- Placebo
-
For other uses, see Placebo (disambiguation) and Placebo effect (disambiguation)."Sugar pill" redirects here. For Kids of 88 album, see Sugarpills.

 The placebo effect can be produced by inert tablets, by sham surgery, and by false information, such as when electrical stimulation is turned "off" in those with Parkinson's disease implanted brain electrodes.[1]
The placebo effect can be produced by inert tablets, by sham surgery, and by false information, such as when electrical stimulation is turned "off" in those with Parkinson's disease implanted brain electrodes.[1]A placebo (
 /pləˈsiboʊ/; Latin: I shall please[2]) is a sham or simulated medical intervention. Sometimes patients given a placebo treatment will have a perceived or actual improvement in a medical condition, a phenomenon commonly called the placebo effect.
/pləˈsiboʊ/; Latin: I shall please[2]) is a sham or simulated medical intervention. Sometimes patients given a placebo treatment will have a perceived or actual improvement in a medical condition, a phenomenon commonly called the placebo effect.In medical research, placebos are given as control treatments and depend on the use of measured deception. Common placebos are inert tablets, sham surgery,[3] and other procedures based on false information.[1] However, placebos can also have a surprisingly positive effect on a patient who knows that the given treatment is without any active drug, as compared with a control group who knowingly did not get a placebo.[4]
In one common placebo procedure, however, a patient is given an inert pill, told that it may improve his/her condition, but not told that it is in fact inert. Such an intervention may cause the patient to believe the treatment will change his/her condition; and this belief may produce a subjective perception of a therapeutic effect, causing the patient to feel their condition has improved — or an actual improvement in their condition. This phenomenon is known as the placebo effect.
Placebos are widely used in medical research and medicine,[5] and the placebo effect is a pervasive phenomenon;[5] in fact, it is part of the response to any active medical intervention.[6] The placebo effect points to the importance of perception and the brain's role in physical health. However, when used as treatment in clinical medicine (as opposed to laboratory research), the deception involved in the use of placebos creates tension between the Hippocratic Oath and the honesty of the doctor-patient relationship.[7] The United Kingdom Parliamentary Committee on Science and Technology has stated that: "...prescribing placebos... usually relies on some degree of patient deception" and "prescribing pure placebos is bad medicine. Their effect is unreliable and unpredictable and cannot form the sole basis of any treatment on the NHS."[3]
Since the publication of Henry K. Beecher's The Powerful Placebo in 1955, the phenomenon has been considered to have clinically important effects.[8] This view was notably challenged when, in 2001, a systematic review of clinical trials concluded that there was no evidence of clinically important effects, except perhaps in the treatment of pain and continuous subjective outcomes.[8] The article received a flurry of criticism,[9] but the authors later published a Cochrane review with similar conclusions (updated as of 2010[update]).[10] Most studies have attributed the difference from baseline till the end of the trial to a placebo effect, but the reviewers examined studies which had both placebo and untreated groups in order to distinguish the placebo effect from the natural progression of the disease.[8] However these conclusions have been criticized because of the great variety of diseases - more than 40 - in this metastudy. The effect of placebo is very different in different diseases. By pooling quite different diseases the results can be levelled out.
Contents
Definitions, effects, and ethics
See also: Medical ethicsA placebo has been defined as "a substance or procedure… that is objectively without specific activity for the condition being treated".[9] Under this definition, a wide variety of things can be placebos and exhibit a placebo effect. Pharmacological substances administered through any means can act as placebos, including pills, creams, inhalants, and injections. Medical devices such as ultrasound can act as placebos.[11][12] Sham surgery,[13][14][15] sham electrodes implanted in the brain,[1] and sham acupuncture, either with sham needles or on fake acupuncture points, have all exhibited placebo effects.[16] Bedding not treated to reduce allergies has been used as a placebo to control for treated bedding.[17] The physician has even been called a placebo;[18]33–34 a study found that patient recovery can be increased by words that suggest the patient “would be better in a few days”, and if the patient is given treatment, that “the treatment would certainly make him better” rather than negative words such as “I am not sure that the treatment I am going to give you will have an effect”.[19] The placebo effect may be a component of pharmacological therapies: Pain killing and anxiety reducing drugs that are infused secretly without an individual’s knowledge are less effective than when a patient knows they are receiving them. Likewise, the effects of stimulation from implanted electrodes in the brains of those with advanced Parkinson's disease are greater when they are aware they are receiving this stimulation.[20] Sometimes administering or prescribing a placebo merges into fake medicine.
The placebo effect has sometimes been defined as a physiological effect caused by the placebo, but Moerman and Jonas have pointed out that this seems illogical, as a placebo is an inert substance that does not directly cause anything. Instead they introduced the word "meaning response" for the meaning that the brain associates with the placebo, which causes a physiological placebo effect. They propose that the placebo, which may be unethical, could be avoided entirely if doctors comfort and encourage their patients' health.[9] Ernst and Resch also attempted to distinguish between the "true" and "perceived" placebo effect, as they argued that some of the effects attributed to the placebo effect could be due to other factors.[21]
The placebo effect has been controversial throughout history. Notable medical organizations have endorsed it,[22] but in 1903 Richard Cabot concluded that it should be avoided because it is deceptive. Newman[23] points out the "placebo paradox", – it may be unethical to use a placebo, but also unethical "not to use something that heals". He suggests to solve this dilemma by appropriating the meaning response in medicine, that is make use of the placebo effect, as long as the "one administering… is honest, open, and believes in its potential healing power".[7] Another possible resolution of the ethical dilemma might come from the "honest placebo" effect found in a 2010 study[4] carried out by researchers in the Program in Placebo Studies at the Harvard Medical School, where patients with irritable bowel syndrome experienced a significant beneficial effect even though they were told the pills they were taking were placebos, as compared to a control group who received no pills.
History
Main article: Placebo in historyThe word 'placebo', Latin for "I will please", dates back to a Latin translation of the Bible by Jerome.[24] It was first used in a medicinal context in the 18th century. In 1785 it was defined as a "commonplace method or medicine" and in 1811 it was defined as "any medicine adapted more to please than to benefit the patient", sometimes with a derogatory implication[25] but not with the implication of no effect.[26] Placebos were widespread in medicine until the 20th century, and they were sometimes endorsed as necessary deceptions.[22] In 1903 Richard Cabot said that he was brought up to use placebos,[22] but he ultimately concluded by saying that "I have not yet found any case in which a lie does not do more harm than good".[7] In 1961 Henry K. Beecher found[27] that surgeons he categorized as enthusiasts relieved their patients' chest pain and heart problems more than skeptic surgeons.[7] In 1961 Walter Kennedy introduced the word nocebo.[22] Beginning in the 1960s, the placebo effect became widely recognized and placebo controlled trials became the norm in the approval of new medications.[28] Later, researchers became interested in understanding the placebo effect, rather than just controlling for its effects, and in 2011, a Program in Placebo Studies was established at the Harvard Medical School.
Mechanism of the effect
The phenomenon of an inert substance's resulting in a patient's medical improvement is called the placebo effect. The phenomenon is related to the perception and expectation that the patient has; if the substance is viewed as helpful, it can heal, but, if it is viewed as harmful, it can cause negative effects, which is known as the nocebo effect. The basic mechanisms of placebo effects have been investigated since 1978, when it was found that the opioid antagonist naloxone could block placebo painkillers, suggesting that endogenous opioids are involved.[29]
Expectancy and conditioning
In 1985, Irving Kirsch hypothesized that placebo effects are produced by the self-fulfilling effects of response expectancies, in which the belief that one will feel different leads a person to actually feel different.[30] According to this theory, the belief that one has received an active treatment can produce the subjective changes thought to be produced by the real treatment. Placebos can act similarly through classical conditioning, wherein a placebo and an actual stimulus are used simultaneously until the placebo is associated with the effect from the actual stimulus.[31] Both conditioning and expectations play a role in placebo effect,[32] and make different kinds of contribution. Conditioning has a longer-lasting effect,[33] and can affect earlier stages of information processing.[34] The expectancy effect can be enhanced through factors such as the enthusiasm of the doctor, differences in size and color of placebo pills, or the use of other interventions such as injections. In one study, the response to a placebo increased from 44% to 62% when the doctor treated them with "warmth, attention, and confidence".[35] Expectancy effects have been found to occur with a range of substances. Those that think that a treatment will work display a stronger placebo effect than those that do not, as evidenced by a study of acupuncture.[36][37]
Because the placebo effect is based upon expectations and conditioning, the effect disappears if the patient is told that their expectations are unrealistic, or that the placebo intervention is ineffective. A conditioned pain reduction can be totally removed when its existence is explained.[38] It has also been reported of subjects given placebos in a trial of anti-depressants, that "Once the trial was over and the patients who had been given placebos were told as much, they quickly deteriorated."[39]
A placebo described as a muscle relaxant will cause muscle relaxation and, if described as the opposite, muscle tension.[40] A placebo presented as a stimulant will have this effect on heart rhythm, and blood pressure, but, when administered as a depressant, the opposite effect.[41] The perceived consumption of caffeine has been reported to cause similar effects even when decaffeinated coffee is consumed,[42] [43] although a 2003 study found only limited support for this.[44] Alcohol placebos can cause intoxication[45] and sensorimotor impairment.[46] Perceived ergogenic aids can increase endurance,[47] speed[48] and weight-lifting ability,[49] leading to the question of whether placebos should be allowed in sport competition.[50] Placebos can help smokers quit.[51] Perceived allergens that are not truly allergenic can cause allergies.[52] Interventions such as psychotherapy can have placebo effects.[53]pp 164–173 The effect has been observed in the transplantation of human embryonic neurons into the brains of those with advanced Parkinson's disease.[54]
Because placebos are dependent upon perception and expectation, various factors that change the perception can increase the magnitude of the placebo response. For example, studies have found that the color and size of the placebo pill makes a difference, with "hot-colored" pills working better as stimulants while "cool-colored" pills work better as depressants. Capsules rather than tablets seem to be more effective, and size can make a difference.[55] One researcher has found that big pills increase the effect[56] while another has argued that the effect is dependent upon cultural background.[57] More pills,[58] branding,[59] past experience,[60] and high price[61] increase the effect of placebo pills. Injection[62] and acupuncture[16] have larger effect than pills. Proper adherence to placebos is associated with decreased mortality.[63]
Motivation may contribute to the placebo effect. The active goals of an individual changes his/her somatic experience by altering the detection and interpretation of expectation-congruent symptoms, and by changing the behavioral strategies a person pursues.[64][65] Motivation may link to the meaning through which people experience illness and treatment. Such meaning is derived from the culture in which they live and which informs them about the nature of illness and how it responds to treatment. Research upon the placebo treatment of gastric and duodenal ulcers shows that this varies widely with society: those in Germany having a high-rate placebo effect while those in Brazil a low one.[9] Placebo effects in treating gastric ulcers is low in Brazil, higher in northern Europe (Denmark, Netherlands), and extremely high in Germany. But the placebo effect for hypertension is lower in Germany than elsewhere[66] Social observation can induce a placebo effect such when a person sees another having reduced pain following what they believe is a pain reducing procedure.[67]
