- Nitrazepam
-
Nitrazepam 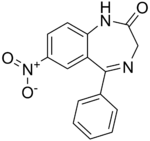
Systematic (IUPAC) name 9-nitro-6-phenyl-2,5-diazabicyclo[5.4.0]undeca-5,8,10,12-tetraen-3-one Clinical data Trade names Alodorm, Arem, Insoma, Mogadon, Nitrados, Nitrazadon, Ormodon, Paxadorm, Remnos, and Somnite AHFS/Drugs.com International Drug Names Pregnancy cat. D(AU) D(US) Legal status Schedule IV (International) Routes Oral Pharmacokinetic data Bioavailability 53-94% Metabolism Hepatic Half-life 16-38 hours Excretion Renal Identifiers CAS number 146-22-5 
ATC code N05CD02 PubChem CID 4506 DrugBank none ChemSpider 4350 UNII 9CLV70W7HS KEGG D00531 ChEMBL CHEMBL13209 Chemical data Formula C15H11N3O3 Mol. mass 281.3 g/mol SMILES eMolecules & PubChem - InChI=1S/C15H11N3O3/c19-14-9-16-15(10-4-2-1-3-5-10)12-8-11(18(20)21)6-7-13(12)17-14/h1-8H,9H2,(H,17,19)
Key:KJONHKAYOJNZEC-UHFFFAOYSA-N
 (what is this?) (verify)
(what is this?) (verify) Alodorm bottle containing 25 tablets of 5mg Nitrazepam.
Alodorm bottle containing 25 tablets of 5mg Nitrazepam.
Nitrazepam[1] is a type of benzodiazepine drug and is marketed in English-speaking countries under the following brand names: Alodorm, Arem, Insoma, Mogadon, Nitrados, Nitrazadon, Ormodon, Paxadorm, Remnos, and Somnite.[2] It is a hypnotic drug used in the treatment of moderate to severe insomnia which has sedative and motor impairing properties,[3] as well as anxiolytic, amnestic, anticonvulsant, and skeletal muscle relaxant properties. Nitrazepam is available in 5 mg and 10 mg tablets. In the Netherlands, Australia, Israel, and the United Kingdom it is only available in 5 mg tablets. In Denmark it is available as 2.5 mg and 5 mg tablets under the name Pacisyn.
Tolerance to the sleep inducing effects of nitrazepam occurs after about seven days;[4][5] tolerance also frequently occurs to the anticonvulsant effects of nitrazepam.[6][7] A benzodiazepine dependence can develop with a benzodiazepine withdrawal syndrome occurring when the drug is stopped or the dose lowered.[8] Common withdrawal symptoms include; anxiety, insomnia, concentration problems and fatigue.[9] Long-term effects of benzodiazepines such as nitrazepam include worsening mental and physical health as well as cognitive deficits;[10][11] immunological disturbances[12] and an increased risk of developing cancer has also been associated with long-term use.[13]
Nitrazepam at doses of 5 mg or higher impairs driving skills[14] and nitrazepam, like other hypnotic drugs is associated with an increased risk of road traffic accidents.[15] In the elderly nitrazepam is associated with an increased risk of falls and hip fractures due to impairments on body balance.[16] The elimination half-life of nitrazepam is 40 hours in the elderly and 29 hours in younger adults.[17][18] Nitrazepam is commonly taken in overdose by drug abusers or suicidal individuals, sometimes leading to death.[19][20][21] Nitrazepam is teratogenic if taken in overdose during pregnancy with 30 percent of births showing congenital abnormalities.[22] Nitrazepam is a popular drug of abuse in countries where it is available.[23][24][25]
Nitrazepam is not recommended during pregnancy as it is associated with causing a neonatal withdrawal syndrome[26] and is not generally recommended in alcohol- or drug-dependent individuals as well as people with comorbid psychiatric disorders.[27] The Dutch, British and French system called the System of Objectified Judgement Analysis for assessing whether drugs should be included in drug formularies based on clinical efficacy, adverse effects, pharmacokinetic properties, toxicity and drug interactions was used to assess nitrazepam. A Dutch analysis using the system found that nitrazepam is unsuitable to be included in drug prescribing formularies.[28]
Contents
Therapeutic uses
Nitrazepam is used to treat short-term sleeping problems (insomnia),[29] namely difficulty falling asleep, frequent awakening, early awakenings, or a combination of each.
Nitrazepam is sometimes used for refractory epilepsies. However, long term prophylactic treatment of epilepsy has considerable drawbacks. Most importantly the loss of antiepileptic effects due to tolerance which renders prolonged nitrazepam therapy ineffective. Nitrazepam also has the drawback of significant side effects such as sedation, which is why nitrazepam and benzodiazepines in general are only prescribed in the acute management of epilepsies.[30] Nitrazepam has been found to be more effective than clonazepam in the treatment of West syndrome which is an age dependent epilepsy, affecting the very young. However, as with other epilepsies treated with benzodiazepines, long term therapy becomes ineffective with prolonged therapy and the side effects of hypotonia and drowsiness are troublesome with nitrazepam therapy, other antiepileptic agents are therefore recommended for long term therapy, possibly Corticotropin (ACTH) or vigabatrin.[31] In uncontrolled studies nitrazepam has shown effectiveness in infantile spasms; nitrazepam is sometimes considered as a treatment option for this indication when other drugs fail to control infantile spasms.[32]
Popularity
Nitrazepam along with diazepam, oxazepam, and temazepam in 1993 represented 82% of the benzodiazepine market in Australia.[33] The rate of benzodiazepine prescribing in Tasmania is higher than in other Australian states; Nitrazepam and flunitrazepam prescribing levels in Tasmania are disturbingly high.[34] Prescribing of hypnotics in Norway is quite restrictive with only 4 hypnotics which are prescribable; nitrazepam, flunitrazepam, zolpidem and zopiclone.[35] The usage of benzodiazepine hypnotics in local authority homes for the elderly 1982 in Edinburgh, established via a clinical survey, was that 34% of residents were taking sleeping medication. However, the number varied between the homes, with some homes reporting only 2.3% of residents to be on hypnotic medication and others up to 56.5% on hypnotic drugs. Nitrazepam was the most frequently prescribed hypnotic medication accounting for a third of hypnotic use in Edinburgh residential homes in 1982.[36]
Side effects
Common side effects
Central nervous system depression including, somnolence, dizziness, depressed mood, rage, violence, fatigue, ataxia, headache, vertigo, impairment of memory, impairment of motor functions, hangover feeling in the morning, slurred speech, decreased physical performance, numbed emotions, reduced alertness, muscle weakness, double vision and inattention have been reported. Unpleasant dreams and rebound insomnia have also been reported. High levels of confusion, clumsiness also occurs after administration of nitrazepam.[37] Increased reaction time, co-ordination problems and impaired learning and memory.[38]
Impaired learning and memory occurs due to the action of the drug on benzodiazepine receptors which causes a dysfunction in the cholinergic neuronal system.[39] Nitrazepam causes a reduced output of serotonin which is closely involved in regulating mood and may be the cause of feelings of depression in users of nitrazepam or other benzodiazepines.[40]
Nitrazepam is a long acting benzodiazepine with an elimination half-life of 15-38 (mean elimination half-life 26 hours).[1] Residual "hangover" effects after nighttime administration of nitrazepam such as sleepiness, impaired psychomotor and cognitive functions may persist into the next day which may impair the ability of users to drive safely and increases the risk of falls and hip fractures.[41] Significant impairment of visual perception and sedative effects persisting into the next day typically occurs with nitrazepam administration as was demonstrated in a human clinical trial assessing the effect of nitrazepam on peak saccade velocity.[42]
Impairment of psychomotor function may especially occur after repeated administration, with the elderly being more vulnerable to this adverse effect.[43] Overall accuracy of completing tasks is impaired after repeated administration of nitrazepam and is due to drug accumulation of nitrazepam. The elderly are more vulnerable to these side effects.[44]
Less common side effects
Hypotension,[45] faintness, palpitation, rash or pruritus, gastrointestinal disturbances, changes in libido. Very infrequently, paradoxical reactions may occur,for example, excitement, stimulation, hallucinations, hyperactivity and insomnia. Also depressed or increased dreaming, disorientation, severe sedation, retrograde amnesia, headache, hypothermia, delirium tremens.[46] Acroparaesthesia has been reported as a side effect from nitrazepam with symptoms including, pins and needles in hands and loss of power of fingers and clumsiness of the fingers.[47] Severe liver toxicity has also been reported.[48]
Tolerance dependence and withdrawal
Tolerance
