- Isoniazid
-
Isoniazid 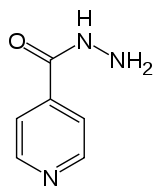
Systematic (IUPAC) name isonicotinohydrazide Clinical data AHFS/Drugs.com monograph MedlinePlus a682401 Pregnancy cat. C Legal status prescription only (US) Routes oral, intramuscular, intravenous Pharmacokinetic data Protein binding Very low (0-10%) Metabolism liver; CYP450: 2C19, 3A4 inhibitor Half-life 0.5-1.6h (fast acetylators), 2-5h (slow acetylators) Excretion urine (primarily), feces Identifiers CAS number 54-85-3 
ATC code J04AC01 PubChem CID 3767 DrugBank APRD01055 ChemSpider 3635 UNII V83O1VOZ8L KEGG D00346 ChEBI CHEBI:6030 ChEMBL CHEMBL64 Chemical data Formula C6H7N3O Mol. mass 137.139 g/mol SMILES eMolecules & PubChem - InChI=1S/C6H7N3O/c7-9-6(10)5-1-3-8-4-2-5/h1-4H,7H2,(H,9,10)
Key:QRXWMOHMRWLFEY-UHFFFAOYSA-N
 (what is this?) (verify)
(what is this?) (verify)Isoniazid (Laniazid, Nydrazid), also known as isonicotinylhydrazine (INH), is an organic compound that is the first-line antituberculosis medication in prevention and treatment. It was first discovered in 1912, and later in 1951 it was found to be effective against tuberculosis by inhibiting its mycolic acid (wax coat). Isoniazid is never used on its own to treat active tuberculosis because resistance quickly develops. Isoniazid also has an antidepressant effect, and it was one of the first antidepressants discovered. Isoniazid can also be used in the treatment of a BCG-oma.
The compound was first synthesised in the early 20th century,[1] but its activity against tuberculosis was first reported in the early 1950s and three pharmaceutical companies attempted unsuccessfully to simultaneously patent the drug[2] (the most prominent one being Roche, who launched their version, Rimifon, in 1952). With the introduction of isoniazid, a cure for tuberculosis was first considered reasonable.
Isoniazid is available in tablet, syrup, and injectable forms (given intramuscularly or intravenously). Isoniazid is available worldwide, is inexpensive and is generally well tolerated. It is manufactured from isonicotinic acid, which is produced from 4-methylpyridine.[3]
Contents
Preparation
Isoniazid may be prepared by the base hydrolysis of 4-cyanopyridine to give the amide, followed by displacement of ammonia by hydrazine:[4]
Mechanism of action
Isoniazid is a prodrug and must be activated by a bacterial catalase-peroxidase enzyme that in M. tuberculosis is called KatG.[5] KatG couples the isonicotinic acyl with NADH to form isonicotinic acyl-NADH complex. This complex binds tightly to the enoyl-acyl carrier protein reductase known as InhA, thereby blocking the natural enoyl-AcpM substrate and the action of fatty acid synthase. This process inhibits the synthesis of mycolic acid, required for the mycobacterial cell wall. A range of radicals are produced by KatG activation of Isoniazid, including nitric oxide,[6] which has also been shown to be important in the action of another antimycobacterial prodrug PA-824.[7]
Isoniazid is bactericidal to rapidly-dividing mycobacteria but is bacteriostatic if the mycobacterium is slow-growing.[citation needed]
Isoniazid inhibits the P450 system.[8]
Metabolism
Isoniazid reaches therapeutic concentrations in serum, cerebrospinal fluid (CSF), and within caseous granulomas. Isoniazid is metabolized in the liver via acetylation. There are two forms of the enzyme responsible for acetylation, so that some patients metabolize the drug more quickly than others. Hence, the half-life is bimodal with peaks at 1 hour and 3 hours in the US population. The metabolites are excreted in the urine. Doses do not usually have to be adjusted in case of renal failure.
Dosing
The standard dose of isoniazid in adults is 5 mg/kg/day (max 300 mg daily). When prescribed intermittently (twice or thrice weekly) the dose is 15 mg/kg (max 900 mg daily). Patients with slow clearance of the drug (via acetylation as described above) may require reduced dosages to avoid toxicity. The recommended dose for children is 8 to 12 mg/kg/day.[9]
Side effects
Adverse reactions include rash, abnormal liver function tests, hepatitis, sideroblastic anemia, high anion gap metabolic acidosis, peripheral neuropathy, mild central nervous system (CNS) effects, drug interactions resulting in increased phenytoin (Dilantin) or disulfiram (Antabuse) levels and intractable seizures (status epilepticus).