The placebo effect can work selectively. If an analgesic placebo cream is applied on one hand, it will reduce pain only in that hand and not elsewhere on the body[68] If a person is given a placebo under one name, and they respond, they will respond in the same way on a later occasion to that placebo under that name but not if under another.[69]
Placebo effect and the brain
Functional imaging upon placebo analgesia shows that it links to the activation, and increased functional correlation between this activation, in the anterior cingulate, prefrontal, orbitofrontal and insular cortices, nucleus accumbens, amygdala, the brainstem periaqueductal gray matter,[70][71][72] and the spinal cord.[73][74][75][76]
These changes can act upon the brain’s early stages of information processing: Research using evoked brain potentials upon painful laser pulses, for example, finds placebo effects upon the N2–P2, a biphasic negative–positive complex response, the N2 peak of which is at about 230 ms, and the P2 one at about 380 ms.[34] They occur not only during placebo analgesia but after receiving the analgesic placebo (the areas are different here, and involve the medial prefrontal cortex, posterior parietal cortex and inferior parietal lobule).[77]
Different areas in the higher brain have different functions. The prefrontal involvement could be related to recalling the placebo and maintaining its cognitive presence in a "self-reinforcing feedback loop" (during pain an individual recalls having taken the placebo and reduced pain reinforces its status as an analgesic).[78] The rostral anterior cingulate cortex (rACC) and its subcortical connectivity could be related to the expectation of potential pain stimuli[79][80]
The higher brain works by regulating subcortical processes. High placebo responses link with enhanced dopamine and mu-opioid activity in the circuitry for reward responses and motivated behavior of the nucleus accumbens, and, on the converse, anti-analgesic nocebos responses were associated with deactivation in this part of the brain of dopamine and opioid release.[71] (It has been known that placebo analgesia depends upon the release in the brain of endogenous opioids since 1978.[81]) Such analgesic placebos activation changes processing lower down in the brain by enhancing the descending inhibition through the periaqueductal gray[71] on spinal nociceptive reflexes, while the expectations of anti-analgesic nocebos acts in the opposite way to block this.[73]
The brain is also involved in less-studied ways upon nonanalgesic placebo effects:
- Parkinson's disease: Placebo relief is associated with the release of dopamine in the brain.[82]
- Depression: Placebos reducing depression affect many of the same areas that are activated by antidepressants with the addition of the prefrontal cortex[83][84]
- Caffeine: Placebo-caffeinated coffee causes an increase in bilateral dopamine release in the thalamus.[85]
- Glucose: The expectation of an intravenous injection of glucose increases the release of dopamine in the basal ganglia of men (but not women).[86]
- Methylphenidate: The expectation of intravenous injection of this drug in inexperienced drug users increased the release of dopamine in the ventral cingulate gyrus and nucleus accumbens, with this effect being largest in those with no prior experience of the drug.[87]
Present functional imaging upon placebo analgesia has been summarized as showing that the placebo response is "mediated by "top-down" processes dependent on frontal cortical areas that generate and maintain cognitive expectancies. Dopaminergic reward pathways may underlie these expectancies".[88] "Diseases lacking major 'top-down' or cortically based regulation may be less prone to placebo-related improvement".[89]
Brain and body
For more details on this topic, see neural top down control of physiology.The brain has control over the body processes affected by placebos. Pain, motor fatigue, and fever are directly organized by the brain. Other processes usually regulated by the body such as the immune system are also controlled indirectly through the sympathetic and parasympathetic nervous system.
Research upon conditioning in animals shows the brain can learn control over them. In conditioning, a neutral stimulus saccharin is paired in a drink with an agent that produces an unconditioned response. For example, that agent might be cyclophosphamide that causes immunosuppression. After learning this pairing, the taste of saccharin by itself through neural top-down control created immunosuppression, as a new conditioned response.[90] Such conditioning has been found to affect a diverse variety of not just basic physiological processes in the immune system but ones such as serum iron levels, oxidative DNA damage levels, and insulin secretion. This work was originally done on rats, however the same conditioning of basic physiological processes can also occur in humans. Recent reviews have argued the placebo effect is due to top-down control by the brain for immunity[91] and pain.[92] Pacheco-López and colleagues have raised the possibility of "neocortical-sympathetic-immune axis providing neuroanatomical substrates that might explain the link between placebo/conditioned and placebo/expectation responses."[91]pp 441
A recent fMRI study has shown that a placebo can reduce pain-related neural activity in the spinal cord, indicating that placebo effects can extend beyond the brain.[93]
Evolved health regulation
Evolutionary medicine identifies many symptoms such as fever, pain, and sickness behavior as evolved responses to protect or enhance the recovery from infection and injury. Fever, for example, is an evolved self-treatment that removes bacteria or viruses through raised body temperature. These evolved responses, however, also have a cost that depending upon circumstances can outweigh their benefit (due to this, for example, there is a reduction in fever during malnutrition or late pregnancy). According to the health management system theory proposed by Nicholas Humphrey, the brain has been selected to ensure that evolved responses are deployed only when the cost benefit is biologically advantageous. To do this, the brain factors in a variety of information sources, including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses. One such source of information is the knowledge the body is receiving care and treatment. The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it selects not to deploy an evolved self-treatment.[94]
Clinical utility
Duration
Placebo effects can last for a long time: over 8 weeks for panic disorder,[95] 6 months for angina pectoris,[96] and two and half years for rheumatoid arthritis.[97] Placebo effects after verbal suggestion for mild pain can be robust and still exist after being repeated ten times even if they have no actual pharmacological pain killing action.[38]
Clinical significance
Hróbjartsson and Peter Gøtzsche published a study in 2001[8] and a follow-up study in 2004[98] questioning the nature of the placebo effect. The studies were performed as two meta-analyses. They found that in studies with a binary outcome, meaning patients were classified as improved or not improved, the placebo group had no statistically significant improvement over the no-treatment group. Likewise, there was no significant placebo effect in studies in which objective outcomes (such as blood pressure) were measured by an independent observer. The placebo effect could be documented only in studies in which the outcomes (improvement or failure to improve) were reported by the subjects themselves. The authors concluded that the placebo effect does not have "powerful clinical effects," (objective effects) and that patient-reported improvements (subjective effects) in pain were small and could not be clearly distinguished from reporting bias. Other researchers (Wampold et al.) re-analysed the same data from the 2001 meta-analysis and concluded that the placebo effects for objective symptom measures are comparable to placebo effects for subjective ones and that the placebo effect can exceed the effect of the active treatment by 20% for disorders amenable to the placebo effect,[99][100] a conclusion which Hróbjartsson & Gøtzsche described as "powerful spin".[101] Another group of researchers noted the dramatically different conclusions between these two sets of authors despite nearly identical meta-analytic results, and suggested that placebo effects are indeed significant but small in magnitude.[102]
Hróbjartsson and Gøtzsche's conclusion has been criticised on several grounds. Their meta-analysis covered studies into a highly mixed group of conditions: The placebo effect does occur with peripheral disease processes (such as hypertension, asthma, prostatic hyperplasia, anal fissure, bronchitis), though not for processes reflecting physical disease (such as venous leg ulcers, Crohn’s disease, urinary tract infection, and chronic heart failure).[103] Placebos also do not work as strongly in clinical trials because the subjects do not know whether they might be getting a real treatment or a sham one. Where studies are made of placebos in which people think they are receiving actual treatment (rather than merely its possibility) the placebo effect has been observed.[104] Other writers have argued that the placebo effect can be reliably demonstrated under appropriate conditions.[105]
In another update by Hróbjartsson & Gøtzsche, published as a 2010 Cochrane systematic review which confirms and modifies their previous work, over 200 trials investigating 60 clinical conditions were included. Placebo interventions were again not found to have important clinical effects in general but may influence patient-reported outcomes in some situations, especially pain and nausea, although it was "difficult to distinguish patient-reported effects of placebo from response bias". The pooled relative risk they calculated for placebo was 0.93 (effect of only 7%) but significant. Effects were also found for phobia and asthma but were uncertain due to high risk of bias. In other conditions involving three or more trials, there was no statistically significant effect for smoking, dementia, depression, obesity, hypertension, insomnia and anxiety, although confidence intervals were wide. Several clinical (physical placebos, patient-involved outcomes, falsely informing patients there was no placebo) and methodological (small sample size, explicit aim of studying the placebo effect) factors were associated with higher effects of placebo. Despite low effects in general and the risk of bias, the authors acknowledged that large effects of placebo interventions may occur in certain situations.[106]
Negative effects
Similar to the placebo effect, inert substances have the potential to cause negative effects via the "nocebo effect" (Latin nocebo = "I will harm"). In this effect, giving an inert substance has negative consequences.[107]
Another negative consequence is that placebos can cause side-effects associated with real treatment.[108] One example of this is with those that have already taken an opiate, can then show respiratory depression when given it again in the form of a placebo.[109]
Withdrawal symptoms can also occur after placebo treatment. This was found, for example, after the discontinuation of the Women's Health Initiative study of hormone replacement therapy for menopause. Women had been on placebo for an average of 5.7 years. Moderate or severe withdrawal symptoms were reported by 40.5% of those on placebo compared to 63.3% of those on hormone replacement.[110]
Doctor-patient relationship
A study of Danish general practitioners found that 48% had prescribed a placebo at least 10 times in the past year.[5] The most frequently prescribed placebos were antibiotics for viral infections, and vitamins for fatigue. Specialists and hospital-based physicians reported much lower rates of placebo use. A 2004 study in the British Medical Journal of physicians in Israel found that 60% used placebos in their medical practice, most commonly to "fend off" requests for unjustified medications or to calm a patient.[111] The accompanying editorial concluded, "We cannot afford to dispense with any treatment that works, even if we are not certain how it does."[112] Other researches have argued that open provision of placebos for treating ADHD in children can be effective in maintaining ADHD children on lower stimulant doses in the short term.[113]
Critics of the practice responded that it is unethical to prescribe treatments that do not work, and that telling a patient (as opposed to a research test subject) that a placebo is a real medication is deceptive and harms the doctor-patient relationship in the long run. Critics also argued that using placebos can delay the proper diagnosis and treatment of serious medical conditions.
The following impracticalities exist with placebos: (See the BMJ posted responses to Spiegel's editorial rapid response online section.[112])
- Roughly only 30% of the population seems susceptible to placebo effects, and it is not possible to determine ahead of time whether a placebo will work or not. (However the placebo effect is zero in studies of blood poisoning and up to 80% in studies of wound on the duodenum).
