB subtype of diffuse large B-cell lymphoma is less frequent in Asian countries". Leuk. Res. 31 (11): 1579–83. doi:10.1016/j.leukres.2007.03.017. PMID 17448534. http://linkinghub.elsevier.com/retrieve/pii/S0145-2126(07)00107-5.
- ^ "Diffuse large cell lymphoma" at Atlas of Genetics and Cytogenetics in Oncology and Haematology
- ^ Bosga-Bouwer AG, Haralambieva E, Booman M, et al. (November 2005). "BCL6 alternative translocation breakpoint cluster region associated with follicular lymphoma grade 3B". Genes Chromosomes Cancer 44 (3): 301–4. doi:10.1002/gcc.20246. PMID 16075463.
- ^ Sehn LH, Berry B, Chhanabhai M, et al. (March 2007). "The revised International Prognostic Index (R-IPI) is a better predictor of outcome than the standard IPI for patients with diffuse large B-cell lymphoma treated with R-CHOP". Blood 109 (5): 1857–61. doi:10.1182/blood-2006-08-038257. PMID 17105812. http://www.bloodjournal.org/cgi/pmidlookup?view=long&pmid=17105812.
- ^ Charles M. Farber, MD, PhD; and Randy C. Axelrod, MD (2011). "The Clinical and Economic Value of Rituximab for the Treatment of Hematologic Malignancies". Contemporary Oncology 3 (1). http://www.onclive.com/publications/contemporary-oncology/2011/spring-2011/the-clinical-and-economic-value-of-rituximab-for-the-treatment-of-hematologic-malignancies.
Hematological malignancy/leukemia histology (ICD-O 9590–9989, C81–C96, 200–208)
Lymphoid/Lymphoproliferative, Lymphomas/Lymphoid leukemias (9590–9739, 9800–9839)By development/
markerALL (Precursor B acute lymphoblastic leukemia/lymphoma)CD5+CD22+germinal center/follicular B cell (Follicular, Burkitt's, GCB DLBCL, Primary cutaneous follicular lymphoma)marginal zone/marginal-zone B cell (Splenic marginal zone, MALT, Nodal marginal zone, Primary cutaneous marginal zone lymphoma)see immunoproliferative immunoglobulin disordersBy infectionDiffuse large B-cell lymphoma · Intravascular large B-cell lymphoma · Primary cutaneous marginal zone lymphoma · Primary cutaneous immunocytoma · Plasmacytoma · Plasmacytosis · Primary cutaneous follicular lymphomaBy development/
markerTdT+: ALL (Precursor T acute lymphoblastic leukemia/lymphoma)
prolymphocyte (Prolymphocytic)
CD30+ (Anaplastic large-cell lymphoma, Lymphomatoid papulosis type A)indolent: Mycosis fungoides · Pagetoid reticulosis · Granulomatous slack skin
aggressive: Sézary's disease · Adult T-cell leukemia/lymphomaNon-MFCD30-: Non-mycosis fungoides CD30− cutaneous large T-cell lymphoma · Pleomorphic T-cell lymphoma · Lymphomatoid papulosis type B
CD30+: CD30+ cutaneous T-cell lymphoma · Secondary cutaneous CD30+ large cell lymphoma · Lymphomatoid papulosis type AOther peripheralHepatosplenic · Angioimmunoblastic · Enteropathy-associated T-cell lymphoma · Peripheral T-cell lymphoma-Not-Otherwise-Specified (Lennert lymphoma) · Subcutaneous T-cell lymphomaBy infectionHTLV-1 (Adult T-cell leukemia/lymphoma)NK cell/
(most CD56)Aggressive NK-cell leukemia · Blastic NK cell lymphomaT or NKLymphoid+myeloidCutaneous lymphoid hyperplasia Cutaneous lymphoid hyperplasia with bandlike and perivascular patterns · Cutaneous lymphoid hyperplasia with nodular pattern · Jessner lymphocytic infiltrate of the skinCategories:
Wikimedia Foundation. 2010.