- Appendicitis
-
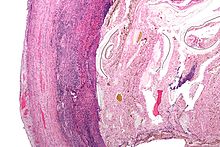
Appendicitis Classification and external resources 
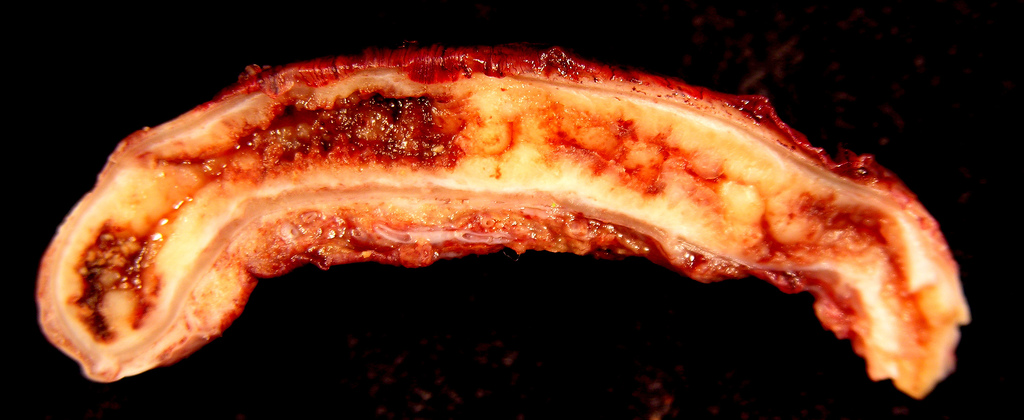
An acutely inflamed and enlarged appendix, sliced lengthwise.ICD-10 K35 - K37 ICD-9 540-543 DiseasesDB 885 MedlinePlus 000256 eMedicine med/3430 emerg/41 ped/127 ped/2925 MeSH C06.405.205.099 Appendicitis is a condition characterized by inflammation of the appendix. It is classified as a medical emergency and many cases require removal of the inflamed appendix, either by laparotomy or laparoscopy. Untreated, mortality is high, mainly because of the risk of rupture leading to peritonitis and shock.[1] Reginald Fitz first described acute and chronic appendicitis in 1886,[2] and it has been recognized as one of the most common causes of severe acute abdominal pain worldwide. A correctly diagnosed non-acute form of appendicitis is known as "rumbling appendicitis".
The term "pseudoappendicitis" is used to describe a condition mimicking appendicitis.[3] It can be associated with Yersinia enterocolitica.[4]
Contents
Signs and symptoms
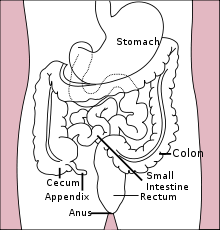 Location of the appendix in the digestive system
Location of the appendix in the digestive system
For the most part, symptoms are related to disturbed bowel functions. Pain first, vomiting next and fever last has been described as classic presentation of acute appendicitis. Pain starts mid abdomen, and except in children below 3 years, tends to localize in right iliac fossa in a few hours. This pain can be elicited through various signs. Signs include localized findings in the right iliac fossa. The abdominal wall becomes very sensitive to gentle pressure (palpation). Also, there is severe pain on suddenly releasing a deep pressure in lower abdomen (rebound tenderness). In case of a retrocecal appendix, however, even deep pressure in the right lower quadrant may fail to elicit tenderness (silent appendix), the reason being that the cecum, distended with gas, prevents the pressure exerted by the palpating hand from reaching the inflamed appendix. Similarly, if the appendix lies entirely within the pelvis, there is usually complete absence of the abdominal rigidity. In such cases, a digital rectal examination elicits tenderness in the rectovesical pouch. Coughing causes point tenderness in this area (McBurney's point) and this is the least painful way to localize the inflamed appendix. If the abdomen on palpation is also involuntarily guarded (rigid), there should be a strong suspicion of peritonitis requiring urgent surgical intervention.
Not typical Pain is usually not typical in some patients, who may just only have lower right abdominal pain no mid-upper abdominal pain at the beginning. Often, the pain is not prominent in the elderly or children below 3-year-old. Or the pain point moves to other locations, especially just below the liver in pregnant woman. In this case, the inflamed appendix is pushed up by enlarged uterus.[5]
Rovsing's sign
Continuous deep palpation starting from the left iliac fossa upwards (counterclockwise along the colon) may cause pain in the right iliac fossa, by pushing bowel contents towards the ileocaecal valve and thus increasing pressure around the appendix. This is the Rovsing's sign.[6]
Psoas sign
Main article: Psoas signPsoas sign or "Obraztsova's sign" is right lower-quadrant pain that is produced with either the passive extension of the patient's right hip (patient lying on left side, with knee in flexion) or by the patient's active flexion of the right hip while supine. The pain elicited is due to inflammation of the peritoneum overlying the iliopsoas muscles and inflammation of the psoas muscles themselves. Straightening out the leg causes pain because it stretches these muscles, while flexing the hip activates the iliopsoas and therefore also causes pain.
Obturator sign
If an inflamed appendix is in contact with the obturator internus, spasm of the muscle can be demonstrated by flexing and internal rotation of the hip. This maneuver will cause pain in the hypogastrium.
Dunphy's sign
Increased pain in the right lower quadrant with coughing.[7]
Kocher's (Kosher's) sign
From the history given, the appearance of pain in the epigastric region or around the stomach at the beginning of disease with a subsequent shift to the right iliac region.
Sitkovskiy (Rosenstein)'s sign
Increased pain in the right iliac region as patient lies on his/her left side.
Bartomier-Michelson's sign
Increased pain on palpation at the right iliac region as patient lies on his/her left side compared to when patient was on supine position.
Aure-Rozanova's sign
Increased pain on palpation with finger in right Petit triangle (can be a positive Shchetkin-Bloomberg's sign) - typical in retrocecal position of the appendix.[8]
Blumberg sign
Also referred as rebound tenderness. Deep palpation of the viscera over the suspected inflamed appendix followed by sudden release of the pressure causes the severe pain on the site indicating positive Blumberg's sign and peritonitis.[9]
Causes
On the basis of experimental evidence, acute appendicitis seems to be the end result of a primary obstruction of the appendix lumen (the inside space of a tubular structure).[10][11] Once this obstruction occurs the appendix subsequently becomes filled with mucus and swells, increasing pressures within the lumen and the walls of the appendix, resulting in thrombosis and occlusion of the small vessels, and stasis of lymphatic flow. Rarely, spontaneous recovery can occur at this point. As the former progresses, the appendix becomes ischemic and then necrotic. As bacteria begin to leak out through the dying walls, pus forms within and around the appendix (suppuration). The end result of this cascade is appendiceal rupture (a 'burst appendix') causing peritonitis, which may lead to septicemia and eventually death.