- Patients rightfully want immediate relief or improvement from their illness or symptoms. A non-placebo can often provide that, while a placebo might not.
- Legitimate doctors and pharmacists could open themselves up to charges of fraud since sugar pills would cost pennies or cents for a bottle, but the price for a "real" medication would have to be charged to avoid making the patient suspicious.
About 25% of physicians in both the Danish and Israeli studies used placebos as a diagnostic tool to determine if a patient's symptoms were real, or if the patient was malingering. Both the critics and defenders of the medical use of placebos agreed that this was unethical. The British Medical Journal editorial said, "That a patient gets pain relief from a placebo does not imply that the pain is not real or organic in origin...the use of the placebo for 'diagnosis' of whether or not pain is real is misguided."
The placebo administration may prove to be a useful treatment in some specific cases where recommended drugs cannot be used. For example, burn patients who are experiencing respiratory problems cannot often be prescribed opioid (morphine) or opioid derivatives (pethidine), as these can cause further respiratory depression. In such cases placebo injections (normal saline, etc.) are of use in providing real pain relief to burn patients if those not in delirium are told they are being given a powerful dose of painkiller.
Referring specifically to homeopathy, the House of Commons of the United Kingdom Science and Technology Committee has stated:
In the Committee’s view, homeopathy is a placebo treatment and the Government should have a policy on prescribing placebos. The Government is reluctant to address the appropriateness and ethics of prescribing placebos to patients, which usually relies on some degree of patient deception. Prescribing of placebos is not consistent with informed patient choice-which the Government claims is very important-as it means patients do not have all the information needed to make choice meaningful.
Beyond ethical issues and the integrity of the doctor-patient relationship, prescribing pure placebos is bad medicine. Their effect is unreliable and unpredictable and cannot form the sole basis of any treatment on the NHS.[3]A survey in the United States of more than 10,000 physicians came to the result that while 24% of physicians would prescribe a treatment that is a placebo simply because the patient wanted treatment, 58% would not, and for the remaining 18%, it would depend on the circumstances.[114]
The individual
Who is affected
Placebos do not work for everyone.[115][116] Henry K. Beecher, in a paper in 1955[117] suggested placebo effects occurred in about 35% of people. However, the response rate is wide, ranging from 0% up to nearly everyone. In a dental postoperative pain model, placebo analgesia occurred in 39%.[116] In research upon ischemic arm pain, placebo analgesia was found in 27%.[115] The placebo analgesia rate for cutaneous healing of left hand skin was 56%.[118]
Though not everyone responds to a placebo, neither does everyone respond to an active drug. The percentage of patients who reported relief following placebo (39%) is similar to the percentage following 4 mg (36%) and 6 mg (50%) of hidden morphine.[119]
Individual differences
In the 1950s, there was considerable research to find whether there was a specific personality to those that responded to placebos. The findings could not be replicated[120] and it is now thought to have no effect.[121]
The desire for relief from pain, "goal motivation", and how far pain is expected to be relieved increases placebo analgesia.[64] Another factor increasing the effectiveness of placebos is the degree to which a person attends to their symptoms, "somatic focus".[65] Individual variation in response to analgesic placebos has been linked to regional neurochemical differences in the internal affective state of the individuals experiencing pain.[122]
Those with Alzheimer’s disease lose the capacity to be influenced by placebos, and this is attributed to the loss of their prefrontal cortex dependent capacity to have expectations.[123]
Children seem to have greater response than adults to placebos.[124]
Genes
In social anxiety disorder (SAD) an inherited variant of the gene for tryptophan hydroxylase 2 (enzyme that synthesizes the neurotransmitter serotonin) is linked to reduced amygdala activity and greater susceptibility to the placebo effect.[125][126][127] The authors note "additional work is necessary to elucidate the generalizability of the findings".
Symptoms and conditions
The placebo effect occurs more strongly in some conditions than others. One study found placebo effects are most likely to be found with the peripheral aspects of disease processes, rather than processes that reflect physical disease.[103] Dylan Evans has suggested as another factor, that placebos work most strongly upon conditions such as pain, swelling, stomach ulcers, depression, and anxiety that have been linked with activation of the acute-phase response.[53]
Pain
Placebo analgesia is more likely to work the more severe the pain.[128] One study found that for postoperative pain following the extraction of the third molar, saline injected while telling the patient it was a powerful painkiller was as potent as a 6–8 mg dose of morphine.[119]
Most research reports average reduction for a group of people, but this can be lower (some people do not respond). In one study using injection of capsaicin below the skin found that this reduced group average pain compared to no placebo by ~46% to ~57%.[68] Another measure is the ability to endure pain. In one study, placebos increased this on average by about 3.5 minutes compared to just under 14 minutes without it.[129] The average strength of placebos upon pain on a visual analog scale is 2 out of 10 units.[121][130] Individuals who respond to placebos may show even greater effects up to 5 out of 10 units.[115]
Depression
In 1998, a meta-analysis of published antidepressant trials found that 75% of the effectiveness of anti-depressant medication is due to the placebo effect and other non-specific effects, rather than the treatment itself.[131] Later, meta-analyses including data from unpublished trials found that the overall difference between drug and placebo is not clinically significant except in cases of very extreme depression,[132][133] Another meta-analysis found that 79% of depressed patients receiving placebo remained well (for 12 weeks after an initial 6–8 weeks of successful therapy) compared to 93% of those receiving antidepressants.[134] A meta-analysis in 2002 found a 30% reduction in suicide and attempted suicide in the placebo groups compared to a 40% reduction in the treated groups.[135]
A 2002 article in The Washington Post titled "Against Depression, a Sugar Pill Is Hard to Beat" summarized research as follows: "In the majority of trials conducted by drug companies in recent decades, sugar pills have done as well as -- or better than -- antidepressants. Companies have had to conduct numerous trials to get two that show a positive result, which is the Food and Drug Administration's minimum for approval. The makers of Prozac had to run five trials to obtain two that were positive, and the makers of Paxil and Zoloft had to run even more”.[39]
Gastric and duodenal ulcers
A meta-study of 31 placebo-controlled trials of the gastric acid secretion inhibitor drug cimetidine in the treatment of gastric or duodenal ulcers found that placebo treatments, in many cases, were as effective as active drugs: of the 1692 patients treated in the 31 trials, 76% of the 916 treated with the drug were "healed", and 48% of the 776 treated with placebo were "healed".[9][136] These results were confirmed by the direct post-treatment endoscopy. It was also found that German placebos were "stronger" than others; and that, overall, different physicians evoked quite different placebo responses in the same clinical trial (p. 15). Moreover, in many of these trials the gap between the active drugs and the placebo controls was "not because [the trials' constituents] had high drug effectiveness, but because they had low placebo effectiveness" (p. 13).
In some trials, placebos were effective in 90% of the cases, whereas in others the placebos were effective in only 10% of the cases. It was argued that "what is demonstrated in [these] studies is not enhanced healing in drug groups but reduced healing in placebo groups" (p. 14). It was also noted the results of two studies (one conducted in Germany, the other in Denmark), which examined "ulcer relapse in healed patients" showed that the rate of relapse amongst those "healed" by the active drug treatment was five times that of those "healed" by the placebo treatment (pp. 14–15).
Chronic fatigue syndrome
It was previously assumed that placebo response rates in patients with chronic fatigue syndrome (CFS) are unusually high, "at least 30% to 50%", because of the subjective reporting of symptoms and the fluctuating nature of the condition. According to a meta-analysis and contrary to conventional wisdom, the pooled response rate in the placebo group was 19.6%, even lower than in some other medical conditions. The authors offer possible explanations for this result: CFS is widely understood to be difficult to treat, which could reduce expectations of improvement. In context of evidence showing placebos do not have powerful clinical effects when compared to no treatment, a low rate of spontaneous remission in CFS could contribute to reduced improvement rates in the placebo group. Intervention type also contributed to the heterogeneity of the response. Low patient and provider expectations regarding psychological treatment may explain particularly low placebo responses to psychiatric treatments.[137]
List of medical conditions
The effect of placebo treatments (an inert pill unless otherwise noted) has been studied for the following medical conditions:
Effects on research
Placebo-controlled studies
Main article: Placebo-controlled studiesThe placebo effect makes it more difficult to evaluate new treatments. Apparent benefits of a new treatment (usually a drug but not necessarily so) may not derive from the treatment but from the placebo effect. This is particularly likely, given that new therapies seem to have greater placebo effects.[citation needed] Clinical trials control for this effect by including a group of subjects that receives a sham treatment. The subjects in such trials are blinded as to whether they receive the treatment or a placebo. Clinical trials are often double-blinded so that the researchers also do not know which test subjects are receiving the active or placebo treatment.
The placebo effect in such clinical trials is weaker than in normal therapy since the subjects are not sure whether the treatment they are receiving is active.[104]
Knowingly giving a person a placebo when there is an effective treatment available is a bioethically complex issue. While placebo-controlled trials might provide information about the effectiveness of a treatment, it denies some patients what could be the best available (if unproven) treatment. Informed consent is usually required for a study to be considered ethical, including the disclosure that some test subjects will receive placebo treatments.
The ethics of placebo-controlled studies have been debated in the revision process of the Declaration of Helsinki. Of particular concern has been the difference between trials comparing inert placebos with experimental treatments, versus comparing the best available treatment with an experimental treatment; and differences between trials in the sponsor's developed countries versus the trial's targeted developing countries.[184]
A further issue of concern to pharmaceutical companies is that the effectiveness of placebos has increased over time,[185] thus making it more difficult to demonstrate the effectiveness of new drugs. The reason for the increased effectiveness in disputed.
Nocebo
Main article: NoceboIn the opposite effect, a patient who disbelieves in a treatment may experience a worsening of symptoms. This effect, now called by analogy nocebo (Latin nocebo = "I shall harm") can be measured in the same way as the placebo effect, e.g., when members of a control group receiving an inert substance report a worsening of symptoms. The recipients of the inert substance may nullify the placebo effect intended by simply having a negative attitude towards the effectiveness of the substance prescribed, which often leads to a nocebo effect, which is not caused by the substance, but due to other factors, such as the patient's mentality towards his or her ability to get well, or even purely coincidental worsening of symptoms.[107]
Placebo ingredients
Placebos used in clinical trials have sometimes had unintended consequences. A report in the Annals of Internal Medicine that looked at details from 150 clinical trials found that certain placebos used in the trials affected the results. For example, one study on cholesterol-lowering drugs used olive oil and corn oil in the placebo pills. However, according to the report, this "may lead to an understatement of drug benefit: The monounsaturated and polyunsaturated fatty acids of these 'placebos,' and their antioxidant and anti-inflammatory effects, can reduce lipid levels and heart disease." Another example researchers reported in the study was a clinical trial of a new therapy for cancer patients suffering from anorexia. The placebo that was used included lactose. However, since cancer patients typically face a higher risk of lactose intolerance, the placebo pill might actually have caused unintended side-effects that made the experimental drug look better in comparison.[186][187][188]
References
- ^ a b c Lanotte M, Lopiano L, Torre E, Bergamasco B, Colloca L, Benedetti F (November 2005). "Expectation enhances autonomic responses to stimulation of the human subthalamic limbic region". Brain, Behavior, and Immunity 19 (6): 500–9. doi:10.1016/j.bbi.2005.06.004. PMID 16055306.