Tolerance to a drug's effects occurs after regular exposure to a drug. The mechanism of nitrazepam tolerance may be due to down-regulation of benzodiazepine receptors (observed in rats).[49] When tolerance and habituation occurs to nitrazepam its pharmacokinetic profile changes with absorption of the drug slowing down, elimination increasing and brain concentration of nitrazepam increasing significantly.[50] Increased levels of GABA in cerebral tissue and alterations in the activity state of the serotoninergic system occurs as a result of nitrazepam tolerance.[51]
After six days of use, tolerance to nitrazepam's but not temazepam's sleep-inducing effects and performance-impairing effects occurred in a study.[4] One study demonstrated tolerance to the sleep promoting effects of nitrazepam and temazepam after seven days nightly administration in 19 elderly inpatients. Self reported quality of sleep was found to be increased after the first nights administration of either nitrazepam or temazepam but by day seven self reported quality of sleep was found to have returned to baseline in these patients, suggesting the development of tolerance after seven days use. The effect was more pronounced in patients of lower intelligence.[5] In mice tolerance to the anticonvulsant properties of nitrazepam developed profoundly and rapidly over six days, and then did not proceed. Some anticonvulsant effects were still apparent after six days administration.[52] In humans tolerance to the anticonvulsant effects of nitrazepam is a frequent occurrence.[6][7]
Dependence and withdrawal
Benzodiazepine drugs such as nitrazepam can cause dependence and addiction and is what is known as the benzodiazepine withdrawal syndrome. Withdrawal from nitrazepam or other benzodiazepines often leads to withdrawal symptoms which are similar to those seen with alcohol and barbiturates, including delirium tremens.[53][54] The higher the dose and the longer the drug is taken the greater the risk of experiencing unpleasant withdrawal symptoms. Withdrawal symptoms can however occur at standard dosages and also after short term treatment. Benzodiazepine treatment should be discontinued as soon as possible via a slow and gradual dose reduction regime.[55] Common withdrawal symptoms include, anxiety, insomnia, concentration problems and fatigue.[9]
Frequent use of nitrazepam may cause dependence and when the drug is reduced or stopped, withdrawal symptoms occur. Withdrawal symptoms including a worsening of insomnia compared to baseline typically occurs after discontinuation of nitrazepam even after short term single nightly dose therapy.[56] Dependence on benzodiazepines such as nitrazepam or temazepam often occurs due to discharging patients from hospital on benzodiazepines who were started on benzodiazepine hypnotics in hospital. It is recommended that hypnotic use in hospital be limited to five days to avoid the development of drug dependence and withdrawal insomnia.[8]
After discontinuation of nitrazepam a rebound effect may occur about four days after stopping medication.[57] Nitrazepam has more side effects than other hypnotic drugs and tolerance to sedative properties and rebound insomnia after discontinuation occurs after only seven days administration.[58] Tolerance to the anticonvulsant and anxiolytic effects also develops rapidly during daily administration.[59]
Abrupt withdrawal after long term use from therapeutic doses of nitrazepam may result in a severe benzodiazepine withdrawal syndrome. Reports in the medical literature report of two psychotic states developing after abrupt withdrawal from nitrazepam including delirium after abrupt withdrawal of 10 mg of nitrazepam and in another case auditory hallucinations and visual cognitive disorder developed after abrupt withdrawal from 5 mg of nitrazepam and 0.5 mg of triazolam. Gradual and careful reduction of the dosage was recommended to prevent severe withdrawal syndromes from developing.[60] Antipsychotics increase the severity of benzodiazepine withdrawal effects with an increase in the intensity and severity of convulsions.[61] Depersonalisation has also been reported as a benzodiazepine withdrawal effect from nitrazepam.[62]
Special precautions
Benzodiazepines require special precaution if used in the alcohol or drug dependent individuals and individuals with comorbid psychiatric disorders.[27] It has been recommended that caution should be exercised in prescribing nitrazepam to anyone who is of working age due to the significant impairment of psychomotor skills; This impairment is greater the higher the dosage that is prescribed.[63] Nitrazepam in doses of 5 mg or more causes significant deterioration in vigilance performance combined with increased feelings of sleepiness.[64] Doses as low as 5 mg of nitrazepam can impair driving skills.[14] Therefore people driving or conducting activities which require vigilance should exercise caution in using nitrazepam or possibly avoid it all together.[65]
Elderly
Nitrazepam, similar to other benzodiazepines and nonbenzodiazepines causes impairments in body balance and standing steadiness in individuals who wake up at night or the next morning. Falls and hip fractures are frequently reported. The combination with alcohol increases these impairments. Partial, but incomplete tolerance develops to these impairments.[16] Nitrazepam has been found to be dangerous in elderly patients due to a significant increased risk of falls.[66] This increased risk is probably due to the persisting drug effects of nitrazepam well into the next day.[67] Nitrazepam is a particularly unsuitable hypnotic for the elderly as it induces a disability characterised by general mental deterioration, inability to walk, incontinence, dysarthric, confusion, prone to stumbling, falls, and disoriention which can occur from doses as low as 5 mg. The nitrazepam induced symptomatology can lead to a misdiagnosis of brain disease in the elderly, for example dementia and can also lead to the symptoms of postural hypotension which may also get misdiagnosed. It was reported that a geriatric unit was seeing as many as 7 patients a month with nitrazepam induced disabilities and health problems. It was recommended that nitrazepam should join the barbiturates in not being prescribed to the elderly.[68] Only nitrazepam and lorazepam were found to increase the risk of falls and fractures in the elderly.[69] CNS depression occurs much more frequently in the elderly and is especially common in doses above 5 mg of nitrazepam.[70] Both young and old patients report sleeping better after three nights use of nitrazepam however they also report feeling less awake and are slower on psychomotor testing up to 36 hours after intake of nitrazepam. The elderly showed cognitive deficits, making significantly more mistakes in psychomotor testing than younger patients despite similar plasma levels of the drug, suggesting that the elderly are more sensitive to nitrazepam due to increased sensitivity of the aging brain to nitrazepam. Confusion and disorientation can result from chronic nitrazepam administration to elderly subjects. Also the effects of a single dose of nitrazepam may last up to 60 hours after administration.[71]
Children
Nitrazepam is not recommended for use in those under eighteen years of age. Use in very young children may be especially dangerous. Children treated with nitrazepam for epilepsies may develop tolerance within months of continued use, with dose escalation often occurring with prolonged use. Sleepiness, deterioration in motor skills and ataxia were common side effects in children with tuberous sclerosis treated with nitrazepam. The side effects of nitrazepam may impair the development of motor and cognitive skills in children treated with nitrazepam. Withdrawal of nitrazepam only occasionally resulted in a return of seizures and some children withdrawn from nitrazepam appeared to improve. Development, for example, able to walk at five years was impaired in many children taking nitrazepam but was not impaired with several other non benzodiazepine antiepileptic agents. It has been recommended that children being treated with nitrazepam should be reviewed and have their nitrazepam gradually discontinued whenever appropriate.[7] Excess sedation, hypersalivation, swallowing difficulty, high incidence of aspiration pneumonia as well as several deaths has been associated with nitrazepam therapy in children.[32]
Pregnancy
The use of nitrazepam during pregnancy can lead to intoxication of the new born. A neonatal withdrawal syndrome can also occur if nitrazepam or other benzodiazepines are used during pregnancy with symptoms such as hyper-excitability, tremor and gastro-intestinal upset (diarrhea or vomiting) occurring. Breast feeding by mothers using nitrazepam is not recommended.[72] Nitrazepam is a long acting benzodiazepine and there is a risk of drug accumulation, even though no active metabolites are formed during metabolism. Accumulation can occur in various body organs including the heart, accumulation is even greater in babies. Nitrazepam rapidly crosses the placenta and also is present in breast milk in high quantities. Therefore benzodiazepines including nitrazepam should be avoided during pregnancy.[73] In early pregnancy nitrazepam levels are lower in the baby than in the mother and in the later stages of pregnancy nitrazepam is found in equal levels in both the mother and the unborn child.[74] Internationally benzodiazepines are known to cause harm when used during pregnancy and nitrazepam is a category D drug during pregnancy.
