- Philadelphia chromosome
Infobox_Disease
Name = Philadelphia chromosome
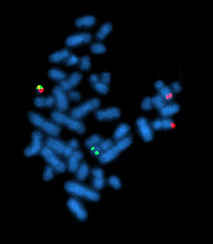
Caption = A metaphase cell positive for the bcr/abl rearrangement using FISH
DiseasesDB =
ICD10 = ICD10|C|92|1|c|81
ICD9 = ICD9|205.1
ICDO = 9875/3
OMIM =
MedlinePlus =
eMedicineSubj =
eMedicineTopic =
MeshID = D010677Philadelphia chromosome or Philadelphia translocation is a specific chromosomal abnormality that is associated with
chronic myelogenous leukemia (CML). It is the result of a reciprocal translocation between chromosome 9 and 22, and is specifically designated t(9;22)(q34;q11). The presence of this translocation is a highly sensitive test for CML, since 95% of people with CML have this abnormality (The remainder have either a cryptic translocation that is invisible on G-banded chromosome preparations, or a variant translocation involving another chromosome or chromosomes "as well as" the long arm of chromosomes 9 and 22). However, the presence of the Philadelphia (Ph) chromosome is not sufficiently specific to diagnose CML, since it is also found inacute lymphoblastic leukemia (ALL, 25–30% in adult and 2–10% in pediatric cases) and occasionally inacute myelogenous leukemia (AML).Molecular biology
The exact chromosomal defect in Philadelphia chromosome is translocation. Parts of two chromosomes, 9 and 22, swap places. The result is that part of the "BCR" ("breakpoint cluster region") gene from
chromosome 22 (region q11) is fused with part of the "ABL" gene on chromosome 9 (region q34). In agreement with theInternational System for Human Cytogenetic Nomenclature (ISCN), thischromosomal translocation is designated as t(9;22)(q34;q11). "Abl" stands for "Abelson", the name of a leukemia virus which carries a similar protein.The result of the translocation is a protein of p210 or sometimes p185("p" simply stands for "protein"; the numbers represent the apparent molecular weight of the mutant proteins in
kDa ). The fused "bcr-abl" gene is located on the resulting, shorter chromosome 22. Because "abl" carries a domain that can add phosphate groups totyrosine residues (tyrosine kinase ) the "bcr-abl" fusion gene is also a tyrosine kinase. (Although the "bcr" region is also a serine/threonine kinase, the tyrosine kinase function is very relevant for therapy, as will be shown.) P210 occurs primarily in CML, and sometimes in PH+ ALL, for which the P190 fusion protein is more common. For pediatric PH+ ALL, the impact of the type of fusion on prognosis after therapy is unknown, since PH+ ALL is rare and populating statistically relevant studies is difficult.The fused "bcr-abl" protein interacts with the
interleukin-3 receptor beta(c) subunit. The "bcr-abl" transcript is constitutively active, i.e. it does not require activation by other cellular messaging proteins. In turn, "bcr-abl" activates a number ofcell cycle -controllingprotein s andenzyme s, speeding up cell division. Moreover, it inhibitsDNA repair , causinggenomic instability and potentially causing the feared blast crisis in CML.Nomenclature
Philadelphia chromosome is designated Ph (or Ph') chromosome and the translocation is termed t(9;22)(q34.1;q11.2).
Therapy
In the late 1990s, STI-571 (
imatinib , Gleevec/Glivec) was identified byNovartis pharmaceuticals in high-throughput screens for tyrosine kinase inhibitors. Subsequent clinical trials led by Dr Brian J. Druker at Oregon Health & Science University in collaboration with Dr. Charles Sawyers and Dr. Moshe Talpaz demonstrated that STI-571 inhibits proliferation of BCR-ABL-expressing hematopoietic cells. Although it did not eradicate CML cells, it did greatly limit the growth of the tumor clone and decreased the risk of the feared "blast crisis ". In 2000John Kuriyan determined the mechanism by which STI-571 inhibits the Abl kinase domain. It was marketed in 2001 by thepharmaceutical company Novartis as imatinib mesylate (Gleevec in the US, Glivec in Europe). Other pharmacological inhibitors are being developed, which are more potent and/or are active against the emerging Gleevec/Glivec resistant BCR-abl clones in treated patients. The majority of these resistant clones are point-mutations in the kinase of BCR-abl. New inhibitors includedasatinib andnilotinib , which are significantly more potent than imatinib and may overcome resistance. Treatment of pediatric Ph+ ALL with a combination of standard chemotherapy and RTK inhibitors may result in remission, but the curative potential is unknown. COG study AALL 0031, which examines the use of Gleevec with standard chemotherapeutic regimens and bone marrow transplant from HLA-matched related donors for high risk ALL (including PH+ ALL), has concluded, and findings will be published in the near future. A potentially curative, but risky option for pediatric PH+ ALL or PH+ CML includes bone marrow transplant or cord blood transplant, but chemotherapy is favored by some for achieving first remission (CR1). For some, bone marrow transplant from a matched sibling donor or a matched, unrelated donor may be favored when remission is obtained. Cord blood transplant is favored by some when a 10/10 bone marrow match is not available, and cord blood transplant may have some advantages, including a reduced incidence of graft-vs-host disease (GVHD), which is a common and significant complication of transplant. However, transplant with cord blood sometimes requires longer periods of time for engraftment, which may increase the potential for complications due to infection. Regardless of the type of transplant, transplant-related mortality and relapse are possible, and the rates may change as treatment protocols improve. For second remission (CR2), if achieved, both chemotherapy and transplant options are possible, and many physicicans prefer tranpslant.History
The Philadelphia chromosome was first discovered and described in 1960 by Peter Nowell from
University of Pennsylvania School of Medicine and David Hungerford from theFox Chase Cancer Center 's Institute for Cancer Research and was therefore named after the city in which both facilities are located.In 1973, Janet D. Rowley at the
University of Chicago identified the mechanism by which the Philadelphia chromosome arises as a translocation.See also
*Refer to the article on
Chronic myelogenous leukemia for more details on diagnosis and treatment.
*Chromosomal translocation Sources
*
* Nowell P, Hungerford D. "A minute chromosome in chronic granulocytic leukemia." "Science" 1960;132:1497.
*
*
*
*
*
*External links
*
Wikimedia Foundation. 2010.