- Dermatomyositis
-
Dermatomyositis Classification and external resources 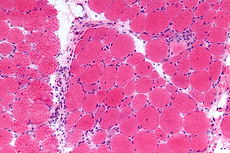
Micrograph of dermatomyositis. Muscle biopsy. H&E stain.ICD-10 M33.0-M33.1 (ILDS M33.910) ICD-9 710.3 DiseasesDB 10343 MedlinePlus 000839 eMedicine med/2608 derm/98 MeSH D003882 Dermatomyositis (DM) is a connective-tissue disease related to polymyositis (PM) and Bramaticosis that is characterized by inflammation of the muscles and the skin.
Contents
Causes
The cause is unknown, but it may result from either a viral infection or an autoimmune reaction. In the latter case it is a systemic autoimmune disease. Many people diagnosed with dermatomyositis were previously diagnosed with infectious mononucleosis and Epstein-Barr virus. Some cases of dermatomyositis actually "overlap" (are combined with) other autoimmune diseases such as: Sjögren's syndrome, lupus, scleroderma, or vasculitis. Because of the link between dermatomyositis and autoimmune disease, doctors and patients suspecting dermatomyositis may find it helpful to run an ANA - antinuclear antibody - test, which in cases of a lupus-like nature may be positive (usually from 1:160 to 1:640, with normal ranges at 1:40 and below).[citation needed]
Several cases of polymyositis and dermatomyositis were reported as being triggered by the use of various statin drugs used to control blood cholesterol. Muscle biopsies of these patients showed rhabdomyolysis, and degeneration and regeneration of muscle tissue.
High blood levels of creatine kinase (CPK) showed greater than 5 times the normal levels also supporting the rhabdomyolysis findings[clarification needed]. CPK is an enzyme found mainly in the heart, brain, and skeletal muscle that tends to rise when inflammation occurs during normal exercising. When these levels rise in excess of the normal level (less than 200), and become more than five times higher, severe cell damage to the muscles, brain, and heart ensue[clarification needed]. The higher the CPK, the greater the cellular damage done[clarification needed]. Extremely high levels of CPK cause rhabdomyolysis to these muscles and organs[clarification needed]. Without treatment, kidney damage occurs and death in the more severe cases. Confirmed polymyositis with the skin signs is known as dermatomyositis which amplifies the problem to various cancers[clarification needed].
Some cases of dermatomyositis are a paraneoplastic phenomenon, indicating the presence of cancer.[1] In cases involving cancer, the cancer is usually pre-existent, with removal of the cancer resulting in remission of the dermatomyositis. The onset of a rash in patients with pre-existing myositis requires investigation of the neoplastic possibility.
In his 1988 article, Clinical pathologic correlations of Lyme disease by stage, noted Lyme disease researcher Dr. Alan Steere observed, "[...] the perivascular lymphoid infiltrate in clinical myositis does not differ from that seen in polymyositis or dermatomyositis. All of these histologic derangements suggest immunologic damage in response to persistence of the spirochete, however few in number."
Prognosis
Before the advent of modern treatments such as prednisone, Intravenous immunoglobulin, plasmapheresis, chemotherapies, and other drugs, prognosis was poor.[2] Now there are numerous treatments and immune-modulating drugs. Fortunately, over 90% of patients today will do well for many years, with remission being a possibility. However, it is still important that treatment begin as soon as possible.
Presentation