Benzodiazepines are lipophilic and rapidly penetrate membranes and therefore rapidly penetrate the placenta with significant uptake of the drug. Use of benzodiazepines such as nitrazepam in late pregnancy especially high doses may result in floppy infant syndrome.[75] Use in the third trimester stage of pregnancy may result in the development of a severe benzodiazepine withdrawal syndrome in the neonate. Withdrawal symptoms from benzodiazepines in the neonate may include hypotonia, and reluctance to suck, to apnoeic spells, cyanosis, and impaired metabolic responses to cold stress. These symptoms may persist for hours or months after birth.[26]
Other precautions
Caution in hypotension.
Caution in those suffering from hypotension, nitrazepam may worsen hypotension.[45]
Caution in hypothyroidism.
Caution should be exercised by people who have hypothyroidism as this condition may cause a long delay in the metabolism of nitrazepam leading to significant drug accumulation.[76]
Contraindications
Nitrazepam should be avoided in patients with chronic obstructive pulmonary disease (COPD), especially during acute exacerbations of COPD, because serious respiratory depression may occur in patients who are receiving hypnotics.[77]
As with other hypnotic drugs nitrazepam is associated with an increased risk of road traffic accidents.[15] Nitrazepam is recommended to be avoided in patients who drive or operate machinery. A study assessing driving skills of sedative hypnotic users found that users of nitrazepam were found to be significantly impaired up to 17 hours after dosing, whereas users of temazepam did not show significant impairments of driving ability. These results reflect the long acting nature of nitrazepam.[78]
Toxicity
Humans
The Journal of Clinical Sleep Medicine published a paper which had carried out a systematic review of the medical literature concerning insomnia medications and raised concerns about benzodiazepine receptor agonist drugs, the benzodiazepines and the Z-drugs that are used as hypnotics in humans. The review found that almost all trials of sleep disorders and drugs are sponsored by the pharmaceutical industry. It was found that the odds ratio for finding results favorable to industry in industry-sponsored trials was 3.6 times higher than non-industry-sponsored studies and that 24% of authors did not disclose being funded by the drug companies in their published paper when they were funded by the drug companies. The paper found that there is little research into hypnotics that is independent from the drug manufacturers. Also of concern was the lack of focus in industry sponsored trials on their own results showing that use of hypnotics is correlated with depression. The author was concerned that there is no discussion of adverse effects of benzodiazepine agonist hypnotics discussed in the medical literature such as significant increased levels of infection, cancers and increased mortality in trials of hypnotic drugs and an overemphasis on the positive effects. No hypnotic manufacturer has yet tried to refute the epidemiology data that shows that use of their product is correlated with excess mortality. The author stated that "major hypnotic trials is needed to more carefully study potential adverse effects of hypnotics such as daytime impairment, infection, cancer, and death and the resultant balance of benefits and risks." The author concluded that more independent research into daytime impairment, infection, cancer, and shortening of lives of sedative hypnotic users is needed to find the true balance of benefits and risks of benzodiazepine agonist hypnotic drugs in the treatment of insomnia.[13] Chronic use of benzodiazepines seemed to cause significant immunological disorders in a study of selected outpatients attending a psychopharmacology department.[12]
Cancer
Benzodiazepine usage for more than one to six months at prescribed doses is associated with an increased risk of the development of ovarian cancer.[79] There have been fifteen epidemiologic studies which have shown that hypnotic drug use is associated with increased mortality, mainly due to increased cancer deaths in humans. The cancers included cancer of the brain, lung, bowel, breast, and bladder, and other neoplasms. Not only are benzodiazepines associated with an increased risk of cancer, the benzodiazepine receptor agonist Z-drugs also are associated with cancer in humans in these studies. Initially U.S. Food and Drug Administration (FDA) reviewers did not want to approve the Z-drugs due to concerns of cancer but ultimately changed their mind and approved the drugs despite the concerns. The data shows that trial subjects receiving hypnotic drugs had an increased the risk of developing cancer. The review author concluded saying; "the likelihood of cancer causation is sufficiently strong now that physicians and patients should be warned that hypnotics possibly place patients at higher risk for cancer".[80]
Mortality
Nitrazepam therapy compared with other drug therapies increases risk of death when used for intractable epilepsy in an analysis of 302 patients. The risk of death from nitrazepam therapy may be greater in younger patients (children below 3.4 years in the study) with intractable epilepsy. In older children (above 3.4 years) the tendency appears to be reversed in this study.[81] Nitrazepam may cause sudden death in children. Nitrazepam therapy can cause swallowing incoordination, high-peaked esophageal peristalsis, bronchospasm, delayed cricopharyngeal relaxation and severe respiratory distress necessitating ventilatory support in children. Nitrazepam may promote the development of parasympathetic overactivity or vagotonia leading to potentially fatal respiratory distress in children.[82]
Liver
Nitrazepam has been associated with severe hepatic disorders, similar to other nitrobenzodiazepines. Nitrobenzodiazepines such as nitrazepam, nimetazepam, flunitrazepam, and clonazepam are more toxic to the liver than other benzodiazepines as they are metabolically activated by CYP3A4 which can result in cytotoxicity. This activation can lead to the generation of free radicals, oxidation of thiol as well as covalent binding with endogenous macromolecules; this results then in oxidation of cellular components or inhibition of normal cellular function. Metabolism of a non-toxic drug to reactive metabolites is has been connected with causing a variety of adverse reactions.[48]
Long-term effects
Long-term effects of benzodiazepine drugs such as nitrazepam include worsening mental and physical health as well as cognitive deficits. These adverse effects show improvement after a period of abstinence.[10][11]
Interactions
Nitrazepam interacts with the antibiotic erythromycin which is a strong inhibitor of CYP3A4, which affects concentration peak time. This interaction is not to believed to be clinically important.[83] However, anxiety, tremor and depression have been documented in a case report following administration of nitrazepam and triazolam. Following administration of erythromycin to the patient, repetitive hallucinations and abnormal bodily sensations developed. The patient had however acute pneumonia and renal failure. Co-administration of benzodiazepine drugs at therapeutic doses with erythromycin may cause serious psychotic symptoms especially in those with other significant physical complications.[84] Oral contraceptive pills, reduce the clearance of nitrazepam which may lead to increased plasma levels of nitrazepam and accumulation.[85] Rifampin increases the clearance of nitrazepam significantly and probenecid decreases the clearance of nitrazepam significantly.[86] Cimetidine slows down the elimination rate of nitrazepam leading to more prolonged effects of nitrazepam and increased risk of accumulation.[87] Alcohol (ethanol) in combination with nitrazepam may cause a synergistic enhancement of the hypotensive properties of both benzodiazepines and alcohol.[88] Benzodiazepines including nitrazepam may inhibit the glucuronidation of morphine leading to increased levels of and prolongation of the effects of morphine in rat experiments.[89]
Pharmacology
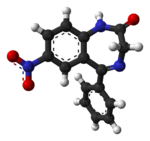
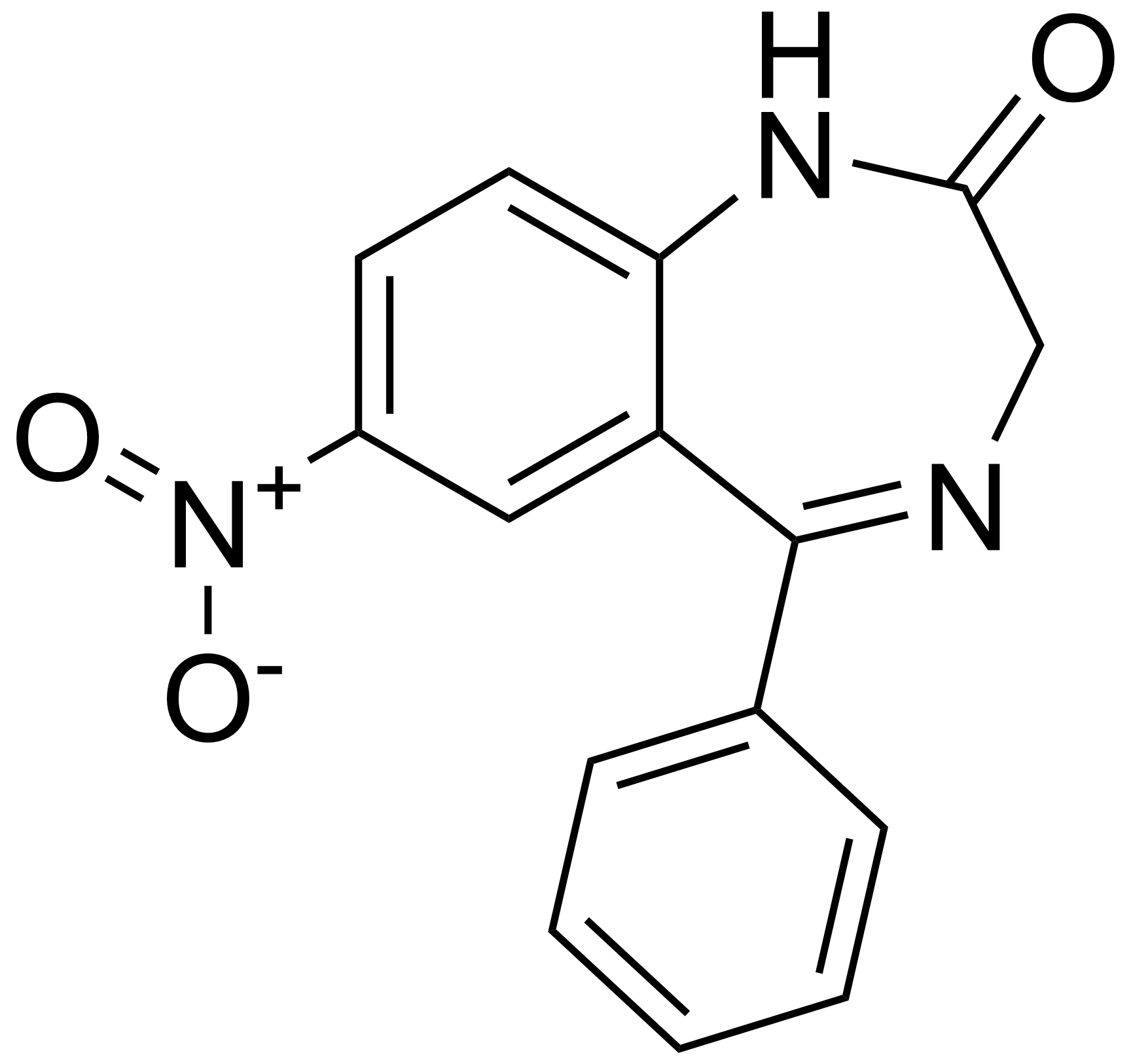
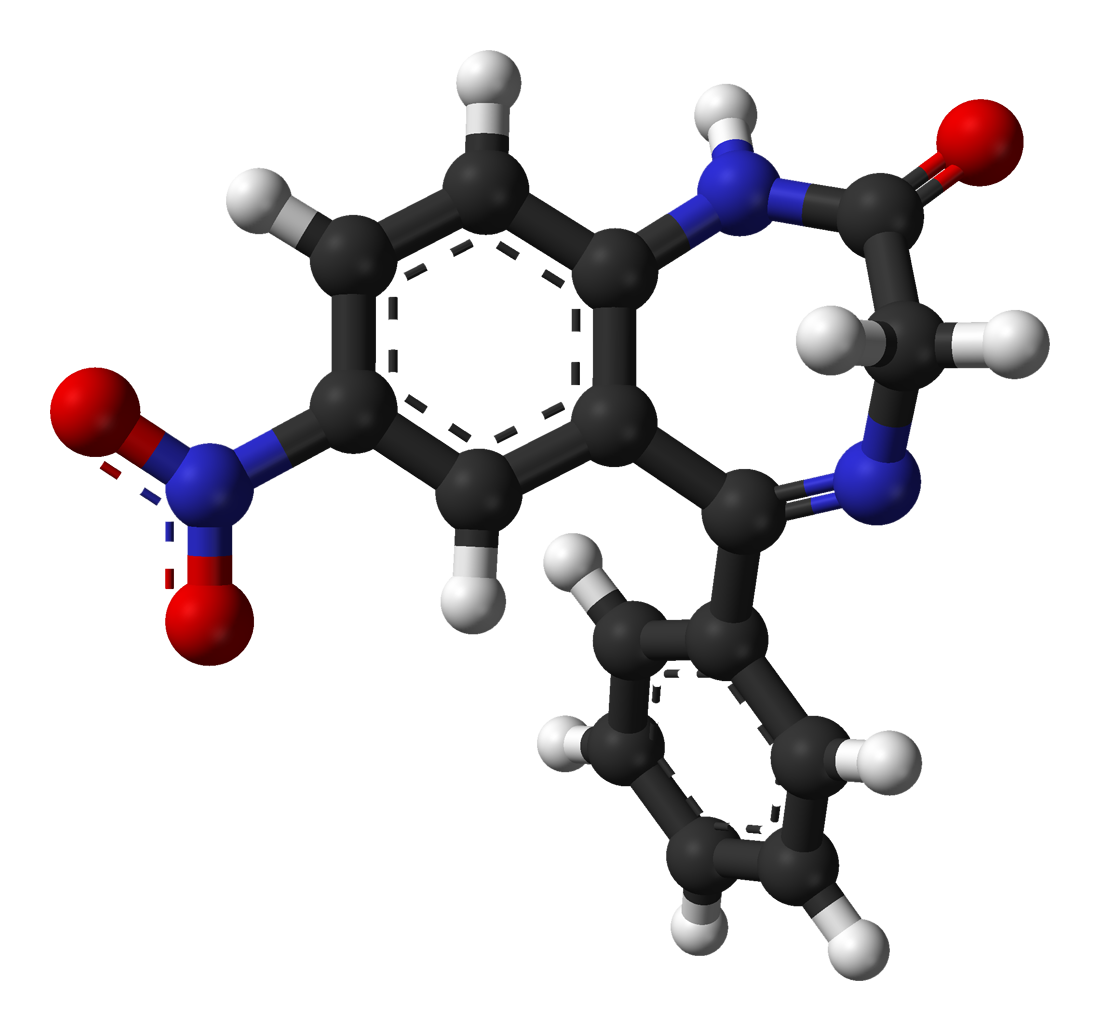
Nitrazepam is a nitrobenzodiazepine.[90][91] It is a 1,4 benzodiazepine, with the chemical name 1,3-Dihydro-7-nitro-5-phenyl-2H-1,4- benzodiazepin-2-one.