- ^ Gensini GF, Conti AA, Conti A (April 2005). "Past and present of what will please the lord: an updated history of the concept of placebo". Minerva Med 96 (2): 121–4. PMID 16172581.
- ^ a b c UK Parliamentary Committee Science and Technology Committee. "Evidence Check 2: Homeopathy". http://www.parliament.uk/parliamentary_committees/science_technology/s_t_homeopathy_inquiry.cfm.
- ^ a b Kaptchuk TJ, Friedlander E, Kelley JM, et al. (2010). "Placebos without deception: a randomized controlled trial in irritable bowel syndrome". PLoS ONE 5 (12): e15591. Bibcode 2010PLoSO...515591K. doi:10.1371/journal.pone.0015591. PMC 3008733. PMID 21203519. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=3008733. Lay summary.
- ^ a b c Hróbjartsson A, Norup M (June 2003). "The use of placebo interventions in medical practice--a national questionnaire survey of Danish clinicians". Evaluation & the Health Professions 26 (2): 153–65. doi:10.1177/0163278703026002002. PMID 12789709. http://ehp.sagepub.com/cgi/pmidlookup?view=long&pmid=12789709.
- ^ a b Eccles R (2002). "The powerful placebo in cough studies?". Pulm Pharmacol Ther 15 (3): 251–2. doi:10.1006/pupt.2002.0364. PMID 12099783.
- ^ a b c d David H. Newman (2008). Hippocrates' Shadow. Scribner. pp. 134–59. ISBN 1-4165-5153-0.
- ^ a b c d Hróbjartsson A, Gøtzsche PC (2001). "Is the placebo powerless? An analysis of clinical trials comparing placebo with no treatment". New England Journal of Medicine 344 (21): 1594–1602. doi:10.1056/NEJM200105243442106. PMID 11372012. http://content.nejm.org/cgi/content/short/344/21/1594.
- ^ a b c d e Moerman DE, Jonas WB (2002). "Deconstructing the placebo effect and finding the meaning response". Ann Intern Med. 136 (6): 471–6. PMID 11900500. http://www.annals.org/cgi/content/full/136/6/471.
- ^ Hróbjartsson A, Gøtzsche PC (20 January 2010). "Placebo interventions for all clinical conditions". Cochrane Database Syst Rev 106 (1): CD003974. doi:10.1002/14651858.CD003974.pub3. PMID 20091554.
- ^ a b Ho KH, Hashish I, Salmon P, Freeman R, Harvey W (1988). "Reduction of post-operative swelling by a placebo effect". Journal of Psychosomatic Research 32 (2): 197–205. doi:10.1016/0022-3999(88)90055-4. PMID 3404502.
- ^ a b Hashish I, Harvey W, Harris M (February 1986). "Anti-inflammatory effects of ultrasound therapy: evidence for a major placebo effect". British Journal of Rheumatology 25 (1): 77–81. doi:10.1093/rheumatology/25.1.77. PMID 2417648. http://rheumatology.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=2417648.
- ^ Cobb LA, Thomas GI, Dillard DH, Merendino KA, Bruce RA (May 1959). "An evaluation of internal-mammary-artery ligation by a double-blind technic". The New England Journal of Medicine 260 (22): 1115–8. doi:10.1056/NEJM195905282602204. PMID 13657350.
- ^ Benson H, McCallie DP (June 1979). "Angina pectoris and the placebo effect". The New England Journal of Medicine 300 (25): 1424–9. doi:10.1056/NEJM197906213002508. PMID 35750.
- ^ Moseley JB, O'Malley K, Petersen NJ, et al. (July 2002). "A controlled trial of arthroscopic surgery for osteoarthritis of the knee". The New England Journal of Medicine 347 (2): 81–8. doi:10.1056/NEJMoa013259. PMID 12110735.
- ^ a b Kaptchuk TJ, Stason WB, Davis RB, et al. (February 2006). "Sham device v inert pill: randomised controlled trial of two placebo treatments". BMJ 332 (7538): 391–7. doi:10.1136/bmj.38726.603310.55. PMC 1370970. PMID 16452103. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1370970.
- ^ Holm L, Bengtsson A, van Hage-Hamsten M, Ohman S, Scheynius A (February 2001). "Effectiveness of occlusive bedding in the treatment of atopic dermatitis—a placebo-controlled trial of 12 months' duration". Allergy 56 (2): 152–8. doi:10.1034/j.1398-9995.2001.056002152.x. PMID 11167376.
- ^ Margo CE (1999). "The placebo effect". Surv Ophthalmol. 44 (1): 33–4. doi:10.1016/S0039-6257(99)00060-0. PMID 10466586.
- ^ Thomas KB (1987). "General practice consultations: is there any point in being positive?". Br Med J (Clin Res Ed) 294 (6581): 1200–2. doi:10.1136/bmj.294.6581.1200. PMC 1246362. PMID 3109581. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1246362.
- ^ Colloca L, Lopiano L, Lanotte M, Benedetti F (2004). "Overt versus covert treatment for pain, anxiety, and Parkinson's disease". Lancet Neurol. 3 (11): 679–84. doi:10.1016/S1474-4422(04)00908-1. PMID 15488461.
- ^ Ernst E, Resch KL (August 1995). "Concept of true and perceived placebo effects". BMJ 311 (7004): 551–3. PMC 2550609. PMID 7663213. http://bmj.com/cgi/pmidlookup?view=long&pmid=7663213.
- ^ a b c d de Craen AJ, Kaptchuk TJ, Tijssen JG, Kleijnen J (October 1999). "Placebos and placebo effects in medicine: historical overview". J R Soc Med 92 (10): 511–5. PMC 1297390. PMID 10692902. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1297390.
- ^ Leigh bureau, http://leighbureau.com/speaker.asp?id=459.
- ^ Jacobs B. (2000). "Biblical origins of placebo". J R Soc Med. 93 (4): 213–4. PMC 1297986. PMID 10844895. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1297986.
- ^ Shapiro AK (1968). "Semantics of the placebo". Psychiatr Q. 42 (4): 653–95. doi:10.1007/BF01564309. PMID 4891851.
- ^ Kaptchuk TJ (1998). "Powerful placebo: the dark side of the randomised controlled trial". Lancet 351 (9117): 1722–5. doi:10.1016/S0140-6736(97)10111-8. PMID 9734904.
- ^ Beecher HK (July 1961). "Surgery as placebo. A quantitative study of bias". J Am Med Assoc 176: 1102–7. PMID 13688614.
- ^ Kaptchuk, T. J. (1998). Intentional Ignorance: A History of Blind Assessment and Placebo Controls in Medicine. Bulletin of the History of Medicine, 72(3), 389-433.
- ^ Benedetti F, Mayberg HS, Wager TD, Stohler CS, Zubieta JK (November 2005). "Neurobiological mechanisms of the placebo effect". J. Neurosci. 25 (45): 10390–402. doi:10.1523/JNEUROSCI.3458-05.2005. PMID 16280578. http://www.jneurosci.org/cgi/content/short/25/45/10390.
- ^ Kirsch, I. (1985). Response Expectancy as a Determinant of Experience and Behavior. American Psychologist, 40(11), 1189-1202.
- ^ Voudouris NJ, Peck CL, Coleman G (1989). "Conditioned response models of placebo phenomena: further support". Pain 38 (1): 109–16. doi:10.1016/0304-3959(89)90080-8. PMID 2780058.
- ^ Stewart-Williams S, Podd J (2004). "The placebo effect: dissolving the expectancy versus conditioning debate". Psychol Bull 130 (2): 324–40. doi:10.1037/0033-2909.130.2.324. PMID 14979775.
- ^ Klinger R, Soost S, Flor H, Worm M (2007). "Classical conditioning and expectancy in placebo hypoalgesia: a randomized controlled study in patients with atopic dermatitis and persons with healthy skin". Pain 128:31-9 (1-2): 31–9. doi:10.1016/j.pain.2006.08.025. PMID 17030095.
- ^ a b Colloca L, Tinazzi M, Recchia S, Le Pera D, Fiaschi A, Benedetti F, Valeriani M (2008). "Learning potentiates neurophysiological and behavioral placebo analgesic responses". Pain 139 (2): 306–14. doi:10.1016/j.pain.2008.04.021. PMID 18538928.
- ^ Kaptchuk TJ, Kelley JM, Conboy LA, Davis RB, Kerr CE, Jacobson EE, Kirsch I, Schyner RN, Nam BH, Nguyen LT, Park M, Rivers AL, McManus C, Kokkotou E, Drossman DA, Goldman P, Lembo AJ (2008). "Components of placebo effect: randomized controlled trial in patients with irritable bowel syndrome". BMJ 336 (7651): 999–1003. doi:10.1136/bmj.39524.439618.25. PMC 2364862. PMID 18390493. http://www.bmj.com/cgi/reprint/336/7651/999.
- ^ Linde K, Witt CM, Streng A, Weidenhammer W, Wagenpfeil S, Brinkhaus B, Willich SN, Melchart D (2007). "The effect of patient expectations on outcomes in four randomized controlled trials of acupuncture in patients with chronic pain". Pain 128 (3): 264–71. doi:10.1016/j.pain.2006.12.006. PMID 17257756.
- ^ Bausell RB, Lao L, Bergman S, Lee WL, Berman BM (2005). "Is acupuncture analgesia an expectancy effect? Preliminary evidence based on participants' perceived assignments in two placebo-controlled trials". Eval Health Prof. 28 (1): 9–26. doi:10.1177/0163278704273081. PMID 15677384.
- ^ a b Montgomery GH, Kirsch I (1997). "Classical conditioning and the placebo effect". Pain 72 (1-2): 107–13. doi:10.1016/S0304-3959(97)00016-X. PMID 9272794.
- ^ a b "Against Depression, a Sugar Pill Is Hard to Beat". The Washington Post. May 7, 2002. http://www.chelationtherapyonline.com/technical/p58.htm.
- ^ Flaten MA, Simonsen T, Olsen H (1999). "Drug-related information generates placebo and nocebo responses that modify the drug response". Psychosom Med. 61 (2): 250–5. PMID 10204979. http://www.psychosomaticmedicine.org/cgi/reprint/61/2/250.
