- Nalbuphine
-
Nalbuphine 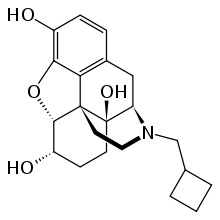
Systematic (IUPAC) name (–)-17-(cyclobutylmethyl)- 4,5α-epoxymorphinan- 3,6α,14-triol hydrochloride Clinical data AHFS/Drugs.com monograph MedlinePlus a682668 Pregnancy cat. B Legal status Legend, Unscheduled Routes intravenous, intramuscular, subcutaneous Pharmacokinetic data Bioavailability 81% @ 10mg and 83% @ 20 mg, intramuscular; 79% @ 10mg and 76% @ 20 mg subcutaneous Metabolism 3 to 6 hours clinically, 5 hours in blood plasma Identifiers CAS number 20594-83-6 
ATC code N02AF02 PubChem CID 5311304 DrugBank APRD01132 ChemSpider 4470813 UNII L2T84IQI2K ChEBI CHEBI:7454 ChEMBL CHEMBL895 Chemical data Formula C21H27NO4 Mol. mass 357.443 g/mol SMILES eMolecules & PubChem - InChI=1S/C21H27NO4/c23-14-5-4-13-10-16-21(25)7-6-15(24)19-20(21,17(13)18(14)26-19)8-9-22(16)11-12-2-1-3-12/h4-5,12,15-16,19,23-25H,1-3,6-11H2/t15-,16+,19-,20-,21+/m0/s1
Key:NETZHAKZCGBWSS-CEDHKZHLSA-N
 (what is this?) (verify)
(what is this?) (verify)Nalbuphine is a semi-synthetic opioid used commercially as an analgesic under a variety of trade names, including Nubain. It is noteworthy in part for the fact that at low dosages, it is found much more effective by women than by men, and may even increase pain in men,[1] leading to its discontinuation in the UK in 2003.
Contents
History and control status
In the search for opioid analgesics with less abuse potential, a number of semi-synthetic opiates were developed. These substances are referred to as mixed agonist-antagonists analgesics. Nalbuphine (Nubain®) belongs to this group of substances. It was approved for marketing in the United States in 1979 and remains as the only opiod analgesic of this type (marketed in the U.S.) not controlled under the Controlled Substances Act (CSA). When the Controlled Substances Act (CSA) was enacted in 1971, nalbuphine was placed in schedule II. Endo Laboratories, Inc. subsequently petitioned the DEA to exclude nalbuphine from all schedules of the CSA in 1973. After receiving a medical and scientific review and a scheduling recommendation from the Department of Health, Education and Welfare, forerunner to the Department of Health and Human Services, nalbuphine was removed from schedule II of the CSA in 1976. Presently, nalbuphine is not a controlled substance under the CSA. Kentucky has controlled nalbuphine in schedule IV of state law.
Clinical pharmacology
Nalbuphine is a semi-synthetic opioid agonist-antagonist analgesic of the phenanthrene series. It is chemically related to both the widely used opioid antagonist, naloxone, and the potent opioid analgesic, oxymorphone. It is available in two concentrations, 10 mg and 20 mg of nalbuphine hydrochloride per mL. Both strengths contain 0.94% sodium citrate hydrous, 1.26% citric acid anhydrous, 0.1% sodium metabisulfite, and 0.2% of a 9:1 mixture of methylparaben and propylparaben as preservatives; pH is adjusted, if necessary, with hydrochloric acid. The 10 mg/mL strength contains 0.1% sodium chloride.
Nalbuphine is also available in a sulfite and paraben-free formulation in two concentrations, 10 mg and 20 mg of nalbuphine hydrochloride per mL. One mL of each strength contains 0.94% sodium citrate hydrous, 1.26% citric acid anhydrous; pH is adjusted, if necessary, with hydrochloric acid. The 10 mg/mL strength contains 0.2% sodium chloride.
Nalbuphine is a potent analgesic. Its analgesic potency is essentially equivalent to that of morphine on a milligram basis. Its onset of action occurs within 2 to 3 minutes after intravenous administration, and in less than 15 minutes following subcutaneous or intramuscular injection. The plasma half-life of nalbuphine is 5 hours and in clinical studies the duration of analgesic activity has been reported to range from 3 to 6 hours.