 Gottron's papules. Discrete erythematous papules overlying the metacarpal and interphalangeal joints in a patient with juvenile dermatomyositis.
Gottron's papules. Discrete erythematous papules overlying the metacarpal and interphalangeal joints in a patient with juvenile dermatomyositis.
 X-Ray of the knee in a patient with dermatomyositis.
X-Ray of the knee in a patient with dermatomyositis.X-ray findings sometimes include dystrophic calcifications in the muscles, and patients may or may not notice small calcium deposits under the skin. Many do not have any calcium deposits of any kind. The rash also may come and go, and may not be dependent on the severity of the muscle involvement at the time. "Gottron's papules", pink patches on the knuckles and other extensor surfaces, and priapism, are associated with this disorder.
Another concern is interstitial lung disease.
Based on the conclusion of the paper "Interstitial lung disease (ILD) in polymyositis and dermatomyositis" by Maryann Fathi and Ingrid E Lundberg published 12/13/2005:
Investigations to detect interstitial lung disease should be performed during the initial evaluation as well as during follow-up of patients with myositis, because ILD is a frequent manifestation in patients with polymyositis or dermatomyositis and because ILD is associated with increased morbidity and mortality. This evaluation should include chest radiograph, HRCT of lungs, pulmonary function tests including diffusing capacity, and serum levels of anti-Jo1 antibodies. In the patients with ILD, clinical or subclinical, treatment with high doses of corticosteroids in combination with other immunosuppressive therapy should be initiated. Some histopathologic features including DAD, UIP, neutrophil alveolitis, digital infarcts showing microangiopathy in dermatomyositis, and amyopathic dermatomyositis have all been reported as risk factors for poor outcome. Presence of these factors suggests the use of aggressive immunosuppressive therapy (i.e. Methotrexate) and careful monitoring of lung function.
Classification
Dermatomyositis is a type of autoimmune connective tissue disease.[3] It is related to polymyositis and inclusion body myositis.
There is a form of this disorder that strikes children, known as juvenile dermatomyositis (JDM). For the most part Juvenile dermatomyositis is the same as the adult form, but the relationship with cancer is far lower, or non-existent.
Signs and symptoms
The main symptoms include skin rash and symmetric proximal muscle weakness which may be accompanied by pain. The pain may resemble the type experienced after strenuous exercise. Some dermatomyositis patients have little pain, while in others (esp. in JDM), the pain may be severe. It is important to remember that this condition varies from person to person in many ways. Also in many cases muscle may deteriorate and render the patient temporarily paralyzed unable to walk, run, get out of bed, or even swallow food and liquids.
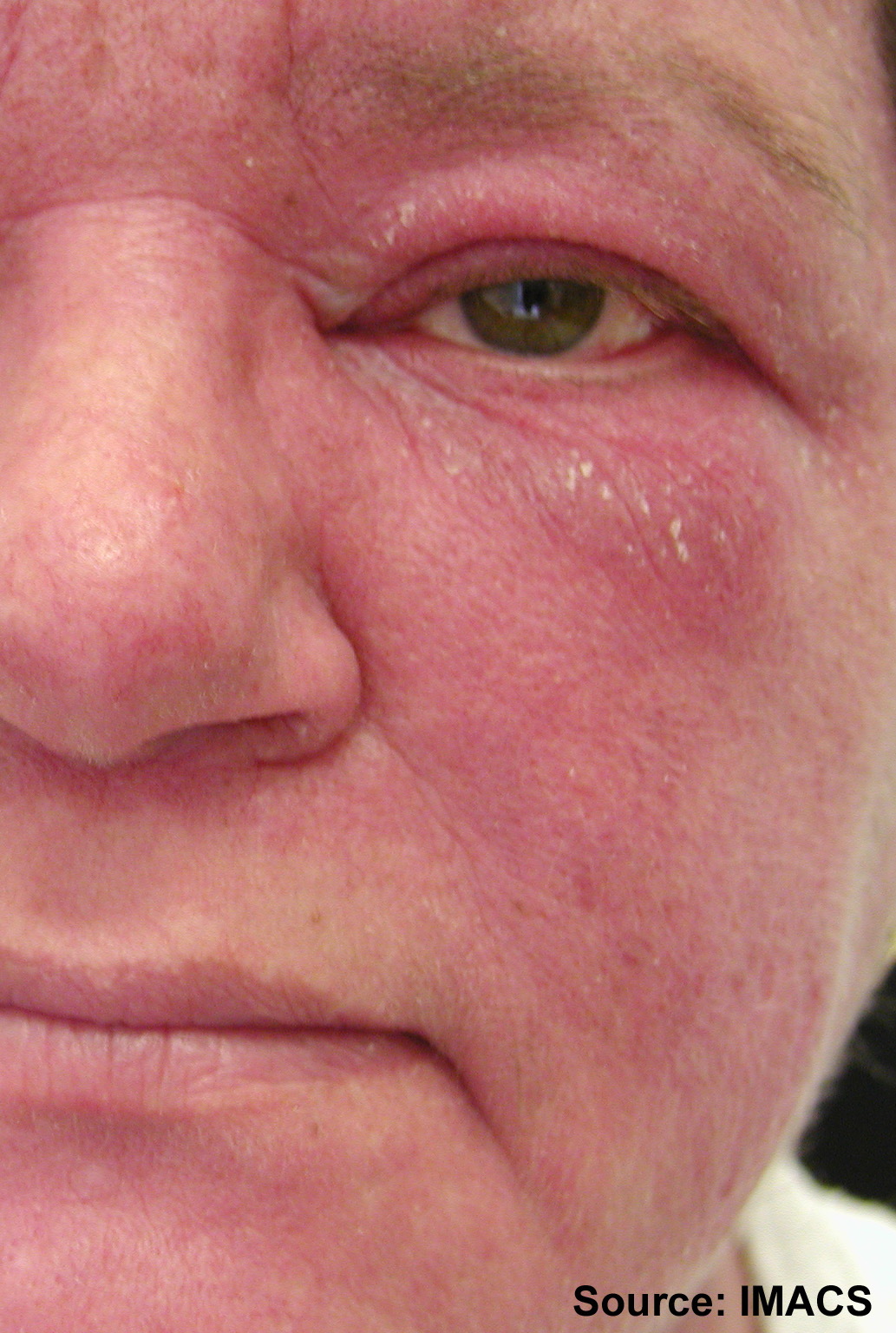
Skin findings occur in dermatomyositis but not PM and are generally present at diagnosis. Gottron's sign is an erythematous, scaly eruption occurring in symmetric fashion over the MCP and interphalangeal joints (can mimic psoriasis). The heliotrope or "lilac" rash [4] is a violaceous eruption on the upper eyelids and in rare cases on the lower eyelids as well, often with itching and swelling (most specific, though uncommon)[clarification needed]. Shawl (or V-) sign is a diffuse, flat, erythematous lesion over the back and shoulders or in a "V" over the posterior neck and back or neck and upper chest, which worsens with UV light. Erythroderma is not a flat, erythematous lesion similar to the shawl sign but located in other areas, such as the malar region and the forehead. Periungual telangiectasias and erythema occur.
