- Fluoxetine
-
"Prozac" redirects here. For other uses, see Prozac (disambiguation).
Fluoxetine 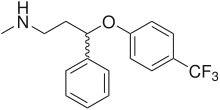

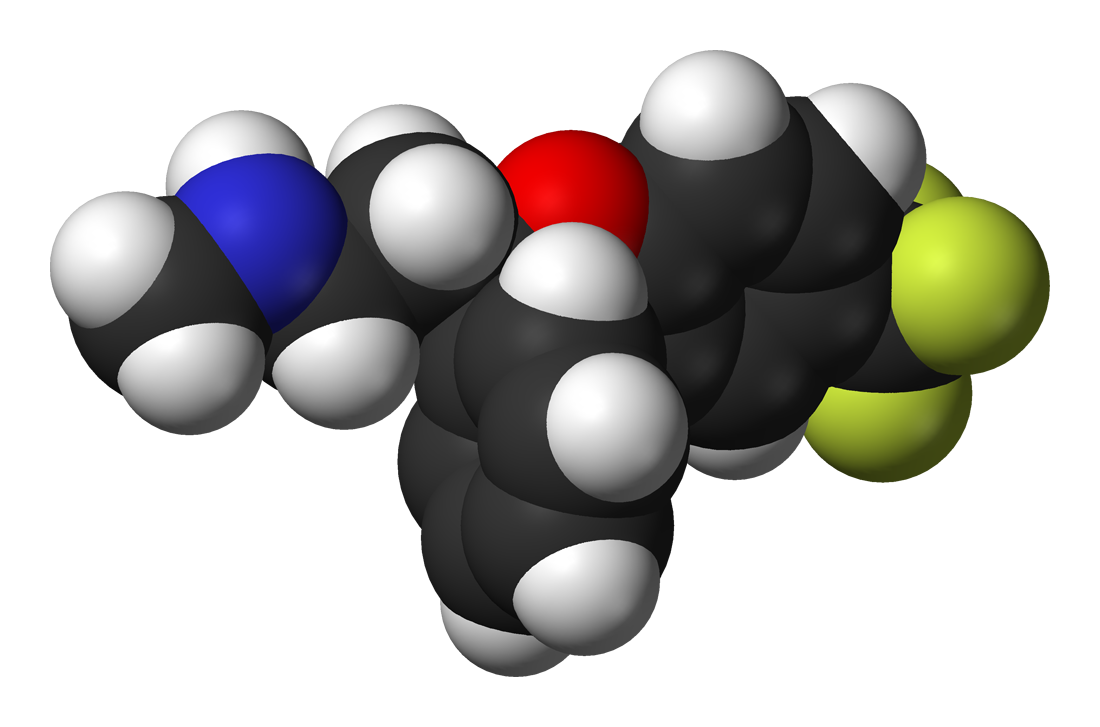
Systematic (IUPAC) name N-methyl-3-phenyl-3-[4-(trifluoromethyl)phenoxy]propan-1-amine Clinical data Trade names Prozac, others (see text) AHFS/Drugs.com fluoxetine-hydrochloride MedlinePlus a689006 Licence data US FDA:link Pregnancy cat. C(AU) C(US) Legal status Prescription Only (S4) (AU) ℞-only (CA) POM (UK) ℞-only (US) Routes Oral Pharmacokinetic data Bioavailability 72% (peak at 6-8 hours) Protein binding 94.5% Metabolism Hepatic (mostly CYP2D6-mediated) Half-life 1-3 days (acute)
4-6 days (chronic)Excretion Renal (80%), fecal (15%) Identifiers CAS number 54910-89-3 
ATC code N06AB03 PubChem CID 3386 IUPHAR ligand 203 DrugBank APRD00530 ChemSpider 3269 UNII 01K63SUP8D KEGG D00326 
ChEBI CHEBI:5118 ChEMBL CHEMBL41 Chemical data Formula C17H18F3NO Mol. mass 309.33 g·mol-1 SMILES eMolecules & PubChem - InChI=1S/C17H18F3NO/c1-21-12-11-16(13-5-3-2-4-6-13)22-15-9-7-14(8-10-15)17(18,19)20/h2-10,16,21H,11-12H2,1H3
Key:RTHCYVBBDHJXIQ-UHFFFAOYSA-N
Physical data Melt. point 179–182 °C (354–360 °F) Boiling point 395 °C (743 °F) Solubility in water 14 mg/mL (20 °C)  (what is this?) (verify)
(what is this?) (verify) Fluoxetine 20 mg capsules
Fluoxetine 20 mg capsules
Fluoxetine (also known by the tradenames Prozac, Sarafem, Fontex) is an antidepressant of the selective serotonin reuptake inhibitor (SSRI) class. It is manufactured and marketed by Eli Lilly and Company. In combination with olanzapine it is known as Symbyax.
