- Toxic megacolon
-
Toxic megacolon Classification and external resources 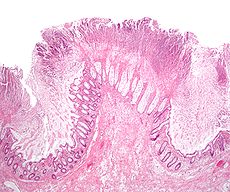
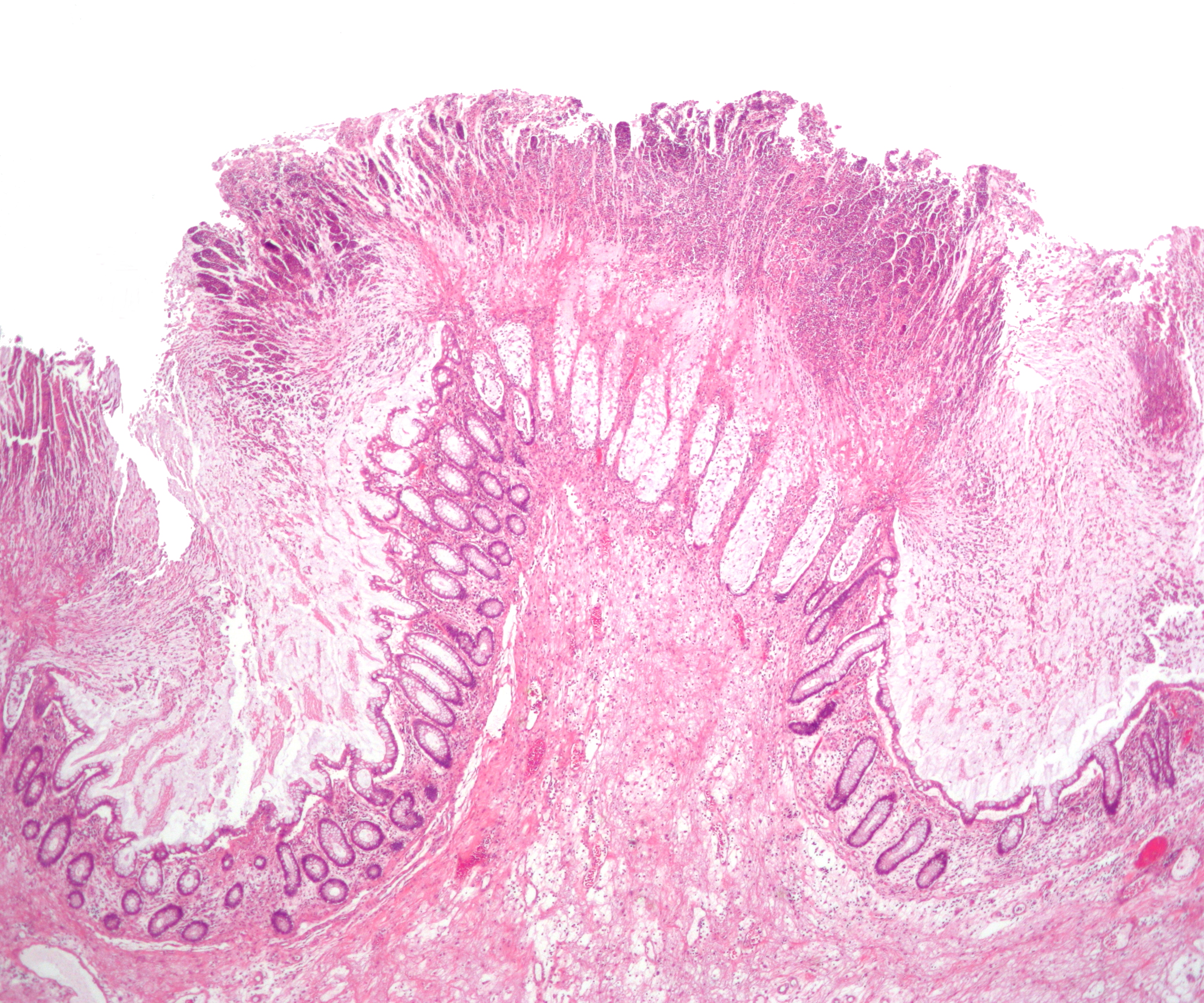
Micrograph of pseudomembranous colitis, a cause of toxic megacolon. H&E stain.ICD-10 K59.3 ICD-9 556.9 DiseasesDB 27702 eMedicine med/1418 radio/702 MeSH D008532 Toxic megacolon (megacolon toxicum) is an acute form of colonic distension.[1] It is characterized by a very dilated colon (megacolon), accompanied by abdominal distension (bloating), and sometimes fever, abdominal pain, or shock.