- ^ Kirsch I (1997). "Specifying non-specifics: Psychological mechanism of the placebo effect". In Harrington A. The Placebo Effect: An Interdisciplinary Exploration. Cambridge: Harvard University Press. pp. 166–86. ISBN 978-0674669864.
- ^ Kirsch, I., & Weixel, L. J. (1988). Double-blind versus deceptive administration of a placebo. Behavioral Neuroscience, 102(2), 319-323.
- ^ Kirsch, I., & Rosadino, M. J. (1993). Do Double-Blind Studies with Informed Consent Yield Externally Valid Results - an Empirical-Test. Psychopharmacology, 110(4), 437-442.
- ^ Flaten MA, Aasli O, Blumenthal TD (2003). "Expectations and placebo responses to caffeine-associated stimuli". Psychopharmacology 169 (2): 198–204. doi:10.1007/s00213-003-1497-8. PMID 12759808.
- ^ O'Boyle DJ, Binns AS, Sumner JJ (1994). "On the efficacy of alcohol placebos in inducing feelings of intoxication". Psychopharmacology (Berl) 115 (1-2): 229–36. doi:10.1007/BF02244776. PMID 7862899.
- ^ Fillmore MT, Mulvihill LE, Vogel-Sprott M (1994). "The expected drug and its expected effect interact to determine placebo responses to alcohol and caffeine". Psychopharmacology 115 (3): 383–8. doi:10.1007/BF02245081. PMID 7871080.
- ^ Beedie CJ, Coleman DA, Foad AJ (2007). "Positive and negative placebo effects resulting from the deceptive administration of an ergogenic aid". Int. J. Sport Nutr. Exerc. Metab. 17: 259–269.
- ^ Clark K, Milliken R (21 August 2000). "Today, it’s "May the best swimsuit win"". US News and World Report: p. 55. http://www.usnews.com/usnews/culture/articles/000821/archive_013509.htm., cited in: Moerman DE, Jonas WB (19 March 2002). "Deconstructing the placebo effect and finding the meaning response". Ann Intern Med 136 (6): 471–6. PMID 11900500. http://www.annals.org/cgi/content/full/136/6/471.
- ^ Pollo A, Carlino E, Benedetti F (July 2008). "The top-down influence of ergogenic placebos on muscle work and fatigue". Eur. J. Neurosci. 28 (2): 379–88. doi:10.1111/j.1460-9568.2008.06344.x. PMID 18702709. http://www3.interscience.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=0953-816X&date=2008&volume=28&issue=2&spage=379.
- ^ Benedetti F, Pollo A, Colloca L (2007). "Opioid-mediated placebo responses boost pain endurance and physical performance – is it doping in sport competitions". J. Neurosci. 27 (44): 11934–9. doi:10.1523/JNEUROSCI.3330-07.2007. PMID 17978033. http://www.jneurosci.org/cgi/reprint/27/44/11934.
- ^ Dar R, Stronguin F, Etter JF (2005). "Assigned versus perceived placebo effects in nicotine replacement therapy for smoking reduction in Swiss smokers". J Consult Clin Psychol 73 (2): 350–3. doi:10.1037/0022-006X.73.2.350. PMID 15796644.
- ^ Ikemi Y, Nakagawa S (1962). "A psychosomatic study of contagious dermatitis". Kyoshu Journal of Medical Science 13: 335–50.
- ^ a b Evens, D. (2003) Placebo: The belief effect. HarperCollins ISBN 978-0007126125
- ^ McRae C, Cherin E, Yamazaki TG, Diem G, Vo AH, Russell D, Ellgring JH, Fahn S, Greene P, Dillon S, Winfield H, Bjugstad KB, Freed CR (2004). "Effects of perceived treatment on quality of life and medical outcomes in a double-blind placebo surgery trial". Arch Gen Psychiatry 61 (4): 412–20. doi:10.1001/archpsyc.61.4.412. PMID 15066900.
- ^ de Craen AJ, Roos PJ, Leonard de Vries A, Kleijnen J (1996). "Effect of colour of drugs: systematic review of perceived effect of drugs and of their effectiveness". BMJ 313 (7072): 1624–6. PMC 2359128. PMID 8991013. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2359128.
- ^ Buckalew LW, Ross S (1981). "Relationship of perceptual characteristics to efficacy of placebos". Psychol. Rep. 49 (3): 955–61. PMID 7330154.
- ^ Dolinska B (1999). "Empirical investigation into placebo effectiveness". Ir J Psych Med 16 (2): 57–58. http://www.ijpm.org/content/pdf/139/placebo.pdf.
- ^ Blackwell B, Bloomfield SS, Buncher CR (1972). "Demonstration to medical students of placebo responses and non-drug factors". Lancet 1 (7763): 1279–82. PMID 4113531.
- ^ Branthwaite A, Cooper P (1981). "Analgesic effects of branding in treatment of headaches". Br Med J (Clin Res Ed) 282 (6276): 1576–8. doi:10.1136/bmj.282.6276.1576. PMC 1505530. PMID 6786566. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1505530.
- ^ Colloca L, Benedetti F (2006). "How prior experience shapes placebo analgesia". Pain 124 (1-2): 126–33. doi:10.1016/j.pain.2006.04.005. PMID 16701952.
- ^ Waber RL, Shiv B, Carmon Z, Ariely D (2008). "Commercial features of placebo and therapeutic efficacy". JAMA 299 (9): 1016–7. doi:10.1001/jama.299.9.1016. PMID 18319411.
- ^ a b Grenfell RF, Briggs AH, Holland WC (1961). "A double-blind study of the treatment of hypertension". JAMA 176: 124–8. PMID 13708477.
- ^ Simpson SH, Eurich DT, Majumdar SR, Padwal RS, Tsuyuki RT, Varney J, Johnson JA (2006). "A meta-analysis of the association between adherence to drug therapy and mortality". BMJ 333 (7557): 15. doi:10.1136/bmj.38875.675486.55. PMC 1488752. PMID 16790458. http://www.bmj.com/cgi/reprint/333/7557/15.
- ^ a b Geers AL, Weiland PE, Kosbab K, Landry SJ, Helfer SG (2005). "Goal activation, expectations, and the placebo effect". J Pers Soc Psychol 89 (2): 143–59. doi:10.1037/0022-3514.89.2.143. PMID 16162050.
- ^ a b Geers AL, Helfer SG, Weiland PE, Kosbab K (2006). "Expectations and placebo response: a laboratory investigation into the role of somatic focus". J Behav Med 29 (2): 171–8. doi:10.1007/s10865-005-9040-5. PMID 16374671.
- ^ a b c Moerman DE (2000). "Cultural variations in the placebo effect: ulcers, anxiety, and blood pressure". Med Anthropol Q 14 (51-72): 51–72. doi:10.1525/maq.2000.14.1.51. PMID 10812563.
- ^ Colloca L, Benedetti F (2009). "Placebo analgesia induced by social observational learning". Pain 144 (1-2): 28–34. doi:10.1016/j.pain.2009.01.033. PMID 19278785.
- ^ a b Benedetti F, Arduino C, Amanzio M (1999). "Somatotopic activation of opioid systems by target-directed expectations of analgesia". J Neurosci 19 (9): 3639–48. PMID 10212322. http://www.jneurosci.org/cgi/reprint/19/9/3639.
- ^ Whalley B, Hyland ME, Kirsch I (2008). "Consistency of the placebo effect". J Psychosom Res 64 (5): 537–41. doi:10.1016/j.jpsychores.2007.11.007. PMID 18440407.
- ^ Oken BS (2008). "Placebo effects: clinical aspects and neurobiology". Brain 131 (Pt 11): 2812–23. doi:10.1093/brain/awn116. PMC 2725026. PMID 18567924. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2725026.
- ^ a b c Scott DJ, Stohler CS, Egnatuk CM, Wang H, Koeppe RA, Zubieta JK (2008). "Placebo and nocebo effects are defined by opposite opioid and dopaminergic responses". Arch Gen Psychiatry 65 (2): 220–31. doi:10.1001/archgenpsychiatry.2007.34. PMID 18250260.
- ^ Lidstone SC, Stoessl AJ (2007). "Understanding the placebo effect: contributions from neuroimaging". Mol Imaging Biol 9 (4): 176–85. doi:10.1007/s11307-007-0086-3. PMID 17334853.
- ^ a b Goffaux P, Redmond WJ, Rainville P, Marchand S (2007). "Descending analgesia--when the spine echoes what the brain expects". Pain 130 (1-2): 137–43. doi:10.1016/j.pain.2006.11.011. PMID 17215080.
- ^ Matre D, Casey KL, Knardahl S (2006). "Placebo-induced changes in spinal cord pain processing". J Neurosci 26 (2): 559–63. doi:10.1523/JNEUROSCI.4218-05.2006. PMID 16407554. http://www.jneurosci.org/cgi/reprint/26/2/559.
- ^ Qiu YH, Wu XY, Xu H, Sackett D (October 2009). "Neuroimaging study of placebo analgesia in humans". Neurosci Bull 25 (5): 277–82. doi:10.1007/s12264-009-0907-2. PMID 19784082.
- ^ Zubieta JK, Stohler CS (March 2009). "Neurobiological mechanisms of placebo responses". Ann N Y Acad Sci 1156: 198–210. doi:10.1111/j.1749-6632.2009.04424.x. PMID 19338509.
- ^ Nemoto H, Nemoto Y, Toda H, Mikuni M, Fukuyama H (2007). "Placebo analgesia: a PET study". Exp Brain Res 179 (4): 655–64. doi:10.1007/s00221-006-0821-z. PMID 17287994.
- ^ Craggs JG, Price DD, Verne GN, Perlstein WM, Robinson MM (2007). "Functional brain interactions that serve cognitive-affective processing during pain and placebo analgesia". Neuroimage 38 (4): 720–9. doi:10.1016/j.neuroimage.2007.07.057. PMC 2100389. PMID 17904390. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2100389.
- ^ Bingel U, Lorenz J, Schoell E, Weiller C, Büchel C (2006). "Mechanisms of placebo analgesia: rACC recruitment of a subcortical antinociceptive network". Pain 120 (1-2): 8–15. doi:10.1016/j.pain.2005.08.027. PMID 16364549.
- ^ Wager TD, Rilling JK, Smith EE, Sokolik A, Casey KL, Davidson RJ, Kosslyn SM, Rose RM, Cohen JD (2004). "Placebo-induced changes in FMRI in the anticipation and experience of pain". Science 303 (5661): 1162–7. doi:10.1126/science.1093065. PMID 14976306.
- ^ Levine JD, Gordon NC, Fields HL (1978). "The mechanism of placebo analgesia". Lancet 2 (8091): 654–7. PMID 80579.