The causative agents include foreign bodies, trauma, intestinal worms, lymphadenitis, and most commonly calcified fecal deposits known as appendicoliths or fecaliths[12] The occurrence of an obstructing fecalith has attracted attention since their presence in patients with appendicitis is significantly higher in developed than in developing countries,[13] and an appendiceal fecalith is commonly associated with complicated appendicitis.[14] Also, fecal stasis and arrest may play a role, as demonstrated by a significantly lower number of bowel movements per week in patients with acute appendicitis compared with healthy controls.[15] The occurrence of a fecalith in the appendix seems to be attributed to a right sided fecal retention reservoir in the colon and a prolonged transit time.[16] From epidemiological data it has been stated that diverticular disease and adenomatous polyps were unknown and colon cancer exceedingly rare in communities exempt for appendicitis.[17][18] Also, acute appendicitis has been shown to occur antecedent to cancer in the colon and rectum.[19] Several studies offer evidence that a low fiber intake is involved in the pathogenesis of appendicitis[20] .[21][22] This is in accordance with the occurrence of a right sided fecal reservoir and the fact that dietary fiber reduces transit time.[23]
Diagnosis
Diagnosis is based on patient history (symptoms) and physical examination backed by an elevation of neutrophilic white blood cells. Histories fall into two categories, typical and atypical. Typical appendicitis usually includes abdominal pain beginning in the region of the umbilicus for several hours, associated with anorexia, nausea or vomiting. The pain then "settles" into the right lower quadrant, where tenderness develops. Atypical histories lack this typical progression and may include pain in the right lower quadrant as an initial symptom. Atypical histories often require imaging with ultrasound and/or CT scanning.[24] A pregnancy test is vital in all women of child bearing age, as ectopic pregnancies and appendicitis present with similar symptoms. The consequences of missing an ectopic pregnancy are serious, and potentially life threatening. Furthermore the general principles of approaching abdominal pain in women (in so much that it is different from the approach in men) should be appreciated.
Blood Test
Most patients suspected of having appendicitis would be asked to do a blood test. 50% of the time, the blood test may be normal, so it is not foolproof in diagnosing appendicitis.
Two form of blood tests are commonly done: FBC (Full blood count) or CBC (Complete blood count), is an inexpensive and commonly requested blood test. It involves measuring the blood for its richness in red blood cells as well as the number of the various white blood cell constituents in it. The number of white cells in the blood is a usually less than 10,000 cells per cubic millimeter. An abnormal rise in the number of white blood cells in the blood is a crude indicator of infection or inflammation going on in the body. Such rise is not specific to appendicitis alone. If it is abnormally elevated, with a good history and examination findings pointing towards appendicitis, the likelihood of having the disease is higher. In pregnancy, there may be a normal elevation of white blood cells, without any infection present.
CRP is an acronym for C-reactive protein. It is an acute phase response protein produced by the liver in response to any infection or inflammatory process in the body. Again, like the FBC, it is not a specific test. It is another crude marker of infection or inflammation. Inflammation at ANY site can lead to the CRP to rise. A significant rise in CRP with corresponding signs and symptoms of appendicitis is a useful indicator in the diagnosis of appendicitis.It is said that if CRP continues to be normal after 72 hours of the onset of pain, it is likely that the appendicitis will resolve on its own without intervention. A worsening CRP with good history is a sure signal of impending perforation or rupture and abscess formation.
Urine Test
Urine test in appendicitis is usually normal. It may however show blood if the appendix is rubbing on the bladder, causing irritation A urine test or urinalysis is compulsory in women, to rule out pregnancy in appendicitis, as well to help ensure that the abdominal pain felt and thought to be acute appendicitis is not in fact, due to ectopic pregnancy.
X–Ray
In 10% of patients with appendicitis, plain abdominal x-ray may demonstrate hard formed feces in the lumen of the appendix (Fecolith). It is agreed that the finding of Fecolith in the appendix on X – ray alone is a reason to operate to remove the appendix, because of the potential to cause worsening symptoms. In this respect, a plain abdominal X-ray may be useful in the diagnosis of appendicitis, though plain abdominal x- ray is no longer requested routinely in suspected cases of appendicitis. An abdominal X – ray may be done with a barium enema contrast to diagnose appendicitis. Barium enema is whitish toothpaste like material that is passed up into the rectum to act as a contrast. It will usually fill the whole of the large bowel. In normal appendix, the lumen will be present and the barium fills it up and is seen when the x-ray film is shot. In appendicitis, the lumen of the appendix will not be visible on the barium film.
Ultrasound
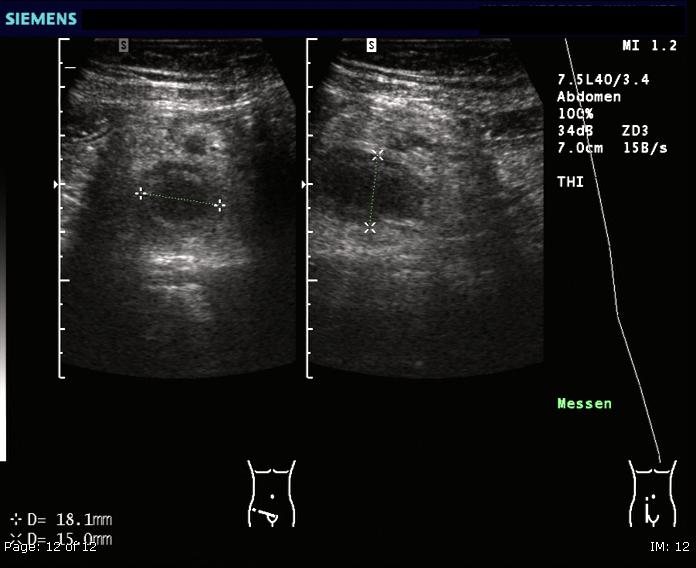
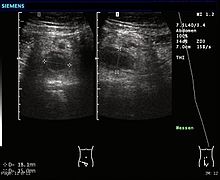 Ultrasound image of an acute appendicitis.