Toxic megacolon is usually a complication of inflammatory bowel disease, such as ulcerative colitis and, more rarely, Crohn’s disease, and of some infections of the colon, including Clostridium difficile infections which have led to Pseudomembranous colitis. Other forms of megacolon exist and can be congenital (present since birth, such as Hirschsprung's disease).
Contents
Signs and symptoms
- Abdominal pain
- Abdominal bloating
- Abdominal tenderness
- Fever
- Tachycardia (rapid heart rate)
- Dehydration
There may be signs of septic shock. A physical examination reveals abdominal tenderness and possible loss of bowel sounds. An abdominal radiography shows colonic dilation. There is usually an elevated white blood cell count. Severe sepsis may present with hypothermia or leukopenia.
Treatment
The objective of treatment is to decompress the bowel and to prevent swallowed air from further distending the bowel. If decompression is not achieved or the patient does not improve within 24 hours, a colectomy (surgical removal of all or part of the colon) is indicated. Fluid and electrolyte replacement help to prevent dehydration and shock. Use of corticosteroids may be indicated to suppress the inflammatory reaction in the colon if megacolon has resulted from active inflammatory bowel disease. Antibiotics may be given to prevent sepsis. [2]
Prognosis
If the condition does not improve, there is a significant risk of death. In case of poor response to conservative therapy a colectomy is usually required. This may involve all or part of the colon being removed, with the resulting option of anastomosis or ileostomy. Ileostomy carries far less risk of infection and post-operative complications because the risk of deterioration of sutures within the intestinal tract (as a result of anastomosis) is not present. The risk of death and shock has been reported to be lower in children, however most children required colectomy in one case-control study [3].
Complications
- Sepsis
- Shock
- Perforation of the colon [4]
Emergency action may be required if severe abdominal pain develops -- particularly if it is accompanied by fever, rapid heart rate, tenderness when the abdomen is pressed, bloody diarrhea, frequent diarrhea, or painful bowel movements.
Colonoscopy is contra-indicated, as it may rupture the dilated colon, thus causing severe hemorrhage.
References
- ^ "Toxic megacolon" at Dorland's Medical Dictionary
- ^ Autenrieth DM, Baumgart DC (August 2011). "Toxic Megacolon". Inflammatory Bowel Diseases. doi:10.1002/ibd.21847. http://onlinelibrary.wiley.com/doi/10.1002/ibd.21847/abstract.
- ^ Benchimol EI, Turner D, Mann EH, Thomas KE, Oprah MND, Gomes T, McLernon RA, Griffiths AM. Toxic megacolon in children with inflammatory bowel disease: clinical and radiographic characteristics. American Journal of Gastroenterology 2008; 103(6):1524-1531.
- ^ Panos MZ, Wood MJ, Asquith P (December 1993). "Toxic megacolon: the knee-elbow position relieves bowel distension". Gut 34 (12): 1726–7. doi:10.1136/gut.34.12.1726. PMC 1374472. PMID 8282262. http://gut.bmj.com/cgi/pmidlookup?view=long&pmid=8282262.
External links
- Toxic megacolon. National Institutes of Health. Used as the public domain source for this article. Update on 1/26/2004 by: Sreeni Jonnalagadda, M.D., Interventional and Pancreatobiliary Endoscopy, Washington University School of Medicine, St. Louis, MO. Review provided by VeriMed Healthcare Network.
Categories:- Diseases of intestines
- Colon (anatomy)
Wikimedia Foundation. 2010.