It is long acting, is lipophilic and is metabolised hepatically via oxidative pathways. It acts on benzodiazepine receptors in the brain which are associated with the GABA receptors, causing an enhanced binding of GABA (gamma-aminobutyric acid) to GABAA receptors.[92] GABA is a major inhibitory neurotransmitter in the brain, involved in inducing sleepiness, muscular relaxation and control of anxiety and seizures, and slows down the central nervous system. The mechanism of action of nitrazepam is the same as other benzodiazepine drugs and zopiclone.[93] The anticonvulsant properties of nitrazepam and other benzodiazepines may be in part or entirely due to binding to voltage-dependent sodium channels rather than benzodiazepine receptors. Sustained repetitive firing seems to be limited by benzodiazepines effect of slowing recovery of sodium channels from inactivation in mouse spinal cord cell cultures.[94] The muscle relaxant properties of nitrazepam are produced via inhibition of polysynaptic pathways in the spinal cord of decerebrate cats.[95] It is a full agonist of the benzodiazepine receptor.[96] The endogenous opioid system may play a role in some of the pharmacological properties of nitrazepam in rats.[97] Nitrazepam causes a decrease in the cerebral contents of the amino acids glycine and alanine in the mouse brain. The decrease may be due to activation of benzodiazepine receptors.[98] At high doses decreases in histamine turnover occur as a result of nitrazepam's action at the benzodiazepine-GABA receptor complex in mouse brain.[99] Nitrazepam has demonstrated cortisol suppressing properties in man.[100] Nitrazepam is an agonist for both central benzodiazepine receptors, and to the peripheral type benzodiazepine receptors found in rat neuroblastoma cells.[101]
EEG and sleep
In sleep laboratory studies, nitrazepam decreased sleep onset latency. In psychogeriatric in-patients nitrazepam was found to be no more effective than placebo tablets in increasing total time spent asleep, was found to significantly impair trial subjects abilities to move and carry out everyday activities the next day and it was concluded that nitrazepam should not be used as a sleep aid in psychogeriatric in-patients.[102]
Stage 2 NREM sleep is significantly increased by nitrazepam but SWS stage sleep is significantly decreased by nitrazepam.[103] There is delay in the onset, and decrease in the duration of REM sleep. Following discontinuation of the drug, REM sleep rebound has been reported in some studies.[104] Nitrazepam is reported to significantly affect stages of sleep; a decrease stage 1, 3, and 4 sleep and to increase stage 2.[105] In young volunteers the pharmacological properties of nitrazepam was found to produce sedation, impaired psychomotor performance and standing steadiness. EEG tests showed a decrease of alpha activity and increased the beta activity. These effects increased according to blood plasma levels of nitrazepam.[106] Performance was significantly impaired 13 hours after dosing with nitrazepam as was decision-making skills. EEG tests show more drowsiness and light sleep 18 hours after nitrazepam intake more so than amylobarbitone. Fast activity was recorded via EEG 18 hours after nitrazepam dosing.[107] An animal study demonstrated that nitrazepam induces a drowsy pattern of spontaneous EEG including high-voltage slow waves and spindle bursts increase in the cortex and amygdala, while the hippocampal theta rhythm is desynchronized. Also low-voltage fast waves occur particularly in the cortical EEG. The EEG arousal response to auditory stimulation and to electric stimulation of the mesencephalic reticular formation, posterior hypothalamus and centromedian thalamus is significantly suppressed. The photic driving response elicited by a flash light in the visual cortex is also suppressed by nitrazepam. Estazolam was found to be more potent however.[108] Nitrazepam increases the slow wave light sleep (SWLS) in a dose-dependent manner whilst suppressing deep sleep stages. Less time is spent in stages 3 and 4 which are the deep sleep stages, when benzodiazepines such as nitrazepam are used. Benzodiazepines are therefore not good hypnotics in the treatment of insomnia. The suppression of deep sleep stages by benzodiazepines may be especially problematic to the elderly as they naturally spend less time in the deep sleep stage.[109]
Pharmacokinetics
Nitrazepam is largely bound to plasma proteins.[110] Benzodiazepines such as nitrazepam are lipid soluble and have a high cerebral uptake.[111] The time for nitrazepam to reach peak plasma concentrations following oral administration is about 2 hours (0.5 to 5 hours). The half-life of nitrazepam is 16.5 to 48.3 (mean 28.8) hours. Both low dose (5 mg) and high dose (10 mg) of nitrazepam significantly increases growth hormone levels in humans.[112] Nitrazepam's half-life in the cerebrospinal fluid, 68 hours, indicates that nitrazepam is eliminated extremely slowly from the cerebrospinal fluid.[113] Nitrazepam has a half-life of about 29 hours in young people and a much longer half-life in the elderly. In the elderly the half-life is about 40 hours.[17][18] Concomitant food intake has no influence on the rate of absorption of nitrazepam nor on its bioavailability. Therefore nitrazepam can be taken with or without food.[114]
Abuse potential
See also: Benzodiazepine drug misuseNitrazepam is a drug which is very frequently involved in drug intoxication.[115] Nitrazepam was the most commonly detected benzodiazepine in urine samples in the UK in 1997 suggesting a high liking and preference amongst drug abusers. However, it has been superseded by temazepam, despite the fact that temazepam is much more highly regulated in the UK.[23][24] Apart from nicotine and alcohol in Nepal in 1996 nitrazepam was a major drug of abuse among young adults as was codeine cough syrup, heroin, buprenorphine and cannabis.[25]
Nitrazepam in animal studies has been shown to increase reward seeking which may suggest increased risk of addictive behavioural patterns in rats.[116] A study found that nitrazepam caused significant euphoria as against placebos and was identified as an active drug by freshly detoxified experienced drug abusers of heroin and other drugs. Nitrazepam resembled diazepam (Valium), however, on certain parameters the effects produced by nitrazepam were more pronounced in these drug abusers. Nitrazepam was found to be an abusable drug and has similar abuse liability like diazepam, if not slightly higher in these drug abusers. Nitrazepam in drug abusers produces effects including feeling energetic, relaxed, drunken, talkative, pleasure and euphoria. In India up to 50-60% of heroin addicts abuse benzodiazepines and 20% of injecting substance misusers also inject benzodiazepines.[117]
Treatment with nitrazepam should usually not exceed seven to ten consecutive days. Use for more than two to three consecutive weeks requires complete re-evaluation of the patient. Prescriptions for nitrazepam should be written for short-term use (seven to ten days) and it should not be prescribed in quantities exceeding a one month supply. Dependence can occur in as little as four weeks.[118]
Benzodiazepines, including diazepam, nitrazepam, and flunitrazepam account for the largest volume of forged drug prescriptions in Sweden, a total of 52% of drug forgeries being for benzodiazepines, suggesting benzodiazepines are a major prescription drug class of abuse.[119] In Bangladesh, benzodiazepines, including nitrazepam, are used in organised crime to commit drug facilitated crime such as robbery.[120]
Nitrazepam and other benzodiazepines are detected frequently in cases of people suspected of driving under the influence of drugs in Sweden. Other benzodiazepines and zolpidem and zopiclone are also found in high numbers in suspected impaired drivers. Many drivers have blood levels far exceeding the therapeutic dose range suggesting a high degree of abuse potential for benzodiazepines and zolpidem and zopiclone.[121] In Northern Ireland in cases where drugs were found in tests on impaired drivers, benzodiazepines were found to be present in 87% of cases.[122][123] In Norway benzodiazepines are the most commonly detected illicit drug in suspected drugged drivers being detected in 38-57 percent of drivers.[124]
Overdose
Nitrazepam overdose may result in stereotypical symptoms of benzodiazepine overdose including intoxication, impaired balance and slurred speech. In cases of severe overdose this may progress to a comatose state with the possibility of death. The risk of nitrazepam overdose is increased significantly if nitrazepam is abused in conjunction with opioids, as was highlighted in a review of deaths of users of the opioid buprenorphine.[125] Nitrobenzodiazepines such as nitrazepam can result in a severe neurological effects.[126] Nitrazepam taken in overdose is associated with a high level of congenital abnormalities (30 percent of births). Most of the congentital abnormalities were mild deformaties.[22]
Severe nitrazepam overdose resulting in coma causes the central somatosensory conduction time (CCT) after median nerve stimulation to be prolonged and the N20 to be dispersed. Brain-stem auditory evoked potentials demonstrate delayed interpeak latencies (IPLs) I-III, III-V and I-V. Toxic overdoses therefore of nitrazepam cause prolonged CCT and IPLs. An alpha pattern coma can be a feature of nitrazepam overdose with alpha patterns being most prominent in the frontal and central regions of the brain.[127][128]
Benzodiazepines were implicated in 39% of suicides by drug poisoning in Sweden, with nitrazepam and flunitrazepam accounting for 90% of benzodiazepine implicated suicides, in the elderly over a period of 2 decades. In three quarters of cases death was due to drowning, typically in the bath. Benzodiazepines were the predominant drug class in suicides in this review of Swedish death certificates. In 72% of the cases benzodiazepines were the only drug consumed. Benzodiazepines and in particular nitrazepam and flunitrazepam should therefore be prescribed with caution in the elderly.[21] In a brain sample of a fatal nitrazepam poisoning high concentrations of nitrazepam and its metabolite were found in the brain of the deceased person.[129]
In a retrospective study of deaths, when benzodiazepines were implicated in the deaths, the benzodiazepines nitrazepam and flunitrazepam were the most common benzodiazepines involved. Benzodiazepines were a factor in all deaths related to drug addiction in this study of causes of deaths. Nitrazepam and flunitrazepam were significantly more commonly implicated in suicide related deaths than natural deaths. In four of the cases benzodiazepines alone were the only cause of death.[19] In Australia, nitrazepam and temazepam were the benzodiazepines most commonly detected in overdose drug related deaths. In a third of cases benzodiazepines were the sole cause of death.[20]
Individuals with chronic illnesses are much more vulnerable to lethal overdose with nitrazepam, as fatal overdoses can occur at relatively low doses in these individuals.[130]
See also
- Benzodiazepine
- Benzodiazepine dependence
- Benzodiazepine withdrawal syndrome
- Long term effects of benzodiazepines
- Nimetazepam
- Temazepam
- Flunitrazepam
External links
References
- ^ US Patent 3141890
- ^ "Benzodiazepine Names". non-benzodiazepines.org.uk. http://www.non-benzodiazepines.org.uk/benzodiazepine-names.html. Retrieved 2008-12-29.
- ^ Yasui M; Kato A, Kanemasa T, Murata S, Nishitomi K, Koike K, Tai N, Shinohara S, Tokomura M, Horiuchi M, Abe K (June 2005). "[Pharmacological profiles of benzodiazepinergic hypnotics and correlations with receptor subtypes]". Nihon Shinkei Seishin Yakurigaku Zasshi 25 (3): 143–51. PMID 16045197.