- ^ de la Fuente-Fernández R, Ruth TJ, Sossi V, Schulzer M, Calne DB, Stoessl AJ (2001). "Expectation and dopamine release: mechanism of the placebo effect in Parkinson's disease". Science 293 (5532): 1164–6. doi:10.1126/science.1060937. PMID 11498597.
- ^ Mayberg HS, Silva JA, Brannan SK, Tekell JL, Mahurin RK, McGinnis S, Jerabek PA (2002). "The functional neuroanatomy of the placebo effect". Am J Psychiatry 159 (5): 728–37. doi:10.1176/appi.ajp.159.5.728. PMID 11986125. http://ajp.psychiatryonline.org/cgi/reprint/159/5/728.
- ^ Leuchter AF, Cook IA, Witte EA, Morgan M, Abrams M (2002). "Changes in brain function of depressed subjects during treatment with placebo". Am J Psychiatry 159 (1): 122–9. doi:10.1176/appi.ajp.159.1.122. PMID 11772700. http://ajp.psychiatryonline.org/cgi/reprint/159/1/122.
- ^ Kaasinen V, Aalto S, Någren K, Rinne JO (2004). "Expectation of caffeine induces dopaminergic responses in humans". Eur J Neurosci 19 (8): 2352–6. doi:10.1111/j.1460-9568.2004.03310.x. PMID 15090062.
- ^ Haltia LT, Rinne JO, Helin S, Parkkola R, Någren K, Kaasinen V (2008). "Effects of intravenous placebo with glucose expectation on human basal ganglia dopaminergic function". Synapse 62 (9): 682–8. doi:10.1002/syn.20541. PMID 18566972.
- ^ Volkow ND, Wang GJ, Ma Y, Fowler JS, Wong C, Jayne M, Telang F, Swanson JM (2006). "Effects of expectation on the brain metabolic responses to methylphenidate and to its placebo in non-drug abusing subjects". Neuroimage 32 (4): 1782–92. doi:10.1016/j.neuroimage.2006.04.192. PMID 16757181.
- ^ Faria V, Fredrikson M, Furmark T (2008). "Imaging the placebo response: a neurofunctional review". Eur Neuropsychopharmacol 18 (7): 473–85. doi:10.1016/j.euroneuro.2008.03.002. PMID 18495442.
- ^ Diederich NJ, Goetz CG (2008). "The placebo treatments in neurosciences: New insights from clinical and neuroimaging studies". Neurology 71 (9): 677–84. doi:10.1212/01.wnl.0000324635.49971.3d. PMID 18725593.
- ^ Ader, R; Cohen, N (1975). "Behaviorally conditioned immunosuppression". Psychosom Med 37 (4): 333–40. PMID 1162023.
- ^ a b Pacheco-López G, Engler H, Niemi MB, Schedlowski M (2006). "Expectations and associations that heal: Immunomodulatory placebo effects and its neurobiology". Brain Behav Immun 20 (430-46): 430–46. doi:10.1016/j.bbi.2006.05.003. PMID 16887325.
- ^ Colloca L, Benedetti F (2005). "Placebos and painkillers: is mind as real as matter?". Nat Rev Neurosci 6 (7): 545–52. doi:10.1038/nrn1705. PMID 15995725.
- ^ Eippert F, Finsterbusch J, Bingel U, Büchel1 C (2009). "Direct evidence for spinal cord involvement in placebo analgesia". Science 326 (5951): 404. doi:10.1126/science.1180142. PMID 19833962.
- ^ Humphrey N (2002). "Great Expectations: The Evolutionary Psychology of Faith-Healing and the Placebo Effect". The Mind Made Flesh: Essays from the Frontiers of Psychology and Evolution. Oxford University Press. pp. 255–85. ISBN 978-0192802279. http://www.humphrey.org.uk/papers/2002GreatExpectations.pdf.
- ^ Coryell W, Noyes R (1988). "Placebo response in panic disorder". Am J Psychiatry 145 (9): 1138–40. PMID 3046384.
- ^ Boissel JP, Philippon AM, Gauthier E, Schbath J, Destors JM (1986). "Time course of long-term placebo therapy effects in angina pectoris". Eur Heart J 7 (12): 1030–6. PMID 3104043.
- ^ Traut EF, Passarelli EW (1957). "Placebos in the treatment of rheumatoid arthritis and other rheumatic conditions". Ann Rheum Dis 16 (1): 18–22. doi:10.1136/ard.16.1.18. PMC 1006924. PMID 13412002. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1006924.
- ^ Hróbjartsson A, Gøtzsche PC (2004). "Is the placebo powerless? Update of a systematic review with 52 new randomized trials comparing placebo with no treatment". J. Intern. Med. 256 (2): 91–100. doi:10.1111/j.1365-2796.2004.01355.x. PMID 15257721. http://www3.interscience.wiley.com/journal/118792130/abstract.
- ^ Wampold BE, Minami T, Tierney SC, Baskin TW, Bhati KS (2005). "The placebo is powerful: estimating placebo effects in medicine and psychotherapy from randomized clinical trials". J Clin Psychol 61 (7): 835–54. doi:10.1002/jclp.20129. PMID 15827993.
- ^ Wampold BE, Imel ZE, Minami T (2007). "The placebo effect: "relatively large" and "robust" enough to survive another assault". J Clin Psychol 63 (4): 401–3. doi:10.1002/jclp.20350. PMID 17279522.
- ^ Hróbjartsson A, Gøtzsche PC (2007). "Powerful spin in the conclusion of Wampold et al.'s re-analysis of placebo versus no-treatment trials despite similar results as in original review". J Clin Psychol 63 (4): 373–7. doi:10.1002/jclp.20357. PMID 17279532.
- ^ Hunsley J, Westmacott R (2007). "Interpreting the magnitude of the placebo effect: mountain or Molehill?". J Clin Psychol 63 (4): 391–9. doi:10.1002/jclp.20352. PMID 17279525.
- ^ a b Meissner K, Distel H, Mitzdorf U (2007). "Evidence for placebo effects on physical but not on biochemical outcome parameters: a review of clinical trials". BMC Med 5: 3. doi:10.1186/1741-7015-5-3. PMC 1847831. PMID 17371590. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1847831.
- ^ a b Vase L, Riley JL 3rd, Price DD (2003). "A comparison of placebo effects in clinical analgesic trials versus studies of placebo analgesia". Pain 104 (3): 714–5. doi:10.1016/S0304-3959(02)00205-1. PMID 12406519.
- ^ Barfod TS (2005). "Placebos in medicine: placebo use is well known, placebo effect is not". BMJ 330 (7481): 45. doi:10.1136/bmj.330.7481.45. PMC 539859. PMID 15626818. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=539859.
- ^ Hróbjartsson A, Gøtzsche PC (January 2010). "Placebo interventions for all clinical conditions". Cochrane Database of Systematic Reviews (1): CD003974. doi:10.1002/14651858.CD003974.pub3. PMID 20091554. http://mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD003974/frame.html.
- ^ a b "The Nocebo Effect". Priory.com. 10 February 2007. http://priory.com/medicine/Nocebo.htm. Retrieved 2009-07-08.
- ^ Shapiro AK, Chassan J, Morris LA, Frick R (1974). "Placebo induced side effects". Journal of Operational Psychiatry 6: 43–6. http://psycnet.apa.org/?fa=main.doiLanding&uid=1977-04006-001.
- ^ Benedetti F, Amanzio M, Baldi S, Casadio C, Cavallo A, Mancuso M, Ruffini E, Oliaro A, Maggi G (1998). "The specific effects of prior opioid exposure on placebo analgesia and placebo respiratory depression". Pain 75 (2-3): 313–9. doi:10.1016/S0304-3959(98)00010-4. PMID 9583767.
- ^ Ockene JK, Barad DH, Cochrane BB, Larson JC, Gass M, Wassertheil-Smoller S, Manson JE, Barnabei VM, Lane DS, Brzyski RG, Rosal MC, Wylie-Rosett J, Hays J (2005). "Symptom experience after discontinuing use of estrogen plus progestin". JAMA 294 (2): 183–93. doi:10.1001/jama.294.2.183. PMID 16014592. http://jama.ama-assn.org/cgi/reprint/294/2/183.
- ^ Nitzan U, Lichtenberg P (October 23, 2004). "Questionnaire survey on use of placebo". BMJ 329 (7472): 944–6. doi:10.1136/bmj.38236.646678.55. PMC 524103. PMID 15377572. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=524103.
- ^ a b Spiegel D (October 23, 2004). "Placebos in practice". BMJ 329 (7472): 927–8. doi:10.1136/bmj.329.7472.927. PMC 524090. PMID 15499085. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=524090.
- ^ a b Sandler AD, Bodfish JW (2008). "Open-label use of placebos in the treatment of ADHD: a pilot study". Child Care Health Dev 34 (1): 104–10. doi:10.1111/j.1365-2214.2007.00797.x. PMID 18171451.
- ^ Doctors Struggle With Tougher-Than-Ever Dilemmas: Other Ethical Issues Author: Leslie Kane. 11/11/2010
- ^ a b c Benedetti F (1996). "The opposite effects of the opiate antagonist naloxone and the cholecystokinin antagonist proglumide on placebo analgesia". Pain 64 (3): 535–43. doi:10.1016/0304-3959(95)00179-4. PMID 8783319.
- ^ a b Levine JD, Gordon NC, Bornstein JC, Fields HL (1979). "Role of pain in placebo analgesia". Proc Natl Acad Sci U S A 76 (7): 3528–31. doi:10.1073/pnas.76.7.3528. PMC 383861. PMID 291020. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=383861.
- ^ Beecher HK (1955). "The powerful placebo". J Am Med Assoc 159 (17): 1602–6. PMID 13271123.
- ^ Petrovic P, Kalso E, Petersson KM, Ingvar M (2002). "Placebo and opioid analgesia-- imaging a shared neuronal network". Science 295 (5560): 1737–40. doi:10.1126/science.1067176. PMID 11834781. (in Supplementary Material)
- ^ a b Levine JD, Gordon NC, Smith R, Fields HL (1981). "Analgesic responses to morphine and placebo in individuals with postoperative pain". Pain 10 (3): 379–89. doi:10.1016/0304-3959(81)90099-3. PMID 7279424.
- ^ Doongaji DR, Vahia VN, Bharucha MP (1978). "On placebos, placebo responses and placebo responders. (A review of psychological, psychopharmacological and psychophysiological factors)". J Postgrad Med 24 (2): 91–7. PMID 364041.
- ^ a b c Hoffman GA, Harrington A, Fields HL (2005). "Pain and the placebo: what we have learned". Perspect Biol Med 48 (2): 248–65. doi:10.1353/pbm.2005.0054. PMID 15834197.