Fluoxetine is approved for the treatment of major depression (including pediatric depression), obsessive-compulsive disorder (in both adult and pediatric populations), bulimia nervosa, panic disorder and premenstrual dysphoric disorder.[1]
Despite the availability of newer agents, fluoxetine remains extremely popular. In 2010, over 24.4 million prescriptions for generic formulations of fluoxetine were filled in the United States alone,[2] making it the third most prescribed antidepressant after sertraline (SSRI; became generic in 2006) and citalopram (SSRI; became generic in 2003) in that country.[2]
Contents
Medical uses
Fluoxetine is frequently used to treat major depression, bipolar disorder, obsessive compulsive disorder, bulimia nervosa, panic disorder and premenstrual dysphoric disorder.[3] It has also been used for cataplexy, obesity, and alcohol dependence,[3] as well as binge eating disorder.[4]
Depression
Fluoxetine was shown to be effective for depression in 6-week long double-blind controlled trials, where it also alleviated anxiety and improved sleep. Fluoxetine was better than placebo for the prevention of depression recurrence when the patients, who originally responded to fluoxetine, were treated for a further 38 weeks. Efficacy of fluoxetine for geriatric, as well as pediatric, depression was also demonstrated in placebo-controlled trials.[5]
The recent research suggests that a significant part of the resistance to the SSRIs paroxetine (Paxil) and citalopram (Celexa) can be explained by the genetic variation of Pgp transporter. Paroxetine and citalopram, which are Pgp substrates, are actively transported from the brain by this protein. Fluoxetine is not a substrate of Pgp, and thus a switch from paroxetine or citalopram to fluoxetine may be beneficial to the nonresponders.[6][7]
Obsessive-compulsive disorder
OCD was successfully treated by fluoxetine in two adult and one pediatric placebo-controlled 13-week trials. The higher doses of fluoxetine appeared to result in better response, while the reverse relationship was observed in the treatment of depression.[5] Fluoxetine dramatically, by 40-50%, decreased the frequency of panic attacks in two controlled trials of panic disorder patients. In three double-blind trials, fluoxetine significantly decreased the number of binge-eating and purging episodes of bulimia nervosa. Continued year-long treatment of the patients, who originally responded to fluoxetine, was more effective than placebo for the prevention of bulimia nervosa episodes.[5]
Adverse effects
 Fluoxetine capsules (20 mg), as prescribed in the United Kingdom
Fluoxetine capsules (20 mg), as prescribed in the United KingdomSexual dysfunction is a common side effect with SSRIs. Specifically, side effects often include difficulty becoming aroused, erectile dysfunction, lack of interest in sex, and anorgasmia (inability to achieve orgasm). Genital anesthesia,[8] loss of or decreased response to sexual stimuli, and ejaculatory anhedonia are also possible. Although usually reversible, these sexual side effects can last for months, years, or permanence after the drug has been completely withdrawn.[9] This is known as Post SSRI Sexual Dysfunction.
According to the manufacturer of Prozac brand of fluoxetine, Eli Lilly, fluoxetine is contraindicated in individuals taking monoamine oxidase inhibitors, pimozide (Orap) or thioridazine (Mellaril).[5] The prescribing information recommends that the treatment of the patients with liver impairment "must be approached with caution". The elimination of fluoxetine and its metabolite norfluoxetine is about half as fast in these patients, resulting in the proportionate increase of exposure to the drug.[5] Ibuprofen used in combination with fluoxetine can cause significant intestinal bleeding after a period of use.