- ^ a b Griffiths AN; Tedeschi G, Richens A (1986). "The effects of repeated doses of temazepam and nitrazepam on several measures of human performance". Acta Psychiatrica Scandinavica. Supplementum 332: 119–26. doi:10.1111/j.1600-0447.1986.tb08988.x. PMID 2883819.
- ^ a b Cook PJ; Huggett A, Graham-Pole R, Savage IT, James IM (January 8, 1983). "Hypnotic accumulation and hangover in elderly inpatients: a controlled double-blind study of temazepam and nitrazepam". Br Med J (Clin Res Ed) 286 (6359): 100–2. doi:10.1136/bmj.286.6359.100. PMC 1546430. PMID 6129914. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1546430.
- ^ a b Loiseau P (1983). "[Benzodiazepines in the treatment of epilepsy]". Encephale 9 (4 Suppl 2): 287B–292B. PMID 6373234.
- ^ a b c Dennis J; Hunt A (September 14, 1985). "Prolonged use of nitrazepam for epilepsy in children with tuberous sclerosis". Br Med J (Clin Res Ed) 291 (6497): 692–3. doi:10.1136/bmj.291.6497.692. PMC 1416679. PMID 3929902. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1416679.
- ^ a b Hecker R; Burr M, Newbury G (1992). "Risk of benzodiazepine dependence resulting from hospital admission". Drug Alcohol Rev 11 (2): 131–5. doi:10.1080/09595239200185601. PMID 16840267.
- ^ a b Străulea, AO.; Chiriţă, V. (July–September 2009). "[The withdrawal syndrome in benzodiazepine dependence and its management]". Rev Med Chir Soc Med Nat Iasi 113 (3): 879–84. PMID 20191849.
- ^ a b Ashton H (2005). "The diagnosis and management of benzodiazepine dependence" (PDF). Curr Opin Psychiatry 18 (3): 249–55. doi:10.1097/01.yco.0000165594.60434.84. PMID 16639148. http://www.benzo.org.uk/amisc/ashdiag.pdf.
- ^ a b Ashton H (2004). "Benzodiazepine dependence". In Haddad P, Dursun S, Deakin B (eds.). Adverse Syndromes and Psychiatric Drugs: A Clinical Guide. Oxford University Press. pp. 239–60. ISBN 978-0198527480.
- ^ a b Lechin F; van der Dijs B, Vitelli-Flores G, Báez S, Lechin ME, Lechin AE, Orozco B, Rada I, León G, Jiménez V (February 1994). "Peripheral blood immunological parameters in long-term benzodiazepine users". Clin Neuropharmacol 17 (1): 63–72. doi:10.1097/00002826-199402000-00007. PMID 7908607.
- ^ a b Kripke DF (December 15, 2007). "Who should sponsor sleep disorders pharmaceutical trials?". J Clin Sleep Med 3 (7): 671–3. PMC 2556906. PMID 18198797. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2556906. "major hypnotic trials is needed to more carefully study potential adverse effects of hypnotics such as daytime impairment, infection, cancer, and death and the resultant balance of benefits and risks."
- ^ a b Törnros J; Laurell H (July 1990). "Acute and carry-over effects of brotizolam compared to nitrazepam and placebo in monotonous simulated driving". Pharmacol Toxicol 67 (1): 77–80. doi:10.1111/j.1600-0773.1990.tb00786.x. PMID 2395820.
- ^ a b Gustavsen, I.; Bramness, JG.; Skurtveit, S.; Engeland, A.; Neutel, I.; Mørland, J. (Dec 2008). "Road traffic accident risk related to prescriptions of the hypnotics zopiclone, zolpidem, flunitrazepam and nitrazepam.". Sleep Med 9 (8): 818–22. doi:10.1016/j.sleep.2007.11.011. PMID 18226959.
- ^ a b Mets, MA.; Volkerts, ER.; Olivier, B.; Verster, JC. (Feb 2010). "Effect of hypnotic drugs on body balance and standing steadiness.". Sleep Med Rev 14 (4): 259–67. doi:10.1016/j.smrv.2009.10.008. PMID 20171127.
- ^ a b Kangas L; Iisalo E, Kanto J, Lehtinen V, Pynnönen S, Ruikka I, Salminen J, Sillanpää M, Syvälahti E (April 1979). "Human pharmacokinetics of nitrazepam: effect of age and diseases". Human pharmacokinetics of nitrazepam: effect of age and diseases 15 (3): 163–70. PMID 456400.
- ^ a b Vozeh S (November 21, 1981). "[Pharmacokinetic of benzodiazepines in old age]". Schweiz Med Wochenschr 111 (47): 1789–93. PMID 6118950.
- ^ a b Ericsson HR; Holmgren P, Jakobsson SW, Lafolie P, De Rees B (November 10, 1993). "[Benzodiazepine findings in autopsy material. A study shows interacting factors in fatal cases]". Läkartidningen 90 (45): 3954–7. PMID 8231567.
- ^ a b Drummer OH; Ranson DL (December 1996). "Sudden death and benzodiazepines". Am J Forensic Med Pathol 17 (4): 336–42. doi:10.1097/00000433-199612000-00012. PMID 8947361.
- ^ a b Carlsten, A; Waern M, Holmgren P, Allebeck P (2003). "The role of benzodiazepines in elderly suicides". Scand J Public Health 31 (3): 224–8. doi:10.1080/14034940210167966. PMID 12850977.
- ^ a b Gidai, J.; Acs, N.; Bánhidy, F.; Czeizel, AE. (Feb 2010). "Congenital abnormalities in children of 43 pregnant women who attempted suicide with large doses of nitrazepam.". Pharmacoepidemiol Drug Saf 19 (2): 175–82. doi:10.1002/pds.1885. PMID 19998314.
- ^ a b Professor C Heather Ashton (2002). "BENZODIAZEPINE ABUSE". Drugs and Dependence. Harwood Academic Publishers. http://www.benzo.org.uk/ashbzab.htm. Retrieved September 25, 2007.
- ^ a b Garretty DJ; Wolff K, Hay AW, Raistrick D (January 1997). "Benzodiazepine misuse by drug addicts". Annals of clinical biochemistry 34 (Pt 1): 68–73. PMID 9022890.
- ^ a b Chatterjee A; Uprety L, Chapagain M, Kafle K (1996). "Drug abuse in Nepal: a rapid assessment study". Bull Narc 48 (1-2): 11–33. PMID 9839033.
- ^ a b McElhatton PR (Nov-December 1994). "The effects of benzodiazepine use during pregnancy and lactation". Reprod Toxicol 8 (6): 461–75. doi:10.1016/0890-6238(94)90029-9. PMID 7881198.
- ^ a b Authier, N.; Balayssac, D.; Sautereau, M.; Zangarelli, A.; Courty, P.; Somogyi, AA.; Vennat, B.; Llorca, PM. et al. (Nov 2009). "Benzodiazepine dependence: focus on withdrawal syndrome.". Ann Pharm Fr 67 (6): 408–13. doi:10.1016/j.pharma.2009.07.001. PMID 19900604.
- ^ Janknegt R, van der Kuy A, Declerck G, Idzikowski C (August 1996). "Hypnotics. Drug selection by means of the System of Objectified Judgement Analysis (SOJA) method". Pharmacoeconomics 10 (2): 152–63. doi:10.2165/00019053-199610020-00007. PMID 10163418.
- ^ Tanaka, M.; Suemaru, K.; Watanabe, S.; Cui, R.; Li, B.; Araki, H. (Jul 2008). "Comparison of short- and long-acting benzodiazepine-receptor agonists with different receptor selectivity on motor coordination and muscle relaxation following thiopental-induced anesthesia in mice." (PDF). J Pharmacol Sci 107 (3): 277–84. doi:10.1254/jphs.FP0071991. PMID 18603831. http://www.jstage.jst.go.jp/article/jphs/107/3/277/_pdf.
- ^ Isojärvi, JI; Tokola RA (December 1998). "Benzodiazepines in the treatment of epilepsy in people with intellectual disability". J Intellect Disabil Res 42 (1): 80–92. PMID 10030438.
- ^ Djurić M; Marjanović B, Zamurović D (May–June 2001). "[West syndrome--new therapeutic approach]". Srp Arh Celok Lek 129 (1): 72–7. PMID 15637997.
- ^ a b Tsao, CY. (May 20, 2009). "Current trends in the treatment of infantile spasms." (PDF). Neuropsychiatr Dis Treat 5: 289–99. PMC 2695218. PMID 19557123. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2695218.
- ^ Mant A; Whicker SD, McManus P, Birkett DJ, Edmonds D, Dumbrell D (December 1993). "Benzodiazepine utilisation in Australia: report from a new pharmacoepidemiological database". Aust J Public Health 17 (4): 345–9. doi:10.1111/j.1753-6405.1993.tb00167.x. PMID 7911332.
- ^ Jacobson GA; Friesen WT, Peterson GM, Rumble RH, Polack AE (July 6, 1992). "Psychoactive drug prescribing in the Tasmanian community". Med J Aust 157 (1): 20–4. PMID 1353603.
- ^ Kayed K (March 30, 1995). "[Insomnia and hypnotics]". Tidsskr nor Laegeforen 115 (9): 1087–90. PMID 7725291.
- ^ Morgan K; Gilleard CJ, Reive A (November 1982). "Hypnotic usage in residential homes for the elderly: a prevalence and longitudinal analysis". Age Ageing 11 (4): 229–34. doi:10.1093/ageing/11.4.229. PMID 7180725.
- ^ Sanders LD; Yeomans WA, Rees J, Rosen M, Robinson JO (November 1988). "A double-blind comparison between nitrazepam, lorazepam, lormetazepam and placebo as preoperative night sedatives". Eur J Anaesthesiol 5 (6): 377–83. PMID 2907315.
- ^ Liljequist R; Mattila MJ (May 1979). "Acute effects of temazepam and nitrazepam on psychomotor skills and memory". Acta Pharmacol Toxicol (Copenh) 44 (5): 364–9. doi:10.1111/j.1600-0773.1979.tb02346.x. PMID 38627.
- ^ Nabeshima T; Tohyama K, Ichihara K, Kameyama T (November 1990). "Effects of benzodiazepines on passive avoidance response and latent learning in mice: relationship to benzodiazepine receptors and the cholinergic neuronal system". J Pharmacol Exp Ther 255 (2): 789–94. PMID 2173758.
- ^ Antkiewicz-Michaluk, L; Grabowska M, Baran L, Michaluk J (1975). "Influence of benzodiazepines on turnover of serotonin in cerebral structures in normal and aggressive rats". Arch Immunol Ther Exp (Warsz) 23 (6): 763–7. PMID 1241268.