- ^ Zubieta JK, Yau WY, Scott DJ, Stohler CS (2006). "Belief or Need? Accounting for individual variations in the neurochemistry of the placebo effect". Brain Behav Immun 20 (1): 15–26. doi:10.1016/j.bbi.2005.08.006. PMID 16242910.>
- ^ Benedetti F, Arduino C, Costa S, Vighetti S, Tarenzi L, Rainero I, Asteggiano G (2006). "Loss of expectation-related mechanisms in Alzheimer's disease makes analgesic therapies less effective". Pain 121 (1-2): 133–44. doi:10.1016/j.pain.2005.12.016. PMID 16473462.
- ^ Rheims S, Cucherat M, Arzimanoglou A, Ryvlin P (August 12, 2008). "Greater response to placebo in children than in adults: a systematic review and meta-analysis in drug-resistant partial epilepsy". PLoS Med 5 (8): e166. doi:10.1371/journal.pmed.0050166. PMC 2504483. PMID 18700812. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2504483.
- ^ Furmark T, Appel L, Henningsson S, et al. (December 2008). "A link between serotonin-related gene polymorphisms, amygdala activity, and placebo-induced relief from social anxiety". J. Neurosci. 28 (49): 13066–74. doi:10.1523/JNEUROSCI.2534-08.2008. PMID 19052197. http://www.jneurosci.org/cgi/pmidlookup?view=long&pmid=19052197.
- ^ "The Placebo Effect: Not All in Your Head", ScienceNOW Daily News, 2 December 2008
- ^ "First 'placebo gene' discovered", New Scientist, 03 December 2008
- ^ Levine JD, Gordon NC, Bornstein JC, Fields HL. (1979) Role of pain in placebo analgesia. Proc Natl Acad Sci U S A. 76:3528-31.PubMed
- ^ Amanzio M, Benedetti F. (1999) Neuropharmacological dissection of placebo analgesia: expectation-activated opioid systems versus conditioning-activated specific subsystems. J Neurosci. 19:484-94. PubMed
- ^ Levine JD, Gordon NC. (1984) Influence of the method of drug administration on analgesic response. Nature. 312(5996):755-6. PubMed
- ^ a b Kirsch, I. Sapirstein, G. (1998) Listening to Prozac but hearing placebo: A meta-analysis of antidepressant medication. Prevention & Treatment. 1, ArtID 2a abstract
- ^ Kirsch, I., Deacon, B. J., Huedo-Medina, T. B., Scoboria, A., Moore, T. J., & Johnson, B. T. (2008). Initial severity and antidepressant benefits: A meta-analysis of data submitted to the Food and Drug Administration. PLoS Medicine, 5(2). Retrieved from http://medicine.plosjournals.org/perlserv/?request=get-document&doi=10.1371/journal.pmed.0050045
- ^ Fournier, J. C., DeRubeis, R. J., Hollon, S. D., Dimidjian, S., Amsterdam, J. D., Shelton, R. C., et al. (2010). Antidepressant Drug Effects and Depression Severity: A Patient-Level Meta-analysis. Journal of the American Medical Association, 303(1), 47-53.
- ^ Khan A, Redding N, Brown WA (2008). "The persistence of the placebo response in antidepressant clinical trials". Journal of Psychiatric Research 42 (10): 791–796. doi:10.1016/j.jpsychires.2007.10.004. PMID 18036616.
- ^ Khan A, Warner HA, and Brown WA. 2000. Symptom reduction and suicide risk in patients treated with placebo in antidepressant clinical trials: an analysis of the Food and Drug Administration database. Arch Gen Psychiatry 57:311–317. PubMed
- ^ a b Moerman, Daniel E. (2002). Meaning, Medicine and the Placebo Effect. Cambridge University Press. ISBN 0521806305. ISSN 978-0521000871.
- ^ Cho HJ, Hotopf M, Wessely S (2005). "The placebo response in the treatment of chronic fatigue syndrome: A systematic review and meta-analysis". Psychosom Med 67 (2): 301–13. doi:10.1097/01.psy.0000156969.76986.e0. PMID 15784798. http://www.psychosomaticmedicine.org/cgi/content/full/67/2/301.pdf. Retrieved 2008-12-12.
- ^ Levin FR, Evans SM, Brooks DJ, Kalbag AS, Garawi F, Nunes EV (2006). "Treatment of methadone-maintained patients with adult ADHD: double-blind comparison of methylphenidate, bupropion and placebo". Drug Alcohol Depend 81 (2): 137–48. doi:10.1016/j.drugalcdep.2005.06.012. PMID 16102908.
- ^ Grandjean P, Guldager B, Larsen IB, Jørgensen PJ, Holmstrup P (1997). "Placebo response in environmental disease. Chelation therapy of patients with symptoms attributed to amalgam fillings". J Occup Environ Med 39 (8): 707–14. PMID 9273873.
- ^ Schweizer E, Rickels K. (1997). "Placebo response in generalized anxiety: its effect on the outcome of clinical trials". J Clin Psychiatry 58 (Suppl 11): 30–8. PMID 9363046.
- ^ Piercy MA, Sramek JJ, Kurtz NM, Cutler NR (1996). "Placebo response in anxiety disorders". Ann Pharmacother 30 (9): 1013–9. PMID 8876864.
- ^ Butler C, Steptoe A (1986). "Placebo responses: an experimental study of psychophysiological processes in asthmatic volunteers". Br J Clin Psychol 25: 173–83. PMID 3768575.
- ^ Kemeny ME, Rosenwasser LJ, Panettieri RA, Rose RM, Berg-Smith SM, Kline JN (2007). "Placebo response in asthma: a robust and objective phenomenon". J Allergy Clin Immunol 119 (6): 1375–81. doi:10.1016/j.jaci.2007.03.016. PMID 17451796.
- ^ Kaptchuk TJ, Kelley JM, Deykin A, Wayne PM, Lasagna LC, Epstein IO, Kirsch I, Wechsler ME (2008). "Do "placebo responders" exist?". Contemp Clin Trials 29 (4): 587–95. doi:10.1016/j.cct.2008.02.002. PMID 18378192.
- ^ Sandler A (2005). "Placebo effects in developmental disabilities: implications for research and practice". Ment Retard Dev Disabil Res Rev 11 (2): 164–70. doi:10.1002/mrdd.20065. PMID 15977316.
- ^ Sandler AD, Sutton KA, DeWeese J, Girardi MA, Sheppard V, Bodfish JW (1999). "Lack of benefit of a single dose of synthetic human secretin in the treatment of autism and pervasive developmental disorder". N Engl J Med 341 (24): 1801–6. doi:10.1056/NEJM199912093412404. PMID 10588965. http://content.nejm.org/cgi/reprint/341/24/1801.pdf.
- ^ Madersbacher S, Marszalek M, Lackner J, Berger P, Schatzl G (2007). "The long-term outcome of medical therapy for BPH". Eur Urol 51 (6): 1522–33. doi:10.1016/j.eururo.2007.03.034. PMID 17416456.
- ^ Bulik CM, Brownley KA, Shapiro JR (2007). "Diagnosis and management of binge eating disorder". World Psychiatry 6 (3): 142–8. PMC 2174583. PMID 18188431. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2174583.
- ^ Sysko R, Walsh BT (2007). "A systematic review of placebo response in studies of bipolar mania". J Clin Psychiatry 68 (8): 1213–7. doi:10.4088/JCP.v68n0807. PMID 17854245.
- ^ Su C, Lichtenstein GR, Krok K, Brensinger CM, Lewis JD (2004). "A meta-analysis of the placebo rates of remission and response in clinical trials of active Crohn's disease". Gastroenterology 126 (5): 1257–69. doi:10.1053/j.gastro.2004.01.024. PMID 15131785.
- ^ Loving RT, Kripke DF, Elliott JA, Knickerbocker NC, Grandner MA (2005). "Bright light treatment of depression for older adults (ISRCTN55452501)". BMC Psychiatry 5: 41. doi:10.1186/1471-244X-5-41. PMC 1298312. PMID 16283925. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1298312.
- ^ Egbert LD, Battit GE, Welch CE, Bartlett MK (1964). "Reduction of postoperative pain by encouragement and instruction of patients. A study of doctor-patient rapport". N Engl J Med 270: 825–7. doi:10.1056/NEJM196404162701606. PMID 14108087.
- ^ Andrews G (2001). "Placebo response in depression: bane of research, boon to therapy". Br J Psychiatry 178 (3): 192–4. doi:10.1192/bjp.178.3.192. PMID 11230026. http://bjp.rcpsych.org/cgi/reprint/178/3/192.
- ^ Moncrieff J, Wessely S, Hardy R (2004). "Active placebos versus antidepressants for depression". Cochrane Database Syst Rev (1): CD003012. doi:10.1002/14651858.CD003012.pub2. PMID 14974002. CD003012.
- ^ Mearin F, Balboa A, Zárate N, Cucala M, Malagelada JR (1999). "Placebo in functional dyspepsia: symptomatic, gastrointestinal motor, and gastric sensorial responses". Am J Gastroenterol 94 (1): 116–25. doi:10.1111/j.1572-0241.1999.00781.x. PMID 9934741.
- ^ Niklson I, Edrich P, Verdru P (2006). "Identifying baseline characteristics of placebo responders versus nonresponders in randomized double-blind trials of refractory partial-onset seizures". Epileptic Disord 8 (1): 37–44. PMID 16567324.
- ^ Kriston L, Harms A, Berner MM (2006). "A meta-regression analysis of treatment effect modifiers in trials with flexible-dose oral sildenafil for erectile dysfunction in broad-spectrum populations". Int J Impot Res 18 (6): 559–65. doi:10.1038/sj.ijir.3901479. PMID 16688210.
- ^ Moerman DE (2000). "Cultural variations in the placebo effect: ulcers, anxiety, and blood pressure". Medical Anthropology Quarterly 14: 51–72. doi:10.1525/maq.2000.14.1.51. PMID 10812563.
- ^ Diener HC, Schorn CF, Bingel U, Dodick DW (2008). "The importance of placebo in headache research". Cephalagia 28 (10): 1003–11. doi:10.1111/j.1468-2982.2008.01660.x. PMID 18727647.
- ^ Archer TP, Leier CV (1992). "Placebo treatment in congestive heart failure". Cardiology 81 (2-3): 125–33. doi:10.1159/000175787. PMID 1286471.
- ^ Marks R, Koutts J (April 12, 1975). "Topical treatment of recurrent herpes simplex with cytosine arabinoside". Med J Aust 01 (15): 479–80. PMID 1097864.>
- ^ Asmar R, Safar M, Queneau P (2001). "Evaluation of the placebo effect and reproducibility of blood pressure measurement in hypertension". Am J Hypertens 14 (6 Pt 1): 546–52. doi:10.1016/S0895-7061(00)01286-3. PMID 11411734.
