- Subdural hematoma
Infobox_Disease
Name = PAGENAME
Caption =
DiseasesDB = 12614
ICD10 = ICD10|I|61|0|i|60, ICD10|S|06|5|s|00
ICD9 = ICD9|852.2 - traumatic; ICD9|432.1 - nontraumatic
ICDO =
OMIM =
MedlinePlus = 000713
eMedicineSubj = neuro
eMedicineTopic = 575
MeshID = D006408
A subduralhematoma (Subdural haematoma) (SDH) is a form oftraumatic brain injury in whichblood gathers between the dura (the outer protective covering of thebrain ) and the arachnoid (the middle layer of themeninges ). Unlike inepidural hematomas , which are usually caused by tears in arteries, subdural bleeding usually results from tears in veins that cross thesubdural space . This bleeding often separates the dura and the arachnoid layers. Subdural hemorrhages may cause an increase inintracranial pressure (ICP), which can cause compression of and damage to delicate brain tissue. Acute subdural hematoma (ASDH) has a high mortality rate and is a severemedical emergency . "
=Causes= Subdural hematomas are most often caused byhead injury , when fast changing velocities within theskull may stretch and tear small bridgingvein s. Subdural hematomas due to head injury are described as traumatic. Much more common thanepidural hemorrhage s, subdural hemorrhages generally result from shearing injuries due to various rotational or linear forces.University of Vermont College of Medicine. [http://web.archive.org/web/20030821142023/http://cats.med.uvm.edu/cats_teachingmod/pathology/path302/np/home/neuroindex.html "Neuropathology: Trauma to the CNS."] Accessed through web archive onAugust 8 ,2007 . ] Wagner AL. 2004. [http://www.emedicine.com/radio/topic664.htm "Subdural hematoma."] Emedicine.com. Retrieved onAugust 8 ,2007 . ] It is also commonly seen in the elderly and in alcoholics, who have evidence of brain atrophy. Cerebral atrophy increases the length the bridging veins have to traverse between the two meningeal layers, hence increasing the likelihood of shearing forces causing a tear. It is also more common in patients on anticoagulants, esp Aspirin and Warfarin. Patients on these medications can have a subdural hematoma with a minor injury.igns and symptoms
Symptoms of subdural hemorrhage have a slower onset than those of
epidural hemorrhage s because the lower pressure veins bleed more slowly than arteries. Thus, signs and symptoms may show up within 24 hours but can be delayed as much as 2 weeks.Sanders MJ and McKenna K. 2001. "Mosby’s Paramedic Textbook", 2nd revised Ed. Chapter 22, "Head and facial trauma." Mosby.] If the bleeds are large enough to put pressure on the brain, signs of increased ICP or damage to part of the brain will be present. (Dr.Gill Mohinder MD) Othersigns andsymptom s of subdural hematoma include the following:
* A history of recenthead injury
* Loss ofconsciousness or fluctuating levels of consciousness
* Irritability
*Seizures
*Numbness
*Headache (either constant or fluctuating)
*Dizziness
*Disorientation
*Amnesia
* Weakness orlethargy
*Nausea or vomiting
* Personality changes
* Inability to speak or slurred speech
*Ataxia , or difficulty walking
* Altered breathing patterns
* Blurred Vision
*Deviated gaze , or abnormal movement of the eyes.Features
Most of the time, subdural hematomas occur around the tops and sides of the frontal and
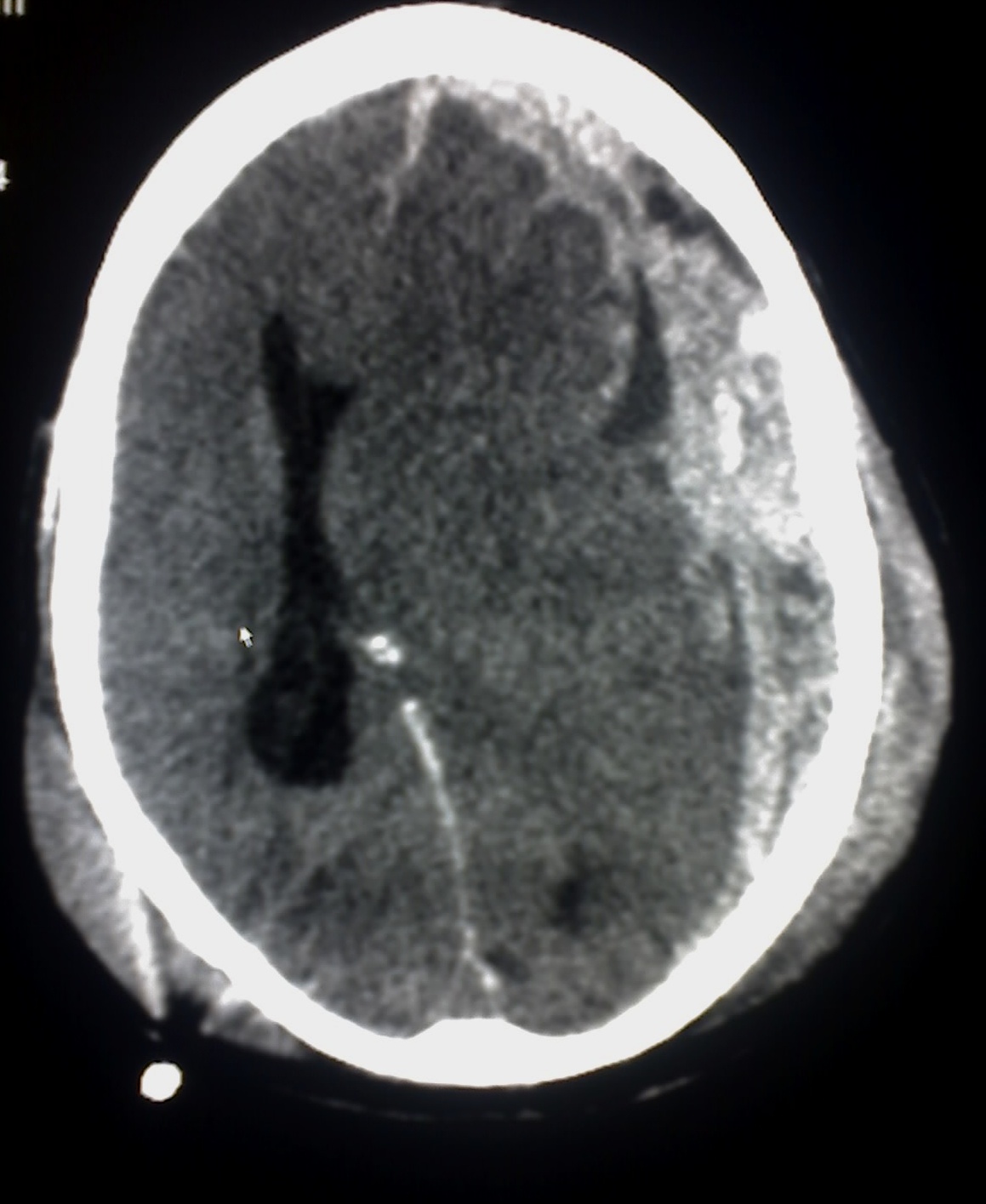