Mechanic's hands (also in PM) refers to rough, cracked skin at the tips and lateral aspects of the fingers forming irregular dirty-appearing lines that resemble those seen in a laborer (this is also associated with the anti-synthetase syndrome). See: sclerodactyly. Psoriaform changes in the scalp can occur. Centripetal flagellate erythema comprises linear, violaceous streaks on the trunk (possibly caused by itching pruritic skin). Calcinosis cutis (deposition of calcium in the skin) is usually seen in juvenile dermatomyositis, not adult dermatomyositis. Dysphagia (difficulty swallowing) is another feature, occurring in as many as 33% of cases.
Pathology
The diagnosis of dermatomyositis can be confirmed by muscle biopsy, EMG,and blood tests. It should be noted, however, that only muscle biopsy is truly diagnostic (pathognomonic); liver enzymes and EMG are relatively non-specific. Liver enzymes, specifically creatine phosphokinase (CPK), are the major tool in assessing the progress of the disease and/or the efficacy of treatment. On the muscle biopsy, there are two classic microscopic findings of dermatomyositis. They are:
- A mixed B- and T-cell perivascular inflammatory infiltrate
- Perifascicular muscle fiber atrophy
Dermatomyositis is associated with autoantibodies, especially anti-Jo1 antibody.[5]
Microscopic findings
Cross sections of muscle reveal muscle fascicles with small, shrunken polygonal muscle fibers on the periphery of a fascicle surrounding central muscle fibers of normal, uniform size.
Aggregates of mature lymphocytes with small, dark nuclei and scant cytoplasm are seen surrounding vessels. Other inflammatory cells are distinctly uncommon. Immunohistochemistry can be used to demonstrate that both B- and T-cells are present in approximately equal numbers.
Mechanism
The mechanism is conjectured to be complement-mediated damage of microscopic vessels with muscle atrophy and lymphocytic inflammation secondary to tissue ischemia.[6]
Differential diagnosis
Dermatomyositis must be differentiated from other common, lymphocyte predominant inflammatory myopathies. If present, the characteristic perifascicular atrophy makes this distinction trivial.
There is some overlap in the microscopic appearances of different inflammatory myopathies, but some helpful differences are often present.[7] The rimmed vacuoles of inclusion body myositis (IBM) are absent in dermatomyositis. Polymyositis is characterised by diffuse or patchy inflammation of the muscle fascicles, a random pattern of muscle atrophy, and T-cell predominance with T-cells seen invading otherwise viable appearing muscle fibers.[1] Pubmed reports 15 articles where Dermatomyositis and Lyme Disease are associated.
Treatment
This disease has no known cure. Specialized exercise therapy may supplement treatment to enhance quality of life.
Medications to help relieve symptoms include:
- Prednisolone
- Methotrexate
- Mycophenolate (CellCept / Myfortic)
- Intravenous immunoglobulin
- Azathioprine
- Cyclophosphamide
- Rituximab[8]
Notable individuals with dermatomyositis
- Actor Laurence Olivier (1907–1989) suffered from dermatomyositis in 1974 aged 67, and nearly died from the disease.
- American football running back Ricky Bell, the 1976 Heisman Trophy runner up and #1 pick in the 1977 NFL draft, died at age 29 from the disease.[9]
- Rob Buckman doctor, comedian, author and president of the Humanist Association of Canada.
Gallery
-