Among the common adverse effects associated with fluoxetine and listed in the prescribing information, the effects with the greatest difference from placebo are nausea (22% vs 9% for placebo), insomnia (19% vs 10% for placebo), somnolence (12% vs 5% for placebo), anorexia (10% vs 3% for placebo), anxiety (12% vs 6% for placebo), nervousness (13% vs 8% for placebo), asthenia (11% vs 6% for placebo) and tremor (9% vs 2% for placebo). Those that most often resulted in interruption of the treatment were anxiety, insomnia, and nervousness (1-2% each), and in pediatric trials—mania (2%).[5][10][11] Similarly to other SSRIs, sexual side effects are common with fluoxetine; they include anorgasmia and reduced libido.[12]
In addition, rash or urticaria, sometimes serious, was observed in 7% patients in clinical trials; one-third of these cases resulted in discontinuation of the treatment. Postmarketing reports note several cases of complications developed in patients with rash. The symptoms included vasculitis and lupus-like syndrome. Death has been reported to occur in association with these systemic events.[5]
Akathisia, that is inner tension, restlessness, and the inability to stay still, often accompanied by "constant pacing, purposeless movements of the feet and legs, and marked anxiety", is a common side effect of fluoxetine.[13][14] Akathisia usually begins after the initiation of the treatment or increase of the dose and disappears after fluoxetine is stopped or its dose is decreased, or after treatment with propranolol.[13][15][16] There are case reports directly linking akathisia with suicidal attempts, with patients feeling better after the withdrawal of fluoxetine, and again developing severe akathisia on repeated exposure to fluoxetine. These patients described "that the development of the akathisia made them feel suicidal and that it had precipitated their prior suicide attempts".[16] The experts note that because of the link of akathisia with suicide and the distress it causes to the patient, "it is of vital importance to increase awareness amongst staff and patients of the symptoms of this relatively common condition".[17][18] More rarely, fluoxetine has been associated with related movement disorders acute dystonia and tardive dyskinesia.[14][19][20]
Fluoxetine taken during pregnancy also increases rate of poor neonatal adaptation.[12] Because fluoxetine is excreted in human milk, nursing while on fluoxetine is not recommended.[21] A study of fluoxetine administered to newborn mice found that early postnatal exposure of the drug later caused the adult mice to exhibit depressive and anxious behavior similar to those of induced depression, which could be relieved by fluoxetine.[22] The American Association of Pediatrics classifies fluoxetine as a drug for which the effect on the nursing infant is unknown but may be of concern.[23]
Discontinuation syndrome
Several case reports in the literature describe severe withdrawal or discontinuation symptoms following an abrupt interruption of fluoxetine treatment.[24] However, various studies have shown that the side effects of the fluoxetine discontinuation are uncommon and mild, especially compared to paroxetine, venlafaxine and fluvoxamine, probably due to the relatively long pharmacological half-life of fluoxetine.[24] One of the recommended strategies for the management of discontinuation syndrome with other SSRIs is to substitute fluoxetine for the original agent, in cases where tapering off the dose of the original SSRI is ineffective.[25][26] The double-blind controlled studies support this opinion. No increase in side effects was observed in several studies when the treatment with fluoxetine was blindly interrupted for a short time (4–8 days) and then reinstated, this result being consistent with its slow elimination from the body. More side effects occurred during the interruption of sertraline (Zoloft) in these studies, and significantly more during the interruption of paroxetine.[27] In a longer, 6 week-long, blind discontinuation study, an insignificantly higher (32% vs 27%) overall rate of new or worsened side effects was observed in the group that discontinued fluoxetine than in the group that continued treatment. However, a significantly higher 4.2% rate of somnolence at week 2 and 5-7% rate of dizziness at weeks 4-6 were reported by the patients in the discontinuation group. This prolonged course of the discontinuation symptoms, with dizziness persisting to the end of the study, is also consistent with the long half-life of fluoxetine in the body.[28] According to a 2007 summary report of available evidence, fluoxetine has the lowest incidence of discontinuation syndrome among several antidepressants including paroxetine and venlafaxine. [29] See also SSRI discontinuation syndrome.