Peripheral neuropathy and CNS effects are associated with the use of isoniazid and are due to pyridoxine (vitamin B6) depletion, but are uncommon at doses of 5 mg/kg. Persons with conditions in which neuropathy is common (e.g., diabetes, uremia, alcoholism, malnutrition, HIV-infection), as well as pregnant women and persons with a seizure disorder, may be given pyridoxine (vitamin B6) (10–50 mg/day) with isoniazid.
Hepatotoxicity of INH is by nitrogen group in its chemical structure, as it is metabolized in the liver and gets converted in to an ammonium molecule, which causes hepatitis.
Hepatotoxicity can be avoided with close clinical monitoring of the patient, to be specific, nausea, vomiting, abdominal pain, and appetite. Isoniazid is metabolized by the liver mainly by acetylation and dehydrazination. The N-acetylhydrazine metabolite is believed to be responsible for the hepatotoxic effects seen in patients treated with isoniazid. The rate of acetylation is genetically determined. Approximately 50% of blacks and Caucasians are slow inactivators; the majority of Inuit and Asians are rapid inactivators. The half-life in fast acetylators is 1 to 2 hours, while in slow acetylators it is 2 to 5 hours. Elimination is largely independent of renal function, however the half-life may be prolonged in liver disease. The rate of acetylation has not been shown to significantly alter the effectiveness of isoniazid. However, slow acetylation may lead to higher blood concentrations with chronic administration of the drug, with an increased risk of toxicity. Fast acetylation leads to higher blood levels of the toxic metabolite acetylisoniazid and thus to an increase in toxic reactions - hepatitis which is 250 times more common than in slow acetylators. Isoniazid and its metabolites are excreted in the urine with 75 to 95% of the dose excreted in 24 hours. Small amounts are also excreted in saliva, sputum, and feces. Isoniazid is removed by hemodialysis and peritoneal dialysis.[10]
Headache, poor concentration, weight-gain, poor memory, and depression have all been associated with isoniazid use. All patients and healthcare workers should be aware of these serious adverse effects, especially if suicidal thinking or behavior are suspected.[11][12][13]
INH is known to reduce cytochrome P450 and in theory promote the efficacy of Contraceptives. Therapy is often combined with Rifampin. Rifampin increases the P450 enzyme and can reduce the efficacy of contraceptives. Alternative means of birth control should be used when taking these medications.
As p450 is required for porphyrin synthesis its deficiency leads to poor heme formation in early RBCs leads to sideroblastic anemia.
Synonyms and abbreviations
- Isonicotinyl hydrazine
- Isonicotinic acid hydrazide
- INH
- H (for "hydrazide", and also the WHO standard abbreviation)
See also
References
- ^ Meyer H, Mally J (1912). "On hydrazine derivatives of pyridine carbonic acids" (in German). Monatshefte Chemie verwandte Teile anderer Wissenschaften 33: 393–414.[1]
- ^ Hans L Riede (2009). "Fourth-generation fluoroquinolones in tuberculosis". Lancet 373 (9670): 1148–1149. doi:10.1016/S0140-6736(09)60559-6. PMID 19345815.
- ^ Shinkichi Shimizu, Nanao Watanabe, Toshiaki Kataoka, Takayuki Shoji, Nobuyuki Abe, Sinji Morishita, Hisao Ichimura (2007). "Pyridine and Pyridine Derivatives". Ullmann's Encyclopedia of Industrial Chemistry. New York: John Wiley & Sons.[page needed]
- ^ T. P. Sycheva, T. N. Pavlova and M. N. Shchukina (1972). "Synthesis of isoniazid from 4-cyanopyridine". Pharmaceutical Chemistry Journal 6 (11): 696–698. doi:10.1007/BF00771896.
- ^ Suarez J, Ranguelova K, Jarzecki AA, et al. (March 2009). "An oxyferrous heme/protein-based radical intermediate is catalytically competent in the catalase reaction of Mycobacterium tuberculosis catalase-peroxidase (KatG)". The Journal of Biological Chemistry 284 (11): 7017–29. doi:10.1074/jbc.M808106200. PMC 2652337. PMID 19139099. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2652337.