Ultrasound image of an acute appendicitis.Ultrasonography and Doppler sonography provide useful means to detect appendicitis, especially in children and shows free fluid collection in right iliac fossa along with a visible appendix without blood flow in color Doppler. In some cases (15% approximately), however, ultrasonography of the iliac fossa does not reveal any abnormalities despite the presence of appendicitis. This is especially true of early appendicitis before the appendix has become significantly distended and in adults where larger amounts of fat and bowel gas make actually seeing the appendix technically difficult. Despite these limitations, in experienced hands sonographic imaging can often distinguish between appendicitis and other diseases with very similar symptoms such as inflammation of lymph nodes near the appendix or pain originating from other pelvic organs such as the ovaries or fallopian tubes.
Computed tomography
 A cat scan demonstrating acute appendicitis (note the appendix has a diameter of 17.1mm and there is surrounding fat stranding.)
A cat scan demonstrating acute appendicitis (note the appendix has a diameter of 17.1mm and there is surrounding fat stranding.) A fecalith marked by the arrow which has resulted in acute appendicitis.
A fecalith marked by the arrow which has resulted in acute appendicitis.In places where it is readily available, CT scan has become frequently used, especially in adults whose diagnosis is not obvious on history and physical. Concerns about radiation, however, tend to limit use of CT in pregnant women and children. A properly performed CT scan with modern equipment has a detection rate (sensitivity) of over 95% and a similar specificity. Signs of appendicitis on CT scan include lack of oral contrast (oral dye) in the appendix, direct visualization of appendiceal enlargement (greater than 6 mm in cross sectional diameter), and appendiceal wall enhancement with IV contrast (IV dye). The inflammation caused by appendicitis in the surrounding peritoneal fat (so called "fat stranding") can also be observed on CT, providing a mechanism to detect early appendicitis and a clue that appendicitis may be present even when the appendix is not well seen. Thus, diagnosis of appendicitis by CT is made more difficult in very thin patients and in children, both of whom tend to lack significant fat within the abdomen. The utility of CT scanning is made clear, however, by the impact it has had on negative appendectomy rates. For example, use of CT for diagnosis of appendicitis in Boston, MA has decreased the chance of finding a normal appendix at surgery from 20% in the pre-CT era to only 3% according to data from the Massachusetts General Hospital.
Ultrasound and CT compared
According to a systematic review from UC-San Francisco comparing ultrasound vs. CT scan, CT scan is more accurate than ultrasound for the diagnosis of appendicitis in adults and adolescents. CT scan has a sensitivity of 94%, specificity of 95%, a positive likelihood ratio of 13.3 (CI, 9.9 to 17.9), and a negative likelihood ratio of 0.09 (CI, 0.07 to 0.12). Ultrasonography had an overall sensitivity of 86%, a specificity of 81%, a positive likelihood ratio of 5.8 (CI, 3.5 to 9.5), and a negative likelihood ratio of 0.19 (CI, 0.13 to 0.27).[25]
Alvarado score
Alvarado score Migratory right iliac fossa pain 1 point Anorexia 1 point Nausea and vomiting 1 point Right iliac fossa tenderness 2 points Rebound tenderness 1 point Fever 1 point Leukocytosis 2 points Shift to left (segmented neutrophils) 1 point Total score 10 points A number of clinical and laboratory based scoring systems have been devised to assist diagnosis. The most widely used is Alvarado score. A score below 5 is strongly against a diagnosis of appendicitis,[26] while a score of 7 or more is strongly predictive of acute appendicitis. In patients with an equivocal score of 5-6, CT scan is used to further reduce the rate of negative appendicectomy.
Other data
- Tzanakis Scoring
- Tzanakis and colleagues, in 2005 published a simplified system, now called the Tzanakis scoring system for appendicitis, to aid the diagnosis of appendicitis. It incorporates the presence 4 variables made up of specific signs and symptoms (presence of right lower abdominal tenderness = 4points and rebound tenderness = 3), laboratory findings (presence of white blood cells greater than 12,000 in the blood = 2) as well as ultrasound findings (presence of positive ultrasound scan findings of appendicitis = 6), to which scores are allocated, in the computing of a scoring to predict the presence of appendicitis.
A total score of 15 is the maximum that can be scored. Where a patient scores 8 or more points, there is greater than 96 percent chance that appendicitis exists.