Suicide
The FDA requires all antidepressants to carry a black box warning stating that antidepressants may increase the risk of suicide in persons younger than 25. This warning is based on statistical analyses conducted by two independent groups of the FDA experts that found a 2-fold increase of the suicidal ideation and behavior in children and adolescents, and 1.5-fold increase of suicidality in the 18–24 age group. The suicidality was slightly decreased for those older than 24, and statistically significantly lower in the 65 and older group.[30][31][32] This analysis was criticized by Donald Klein, who noted that suicidality, that is suicidal ideation and behavior, is not necessarily a good surrogate marker for completed suicide, and it is still possible that antidepressants may prevent actual suicide while increasing suicidality.[33] This opinion goes against the general consensus that "suicidal ideation has been associated with suicide attempt in retrospective studies and with suicide in prospective studies".[34]
There is less data on fluoxetine than on antidepressants as a whole. For the above analysis on the antidepressant level, the FDA had to combine the results of 295 trials of 11 antidepressants for psychiatric indications to obtain statistically significant results. Considered separately, fluoxetine use in children increased the odds of suicidality by 50% (not statistically significant due to the low number of cases),[35] and in adults decreased the odds of suicidality by approximately 30% (statistically significant).[31][32] Similarly, the analysis conducted by the UK MHRA found a 50% increase of odds of suicide-related events, not reaching statistical significance, in the children and adolescents on fluoxetine as compared to the ones on placebo. According to the MHRA data, for adults fluoxetine did not change the rate of self-harm and statistically significantly decreased suicidal ideation by 50%.[36][37]
Interactions
Fluoxetine and norfluoxetine inhibit many isozymes of the cytochrome P450 system that make drug metabolism possible. Both are potent inhibitors of CYP2D6 (the main enzyme responsible for their metabolism) and mild to moderate inhibitors of CYP1A2, CYP2B6, CYP2C9/2C19, and CYP3A4; furthermore, they inhibit the activity of P-glycoprotein, a type of membrane transport protein that plays an important role in drug transport and metabolism.[38] This extensive effect on the body's pathways for drug metabolism creates the potential for interactions with many commonly used drugs.[38][39]
The simultaneous use of fluoxetine with triptans, tramadol or other serotonergic agents can result in a rare, but potentially life-threatening adverse drug reaction called serotonin syndrome.
Fluoxetine has been shown to have antimicrobial activity against several groups of microorganisms. This is mainly against Gram positive microorganisms. It also shows synergistic activity when combined with some antibiotics against several bacteria. [40]
Pharmacokinetics
 3 dimensional representation of the cytochrome P450 isoenzyme CYP2D6. CYP2D6 is responsible for converting fluoxetine to its only active metabolite, norfluoxetine.[41] Both drugs are also potent inhibitors of CYP2D6.[42]
3 dimensional representation of the cytochrome P450 isoenzyme CYP2D6. CYP2D6 is responsible for converting fluoxetine to its only active metabolite, norfluoxetine.[41] Both drugs are also potent inhibitors of CYP2D6.[42]The bioavailability of fluoxetine is relatively high (72%), and peak plasma concentrations are reached in 6 to 8 hours. It is highly bound to plasma proteins, mostly albumin.
Fluoxetine is metabolized in the liver by isoenzymes of the cytochrome P450 system, including CYP2D6.[1] The role of CYP2D6 in the metabolism of fluoxetine may be clinically important, as there is great genetic variability in the function of this enzyme among people. Only one metabolite of fluoxetine, norfluoxetine (N-demethylated fluoxetine), is biologically active.