- ^ Timmins GS, Master S, Rusnak F, Deretic V (August 2004). "Nitric oxide generated from isoniazid activation by KatG: source of nitric oxide and activity against Mycobacterium tuberculosis". Antimicrobial Agents and Chemotherapy 48 (8): 3006–9. doi:10.1128/AAC.48.8.3006-3009.2004. PMC 478481. PMID 15273113. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=478481.
- ^ Singh R, Manjunatha U, Boshoff HI, et al. (November 2008). "PA-824 kills nonreplicating Mycobacterium tuberculosis by intracellular NO release". Science 322 (5906): 1392–5. doi:10.1126/science.1164571. PMC 2723733. PMID 19039139. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2723733.
- ^ Pharmacology, Harvey 4th edition. November 2009.
- ^ McIlleron H, Willemse M, Werely CJ, et al. (June 2009). "Isoniazid plasma concentrations in a cohort of South African children with tuberculosis: implications for international pediatric dosing guidelines". Clinical Infectious Diseases 48 (11): 1547–53. doi:10.1086/598192. PMID 19392636.
- ^ http://www.rxmed.com/b.main/b2.pharmaceutical/b2.1.monographs/CPS-%20Monographs/CPS-%20(General%20Monographs-%20I)/ISONIAZID.html
- ^ Alao AO, Yolles JC (September 1998). "Isoniazid-induced psychosis". The Annals of Pharmacotherapy 32 (9): 889–91. doi:10.1345/aph.17377. PMID 9762376.
- ^ http://journals.lww.com/pec-online/Fulltext/2002/02000/Suicidal_psychosis_secondary_to_isoniazid.8.aspx[dead link]
- ^ Pallone KA, Goldman MP, Fuller MA (February 1993). "Isoniazid-associated psychosis: case report and review of the literature". The Annals of Pharmacotherapy 27 (2): 167–70. PMID 8439690.
External links
-
- Core Curriculum on Tuberculosis (2000) Division of Tuberculosis Elimination, Centers for Disease Control and Prevention
- See Chapter 6, Treatment of LTBI Regimens - Isoniazid::
See Chapter 7 - Treatment of TB Disease Monitoring - Adverse Reactions to First-Line TB Drugs - Isoniazid::
See Table 5 First-Line Anti-TB Medications
-
- Isoniazid Overdose: Recognition and Management American Family Physician 1998 Feb 15
Antimycobacterials, including tuberculosis treatment and leprostatic agents (J04) Nucleic acid inhibitor Antifolates/DSIASA4-Aminosalicylic acid# (Calcium aminosalicylate, Sodium aminosalicylate)Protein synthesis inhibitor Cell envelope antibiotic Peptidoglycan layerAlanine analogue: Cycloserine#Arabinogalactan layerEthylenediamine/arabinosyltransferase inhibitor: Ethambutol#
SQ109†Mycolic acid layerHydrazides/mycolic acid synth. inhibition: Isoniazid#
Thiocarbamides: Ethionamide# • Prothionamide • ThiocarlideOther/unknown phenazine (Clofazimine)# • pyrazine (Pyrazinamide#, Morinamide) • isoxazole (Terizidone) • R207910/TMC207†Combinations Rifampicin/isoniazid/pyrazinamideHydrazines 4-PTSC • Acylhydrazine • ADH • Adjudin • Agaritine • Benmoxin • Cadralazine • Carbazide • Carbazone • Carbidopa • Carbohydrazide • Daminozide • Dihydralazine • DNPH • Endralazine • Gyromitrin • HBT • Hydralazine • Hydrazide • Hydrazine • Hydrazone • IDH • Iproclozide • Iproniazid • Isocarboxazid • Isoniazid • Mebanazine • Metfendrazine • MMH • Nialamide • Octamoxin • PEH • Phenelzine • Pheniprazine • Phenoxypropazine • Phenylhydrazine • Pimagedine • Pivalylbenzhydrazine • Procarbazine • Safrazine • SDH • Semicarbazide • Semicarbazone • SDMH • Tetrafluorohydrazine • Thiosemicarbazide • Thiosemicarbazone • UDMHCategories:- Antibiotics
- Prodrugs
- Isonicotinamides
- Tuberculosis
- World Health Organization essential medicines
- Hydrazides
- Antidepressants
- InChI=1S/C6H7N3O/c7-9-6(10)5-1-3-8-4-2-5/h1-4H,7H2,(H,9,10)


Wikimedia Foundation. 2010.