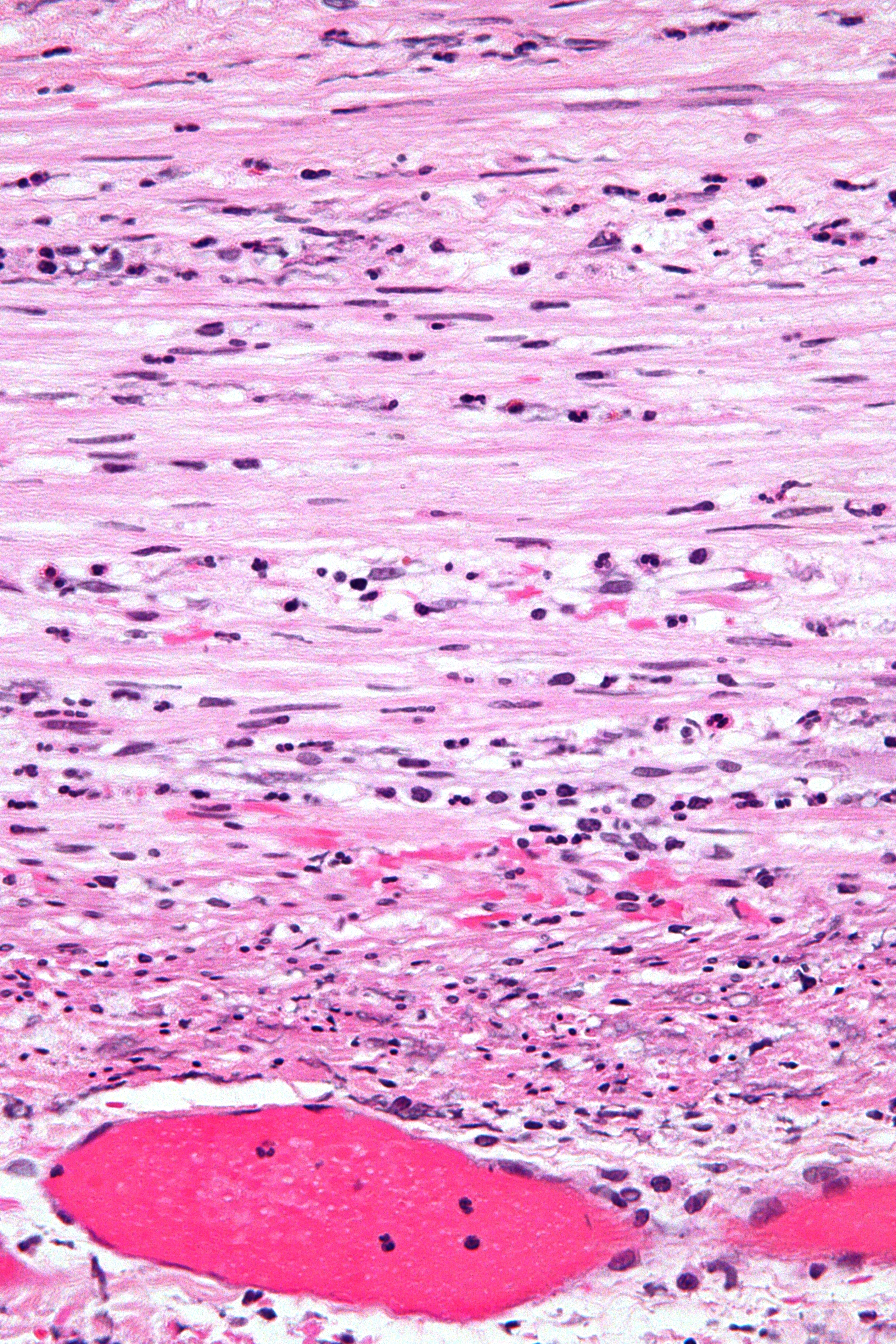
Pathologic diagnosis

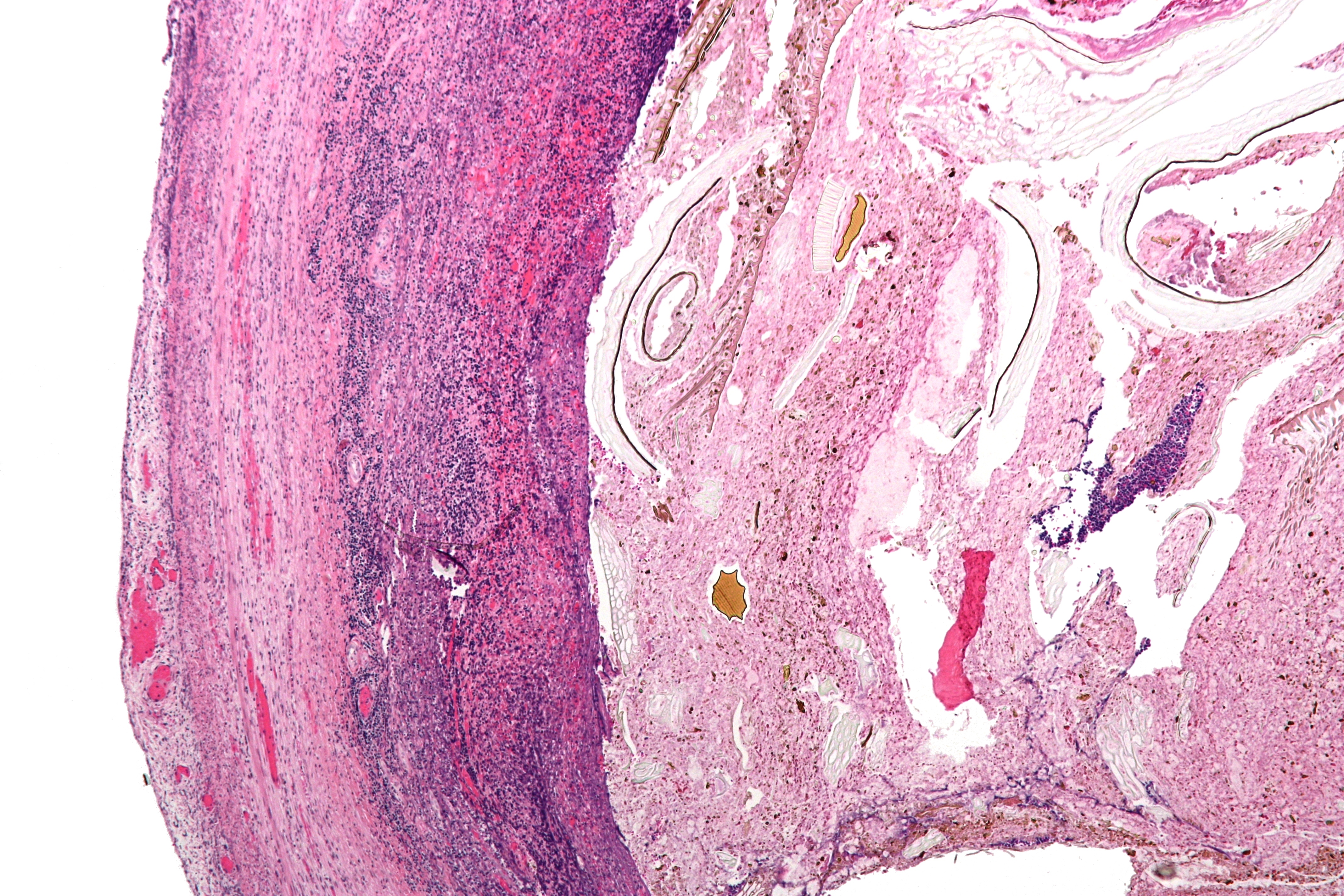
The definitive diagnosis is based on pathology. The histologic findings of appendicits are neutrophils in the muscularis propria.