The extremely slow elimination of fluoxetine and its active metabolite norfluoxetine from the body distinguishes it from other antidepressants. With time, fluoxetine and norfluoxetine inhibit their own metabolism, so fluoxetine elimination half-life changes from 1 to 3 days, after a single dose, to 4 to 6 days, after long-term use. Similarly, the half-life of norfluoxetine is longer (16 days) after long-term use.[1][43][44] Therefore, the concentration of the drug and its active metabolite in the blood continues to grow through the first few weeks of treatment, and their steady concentration in the blood is achieved only after four weeks.[45][46] Moreover, the brain concentration of fluoxetine and its metabolites keeps increasing through at least the first five weeks of treatment.[47] That means that the full benefits of the current dose a patient receives are not realized for at least a month since its initiation. For example, in one 6-week study, the median time to achieving consistent response was 29 days.[45] Likewise, complete excretion of the drug may take several weeks. During the first week after the treatment discontinuation, the brain concentration of fluoxetine decreases only by 50%,[47] The blood level of norfluoxetine 4 weeks after the treatment discontinuation is about 80% of the level registered by the end of the first treatment week, and 7 weeks after the discontinuation norfluoxetine is still detectable in the blood.[43]
A PET study compared the action of a single dose of fluoxetine on exclusively heterosexual and exclusively homosexual men who attested that their past and present sexual behavior, desires, and fantasies were directed entirely toward women or men, respectively. The study found that in some areas of the brain the metabolic response in these two groups was different. "Both groups, however, did exhibit similar widespread lateralized metabolic responses to fluoxetine (relative to placebo), with most areas of the brain responding in the same direction." They "did not differ on behavioral measures or blood levels of fluoxetine".[48]
Fluoxetine is a selective serotonin reuptake inhibitor and does not appreciably inhibit norepinephrine and dopamine reuptake. Nevertheless, Eli Lilly researchers found that a single injection of a rat with a large dose of fluoxetine also results in a significant increase of brain concentrations of norepinephrine and dopamine.[49][50][51] This effect may be mediated by 5HT2a and, in particular, 5HT2c receptors, which are inhibited by higher concentrations of fluoxetine. The Ely Lilly scientists also suggested that the effects on dopamine and norepinephrine may contribute to the antidepressant action of fluoxetine.[51] In the opinion of other researchers, however, the magnitude of this effect is unclear.[47] The dopamine and norepinephrine increase was not observed at a smaller, more clinically relevant dose of fluoxetine.[52] Similarly, in electrophysiological studies only larger and not smaller doses of fluoxetine changed the activity of rat's norepinephrinergic neurons. Some authors, however, argue that these findings may still have clinical relevance for the treatment of severe illness with supratherapeutic doses (60–80 mg) of fluoxetine.[53] Among SSRIs, 'fluoxetine is the least "selective" of all the SSRIs, with a 10-fold difference in binding affinity between its first and second neural targets (i.e., the serotonin and norepinephrine uptake pumps, respectively).' Anything greater than a 10-fold difference results in insignificant activation of the secondary neuronal targets.[54]
Besides its well-known effects on serotonin, fluoxetine also increases density of endogenous opioid receptors in the brains of rats. It is unclear if this occurs in humans, but if so it might account for some of fluoxetine's antidepressant and/or side effect profile.[55]
Measurement in body fluids
Fluoxetine and norfluoxetine may be quantitated in blood, plasma or serum to monitor therapy, confirm a diagnosis of poisoning in hospitalized patients or assist in a medicolegal death investigation. Blood or plasma fluoxetine concentrations are usually in a range of 50-500 μg/L in persons taking the drug for its antidepressant effects, 900-3000 μg/L in survivors of acute overdosage and 1000-7000 μg/L in victims of fatal overdosage. Norfluoxetine concentrations are approximately equal to those of the parent drug during chronic therapy, but may be substantially less following acute overdosage, since it requires at least 1–2 weeks for the metabolite to achieve equilibrium.[56][57][58]
Mechanism of action
Fluoxetine's mechanism of action is primarily that of an SSRI although it may produce some of its effects through 5-HT2C antagonism in a manner similar to the novel antidepressant agomelatine. Other psychopharmacological substances that exhibit 5-HT2C antagonism are mirtazapine, agomelatine, trazodone, some tricyclic antidepressants and various (mainly atypical) antipsychotics.
Fluoxetine acts as an agonist at the σ1-receptor, with a potency greater than that of Citalopram, but less than that of Fluvoxamine.[59][60]
History
The work which eventually led to the discovery of fluoxetine began at Eli Lilly and Company in 1970 as a collaboration between Bryan Molloy and Robert Rathbun. It was known at that time that the antihistamine diphenhydramine shows some antidepressant-like properties. 3-Phenoxy-3-phenylpropylamine, a compound structurally similar to diphenhydramine, was taken as a starting point, and Molloy synthesized dozens of its derivatives. Testing the physiological effects of these compounds in mice resulted in nisoxetine, a selective norepinephrine reuptake inhibitor currently widely used in biochemical experiments.[61][62]
Later, hoping to find a derivative inhibiting only serotonin reuptake, another Eli Lilly scientist, David Wong, proposed to retest the series for the in vitro reuptake of serotonin, norepinephrine and dopamine. This test, carried out by Jong-Sir Horng in May 1972,[62] showed the compound later named fluoxetine to be the most potent and selective inhibitor of serotonin reuptake of the series.[63] Wong published the first article about fluoxetine in 1974. A year later, it was given the official chemical name fluoxetine and the Eli Lilly and Company gave it the trade name Prozac. In February 1977, Dista Products Company, a division of Eli Lilly & Company, presented a new drug request to the U.S. Food and Drug Administration (FDA) for fluoxetine.[64]
A controversy ensued after Lilly researchers published a paper titled "Prozac (fluoxetine, Lilly 110140), the first selective serotonin uptake inhibitor and an antidepressant drug"[62] claiming fluoxetine to be the first selective serotonin reuptake inhibitor (SSRI). Two years later they had to issue a correction, admitting that the first SSRI was zimelidine developed by Arvid Carlsson and colleagues.[65] Fluoxetine made its appearance on the Belgian market in 1986[66] and was approved for use by the FDA in December 1987.[67] Fluoxetine was the fourth SSRI to make it to market, after zimelidine, indalpine and fluvoxamine. However, the first two were withdrawn due to the side effects, and a vigorous marketing campaign by Eli Lilly made sure that in the popular culture fluoxetine has been perceived as a scientific breakthrough and associated with the title of the first SSRI.