- ^ Vermeeren A (2004). "Residual effects of hypnotics: epidemiology and clinical implications". CNS Drugs 18 (5): 297–328. doi:10.2165/00023210-200418050-00003. PMID 15089115.
- ^ Richens A; Mercer AJ, Jones DM, Griffiths A, Marshall RW (July 1993). "Effects of zolpidem on saccadic eye movements and psychomotor performance: a double-blind, placebo controlled study in healthy volunteers". British journal of clinical pharmacology 36 (1): 61–5. PMC 1364556. PMID 8373713. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1364556.
- ^ Morgan K (1985). "Effects of repeated dose nitrazepam and lormetazepam on psychomotor performance in the elderly". Psychopharmacology (Berl) 86 (1-2): 209–11. doi:10.1007/BF00431711. PMID 3927357.
- ^ Morgan K (1984). "Effects of two benzodiazepines on the speed and accuracy of perceptual-motor performance in the elderly". Psychopharmacology Suppl 1: 79–83. PMID 6147843.
- ^ a b Hossmann V; Maling TJ, Hamilton CA, Reid JL, Dollery CT (August 1980). "Sedative and cardiovascular effects of clonidine and nitrazepam". Clin Pharmacol Ther 28 (2): 167–76. doi:10.1038/clpt.1980.146. PMID 7398184.
- ^ Impallomeni M; Ezzat R (January 24, 1976). "Letter: Hypothermia associated with nitrazepam administration". Br Med J 1 (6003): 223–4. doi:10.1136/bmj.1.2665.223. PMC 1638481. PMID 1247796. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1638481.
- ^ MacLean H (February 24, 1973). "Nitrazepam: another interesting syndrome". Br Med J 1 (5851): 488. doi:10.1136/bmj.1.71.488. PMC 1588474. PMID 4689857. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1588474.
- ^ a b Mizuno, K.; Katoh, M.; Okumura, H.; Nakagawa, N.; Negishi, T.; Hashizume, T.; Nakajima, M.; Yokoi, T. (Feb 2009). "Metabolic activation of benzodiazepines by CYP3A4." (PDF). Drug Metab Dispos 37 (2): 345–51. doi:10.1124/dmd.108.024521. PMID 19005028. http://dmd.aspetjournals.org/content/37/2/345.full.pdf+html.
- ^ Szczawińska K; Cenajek-Musiał D, Nowakowska E, Chodera A (February 16, 1988). "Decrease in [3H]flunitrazepam receptor binding in rats tolerant to the effects of nitrazepam". European journal of pharmacology 147 (1): 7–11. doi:10.1016/0014-2999(88)90627-9. PMID 2836221.
- ^ Chodera A; Szczawińska K, Cenajek D, Nowakowska E (Jul-August 1984). "Pharmacokinetic aspects of habituation to benzodiazepines". Pol J Pharmacol Pharm 36 (4): 353–60. PMID 6152051.
- ^ Nowakowska E; Chodera A, Szczawińska K, Cenajek D (May–June 1983). "Development of tolerance to benzodiazepines I. Changes in the systems of central nervous system neurotransmitters during long-term administration of nitrazepam". Acta physiologica Polonica 34 (3): 345–51. PMID 6202092.
- ^ Garratt JC; Gent JP, Feely M, Haigh JR (January 5, 1988). "Can benzodiazepines be classified by characterising their anticonvulsant tolerance-inducing potential?". Eur J Pharmacol 145 (1): 75–80. doi:10.1016/0014-2999(88)90351-2. PMID 2894998.
- ^ Darcy L (August 19, 1972). "Delirium tremens following withdrawal of nitrazepam". Med J Aust 2 (8): 450. PMID 5086307.
- ^ Berezak A; Weber M, Hansmann J, Tulasne PA, Laporte B, Ould Ouali A (1984). "[Physical dependence on benzodiazepines in traumatology]". Ann Fr Anesth Reanim 3 (5): 383–4. PMID 6149713.
- ^ MacKinnon GL; Parker WA (1982). "Benzodiazepine withdrawal syndrome: a literature review and evaluation". The American journal of drug and alcohol abuse 9 (1): 19–33. doi:10.3109/00952998209002608. PMID 6133446.
- ^ Kales A; Scharf MB, Kales JD, Soldatos CR (April 20, 1979). "Rebound insomnia. A potential hazard following withdrawal of certain benzodiazepines". JAMA : the journal of the American Medical Association 241 (16): 1692–5. doi:10.1001/jama.241.16.1692. PMID 430730.
- ^ Hindmarch I (November 1977). "A repeated dose comparison of three benzodiazepine derivative (nitrazepam, flurazepam and flunitrazepam) on subjective appraisals of sleep and measures of psychomotor performance the morning following night-time medication". Acta Psychiatrica Scandinavica 56 (5): 373–81. doi:10.1111/j.1600-0447.1977.tb06678.x. PMID 22990.
- ^ Viukari M; Linnoila M, Aalto U (January 1978). "Efficacy and side effects of flurazepam, fosazepam, and nitrazepam as sleeping aids in psychogeriatric patients". Acta Psychiatrica Scandinavica 57 (1): 27–35. doi:10.1111/j.1600-0447.1978.tb06871.x. PMID 24980.
- ^ Nowakowska E; Chodera A, Cenajek-Musiał D, Szczawińska K (May–June 1987). "Differences in the development of tolerance to various benzodiazepines". Pol J Pharmacol Pharm 39 (3): 245–52. PMID 2894019.
- ^ Terao T; Tani Y (September 1, 1988). "[Two cases of psychotic state following normal-dose benzodiazepine withdrawal]". J UOEH 10 (3): 337–40. PMID 2902678.
- ^ Tagashira E; Hiramori T, Urano T, Nakao K, Yanaura S (October 1981). "Enhancement of drug withdrawal convulsion by combinations of phenobarbital and antipsychotic agents". Jpn J Pharmacol 31 (5): 689–99. doi:10.1254/jjp.31.689. PMID 6118452.
- ^ Terao T; Yoshimura R, Terao M, Abe K (January 15, 1992). "Depersonalization following nitrazepam withdrawal". Biol Psychiatry 31 (2): 212–3. doi:10.1016/0006-3223(92)90209-I. PMID 1737083.
- ^ Lahtinen U; Lahtinen A, Pekkola P (February 1978). "The effect of nitrazepam on manual skill, grip strength, and reaction time with special reference to subjective evaluation of effects on sleep". Acta Pharmacol Toxicol (Copenh) 42 (2): 130–4. doi:10.1111/j.1600-0773.1978.tb02180.x. PMID 343500.
- ^ Kozená L; Frantik E, Horváth M (May 1995). "Vigilance impairment after a single dose of benzodiazepines". Psychopharmacology (Berl) 119 (1): 39–45. doi:10.1007/BF02246052. PMID 7675948.
- ^ Hindmarch I; Parrott AC (1980). "The effects of combined sedative and anxiolytic preparations on subjective aspects of sleep and objective measures of arousal and performance the morning following nocturnal medication. I: Acute doses". Arzneimittelforschung 30 (6): 1025–8. PMID 6106498.
- ^ Shats V; Kozacov S (June 1, 1995). "[Falls in the geriatric department: responsibility of the care-giver and the hospital]". Harefuah 128 (11): 690–3. PMID 7557666.
- ^ Borland RG; Nicholson AN (February 1975). "Comparison of the residual effects of two benzodiazepines (nitrazepam and flurazepam hydrochloride) and pentobarbitone sodium on human performance". Br J Clin Pharmacol 2 (1): 9–17. PMC 1402497. PMID 10941. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1402497.
- ^ Evans JG; Jarvis EH (November 25, 1972). "Nitrazepam and the elderly". Br Med J 4 (5838): 487. doi:10.1136/bmj.4.5838.487-a. PMC 1786736. PMID 4653884. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1786736.
- ^ Trewin VF; Lawrence CJ, Veitch GB (April 1992). "An investigation of the association of benzodiazepines and other hypnotics with the incidence of falls in the elderly". J Clin Pharm Ther 17 (2): 129–33. doi:10.1111/j.1365-2710.1992.tb00750.x. PMID 1349894.
- ^ Greenblatt DJ; Allen MD (May 1978). "Toxicity of nitrazepam in the elderly: a report from the Boston Collaborative Drug Surveillance Program". British journal of clinical pharmacology 5 (5): 407–13. PMC 1429343. PMID 656280. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1429343.
- ^ Castleden CM; George CF, Marcer D, Hallett C (January 1, 1977). "Increased sensitivity to nitrazepam in old age". Br Med J 1 (6052): 10–2. doi:10.1136/bmj.1.157.10. PMC 1603636. PMID 318894. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1603636.
- ^ Serreau, R.; Collége national des gynécologues et obstétriciens; Société française de médecine périnatale; Société française de néonatalogie; Société française de anesthésie et de réanimation (Apr 2010). "[Drugs during preeclampsia. Fetal risks and pharmacology]". Ann Fr Anesth Reanim 29 (4): e37–46. doi:10.1016/j.annfar.2010.02.016. PMID 20347563.
- ^ Olive G; Dreux C (January 1977). "Pharmacologic bases of use of benzodiazepines in peréinatal medicine". Arch Fr Pediatr 34 (1): 74–89. PMID 851373.
- ^ Kangas L; Kanto J, Erkkola R (December 16, 1977). "Transfer of nitrazepam across the human placenta". Eur J Clin Pharmacol 12 (5): 355–7. doi:10.1007/BF00562451. PMID 598407.
- ^ Kanto JH (May 1982). "Use of benzodiazepines during pregnancy, labour and lactation, with particular reference to pharmacokinetic considerations". Drugs 23 (5): 354–80. doi:10.2165/00003495-198223050-00002. PMID 6124415.
- ^ Kenny RA; Kafetz K, Cox M, Timmers J, Impallomeni M (April 1984). "Impaired nitrazepam metabolism in hypothyroidism". Postgrad Med J 60 (702): 296–7. doi:10.1136/pgmj.60.702.296. PMC 2417841. PMID 6728755. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2417841.
- ^ Midgren B; Hansson L, Ahlmann S, Elmqvist D (1990). "Effects of single doses of propiomazine, a phenothiazine hypnotic, on sleep and oxygenation in patients with stable chronic obstructive pulmonary disease". Respiration 57 (4): 239–42. doi:10.1159/000195848. PMID 1982774.
