- Mirizzi's syndrome
-
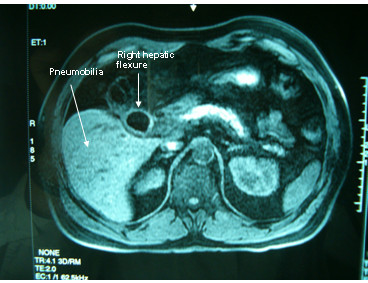
Mirizzi's syndrome Classification and external resources ICD-9 576.2 DiseasesDB 33254 eMedicine radio/451  Spiral CT in a patient with Mirizzi's syndrome with evidence of pneumobilia and suspicion of cholecystocolic fistula.
Spiral CT in a patient with Mirizzi's syndrome with evidence of pneumobilia and suspicion of cholecystocolic fistula.
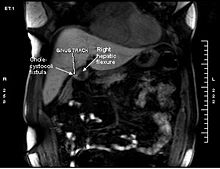 MRI of the same patient:T1 and T2 weighed images with iv contrast Gadolinium- Bopta, revealing fistulous tract between the right colonic flexure and gallbladder (cholecystocolic fistula) and a large gallstone (2 cm).
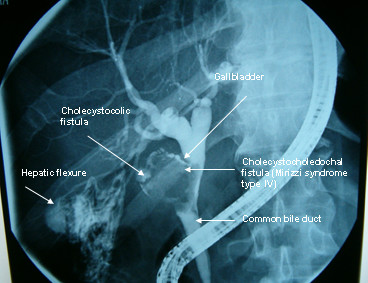
MRI of the same patient:T1 and T2 weighed images with iv contrast Gadolinium- Bopta, revealing fistulous tract between the right colonic flexure and gallbladder (cholecystocolic fistula) and a large gallstone (2 cm).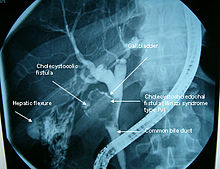 Endoscopic retrograde cholangiopancreatography in the same patient. Severe common bile duct stenosis, with wide cholecystocholedochal communication. A shrunk gallbladder with a large gallstone and a secondary formation of a fistoulous tract, the right hepatic flexure with the contrasted colonic haustration are the highlights of this image modality.
Endoscopic retrograde cholangiopancreatography in the same patient. Severe common bile duct stenosis, with wide cholecystocholedochal communication. A shrunk gallbladder with a large gallstone and a secondary formation of a fistoulous tract, the right hepatic flexure with the contrasted colonic haustration are the highlights of this image modality.Mirizzi's syndrome is a rare cause of acquired jaundice. It is associated with large gallstones that compress the common hepatic duct. The obstructive jaundice can be caused by direct extrinsic compression by the stone or from fibrosis caused by chronic cholecystitis inflammation. A cholecystocholedochal fistula can occur.[1]
Contents
Epidemiology
Mirizzi syndrome occurs in approximately 0.1% of patients with gallstones.[2] It occurs in 0.7 to 2.5 percent of cholecystectomies.[1]
It affects males and females equally, but tends to affect older people more often. There is no evidence of race having any bearing on the epidemiology.
Pathophysiology
Multiple and large gallstones can reside chronically in the Hartmann's pouch of the gallbladder, causing inflammation, necrosis, scarring and ultimately fistula formation into the adjacent common hepatic duct (CHD). As a result, the CHD becomes obstructed by either scar or stone, resulting in jaundice. It can be divided into four types.
Type I - No fistula present
- Type IA - Presence of the cystic duct
- Type IB - Obliteration of the cystic duct
Types II-IV - Fistula present
- Type II - Defect smaller than 33% of the CBD diameter
- Type III - Defect 33-66% of the CBD diameter
- Type IV - Defect larger than 66% of the CBD diameter
Features
Mirizzi syndrome has no consistent or unique clinical features that distinguish it from other more common forms of obstructive jaundice. Symptoms of recurrent cholangitis, jaundice, right upper quadrant pain, and elevated bilirubin and alkaline phosphatase may or may not be present. Acute presentations of the syndrome include pancreatitis or cholecystitis.
Diagnosis
Imaging by CT scan or ultrasonography usually make the diagnosis.[3] Often, ERCP is used to define the lesion anatomically prior to surgery. MRCP is more often used to define the anatomy prior to surgery.
Treatment
The treatment of choice is laparotomic surgical excision of the gallbladder, and reconstruction of the common hepatic duct and common bile duct.
Eponym
It is named for Pablo Luis Mirizzi, an Argentinian physician.[4][5]
References
- ^ a b Vitale M. Mirizzi Syndrome Type IV: An Atypical Presentation That Is Difficult to Diagnose Preoperatively. 2009. Society for Surgery of the Alimentary Tract.http://www.ssat.com/cgi-bin/abstracts/09ddw/P7.cgi
- ^ Hazzan, D; D Golijanin, P Reissman, SN Adler, E Shiloni (06 1999). "Combined endoscopic and surgical management of Mirizzi syndrome". Surgical Endoscopy 13 (6): 618–20. doi:10.1007/s004649901054. PMID 10347304.
- ^ Ross, Jeffrey W; Gary S Sudakoff, Gregory B Snyder, Neela Lamki (editor), Bernard D Coombs (editor), Abraham H Dachman (editor), Robert M Krasny (editor), John Karani (editor) (2006-12-29). "Mirizzi syndrome". eMedicine. WebMD. http://www.emedicine.com/radio/topic451.htm. Retrieved 2007-12-09.
- ^ synd/3587 at Who Named It?
- ^ Mirizzi PL: Syndrome del conducto hepatico. J Int de Chir 1948; 8: 731-77
External links
Categories:- Biliary tract disorders

Wikimedia Foundation. 2010.