Eli Lilly's patent on Prozac (fluoxetine) expired in the United States in August 2001,[68] prompting an influx of generic drugs onto the market. Prozac was rebranded "Sarafem" for the treatment of PMDD in an attempt to stem the post-patent decrease in Eli Lilly's sales of fluoxetine.[69]
Controversy
In 1989, Joseph Wesbecker shot and killed eight people and injured 12 others before killing himself at his place of work in Kentucky. Wesbecker had been taking the selective serotonin reuptake inhibitor (SSRI) antidepressant fluoxetine for four weeks before these homicides, and this led to a legal action against the makers of fluoxetine, Eli Lilly.[70] The case was tried and settled in 1994, and as part of the settlement a number of pharmaceutical company documents about drug-induced activation were released into the public domain. Subsequent legal cases have further raised the possibility of a link between antidepressant use and violence.[71]
The Prozac Survivors Support Group created a report on 288 individuals who had suffered adverse effects from Fluoxetine during 1991 and 1992. It showed that most of the cases led to violence against self or other individuals. There were 164 cases in the suicide and suicide ideation category, including 34 complete suicides. There were also 133 cases of crime and violence, which featured 14 murders, nine attempted murders, 39 violent actions, 54 violent preoccupations and 17 crimes. The report also showed that 13 individuals had become addicted to Fluoxetine and 14 cases of alcoholism forming or worsening.[72] However, Mayo Clinic psychiatrist Daniel K. Hall-Flavin has stated that people cannot get addicted to antidepressants.[73]
A meta-analysis published in February 2008 combined 35 clinical trials of four newer antidepressants (fluoxetine, paroxetine (Paxil), nefazodone (Serzone) and venlafaxine (Effexor)). These antidepressants belonging to three different pharmacological groups were considered together, and the authors did not analyze them separately. The authors concluded that "although the difference [between the placebo and antidepressants] easily attained statistical significance", it did not meet the criterion for clinical significance, as used by National Institute for Health and Clinical Excellence (UK), "for any but the most severely depressed patients".[74] Some articles in the press using the titles "The creation of the Prozac myth"[75] and "Prozac does not work in majority of depressed patients"[76][77] presented these general findings about the relative efficacy of antidepressants and placebo as the findings about ineffectiveness of fluoxetine. In a follow-up article, the authors of the meta-analysis noted that "unfortunately, during its initial coverage, the media often portrayed the results as “antidepressants do not work”, which misrepresented our more nuanced pattern of findings".[78]
As of April 2, 2010, Fluoxetine (Prozac) is one of four antidepressant drugs that the FAA will allow pilots to take without automatically prohibiting them from piloting an aircraft. The others are Sertraline (Zoloft), Citalopram (Celexa), and Escitalopram (Lexapro).[79]
In popular culture
Because of its wide appeal as a popular antidepressant, Prozac has had numerous references to it in popular culture, including many books, movies, and songs. The book Listening to Prozac was written in 1993 by psychiatrist Peter D. Kramer. The memoir Prozac Nation was written in 1994 by Elizabeth Wurtzel; it was made into a movie of the same name in 2001, starring Christina Ricci. Yet another book, Talking Back to Prozac, was authored in 1994 by psychiatrist Peter Breggin. Israeli-American poet Doron Braunshtein named a musical segment "Listening to Prozac (and Hearing my Brain)" which appears in his spoken word CD "(Between Me and Allen Ginsberg)".