parietal lobe s. They also occur in the posteriorfossa , and near thefalx cerebri andtentorium . Unlikeepidural hematoma s, which cannot expand past the sutures of the skull, subdural hematomas can expand along the inside of the skull, creating a convex shape that follows the curve of the brain, stopping only at thedural reflection s like the tentorium and falx cerebri.On a
CT scan , subdural hematomas are crescent-shaped, with a concave surface away from the skull. Subdural blood can also be seen as a layering density along thetentorium cerebelli . This can be a chronic, stable process, since the feeding system is low-pressure. In such cases, subtle signs of bleeding such as effacement of sulci or medial displacement of the junction betweengray matter andwhite matter may be apparent. A chronic bleed can be the same density as brain tissue (calledisodense to brain), meaning that it will show up on CT scan as the same shade as brain tissue, potentially obscuring the finding.ubtypes
Subdural hematomas are divided into acute, subacute, and chronic, depending on their speed of onset. Acute subdural hematomas that are due to trauma are the most lethal of all head injuries and have a high
mortality rate if they are not rapidly treated with surgical decompression.Acute bleeds develop after high speed acceleration or deceleration injuries and are increasingly severe with larger hematomas. They are most severe if associated with
cerebral contusion s. Though much faster than chronic subdural bleeds, acute subdural bleeding is usually venous and therefore slower than the usually arterial bleeding of anepidural hemorrhage . Acute subdural bleeds have a high mortality rate, higher even than epidural hematomas and diffuse brain injuries, because the velocities necessary to cause them cause other severe injuries as well. [Vinas F.C. and Pilitsis J. 2006. [http://www.emedicine.com/med/topic2888.htm Penetrating Head Trauma] . Emedicine.com.] The mortality rate associated with acute subdural hematoma is around 60 to 80% [Dawodu S. 2004. [http://www.emedicine.com/pmr/topic212.htm "Traumatic brain injury: Definition, epidemiology, pathophysiology"] Emedicine.com. Retrieved onAugust 7 ,2007 .]Chronic subdural bleeds develop over the period of days to weeks, often after minor head trauma, though such a cause is not identifiable in 50% of patients.Downie A. 2001. [http://www.radiology.co.uk/srs-x/tutors/cttrauma/tutor.htm "Tutorial: CT in head trauma"] . Retrieved on
August 7 ,2007 .] They may not be discovered until they present clinically months or years after a head injury.cite journal |author=Kushner D |title=Mild Traumatic Brain Injury: Toward Understanding Manifestations and Treatment |journal=Archives of Internal Medicine |volume=158 |issue=15 |pages=1617–1624 |year=1998 |pmid=9701095 |doi= |url=http://archinte.highwire.org/cgi/content/full/158/15/1617] The bleeding from a chronic bleed is slow, probably from repeated minor bleeds, and usually stops by itself.Graham DI and Gennareli TA. Chapter 5, "Pathology of brain damage after head injury" Cooper P and Golfinos G. 2000. "Head Injury", 4th Ed. Morgan Hill, New York. ] Since these bleeds progress slowly, they present the chance to be stopped before they cause significant damage. Small subdural hematomas, those less than a centimeter wide, have much better outcomes than acute subdural bleeds: in one study, only 22% of patients with chronic subdural bleeds had outcomes worse than "good" or "complete recovery". Chronic subdural hematomas are common in the elderly.Pathophysiology