Periappendicits, inflammation of tissues around the appendix, is often found in conjunction with other abdominal pathology.[27]
Differential diagnosis
- In children
- Gastroenteritis, mesenteric adenitis, Meckel's diverticulitis, intussusception, Henoch-Schönlein purpura, lobar pneumonia, urinary tract infection (abdominal pain in the absence of other symptoms can occur in children with UTI), new-onset Crohn's disease or ulcerative colitis, pancreatitis, and abdominal trauma from child abuse; distal intestinal obstruction syndrome in children with cystic fibrosis; typhlitis in children with leukemia;
- In girls
- menarche, dysmenorrhea, severe menstrual cramps, Mittelschmerz, pelvic inflammatory disease, ectopic pregnancy
- In adults
- regional enteritis, renal colic, perforated peptic ulcer, pancreatitis, rectus sheath hematoma; in men: testicular torsion, new-onset Crohn's disease or ulcerative colitis; in women: pelvic inflammatory disease, ectopic pregnancy, endometriosis, torsion/rupture of ovarian cyst, Mittelschmerz (the passing of an egg in the ovaries approximately two weeks before an expected menstruation cycle)
- In elderly
- diverticulitis, intestinal obstruction, colonic carcinoma, mesenteric ischemia, leaking aortic aneurysm.
Management
Largely surgical, any conservative management is done at the threshold of operation theater as the acutely inflamed appendix is liable to rupture during such treatment.
 Inflamed appendix removal by open surgery
Inflamed appendix removal by open surgeryThe treatment begins by keeping the patient from eating or drinking in preparation for surgery. An intravenous drip is used to hydrate the patient. Antibiotics given intravenously such as cefuroxime and metronidazole may be administered early to help kill bacteria and thus reduce the spread of infection in the abdomen and postoperative complications in the abdomen or wound. Equivocal cases may become more difficult to assess with antibiotic treatment and benefit from serial examinations. If the stomach is empty (no food in the past six hours) general anaesthesia is usually used. Otherwise, spinal anaesthesia may be used.
Once the decision to perform an appendectomy has been made, the preparation procedure takes more or less one to two hours. Meanwhile, the surgeon will explain the surgery procedure and will present the risks that must be considered when performing an appendectomy. With all surgeries there are certain risks that must be evaluated before performing the procedures. However, the risks are different depending on the state of the appendix. If the appendix has not ruptured, the complication rate is only about 3% but if the appendix has ruptured, the complication rate rises to almost 59%.[28] The most usual complications that can occur are pneumonia, hernia of the incision, thrombophlebitis, bleeding or adhesions. Recent evidence indicates that a delay in obtaining surgery after admission results in no measurable difference in patient outcomes [29]
The surgeon will also explain how long the recovery process should take. Abdomen hair is usually removed in order to avoid complications that may appear regarding the incision. In most of the cases patients experience nausea or vomiting which requires specific medication before surgery. Antibiotics along with pain medication may also be administrated prior to appendectomies.
Pain management
Pain from appendicitis can be severe. Strong pain medications (i.e., narcotic pain medications) are recommended for pain management prior to surgery. Morphine is generally the standard of care in adults and children in the treatment of pain from appendicitis prior to surgery.[citation needed]
In the past (and in some medical textbooks that are still published today), it was commonly accepted among the majority of academic sources[weasel words] that pain medication not be given until the surgeon has the chance to evaluate the patient, so as to not "corrupt" the findings of the physical examination. This line of practice, combined with the fact that surgeons may sometimes take hours to come to evaluate the patient, especially if he or she is in the middle of surgery or has to drive in from home, often leads to a situation that is ethically questionable at best.[citation needed] More recently, due to better understanding of the importance of pain control in patients, it has been shown that the physical examination is actually not that dramatically disturbed when pain medication is given prior to medical evaluation. Individual hospitals and clinics have adapted to this new approach of pain management of appendicitis by developing a compromise of allowing the surgeon a maximum time to arrive for evaluation, such as 20 to 30 minutes, before active pain management is initiated. Many surgeons also advocate this new approach of providing pain management immediately rather than only after surgical evaluation.
Surgery
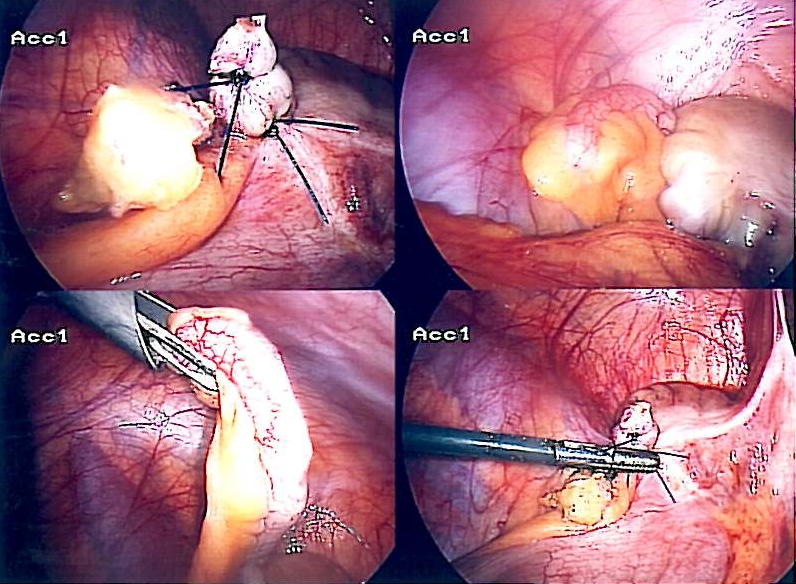
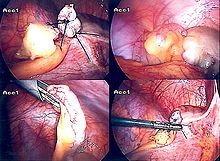 Laparoscopic appendectomy.
Laparoscopic appendectomy.The surgical procedure for the removal of the appendix is called an appendicectomy (also known as an appendectomy). Often now the operation can be performed via a laparoscopic approach, or via three small incisions with a camera to visualize the area of interest in the abdomen. If the findings reveal suppurative appendicitis with complications such as rupture, abscess, adhesions, etc., conversion to open laparotomy may be necessary. An open laparotomy incision if required most often centers on the area of maximum tenderness, McBurney's point, in the right lower quadrant. A transverse or a gridiron diagonal incision is used most commonly.