Other brand names
- Zactin (Australia) [80]
- Lovan (Australia) [81]
- Fluohexal (Australia) [82]
- Auscap (Australia) [83]
- Depreks (Turkey) [84]
- Floxet (Hungary; Egis Pharmaceuticals Ltd.) [85]
- Flunil (India) Intas_Biopharmaceuticals
- Prodep (India)
- Fluox (NZ)
- Fluzac (Ireland)
- Fluxen - Флуксен (Ukraine)
References
- ^ a b c "Prozac Pharmacology, Pharmacokinetics,Studies, Metabolism". RxList.com. 2007. http://www.rxlist.com/cgi/generic/fluoxetine_cp.htm. Retrieved 2007-04-14.
- ^ a b Verispan. "Top 200 Generic Drugs by Units in 2010" (PDF). Drug Topics. http://drugtopics.modernmedicine.com/drugtopics/data/articlestandard//drugtopics/252011/727243/article.pdf.
- ^ a b "Fluoxetine Hydrochloride". The American Society of Health-System Pharmacists. http://www.drugs.com/monograph/fluoxetine-hydrochloride.html. Retrieved 3 April 2011.
- ^ http://www.nimh.nih.gov/health/publications/eating-disorders/binge-eating-disorder.shtml
- ^ a b c d e f g "Prozac prescribing information" (PDF). Eli Lilly. 2007-06-21. http://pi.lilly.com/us/prozac.pdf. Retrieved 2008-01-09.
- ^ Uhr M, Tontsch A, Namendorf C, Ripke S, Lucae S, Ising M, Dose T, Ebinger M, Rosenhagen M, Kohli M, Kloiber S, Salyakina D, Bettecken T, Specht M, Pütz B, Binder EB, Müller-Myhsok B, Holsboer F (2008). "Polymorphisms in the Drug Transporter Gene ABCB1 Predict Antidepressant Treatment Response in Depression". Neuron 57 (2): 203–209. doi:10.1016/j.neuron.2007.11.017. PMID 18215618.
- ^ Kato M, Fukuda T, Serretti A, Wakeno M, Okugawa G, Ikenaga Y, Hosoi Y, Takekita Y, Mandelli L, Azuma J, Kinoshita T (2008). "ABCB1 (MDR1) gene polymorphisms are associated with the clinical response to paroxetine in patients with major depressive disorder". Prog. Neuropsychopharmacol. Biol. Psychiatry 32 (2): 398–404. doi:10.1016/j.pnpbp.2007.09.003. PMID 17913323.
- ^ Bolton JM, Sareen J, Reiss JP (2006). "Genital anaesthesia persisting six years after sertraline discontinuation". J Sex Marital Ther 32 (4): 327–330. doi:10.1080/00926230600666410. PMID 16709553. http://www.informaworld.com/openurl?genre=article&doi=10.1080/00926230600666410&magic=pubmed.
- ^ Csoka AB, Bahrick AS, Mehtonen O-P (2008). "Persistent Sexual Dysfunction after Discontinuation of Selective Serotonin Reuptake Inhibitors (SSRIs)". J Sex Med. 5 (1): 227–233. doi:10.1111/j.1743-6109.2007.00630.x. PMID 18173768. http://www.blackwell-synergy.com/doi/abs/10.1111/j.1743-6109.2007.00630.x.
- ^ Settle Jr, E. C.; G. P. Settle (1984). "A case of mania associated with fluoxetine". American Journal of Psychiatry 141 (2). Chouinard, G.; W. Steiner (1986). "A case of mania induced by high-dose fluoxetine treatment". Am J Psychiatry 143 (5): 686. PMID 3485926.
- ^ Mackay, F. J.; N. R. Dunn, L. V. Wilton, G. L. Pearce, S. N. Freemantle, R. D. Mann (1997). "A comparison of fluvoxamine, fluoxetine, sertraline and paroxetine examined by observational cohort studies". Pharmacoepidemiology and Drug Safety 6 (4). Lavin, M. R.; A. Mendelowitz, S. H. Block (1993). "Adverse Reaction to High-Dose Fluoxetine". Journal of clinical psychopharmacology 13 (6): 452–3. doi:10.1097/00004714-199312000-00013. PMID 8120160.
