- Primary sclerosing cholangitis
-
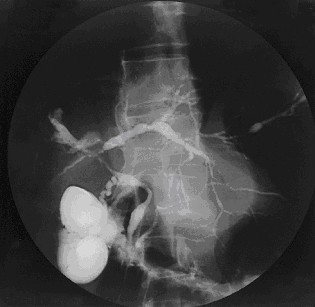
Primary sclerosing cholangitis Classification and external resources 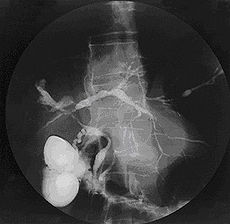
Cholangiogram of primary sclerosing cholangitis.ICD-10 K83.0 ICD-9 576.1 DiseasesDB 10643 MedlinePlus 000285 eMedicine med/3556 MeSH D015209 Primary sclerosing cholangitis (PSC) is a chronic liver disease caused by progressive inflammation and scarring of the bile ducts of the liver. The inflammation impedes the flow of bile to the gut, which can ultimately lead to liver cirrhosis, liver failure and liver cancer. The underlying cause of the inflammation is believed to be autoimmunity;[1] and more than 80% of those with PSC have ulcerative colitis.[2] The definitive treatment is liver transplantation.
Contents
Signs and symptoms
PSC is characterized by recurrent episodes of cholangitis, with progressive biliary scarring and obstruction.
- Chronic fatigue (a non-specific symptom often present in liver disease)
- Severe jaundice with intense itching
- Malabsorption (especially of fat) and steatorrhea (fatty stool) due to biliary obstruction, leading to decreased levels of the fat-soluble vitamins, A, D, E and K.
- Signs of cirrhosis
- Hepatomegaly
- Portal hypertension
- Ascending cholangitis, or infection of the bile duct.
- Dark urine due to excess conjugated bilirubin, which is water soluble, being excreted by the kidneys
- Hepatic encephalopathy
Diagnosis
The diagnosis is by imaging of the bile duct, usually in the setting of endoscopic retrograde cholangiopancreatography (ERCP, endoscopy of the bile duct and pancreas), which shows "beading" (both strictures and dilation) of the intrahepatic and extrahepatic bile ducts. Another option is magnetic resonance cholangiopancreatography (MRCP), where magnetic resonance imaging is used to visualise the biliary tract.
Most patients with PSC have evidence of autoantibodies. Approximately 80% of patients have perinuclear anti-neutrophil cytoplasmic antibodies, also called p-ANCA; however, this finding is not specific for PSC. Antinuclear antibodies and anti-smooth muscle antibody are found in 20%-50% of PSC patients and, likewise, are not specific for the disease.[1]
Other tests often done are a full blood count, liver enzymes, bilirubin levels (usually grossly elevated), renal function, electrolytes. Fecal fat determination is occasionally ordered when the symptoms of malabsorption are prominent.
The differential diagnosis can include primary biliary cirrhosis, drug induced cholestasis, cholangiocarcinoma, and HIV-associated cholangiopathy.
Etiology
The cause of PSC is unknown, although it is thought to be an autoimmune disorder. There is an increased prevalence of HLA alleles A1, B8, and DR3 in primary sclerosing cholangitis.[1]
Pathophysiology
Inflammation damages bile ducts both inside and outside of the liver. The resulting scarring of the bile ducts blocks the flow of bile, causing cholestasis. Bile stasis and back-pressure induces proliferation of epithelial cells and focal destruction of the liver parenchyma, forming bile lakes. Chronic biliary obstruction causes portal tract fibrosis and ultimately biliary cirrhosis and liver failure.[3]
Bile assists in the enteric breakdown and absorption of fat; the absence of bile leads to fat malabsorption and deficiencies of fat-soluble vitamins (A, D, E, K).Epidemiology
There is a 2:1 male-to-female predilection of primary sclerosing cholangitis.[3] The disease normally starts from age 20 to 30, though may begin in childhood. PSC progresses slowly, so the disease can be active for a long time before it is noticed or diagnosed. There is relatively little data on the prevalence and incidence of primary sclerosing cholangitis, with studies in different countries showing annual incidence of 0.068–1.3 per 100,000 people and prevalence 0.22–8.5 per 100,000; given that PSC is closely linked with ulcerative colitis, it is likely that the risk is higher in populations where UC is more common.[4]
Related diseases
Primary sclerosing cholangitis is associated with cholangiocarcinoma, a cancer of the biliary tree, and the lifetime risk for PSC sufferers is 10-15%. Screening for cholangiocarcinoma in patients with primary sclerosing cholangitis is encouraged, but there is no general consensus on the modality and interval of choice.