According to a meta-analysis from the Cochrane Collaboration comparing laparoscopic and open procedures, laparoscopic procedures seem to have various advantages over the open procedure. Wound infections were less likely after laparoscopic appendicectomy than after open appendicectomy (odds ratio (OR) 0.45; confidence interval (CI) 0.35 to 0.58), but the incidence of intraabdominal abscesses was increased (OR 2.48; CI 1.45 to 4.21). The duration of surgery was 12 minutes (CI 7 to 16) longer for laparoscopic procedures. Pain on day 1 after surgery was reduced after laparoscopic procedures by 9 mm (CI 5 to 13 mm) on a 100 millimeter visual analogue scale. Hospital stay was shortened by 1.1 day (CI 0.6 to 1.5). Return to normal activity, work, and sport occurred earlier after laparoscopic procedures than after open procedures. While the operation costs of laparoscopic procedures were significantly higher, the costs outside hospital were reduced. Young female, obese, and employed patients seem to benefit from the laparoscopic procedure more than other groups.[30]
There is debate whether emergency appendicectomy (within 6 hours of admission) reduces the risk of perforation or complication versus urgent appendicectomy (greater than 6 hours after admission). According to a retrospective case review study [31] no significant differences in perforation rate among the two groups were noted (P=.397). Various complications (abscess formation, re-admission) showed no significant differences (P=0.667, 0.999). According to this study, beginning antibiotic therapy and delaying appendicectomy from the middle of the night to the next day does not significantly increase the risk of perforation or other complications. This finding is important not simply for the convenience of the surgeons and staff involved but for the fact that there have been other studies that have shown that surgeries taking place during the night, when people may be more tired and there are fewer staff available, have higher rates of surgical complications.
Findings at the time of surgery are less severe in typical appendicitis. With atypical histories, perforation is more common and findings suggest perforation occurs at the beginning of symptoms. These observations may fit a theory that acute (typical) appendicitis and suppurative (atypical) appendicitis are two distinct disease processes. (1)
Surgery may last from 30 minutes in typical appendicitis in thin patients to several hours in complicated cases.
Laparotomy explained
Laparotomy is the traditional type of surgery used for treating appendicitis. This procedure consists in the removal of the infected appendix through a single larger incision in the lower right area of the abdomen.[32] The incision in a laparotomy is usually 2-3 inches long. This type of surgery is used also for visualizing and examining structures inside the abdominal cavity and it is called exploratory laparotomy.
During a traditional appendectomy procedure, the patient is placed under general anesthesia in order to keep his/her muscles completely relaxed and to keep the patient unconscious. The incision is two to three inches (76 mm) long and it is made in the right lower abdomen, several inches above the hip bone.[33] Once the incision opens the abdomen cavity and the appendix is identified, the surgeon removes the infected tissue and cuts the appendix from the surrounding tissue. After the surgeon inspects carefully and closely the infected area and there are no signs that surrounding tissues are damaged or infected, he will start closing the incision. This means sewing the muscles and using surgical staples or stitches to close the skin up. In order to prevent infections the incision is covered with a sterile bandage. The entire procedure does not last longer than an hour if complications do not occur.
Laparoscopic surgery
The newer method to treat appendicitis is the laparoscopic surgery. This surgical procedure consists of making three to four incisions in the abdomen, each 0.25 to 0.5 inch (6.3 to 13 mm) long. This type of appendectomy is made by inserting a special surgical tool called laparoscope into one of the incisions. The laparoscope is connected to a monitor outside the patient's body and it is designed to help the surgeon to inspect the infected area in the abdomen. The other two incisions are made for the specific removal of the appendix by using surgical instruments. Laparoscopic surgery also requires general anesthesia and it can last up to two hours. The latest methods are NOTES appendectomy pioneered in Coimbatore, India where there is no incision on the external skin[34] and SILS( Single incision laparoscopic Surgery)where a single 2.5 cm incision is made to perform the surgery.
After surgery
 The stitches the day after having his appendix removed by laparoscopic surgery.
The stitches the day after having his appendix removed by laparoscopic surgery.Hospital lengths of stay typically range from a few hours to a few days, but can be a few weeks if complications occur. The recovery process may vary depending on the severity of the condition, if the appendix had ruptured or not before surgery. Appendix surgery recovery is generally a lot faster if the appendix did not rupture.[35] It is important that patients respect their doctor's advice and limit their physical activity so the tissues can heal faster. Recovery after an appendectomy may not require diet changes or a lifestyle change.
After surgery occurs, the patient will be transferred to an Post-anesthesia care unit so his or her vital signs can be closely monitored in order to detect anesthesia and/or surgery related complications. Pain medication may also be administrated if necessary. After patients are completely awake, they are moved into a hospital room to recover. Most individuals will be offered clear liquids the day after the surgery and then progress to a regular diet when the intestines start to function properly. It is highly recommended that patients sit up on the edge of the bed and walk short distances for several times a day. Moving is mandatory and pain medication may be given if necessary. Full recovery from appendectomies takes about 4 to 6 weeks but it can prolong to up to 8 weeks if the appendix had ruptured.
Prognosis
Most appendicitis patients recover easily with surgical treatment, but complications can occur if treatment is delayed or if peritonitis occurs. Recovery time depends on age, condition, complications, and other circumstances, including the amount of alcohol consumption, but usually is between 10 and 28 days. For young children (around 10 years old), the recovery takes three weeks.
The real possibility of life-threatening peritonitis is the reason why acute appendicitis warrants speedy evaluation and treatment. The patient may have to undergo a medical evacuation. Appendectomies have occasionally been performed in emergency conditions (i.e., outside of a proper hospital), when a timely medical evaluation was impossible.
Typical acute appendicitis responds quickly to appendectomy and occasionally will resolve spontaneously. If appendicitis resolves spontaneously, it remains controversial whether an elective interval appendectomy should be performed to prevent a recurrent episode of appendicitis. Atypical appendicitis (associated with suppurative appendicitis) is more difficult to diagnose and is more apt to be complicated even when operated early. In either condition, prompt diagnosis and appendectomy yield the best results with full recovery in two to four weeks usually. Mortality and severe complications are unusual but do occur, especially if peritonitis persists and is untreated. Another entity known as appendicular lump is talked about quite often. It happens when appendix is not removed early during infection and omentum and intestine get adherent to it forming a palpable lump. During this period, operation is risky unless there is pus formation evident by fever and toxicity or by USG. Medical management treats the condition.