Gottron's papules. Discrete erythematous papules overlying the metacarpal and interphalangeal joints in a patient with juvenile dermatomyositis.
-

Gottron's papules. Erythematous to violaceous raised papules overlying the metacarpal and interphalangeal joints in a patient with juvenile dermatomyositis.
-

Gottron's papules. Characteristic raised erythematous papule overlying the proximal interphalangeal joint in a patient with dermatomyositis.
-

Gottron's papules. Erythematous plaques overlying the elbows in two patients with juvenile dermatomyositis. In some patients, small erythematous plaques may overly the extensor aspects of larger joints, such as the elbows, knees, and medial malleoli. This is considered to be an extended part of the spectrum of Gottron's papules.
-

Gottron's papules. Erythematous plaques overlying the elbows in two patients with juvenile dermatomyositis. In some patients, small erythematous plaques may overly the extensor aspects of larger joints, such as the elbows, knees, and medial malleoli. This is considered to be an extended part of the spectrum of Gottron's papules. Note in Figure, a focal area of dystrophic calcification at the site of Gottron's papules, which is indicative of damage, as discussed below.
-

Gottron's papules with telangiectasia. Gottron's papules with prominent atrophy, porcelain white scarring, and telangiectasia.
-

Gottron's sign. Confluent macular erythema with scale confined to the skin overlying the patellae in a girl with juvenile dermatomyositis.
-

Gottron's papules showing secondary atrophy and telangiectasia in a girl with severe juvenile dermatomyositis. These changes are seen in association with prominent periungual erythema, a cutaneous finding indicative of ongoing disease activity.
-

Heliotrope. Confluent macular erythema confined to the upper eyelid, with associated periorbital edema.
-

Heliotrope. In patients who have darker skin types (type III - VI skin), heliotrope can be subtle and perceived as inactive or normal, resulting in under-diagnosis in this presenting sign of dermatomyositis.
-

Heliotrope is often associated with periorbital edema and telangiectasias of the upper eyelids. In the resolution stage, atrophy or dyspigmentation (hypo- or hyperpigmentation) may be apparent. Heliotrope. Subtle erythema and minimal edema involving both upper eyelids, with extension to the lower eyelids.
-

Malar and facial erythema. Acute onset of confluent macular erythema in a periorbital and malar distribution with extension to the chin in a girl with juvenile dermatomyositis. Note the perioral sparing.
-

Malar and facial erythema. Striking malar and facial erythema with facial edema and scale represents a recent disease flare in an adult patient with dermatomyositis.
-

Linear extensor erythema. Confluent erythema of the skin overlying the interphalangeal and extensor tendons of the hand, with extension to the forearm in a patient with dermatomyositis
-