Colon cancer is also associated with PSC.
PSC has a significant association with ulcerative colitis, an inflammatory bowel disease primarily affecting the large intestine. As many as 5% of patients with ulcerative colitis may progress to develop primary sclerosing cholangitis [5] and approximately 70% of people with primary sclerosing cholangitis have ulcerative colitis.[3]
Therapy
Standard treatment includes ursodiol, a bile acid naturally produced by the liver, which has been shown to lower elevated liver enzyme numbers in people with PSC, but has not improved liver- or overall survival.[6] Treatment also includes medication to relieve itching (antipruritics), bile acid sequestrants (cholestyramine), antibiotics to treat infections, and vitamin supplements, as people with PSC are often deficient in vitamin A, vitamin D, vitamin E and vitamin K.
In some cases, ERCP, which may involve stenting of the common bile duct, may be necessary in order to open major blockages (dominant strictures).
Liver transplantation is the only proven long-term treatment of PSC. Indications for transplantation include recurrent bacterial cholangitis, jaundice refractory to medical and endoscopic treatment, decompensated cirrhosis and complications of portal hypertension. In one series, 1, 2, and 5 year survival following liver transplantation for PSC was 90%, 86% and 85% respectively.[1]
Prognosis
A German study in 2007 estimated the average survival time from time of diagnosis to be approximately 25 years, and the median time until either death or liver transplantation to be approximately 10 years.[7]
See also
- Bilirubin
- Child-Pugh score
- Cholangiocarcinoma
- Liver function tests
- Primary biliary cirrhosis
- Alagille syndrome
- Progressive familial intrahepatic cholestasis
- Walter Payton (died of primary sclerosing cholangitis)
- Chris LeDoux (professional rodeo rider and country musician with PSC who died of cholangiocarcinoma)
- Chris Klug (professional snowboarder with PSC who had liver transplant)
References
- ^ a b c d Charatcharoenwitthaya P, Lindor KD (Feb 2006). "Primary sclerosing cholangitis: diagnosis and management". Current Gastroenterology Reports 8 (1): 75–82. doi:10.1007/s11894-006-0067-8. PMID 16510038.
- ^ Sleisenger, MH (2006). Sleisenger and Fordtran's gastrointestinal and liver disease: pathophysiology, diagnosis, management (8th Edition ed.). Philadelphia: Saunders.
- ^ a b c Robbins SL, Kumar V, Cotran RS (2003). "Chapter 16". Robbins basic pathology (7th ed.). Philadelphia: Saunders. pp. 620–1. ISBN 0-7216-9274-5.
- ^ Feld JJ, Heathcote EJ (October 2003). "Epidemiology of autoimmune liver disease". J. Gastroenterol. Hepatol. 18 (10): 1118–28. doi:10.1046/j.1440-1746.2003.03165.x. PMID 12974897. http://onlinelibrary.wiley.com/doi/10.1046/j.1440-1746.2003.03165.x/full.
- ^ Olsson R, Danielsson A, Järnerot G, et al. (1991). "Prevalence of primary sclerosing cholangitis in patients with ulcerative colitis". Gastroenterology 100 (5 Pt 1): 1319–23. PMID 2013375.
- ^ Lindor KD, Kowdley KV, Luketic VA, Harrison ME, McCashland T, Befeler AS, Harnois D, Jorgensen R, Petz J, Keach J, Mooney J, Sargeant C, Braaten J, Bernard T, King D, Miceli E, Schmoll J, Hoskin T, Thapa P, Enders F (Sep 2009). "High-dose ursodeoxycholic acid for the treatment of primary sclerosing cholangitis.". Hepatology 50 (3): 671–3. doi:10.1002/hep.23082. PMC 2758780. PMID 19585548. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2758780.
- ^ Tischendorf, J.; Hecker, H.; Krüger, M.; Manns, M.; Meier, P. (2007). "Characterization, outcome, and prognosis in 273 patients with primary sclerosing cholangitis: A single center study". The American journal of gastroenterology 102 (1): 107–114. doi:10.1111/j.1572-0241.2006.00872.x. PMID 17037993. [1]. Giving survival time: 306 months
External links
- PSC Partners: Patient organization with additional information
- PSC Support : UK based Patient organization with additional information and discussion forum
- Additional Literature about PSC
- Information from The Morgan Foundation for the Study of PSC
Categories:- Autoimmune diseases
- Biliary tract disorders
- Hepatology
- Inflammations
Wikimedia Foundation. 2010.