The opioid antagonist activity of Nalbuphine is one-fourth as potent as nalorphine and 10 times that of pentazocine.
Indication
Nalbuphine is indicated for the relief of moderate to severe pain. It can also be used as a supplement to balanced anesthesia, for preoperative and postoperative analgesia, and for obstetrical analgesia during labor and delivery.
Although Nalbuphine possesses opioid antagonist activity, there is evidence that in nondependent patients it will not antagonize a opioid analgesic administered just before, concurrently, or just after an injection. Therefore, patients receiving an opioid analgesic, general anesthetics, phenothiazines, or other tranquilizers, sedatives, hypnotics, or other CNS depressants (including alcohol) concomitantly with Nalbuphine may exhibit an additive effect. When such combined therapy is contemplated, the dose of one or both agents should be reduced.
Dosing
The usual recommended adult dose is 10 mg for a 70 kg individual, administered subcutaneously, intramuscularly or intravenously; this dose may be repeated every 3 to 6 hours as necessary. Dosage should be adjusted according to the severity of the pain, physical status of the patient, and other medications which the patient may be receiving. In non-tolerant individuals, the recommended single maximum dose is 20 mg, with a maximum total daily dose of 160 mg.
The use of NUBAIN as a supplement to balanced anesthesia requires larger doses than those recommended for analgesia. Induction doses of NUBAIN range from 0.3 mg/kg to 3.0 mg/kg intravenously to be administered over a 10 to 15 minute period with maintenance doses of 0.25 to 0.50 mg/kg in single intravenous administrations as required.
In case of overdose or adverse reaction, the immediate intravenous administration of naloxone (Narcan) is a specific antidote. Oxygen, intravenous fluids, vasopressors and other supportive measures should be used as indicated.
Side effects
The most frequent side effect in 1066 patients treated with nalbuphine was sedation in 381 (36%).
Other, less frequent reactions are: feeling sweaty/clammy 99 (9%), nausea/vomiting 68 (6%), dizziness/vertigo 58 (5%), dry mouth 44 (4%), and headache 27 (3%). Other adverse reactions which may occur (reported incidence of 1% or less) are:
- CNS effects: Nervousness, depression, restlessness, crying, euphoria, floating, hostility, unusual dreams, confusion, faintness, hallucinations, dysphoria, feeling of heaviness, numbness, tingling, unreality. The incidence of psychotomimetic effects, such as unreality, depersonalization, delusions, dysphoria and hallucinations has been shown to be less than that which occurs with pentazocine.
- Cardiovascular: Hypertension, hypotension, bradycardia, tachycardia, pulmonary edema.
- Gastrointestinal: Cramps, dyspepsia, bitter taste.
- Respiration: Depression, dyspnea, asthma.
- Dermatological: Itching, burning, urticaria.
- Obstetric: Pseudo-sinusoidal fetal heart rhythm.
Other possible, but rare side effects include speech difficulty, urinary urgency, blurred vision, flushing and warmth.
References
- Yuan-Yi Chia, Lok-Hi Chow, Chun-Chieh Hung, et al., Gender and pain upon movement are associated with the requirements for postoperative patient-controlled iv analgesia: a prospective survey of 2,298 Chinese patients, Canadian Journal of Anesthesia. 49:249-255 (2002).
- Woods JR, Flynn K, Glantz JC, Pittinaro D. Sinusoidal fetal heart rate patterns. Peri-FACTS, Case #681, 2006. Retrieved from [1], September 10, 2009.
- ^ Gear, RW; Miaskowski C, Gordon NC, Paul SM, Heller PH, Levine JD (November 1999). "The kappa opioid nalbuphine produces gender- and dose-dependent analgesia and antianalgesia in patients with postoperative pain". Pain 83 (2): 339–45. doi:10.1016/S0304-3959(99)00119-0. PMID 10534607.
External links
Categories:- Morphinans
- Ethers
- Alcohols
- Phenols
- Semisynthetic opioids
- Kappa agonists
- InChI=1S/C21H27NO4/c23-14-5-4-13-10-16-21(25)7-6-15(24)19-20(21,17(13)18(14)26-19)8-9-22(16)11-12-2-1-3-12/h4-5,12,15-16,19,23-25H,1-3,6-11H2/t15-,16+,19-,20-,21+/m0/s1

Wikimedia Foundation. 2010.