An unusual complication of an appendectomy is "stump appendicitis": inflammation occurs in the remnant appendiceal stump left after a prior incomplete appendectomy.[36]
Epidemiology
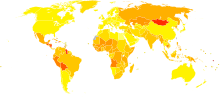 Disability-adjusted life year for appendicitis per 100,000 inhabitants in 2004.[37]no dataless than 2.52.5-55-7.57.5-1010-12.512.5-1515-17.517.5-2020-22.522.5-2525-27.5more than 27.5
Disability-adjusted life year for appendicitis per 100,000 inhabitants in 2004.[37]no dataless than 2.52.5-55-7.57.5-1010-12.512.5-1515-17.517.5-2020-22.522.5-2525-27.5more than 27.5References
- ^ Hobler, K. (Spring 1998). "Acute and Suppurative Appendicitis: Disease Duration and its Implications for Quality Improvement" (– Scholar search). Permanente Medical Journal 2 (2). http://xnet.kp.org/permanentejournal/spring98pj/Spring98.pdf#page=7.[dead link]
- ^ Fitz RH (1886). "Perforating inflammation of the vermiform appendix with special reference to its early diagnosis and treatment". Am J Med Sci (92): 321–46.
- ^ Cunha BA, Pherez FM, Durie N (July 2010). "Swine influenza (H1N1) and acute appendicitis". Heart Lung 39 (6): 544–6. doi:10.1016/j.hrtlng.2010.04.004. PMID 20633930. http://linkinghub.elsevier.com/retrieve/pii/S0147-9563(10)00132-9.
- ^ Zheng H, Sun Y, Lin S, Mao Z, Jiang B (August 2008). "Yersinia enterocolitica infection in diarrheal patients". Eur. J. Clin. Microbiol. Infect. Dis. 27 (8): 741–52. doi:10.1007/s10096-008-0562-y. ISBN 0960080562. PMID 18575909.
- ^ Lawrence W. Way, Gerard M. Doherty (in English). Surgery. US: McGraw-Hill Companies, Inc.. ISBN 0-8385-1456-1.
- ^ N. T. Rovsing: Indirektes Hervorrufen des typischen Schmerzes an McBurney's Punkt. Ein Beitrag zur diagnostik der Appendicitis und Typhlitis. Zentralblatt für Chirurgie, Leipzig, 1907, 34: 1257-1259
- ^ Small V (2008) Surgical emergencies. In Dolan B and Holt L (eds) Accident and Emergency: Theory into Practice, 2nd edition. Elsevier.
- ^ http://max.1gb.ru/surg/s16_pract.shtml
- ^ "Blumberg's sign - Rebound Tenderness" | Offline Clinic
- ^ Wangensteen OH, Bowers WF (1937). "Significance of the obstructive factor in the genesis of acute appendicitis". Arch Surg 34: 496–526.
- ^ Pieper R, Kager L, Tidefeldt U (1982). "Obstruction of appendix vermiformis causing acute appendicitis. On of the most common causes of this is an acute viral infection which causes lymphoid hyperplasia and therefore obstruction. An experimental study in the rabbit". Acta Chir Scand 148 (1): 63–72. PMID 7136413.
- ^ Hollerman, J., et al. (1988). Acute recurrent appendicitis with appendicolith. Am J Emerg Med 6:6 614-7.
- ^ Jones BA, Demetriades D, Segal I, Burkitt DP (1985). "The prevalence of appendiceal fecaliths in patients with and without appendicitis. A comparative study from Canada and South Africa". Ann. Surg. 202 (1): 80–2. doi:10.1097/00000658-198507000-00013. PMC 1250841. PMID 2990360. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1250841.
- ^ Nitecki S, Karmeli R, Sarr MG (1990). "Appendiceal calculi and fecaliths as indications for appendectomy". Surg Gynecol Obstet 171 (3): 185–8. PMID 2385810.
- ^ Arnbjörnsson E (1985). "Acute appendicitis related to faecal stasis". Ann Chir Gynaecol 74 (2): 90–3. PMID 2992354.
- ^ Raahave D, Christensen E, Moeller H, Kirkeby LT, Loud FB, Knudsen LL (2007). "Origin of acute appendicitis: fecal retention in colonic reservoirs: a case control study". Surg Infect (Larchmt) 8 (1): 55–62. doi:10.1089/sur.2005.04250. PMID 17381397.
- ^ Burkitt DP (1971). "The aetiology of appendicitis". Br J Surg 58 (9): 695–9. doi:10.1002/bjs.1800580916. PMID 4937032.
- ^ Segal I, Walker AR (1982). "Diverticular disease in urban Africans in South Africa". Digestion 24 (1): 42–6. doi:10.1159/000198773. PMID 6813167.
- ^ Arnbjörnsson E (1982). "Acute appendicitis as a sign of a colorectal carcinoma". J Surg Oncol 20 (1): 17–20. doi:10.1002/jso.2930200105. PMID 7078180.
- ^ Burkitt DP, Walker AR, Painter NS (1972). "Effect of dietary fibre on stools and the transit-times, and its role in the causation of disease". Lancet 2 (7792): 1408–12. doi:10.1016/S0140-6736(72)92974-1. PMID 4118696.
- ^ Adamis D, Roma-Giannikou E, Karamolegou K (2000). "Fiber intake and childhood appendicitis". Int J Food Sci Nutr 51 (3): 153–7. doi:10.1080/09637480050029647. PMID 10945110.
- ^ Hugh TB, Hugh TJ (2001). "Appendicectomy--becoming a rare event?". Med. J. Aust. 175 (1): 7–8. PMID 11476215. http://www.mja.com.au/public/issues/175_01_020701/hugh/hugh.html.
- ^ Gear JS, Brodribb AJ, Ware A, Mann JI (1981). "Fibre and bowel transit times". Br. J. Nutr. 45 (1): 77–82. doi:10.1079/BJN19810078. PMID 6258626. http://journals.cambridge.org/abstract_S0007114581000111.
- ^ Hobler, K. (Spring 1998). "Acute and Suppurative Appendicitis: Disease Duration and its Implications for Quality Improvement" (– Scholar search). Permanente Medical Journal 2 (2). http://xnet.kp.org/permanentejournal/spring98pj/Spring98.pdf#page=7.[dead link]
- ^ Terasawa T, Blackmore CC, Bent S, Kohlwes RJ (2004). "Systematic review: computed tomography and ultrasonography to detect acute appendicitis in adults and adolescents". Ann. Intern. Med. 141 (7): 537–46. PMID 15466771.