Linear extensor erythema involving the forearm. This image demonstrates linear violaceous discrete and confluent macules, and erosions secondary to excoriation. Pruritus is an under-recognized symptom of active dermatomyositis.
See also
- Poikiloderma vasculare atrophicans
- List of cutaneous conditions
References
- ^ Scheinfeld NS (2006). "Ulcerative paraneoplastic dermatomyositis secondary to metastatic breast cancer". Skinmed 5 (2): 94–6. doi:10.1111/j.1540-9740.2006.03637.x. PMID 16603844. http://www.lejacq.com/articleDetail.cfm?pid=SKINmed_5;2:94.
- ^ Page 285 in: Thomson and Cotton Lecture Notes in Pathology, Blackwell Scientific. Third Edition
- ^ "Polymyositis and Dermatomyositis: Autoimmune Disorders of Connective Tissue: Merck Manual Home Edition". http://www.merck.com/mmhe/sec05/ch068/ch068e.html.
- ^ Page 151 in: Mitchell, Richard Sheppard; Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson (2007). Robbins Basic Pathology. Philadelphia: Saunders. ISBN 1-4160-2973-7. 8th edition.
- ^ Ghirardello, A; Zampieri S, Tarricone E et al. (May 2006). "Clinical implications of autoantibody screening in patients with autoimmune myositis". Autoimmunity 39 (3): 217–221. doi:10.1080/08916930600622645. PMID 16769655.
- ^ Benveniste, O; Squier W, Boyer O et al. (November 2004). "Pathogenesis of primary inflammatory myopathies". Presse Médicale 33 (20): 1444–1450. doi:10.1016/S0755-4982(04)98952-X. PMID 15611679.
- ^ Nirmalananthan, N; Holton JL, Hanna MG (November 2004). "Is it really myositis? A consideration of the differential diagnosis". Current Opinion in Rheumatology 16 (6): 684–691. doi:10.1097/01.bor.0000143441.27065.bc. PMID 15577605.
- ^ Scheinfeld N (2006). "A review of rituximab in cutaneous medicine". Dermatol. Online J. 12 (1): 3. PMID 16638371. http://dermatology.cdlib.org/121/reviews/rituxab/scheinfeld.html.
- ^ "Forgotten: Ricky Bell". Pro Football Weekly. 8 January 2010. http://www.profootballweekly.com/2010/01/08/forgotten-ricky-bell. Retrieved 26 January 2010.
External links
- The Myositis Association [2]
- Muscular Dystrophy Association [3]
- The American College of Rheumatology's patient education page on myopathy
- Illustration of Gottron's papules at University of Iowa
- The Johns Hopkins Myositis Center [4]
- Myositis Support Group
Systemic CT disorders (M32–M36, 710) General Inflammatory myopathy/Myositis: Dermatopolymyositis (Dermatomyositis/Juvenile dermatomyositis, Polymyositis) · Inclusion body myositisOther hypersensitivity/autoimmune Other Paraneoplastic syndromes Endocrine Hematological Neurological Paraneoplastic cerebellar degeneration · Encephalomyelitis · Limbic encephalitis · Opsoclonus · Polymyositis · Transverse myelitis · Lambert–Eaton myasthenic syndrome · Anti-NMDA receptor encephalitisMusculoskeletal Dermatomyositis · Hypertrophic osteoarthropathyMucocutaneous reactive erythema: Erythema gyratum repens · Necrolytic migratory erythema
papulosquamous: Acanthosis nigricans · Acquired ichthyosis · Acrokeratosis paraneoplastica of Bazex · Extramammary Paget's disease · Florid cutaneous papillomatosis · Leser-Trélat sign · Pityriasis rotunda · Tripe palms
other/ungrouped: Febrile neutrophilic dermatosis · Pyoderma gangrenosum · Paraneoplastic pemphigusM: NEO
tsoc, mrkr
tumr, epon, para
drug (L1i/1e/V03)
Categories:- Connective tissue diseases
- Diseases involving the fasciae
- Inflammations
- Autoimmune diseases
- Systemic connective tissue disorders














Wikimedia Foundation. 2010.