- ^ O'Hanlon JF; Volkerts ER (1986). "Hypnotics and actual driving performance". Acta Psychiatrica Scandinavica Suppl 332: 95–104. doi:10.1111/j.1600-0447.1986.tb08985.x. PMID 3554901.
- ^ Harlow BL; Cramer DW (March 1995). "Self-reported use of antidepressants or benzodiazepine tranquilizers and risk of epithelial ovarian cancer: evidence from two combined case-control studies (Massachusetts, United States)". Cancer Causes Control 6 (2): 130–4. doi:10.1007/BF00052773. PMID 7749052.
- ^ Kripke, Daniel F (2008). "Evidence That New Hypnotics Cause Cancer" (PDF). Department of Psychiatry, UCSD (University of California). http://repositories.cdlib.org/cgi/viewcontent.cgi?article=1002&context=ucsdpsych. "the likelihood of cancer causation is sufficiently strong now that physicians and patients should be warned that hypnotics possibly place patients at higher risk for cancer."
- ^ Rintahaka PJ; Nakagawa JA, Shewmon DA, Kyyronen P, Shields WD (April 1999). "Incidence of death in patients with intractable epilepsy during nitrazepam treatment". Epilepsia 40 (4): 492–6. doi:10.1111/j.1528-1157.1999.tb00746.x. PMID 10219277.
- ^ Lim HC; Nigro MA, Beierwaltes P, Tolia V, Wishnow R (September 1992). "Nitrazepam-induced cricopharyngeal dysphagia, abnormal esophageal peristalsis and associated bronchospasm: probable cause of nitrazepam-related sudden death". Brain & development 14 (5): 309–14. PMID 1456385.
- ^ Luurila H; Olkkola KT, Neuvonen PJ (April 1995). "Interaction between erythromycin and nitrazepam in healthy volunteers". Pharmacol Toxicol 76 (4): 255–8. doi:10.1111/j.1600-0773.1995.tb00139.x. PMID 7617555.
- ^ Tokinaga N; Kondo T, Kaneko S, Otani K, Mihara K, Morita S (December 1996). "Hallucinations after a therapeutic dose of benzodiazepine hypnotics with co-administration of erythromycin". Psychiatry and clinical neurosciences 50 (6): 337–9. doi:10.1111/j.1440-1819.1996.tb00577.x. PMID 9014234.
- ^ Back DJ; Orme ML (June 1990). "Pharmacokinetic drug interactions with oral contraceptives". Clin Pharmacokinet 18 (6): 472–84. doi:10.2165/00003088-199018060-00004. PMID 2191822.
- ^ Brockmeyer NH; Mertins L, Klimek K, Goos M, Ohnhaus EE (September 1990). "Comparative effects of rifampin and/or probenecid on the pharmacokinetics of temazepam and nitrazepam". Int J Clin Pharmacol Ther Toxicol 28 (9): 387–93. PMID 2228325.
- ^ Ochs HR; Greenblatt DJ, Gugler R, Müntefering G, Locniskar A, Abernethy DR (August 1983). "Cimetidine impairs nitrazepam clearance". Clin Pharmacol Ther 34 (2): 227–30. doi:10.1038/clpt.1983.157. PMID 6872417.
- ^ Zácková P; Kvĕtina J, Nĕmec J, Nĕmcová J (December 1982). "Cardiovascular effects of diazepam and nitrazepam in combination with ethanol". Pharmazie 37 (12): 853–6. PMID 7163374.
- ^ Pacifici GM; Gustafsson LL, Säwe J, Rane A (April 1986). "Metabolic interaction between morphine and various benzodiazepines". Acta Pharmacol Toxicol (Copenh) 58 (4): 249–52. doi:10.1111/j.1600-0773.1986.tb00103.x. PMID 2872767.
- ^ Robertson MD; Drummer OH (May 1995). "Postmortem drug metabolism by bacteria". J Forensic Sci 40 (3): 382–6. PMID 7782744.
- ^ Danneberg P; Weber KH (1983). "Chemical structure and biological activity of the diazepines". Br J Clin Pharmacol 16 (Suppl 2): 231S–244S. PMC 1428206. PMID 6140944. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1428206.
- ^ Skerritt JH; Johnston GA (May 6, 1983). "Enhancement of GABA binding by benzodiazepines and related anxiolytics". Eur J Pharmacol 89 (3-4): 193–8. doi:10.1016/0014-2999(83)90494-6. PMID 6135616.
- ^ Sato K; Hong YL, Yang MS, Shibuya T, Kawamoto H, Kitagawa H (April 1985). "Pharmacologic studies of central actions of zopiclone: influence on brain monoamines in rats under stressful condition". Int J Clin Pharmacol Ther Toxicol 23 (4): 204–10. PMID 2860074.
- ^ McLean MJ; Macdonald RL (February 1988). "Benzodiazepines, but not beta carbolines, limit high frequency repetitive firing of action potentials of spinal cord neurons in cell culture". J Pharmacol Exp Ther 244 (2): 789–95. PMID 2450203.
- ^ Date SK; Hemavathi KG, Gulati OD (November 1984). "Investigation of the muscle relaxant activity of nitrazepam". Arch Int Pharmacodyn Ther 272 (1): 129–39. PMID 6517646.
- ^ Podhorna J; Krsiak M (2000). "Behavioural effects of a benzodiazepine receptor partial agonist, Ro 19-8022, in the social conflict test in mice". Behavioural pharmacology 11 (2): 143–51. PMID 10877119.
- ^ Nowakowska E; Chodera A (February 1991). "Studies on the involvement of opioid mechanism in the locomotor effects of benzodiazepines in rats". Pharmacology, biochemistry, and behavior 38 (2): 265–6. doi:10.1016/0091-3057(91)90276-8. PMID 1676167.
- ^ Tomono S; Kuriyama K (December 1985). "Effect of 450191-S, a 1H-1,2,4-triazolyl benzophenone derivative, on cerebral content of neuroactive amino acids". Jpn J Pharmacol 39 (4): 558–61. doi:10.1254/jjp.39.558. PMID 2869172.
- ^ Oishi R; Nishibori M, Itoh Y, Saeki K (May 27, 1986). "Diazepam-induced decrease in histamine turnover in mouse brain". Eur J Pharmacol 124 (3): 337–42. doi:10.1016/0014-2999(86)90236-0. PMID 3089825.
- ^ Christensen P; Lolk A, Gram LF, Kragh-Sørensen P (1992). "Benzodiazepine-induced sedation and cortisol suppression A placebo-controlled comparison of oxazepam and nitrazepam in healthy male volunteers". Psychopharmacology 106 (4): 511–6. doi:10.1007/BF02244823. PMID 1349754.
- ^ Watabe S; Yoshii M, Ogata N, Tsunoo A, Narahashi T (March 26, 1993). "Differential inhibition of transient and long-lasting calcium channel currents by benzodiazepines in neuroblastoma cells". Brain Res 606 (2): 244–50. doi:10.1016/0006-8993(93)90991-U. PMID 8387860.
- ^ Linnoila, M; Viukari M (June 1976). "Efficacy and side effects of nitrazepam and thioridazine as sleeping aids in psychogeriatric in-patients". British Journal of Psychiatry 128: 566–9. doi:10.1192/bjp.128.6.566. PMID 776314.
- ^ Nakazawa Y; Kotorii M, Oshima M, Horikawa S, Tachibana H (October 31, 1975). "Effects of thienodiazepine derivatives on human sleep as compared to those of benzodiazepine derivatives". Psychopharmacologia 44 (2): 165–71. doi:10.1007/BF00421005. PMID 709.
- ^ Adam K; Oswald I (July 1982). "A comparison of the effects of chlormezanone and nitrazepam on sleep". Br J Clin Pharmacol 14 (1): 57–65. PMC 1427586. PMID 7104168. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1427586.
- ^ Mizuki Y; Suetsugi M, Hotta H, Ushijima I, Yamada M (May 1995). "Stimulatory effect of butoctamide hydrogen succinate on REM sleep in normal humans". Prog Neuropsychopharmacol Biol Psychiatry 19 (3): 385–401. doi:10.1016/0278-5846(95)00020-V. PMID 7624490.
- ^ Tazaki T; Tada K, Nogami Y, Takemura N, Ishikawa K (1989). "Effects of butoctamide hydrogen succinate and nitrazepam on psychomotor function and EEG in healthy volunteers". Psychopharmacology (Berl) 97 (3): 370–5. doi:10.1007/BF00439453. PMID 2497487.
- ^ Malpas A; Rowan AJ, Boyce CR, Scott DF (June 27, 1970). "Persistent behavioural and electroencephalographic changes after single doses of nitrazepam and amylobarbitone sodium". Br Med J 2 (5712): 762–4. doi:10.1136/bmj.2.3382.762. PMC 1700857. PMID 4913785. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1700857.
- ^ Watanabe S; Ohta H, Sakurai Y, Takao K, Ueki S (July 1986). "[Electroencephalographic effects of 450191-S and its metabolites in rabbits with chronic electrode implants]". Nippon Yakurigaku Zasshi 88 (1): 19–32. doi:10.1254/fpj.88.19. PMID 3758874.
- ^ Noguchi H; Kitazumi K, Mori M, Shiba T (March 2004). "Electroencephalographic properties of zaleplon, a non-benzodiazepine sedative/hypnotic, in rats" (pdf). J Pharmacol Sci 94 (3): 246–51. doi:10.1254/jphs.94.246. PMID 15037809. http://www.jstage.jst.go.jp/article/jphs/94/3/246/_pdf.
- ^ Tokola RA; Neuvonen PJ (1983). "Pharmacokinetics of antiepileptic drugs". Acta neurologica Scandinavica Supplementum 97: 17–27. doi:10.1111/j.1600-0404.1983.tb01532.x. PMID 6143468.
- ^ Hertz MM; Paulson OB (May 1980). "Heterogeneity of cerebral capillary flow in man and its consequences for estimation of blood-brain barrier permeability". J Clin Invest 65 (5): 1145–51. doi:10.1172/JCI109769. PMC 371448. PMID 6988458. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=371448.
- ^ Kangas L; Kanto J, Syvälahti E (July 1977). "Plasma nitrazepam concentrations after an acute intake and their correlation to sedation and serum growth hormone levels". Acta Pharmacol Toxicol (Copenh) 41 (1): 65–73. doi:10.1111/j.1600-0773.1977.tb02124.x. PMID 331868.
- ^ Kangas L; Kanto J, Siirtola T, Pekkarinen A (July 1977). "Cerebrospinal-fluid concentrations of nitrazepam in man". Acta Pharmacol Toxicol (Copenh) 41 (1): 74–9. doi:10.1111/j.1600-0773.1977.tb02125.x. PMID 578380.