Collected blood from the subdural bleed may draw in water due to
osmosis , causing it to expand, which may compress brain tissue and cause new bleeds by tearing other blood vessels. The collected blood may even develop its own membrane. [McCaffrey P. 2001. [http://www.csuchico.edu/~pmccaff/syllabi/SPPA336/336unit11.html "The neuroscience on the web series: CMSD 336 neuropathologies of language and cognition."] California State University, Chico. Retrieved onAugust 7 ,2007 . ]In some subdural bleeds, the
arachnoid layer of themeninges is torn, andcerebrospinal fluid (CSF) and blood both expand in theintracranial space , increasing pressure.Substances that cause vasoconstriction may be released from the collected material in a subdural hematoma, causing further
ischemia under the site by restricting blood flow to the brain. When the brain is denied adequate blood flow, abiochemical cascade known as theischemic cascade is unleashed, and may ultimately lead to brain cell death.The body gradually reabsorbs the clot and replaces it with granulation tissue.
Treatment
It is important that a patient receive medical assessment, including a complete neurological examination, after any head trauma. A
CT scan orMRI scan will usually detect significant subdural hematomas.Treatment of a subdural hematoma depends on its size and rate of growth. Small subdural hematomas can be managed by careful monitoring until the body heals itself. Large or symptomatic hematomas require a
craniotomy , the surgical opening of theskull . A surgeon then opens thedura , removes theblood clot with suction or irrigation, and identifies and controls sites ofbleeding . Postoperative complications include increasedintracranial pressure , brainedema , new or recurrentbleeding ,infection , andseizure . The artery must be repaired.Risk factors
Factors increasing the risk of a subdural hematoma include very young or very old age. As the brain shrinks with age, the
subdural space enlarges and thevein s that traverse the space must travel over a wider distance, making them more vulnerable to tears. This and the fact that the elderly have more brittle veins make chronic subdural bleeds more common in older patients. Infants, too, have larger subdural spaces and are more predisposed to subdural bleeds than are young adults. For this reason, subdural hematoma is a common finding inshaken baby syndrome . In juveniles, anarachnoid cyst is a risk factor for a subdural hematoma. [cite journal |author=Mori K, Yamamoto T, Horinaka N, Maeda M |title=Arachnoid cyst is a risk factor for chronic subdural hematoma in juveniles: twelve cases of chronic subdural hematoma associated with arachnoid cyst |journal=J. Neurotrauma |volume=19 |issue=9 |pages=1017–27 |year=2002 |pmid=12482115 |doi=10.1089/089771502760341938]Other risk factors for subdural bleeds include taking blood thinners (
anticoagulant s), long-term alcohol abuse, anddementia .ee also
*
Head injury
*Traumatic brain injury
*Intra-axial hemorrhage
*Extra-axial hemorrhage
*Epidural hematoma
*Subarachnoid hematoma
*Concussion
*Diffuse axonal injury References
Wikimedia Foundation. 2010.