- ^ "BestBets: The Alvarado Scoring System is an accurate diagnostic tool for appendicitis". http://www.bestbets.org/bets/bet.php?id=1671.
- ^ Fink, AS.; Kosakowski, CA.; Hiatt, JR.; Cochran, AJ. (Jun 1990). "Periappendicitis is a significant clinical finding". Am J Surg 159 (6): 564–8. doi:10.1016/S0002-9610(06)80067-X. PMID 2349982.
- ^ Appendicitis surgery procedures Encyclopedia of surgery Portal. Retrieved on 2010-02-01
- ^ "'Emergency' appendix surgery can wait: MDs". CBC News. 2010-09-21. http://www.cbc.ca/health/story/2010/09/21/appendectomy-waits.html.
- ^ Sauerland S, Lefering R, Neugebauer EA (2004). Sauerland, Stefan. ed. "Laparoscopic versus open surgery for suspected appendicitis". Cochrane Database Syst Rev (4): CD001546. doi:10.1002/14651858.CD001546.pub2. PMID 15495014.
- ^ Yardeni D, Hirschl RB, Drongowski RA, Teitelbaum DH, Geiger JD, Coran AG (2004). "Delayed versus immediate surgery in acute appendicitis: do we need to operate during the night?". J. Pediatr. Surg. 39 (3): 464–9; discussion 464–9. doi:10.1016/j.jpedsurg.2003.11.020. PMID 15017571.
- ^ Appendicitis procedures explained National Digestive Diseases Information Clearinghouse. Retrieved on 2010-02-01
- ^ Laparotomy abdominal surgery About surgeries online portal. Retrieved on 2010-02-01
- ^ 28
- ^ Appendicitis surgery, removal and recovery Retrieved on 2010-02-01
- ^ Liang MK, Lo HG, Marks JL (2006). "Stump appendicitis: a comprehensive review of literature". The American surgeon 72 (2): 162–6. PMID 16536249.
- ^ "WHO Disease and injury country estimates". World Health Organization. 2009. http://www.who.int/healthinfo/global_burden_disease/estimates_country/en/index.html. Retrieved Nov. 11, 2009.
External links
- APPENDIX and APPENDICITS
- Anatomy of Appendix and Appendicits | Medchrome
- Podcast on the management of appendicitis
- Appendicitis and Appendectomy author Dennis Lee, M.D. editor Jay Marks, M.D. - MedicineNet.com, Doctor Produced information plus Patient Discussions provided by MedicineNet.com
- Appendicitis - MayoClinic.com, from the Web site of the Mayo Clinic
- Appendicitis, history, diagnosis and treatment by Surgeons Net Education
- Appendicitis Research Latest research from the literature on appendicitis
- Acute and Suppurative Appendicitis from the Spring 1998 issue of The Permanente Medical Journal
- Appendicitis Update Complete information including laparoscopic appendectomy
- History of Appendicitis Vermiformis: Its diseases and treatment. By Arthur C. McCarty, M.D.
- How to Recognize the Symptoms of Appendicitis, a how-to article from wikiHow
- Appendicitis: Acute Abdomen and Surgical Gastroenterology from the Merck Manual Professional (Content last modified September 2007)
- Abdominal Emergencies, 'Surgical Abdomen'.By DR David Bednarczyk; Pediatric Surgery
Digestive system · Digestive disease · Gastroenterology (primarily K20–K93, 530–579) Upper GI tract Esophagitis (Candidal, Herpetiform) · rupture (Boerhaave syndrome, Mallory-Weiss syndrome) · UES (Zenker's diverticulum) · LES (Barrett's esophagus) · Esophageal motility disorder (Nutcracker esophagus, Achalasia, Diffuse esophageal spasm, Gastroesophageal reflux disease (GERD)) · Laryngopharyngeal reflux (LPR) · Esophageal stricture · MegaesophagusGastritis (Atrophic, Ménétrier's disease, Gastroenteritis) · Peptic (gastric) ulcer (Cushing ulcer, Dieulafoy's lesion) · Dyspepsia · Pyloric stenosis · Achlorhydria · Gastroparesis · Gastroptosis · Portal hypertensive gastropathy · Gastric antral vascular ectasia · Gastric dumping syndrome · Gastric volvulusLower GI tract:
Intestinal/
enteropathyEnteritis (Duodenitis, Jejunitis, Ileitis) — Peptic (duodenal) ulcer (Curling's ulcer) — Malabsorption: Coeliac · Tropical sprue · Blind loop syndrome · small bowel bacterial overgrowth syndrome · Whipple's · Short bowel syndrome · Steatorrhea · Milroy disease · bile acid malabsorptionLarge and/or smallGI bleeding/BIS Accessory Hepatitis (Viral hepatitis, Autoimmune hepatitis, Alcoholic hepatitis) · Cirrhosis (PBC) · Fatty liver (NASH) · vascular (Budd-Chiari syndrome, Hepatic veno-occlusive disease, Portal hypertension, Nutmeg liver) · Alcoholic liver disease · Liver failure (Hepatic encephalopathy, Acute liver failure) · Liver abscess (Pyogenic, Amoebic) · Hepatorenal syndrome · Peliosis hepatisGallbladderCholecystitis · Gallstones/Cholecystolithiasis · Cholesterolosis · Rokitansky-Aschoff sinuses · Postcholecystectomy syndrome · Porcelain gallbladderBile duct/
other biliary treeCholangitis (PSC, Secondary sclerosing cholangitis, Ascending) · Cholestasis/Mirizzi's syndrome · Biliary fistula · Haemobilia · Gallstones/CholelithiasisPancreatitis (Acute, Chronic, Hereditary, Pancreatic abscess) · Pancreatic pseudocyst · Exocrine pancreatic insufficiency · Pancreatic fistulaAbdominopelvic lumbar (Petit's, Grynfeltt-Lesshaft)undefined location (Incisional · Internal hernia)PeritonealCategories:- Inflammations
- Medical emergencies
- General surgery
- Diseases of appendix






Wikimedia Foundation. 2010.