- ^ Patel SM, Stason WB, Legedza A, Ock SM, Kaptchuk TJ, Conboy L, Canenguez K, Park JK, Kelly E, Jacobson E, Kerr CE, Lembo AJ (2005). "The placebo effect in irritable bowel syndrome trials: a meta-analysis". Neurogastroenterol Motil 17 (3): 332–40. doi:10.1111/j.1365-2982.2005.00650.x. PMID 15916620.
- ^ Pitz M, Cheang M, Bernstein CN (2005). "Defining the predictors of the placebo response in irritable bowel syndrome". Clin Gastroenterol Hepatol 3 (237-47): 237–47. doi:10.1016/S1542-3565(04)00626-3. PMID 15765443.
- ^ Macedo A, Baños JE, Farré M (2008). "Placebo response in the prophylaxis of migraine: a meta-analysis". Eur J Pain 12 (1): 68–75. doi:10.1016/j.ejpain.2007.03.002. PMID 17451980.
- ^ La Mantia L, Eoli M, Salmaggi A, Milanese C (1996). "Does a placebo-effect exist in clinical trials on multiple sclerosis? Review of the literature". Ital J Neurol Sci 17 (2): 135–9. doi:10.1007/BF02000844. PMID 8797067.
- ^ Wolf S (1950). "Effects of suggestion and conditioning on the action of chemical agents in human subjects; the pharmacology of placebos". J Clin Invest 29 (1): 100–9. doi:10.1172/JCI102225. PMC 439730. PMID 15399519. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=439730.
- ^ Zhang Z, Wang Y, Wang Y, Xu F (2008). "Antiemetic placebo: reduce adverse drug interactions between chemotherapeutic agents and antiemetic drugs in cancer patients". Med Hypotheses 70 (3): 551–5. doi:10.1016/j.mehy.2007.06.029. PMID 17703892.
- ^ Shiao SY, Dune LS (2006). "Metaanalyses of acustimulations: effects on nausea and vomiting in postoperative adult patients". Explore (NY) 2 (3): 202–15. doi:10.1016/j.explore.2006.02.005. PMID 16781643.
- ^ Beecher HK, Keats AS, Mosteller F, Lasagna L (1953). "The effectiveness of oral analgesics (morphine, codeine, acetylsalicylic acid) and the problem of placebo "reactors" and "non-reactors"". J Pharmacol Exp Ther 109 (4): 393–400. PMID 13109703.
- ^ Baker B, Khaykin Y, Devins G, Dorian P, Shapiro C, Newman D (2003). "Correlates of therapeutic response in panic disorder presenting with palpitations: heart rate variability, sleep, and placebo effect". Can J Psychiatry 48 (6): 381–7. PMID 12894612.
- ^ de la Fuente-Fernández R, Stoessl AJ (2002). "The placebo effect in Parkinson's disease". Trends Neurosci 25 (6): 302–6. doi:10.1016/S0166-2236(02)02181-1. PMID 12086748.
- ^ Goetz CG, Wuu J, McDermott MP, Adler CH, Fahn S, Freed CR, Hauser RA, Olanow WC, Shoulson I, Tandon PK; Parkinson Study Group, Leurgans S (2008). "Placebo response in Parkinson's disease: comparisons among 11 trials covering medical and surgical interventions". Mov Disord 23 (5): 690–9. doi:10.1002/mds.21894. PMID 18228568.
- ^ Black DW, Arndt S, Coryell WH, Argo T, Forbush KT, Shaw MC, Perry P, Allen J (2007). "Bupropion in the treatment of pathological gambling: a randomized, double-blind, placebo-controlled, flexible-dose study". J Clin Psychopharmacol 27 (2): 143–50. doi:10.1097/01.jcp.0000264985.25109.25. PMID 17414236.
- ^ Eriksson E, Ekman A, Sinclair S, Sörvik K, Ysander C, Mattson UB, Nissbrandt H (2008). "Escitalopram administered in the luteal phase exerts a marked and dose-dependent effect in premenstrual dysphoric disorder". J Clin Psychopharmacol 28 (2): 195–202. doi:10.1097/JCP.0b013e3181678a28. PMID 18344730.
- ^ Brockbank J, Gladman D (2002). "Diagnosis and management of psoriatic arthritis". Drugs 62 (17): 2447–57. doi:10.2165/00003495-200262170-00004. PMID 12421102.
- ^ Pace F, Maconi G, Molteni P, Minguzzi M, Bianchi Porro G (1995). "Meta-analysis of the effect of placebo on the outcome of medically treated reflux esophagitis". Scand J Gastroenterol 30 (2): 101–5. doi:10.3109/00365529509093245. PMID 7732329.
- ^ Fulda S, Wetter TC (2008). "Where dopamine meets opioids: a meta-analysis of the placebo effect in restless legs syndrome treatment studies". Brain 131 (Pt 4): 902–17. doi:10.1093/brain/awm244. PMID 17932100.
- ^ Pollo A, Benedetti F (2008). "Placebo response: relevance to the rheumatic diseases". Rheum Dis Clin North Am 34 (2): 331–49. doi:10.1016/j.rdc.2008.04.002. PMID 18638680.
- ^ Bradford A, Meston C (2007). "Correlates of placebo response in the treatment of sexual dysfunction in women: a preliminary report". J Sex Med 4 (5): 1345–51. doi:10.1111/j.1743-6109.2007.00578.x. PMC 2859204. PMID 17666035. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2859204.
- ^ Oosterbaan DB, van Balkom AJ, Spinhoven P, van Dyck R (2001). "The placebo response in social phobia". J Psychopharmacol 15 (3): 199–203. doi:10.1177/026988110101500314. PMID 11565629.
- ^ Ilnyckyj A, Shanahan F, Anton PA, Cheang M, Bernstein CN (1997). "Quantification of the placebo response in ulcerative colitis". Gastroenterology 112 (6): 1854–8. doi:10.1053/gast.1997.v112.pm9178676. PMID 9178676.
- ^ Nyirjesy P, Sobel JD, Weitz MV, Leaman DJ, Small MJ, Gelone SP (2001). "Cromolyn cream for recalcitrant idiopathic vulvar vestibulitis: results of a placebo controlled study". Sex Transm Infect 77 (1): 53–7. doi:10.1136/sti.77.1.53. PMC 1758319. PMID 11158692. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1758319.
- ^ Kottow M (21 July 2010). "The improper use of research placebos". J Eval Clin Pract 16 (6): no. doi:10.1111/j.1365-2753.2009.01246.x. PMID 20663001.
- ^ Placebos Are Getting More Effective. Drugmakers Are Desperate to Know Why
- ^ "So, what's in a placebo, anyway?". Reuters. 18 October 2010. http://www.reuters.com/article/idUSTRE69H51L20101018.
- ^ Los Angeles Times. 18 October 2010. http://www.latimes.com/health/boostershots/la-heb-placebo-20101018,0,6180043.story?track=rss.
- ^ http://www.fiercebiotech.com/story/study-placebo-effect-may-have-hidden-meaning/2010-10-19?utm_medium=nl&utm_source=internal
External links
- Program in Placebo Studies at the Harvard Medical School
- The Placebo Effect at the Skeptic's Dictionary
- The Placebo Effect explained on YouTube
- Placebos: cracking the code part 1 part 2 BBC/Discovery channel program
- "The Placebo Effect: Do You Believe Your Teacher?" Ben Goldacre on The Guardian and on Wikibooks.
- "Placebos are getting more effective. Drugmakers are desperate to know why." Wired magazine on the power of the placebo. Retrieved 2010-07-22
- Biological, clinical, and ethical advances of placebo effects The Lancet (2010)
Categories:- Bioethics
- Deception
- Clinical research
- History of medicine
- Latin medical phrases
- Latin words and phrases
- Medical ethics
- Medical terms
- Medicinal chemistry
- Mind-body interventions
- Pharmacology
- Experimental psychology
- Theories
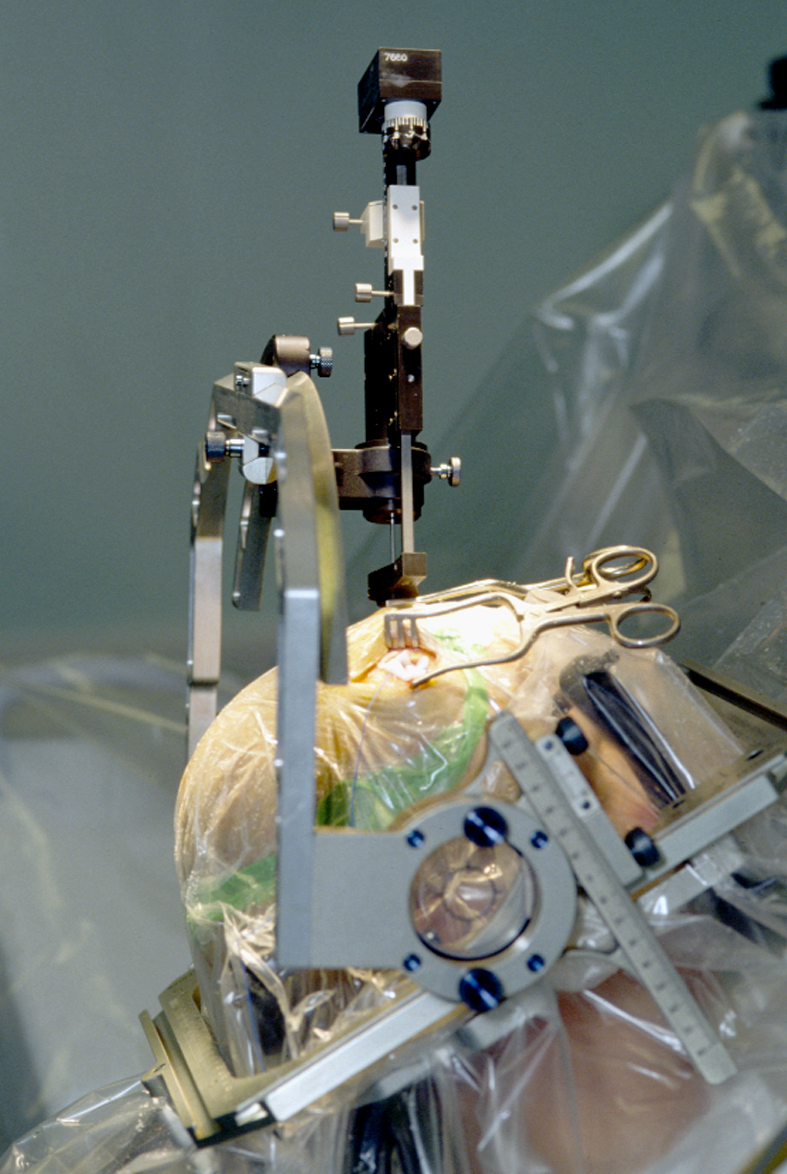
Wikimedia Foundation. 2010.