- ^ Holm V; Melander A, Wåhlin-Boll E (1982). "Influence of food and of age on nitrazepam kinetics". Drug-nutrient interactions 1 (4): 307–11. PMID 6926838.
- ^ Zevzikovas A; Kiliuviene G, Ivanauskas L, Dirse V (2002). "[Analysis of benzodiazepine derivative mixture by gas-liquid chromatography]". Medicina (Kaunas) 38 (3): 316–20. PMID 12474705.
- ^ Thiébot MH; Le Bihan C, Soubrié P, Simon P (1985). "Benzodiazepines reduce the tolerance to reward delay in rats". Psychopharmacology (Berl) 86 (1-2): 147–52. doi:10.1007/BF00431700. PMID 2862657.
- ^ PRAVIN SHANKER PRASAD; RAJAT RAY, RAKA JAIN, B.S.CHAVAN (2001). "ABUSE LIABILITY OF NITRAZEPAM: A STUDY AMONG EXPERIENCED DRUG USERS" (PDF). Indian Journal of Pharmacology (India: MedInd) 33: 357–362. http://medind.nic.in/ibi/t01/i5/ibit01i5p357.pdf.
- ^ "Mogadon". RxMed. http://www.rxmed.com/b.main/b2.pharmaceutical/b2.1.monographs/CPS-%20Monographs/CPS-%20(General%20Monographs-%20M)/MOGADON.html. Retrieved 26 May 2009.
- ^ Bergman U; Dahl-Puustinen ML (1989). "Use of prescription forgeries in a drug abuse surveillance network". Eur J Clin Pharmacol 36 (6): 621–3. doi:10.1007/BF00637747. PMID 2776820.
- ^ Majumder, MM.; Basher, A.; Faiz, MA.; Kuch, U.; Pogoda, W.; Kauert, GF.; Toennes, SW. (Aug 2008). "Criminal poisoning of commuters in Bangladesh: prospective and retrospective study.". Forensic Sci Int 180 (1): 10–6. doi:10.1016/j.forsciint.2008.06.016. PMID 18692332.
- ^ Jones AW; Holmgren A, Kugelberg FC (April 2007). "Concentrations of scheduled prescription drugs in blood of impaired drivers: considerations for interpreting the results". Ther Drug Monit 29 (2): 248–60. doi:10.1097/FTD.0b013e31803d3c04. PMID 17417081.
- ^ Cosbey SH (December 1986). "Drugs and the impaired driver in Northern Ireland: an analytical survey". Forensic Sci Int 32 (4): 245–58. doi:10.1016/0379-0738(86)90201-X. PMID 3804143.
- ^ Holmgren, A.; Holmgren, P.; Kugelberg, FC.; Jones, AW.; Ahlner, J. (Dec 2007). "Predominance of illicit drugs and poly-drug use among drug-impaired drivers in Sweden.". Traffic Inj Prev 8 (4): 361–7. doi:10.1080/15389580701329344. PMID 17994489.
- ^ Christophersen, AS.; Mørland, J. (Jun 2008). "Frequent detection of benzodiazepines in drugged drivers in Norway.". Traffic Inj Prev 9 (2): 98–104. doi:10.1080/15389580701869190. PMID 18398771.
- ^ Lai SH; Yao YJ, Lo DS (October 2006). "A survey of buprenorphine related deaths in Singapore". Forensic Sci Int 162 (1-3): 80–6. doi:10.1016/j.forsciint.2006.03.037. PMID 16879940.
- ^ Linwu, SW.; Syu, CJ.; Chen, YL.; Wang, AH.; Peng, FC. (Jul 2009). "Characterization of Escherichia coli nitroreductase NfsB in the metabolism of nitrobenzodiazepines.". Biochem Pharmacol 78 (1): 96–103. doi:10.1016/j.bcp.2009.03.019. PMID 19447228.
- ^ Carroll WM, Mastiglia FL (December 1977). "Alpha and beta coma in drug intoxication". Br Med J 2 (6101): 1518–9. doi:10.1136/bmj.2.6101.1518-a. PMC 1632784. PMID 589310. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1632784.
- ^ Rumpl E; Prugger M, Battista HJ, Badry F, Gerstenbrand F, Dienstl F (December 1988). "Short latency somatosensory evoked potentials and brain-stem auditory evoked potentials in coma due to CNS depressant drug poisoning. Preliminary observations". Electroencephalography and clinical neurophysiology 70 (6): 482–9. doi:10.1016/0013-4694(88)90146-0. PMID 2461282.
- ^ Moriya F; Hashimoto Y (January 28, 2003). "Tissue distribution of nitrazepam and 7-aminonitrazepam in a case of nitrazepam intoxication". Forensic Sci Int 131 (2-3): 108–12. doi:10.1016/S0379-0738(02)00421-8. PMID 12590048.
- ^ Brødsgaard I; Hansen AC, Vesterby A (June 1995). "Two cases of lethal nitrazepam poisoning". Am J Forensic Med Pathol 16 (2): 151–3. doi:10.1097/00000433-199506000-00015. PMID 7572872.
Anticonvulsants (N03) GABAA receptor agonist Clobazam • Clonazepam • Clorazepate • Diazepam# • Flutoprazepam • Lorazepam • Midazolam • Nimetazepam • Nitrazepam • TemazepamOther GABA agents Carbonic anhydrase inhibitor Channel blockers Primarily sodiumPrimarily calciumUnknown/ungroupedChannel openers PotassiumRetigabineIndirect GABA agents GABA transaminase inhibitor: Valproic acid# (Sodium valproate & Valproate semisodium) • Valpromide • Valnoctamide • Valproate pivoxil
GABA reuptake inhibitor: TiagabineUnknown/multiple/
unsortedPropionatesHypnotics/Sedatives (N05C) GABAA Agonists/PAMs Barbiturates: Allobarbital • Amobarbital • Aprobarbital • Barbital • Butabarbital • Butobarbital • Cyclobarbital • Ethallobarbital • Heptabarbital • Hexobarbital • Mephobarbital • Methohexital • Pentobarbital • Phenobarbital • Proxibarbal • Reposal • Secobarbital • Talbutal • Thiamylal • Thiopental • Vinbarbital • Vinylbital; Benzodiazepines: Brotizolam • Clonazepam • Cinolazepam • Climazolam • Doxefazepam • Estazolam • Flunitrazepam • Flurazepam • Flutoprazepam • Haloxazolam • Loprazolam • Lormetazepam • Midazolam • Nimetazepam • Nitrazepam • Quazepam • Temazepam • Triazolam; Carbamates: Carisoprodol • Ethinamate • Hexapropymate • Meprobamate • Methocarbamol • Procymate • Tybamate; Neuroactive Steroids: Acebrochol • Allopregnanolone • Alphadolone • Alphaxolone • Eltanolone • Ganaxolone • Hydroxydione • Minaxolone • Org 20599 • Org 21465 • Tetrahydrodeoxycorticosterone; Nonbenzodiazepines: CL-218,872 • Eszopiclone • Indiplon • JM-1232 • Lirequinil • Necopidem • Pazinaclone • ROD-188 • Saripidem • Suproclone • Suriclone • SX-3228 • U-89843A • U-90042 • Zaleplon • Zolpidem • Zopiclone; Phenols: Fospropofol • Propofol; Piperidinediones: Glutethimide • Methyprylon • Pyrithyldione • Piperidione; Quinazolinones: Afloqualone • Cloroqualone • Diproqualone • Etaqualone • Mebroqualone • Mecloqualone • Methaqualone • Methylmethaqualone • Nitromethaqualone; Others: 2-Methyl-2-butanol • Acetophenone • Acetylglycinamide chloral hydrate • Bromide (Lithium bromide, Potassium bromide, Sodium bromide) • Centalun • Chloral hydrate • Chloralose • Chloralodol • Clomethiazole • Dichloralphenazone • Ethanol (Alcohol) • Ethchlorvynol • Etomidate • Gaboxadol • Loreclezole • Methylpentynol • Metomidate • Paraldehyde • Petrichloral • Sulfonmethane • Trichloroethanol • Triclofos • Valerenic acid (Valerian)GABAB Agonists H1 Inverse agonists Antihistamines: Captodiame • Cyproheptadine • Dimenhydrinate • Diphenhydramine • Doxylamine • Hydroxyzine • Methapyrilene • Pheniramine • Promethazine • Propiomazine; Others: Tricyclic antidepressants (Amitriptyline, Doxepin, Trimipramine, etc.) • Tetracyclic antidepressants (Mianserin, Mirtazapine, etc.) • Typical antipsychotics (Chlorpromazine, Thioridazine, etc.) • Atypical antipsychotics (Olanzapine, Quetiapine, Risperidone, etc.)α1-Adrenergic Antagonists Mianserin • Niaprazine • Trazodone; Others: Tricyclic antidepressants (Amitriptyline, Doxepin, Trimipramine, etc.) • Typical antipsychotics (Chlorpromazine, Thioridazine, etc.) • Atypical antipsychotics (Olanzapine, Quetiapine, Risperidone, etc.)α2-Adrenergic Agonists 4-NEMD • Clonidine • Detomidine • Dexmedetomidine • Lofexidine • Medetomidine • Romifidine • Tizanidine • Xylazine5-HT2A Antagonists Eplivanserin • Niaprazine • Pruvanserin • Trazodone • Volinanserin; Others: Tricyclic antidepressants (Amitriptyline, Doxepin, Trimipramine, etc.) • Tetracyclic antidepressants (Mianserin, Mirtazapine, etc.) • Typical antipsychotics (Chlorpromazine, Thioridazine, etc.) • Atypical antipsychotics (Olanzapine, Quetiapine, Risperidone, etc.)Melatonin Agonists Orexin Antagonists Others Acecarbromal • Apronal • Bromisoval • Cannabidiol (Cannabis) • Carbromal • Embutramide • Evoxine • Fenadiazole • Gabapentin • Kavalactones (Kava) • Mephenoxalone • Opiates/Opioids (Hydrocodone, Morphine (Opium), etc.) • Passion flower • Scopolamine (Mandrake) • ValnoctamideCategories:- Nitrobenzodiazepines
- Lactams
- InChI=1S/C15H11N3O3/c19-14-9-16-15(10-4-2-1-3-5-10)12-8-11(18(20)21)6-7-13(12)17-14/h1-8H,9H2,(H,17,19)

Wikimedia Foundation. 2010.