- ^ a b NTP_CERHR Expert Panel Report on Reproductive and Developmental Toxicity of fluoxetine. Center for the Evaluation of Risks to Human Reproduction. April 2004. http://cerhr.niehs.nih.gov/chemicals/fluoxetine/fluoxetine_final.pdf.
- ^ a b Lipinski JF, Mallya G, Zimmerman P, Pope HG (1989). "Fluoxetine-induced akathisia: clinical and theoretical implications". J Clin Psychiatry 50 (9): 339–42. PMID 2549018.
- ^ a b Review:Leo RJ (1996). "Movement disorders associated with the serotonin selective reuptake inhibitors". The Journal of clinical psychiatry 57 (10): 449–454. doi:10.4088/JCP.v57n1002. PMID 8909330.
- ^ Hansen L (2003). "Fluoxetine dose-increment related akathisia in depression: implications for clinical care, recognition and management of selective serotonin reuptake inhibitor-induced akathisia". J. Psychopharmacol. (Oxford) 17 (4): 451–452. doi:10.1177/0269881103174003. PMID 14870959.
- ^ a b Rothschild AJ, Locke CA (1991). "Reexposure to fluoxetine after serious suicide attempts by three patients: the role of akathisia". J Clin Psychiatry 52 (12): 491–3. PMID 1752848.
- ^ Hansen L (2001). "A critical review of akathisia, and its possible association with suicidal behaviour". Human Psychopharmacology Clinical and Experimental 16 (7): 495–505. doi:10.1002/hup.325. PMID 12404546.
- ^ Hansen L, Kingdom D (2006). "Akathisia as a risk factor for suicide". The British journal of psychiatry: the journal of mental science 188 (2): 192–192. doi:10.1192/bjp.188.2.192. PMID 16449715.
- ^ Gerber PE, Lynd LD (1998). "Selective serotonin-reuptake inhibitor-induced movement disorders". Ann Pharmacother 32 (6): 692–698. doi:10.1345/aph.17302. PMID 9640489.
- ^ Caley CF (1997). "Extrapyramidal reactions and the selective serotonin-reuptake inhibitors". Ann Pharmacother 31 (12): 1481–9. PMID 9416386.
- ^ Prozac Medication Insert. Eli Lilly and Company Indianapolis, IN 46285, USA Literature revised December 4, 2006
- ^ Karpova NN; Lindholm, J; Pruunsild, P; Timmusk, T; Castrén, E (2009). "Long-lasting behavioural and molecular alterations induced by early postnatal fluoxetine exposure are restored by chronic fluoxetine treatment in adult mice". Eur Neuropsychopharmacol. 19 (2): 97–108. doi:10.1016/j.euroneuro.2008.09.002. PMID 18973993.
- ^ "Fluoxetine Drug Information Provided by Lexi-Comp". Merck Manual. June 2007. http://www.merck.com/mmpe/lexicomp/fluoxetine.html#NA7E33.
- ^ a b Blum D, Maldonado J, Meyer E, Lansberg M (2008). "Delirium following abrupt discontinuation of fluoxetine". Clin Neurol Neurosurg 110 (1): 69–70. doi:10.1016/j.clineuro.2007.08.016. PMID 17913343.For the earlier case reports see the references cited therein.
- ^ Rosenbaum JF, Zajecka J (1997). "Clinical management of antidepressant discontinuation". J Clin Psychiatry 58 Suppl 7: 37–40. PMID 9219493.
- ^ Schatzberg AF, Blier P, Delgado PL, Fava M, Haddad PM, Shelton RC (2006). "Antidepressant discontinuation syndrome: consensus panel recommendations for clinical management and additional research". J Clin Psychiatry 67 Suppl 4: 27–30. PMID 16683860.
- ^ Fava M (2006). "Prospective studies of adverse events related to antidepressant discontinuation". J Clin Psychiatry 67 Suppl 4: 14–21. PMID 16683858.
- ^ Zajecka J, Fawcett J, Amsterdam J, Quitkin F, Reimherr F, Rosenbaum J, Michelson D, Beasley C (1998). "Safety of abrupt discontinuation of fluoxetine: a randomized, placebo-controlled study". J Clin Psychopharmacol 18 (3): 193–197. doi:10.1097/00004714-199806000-00003. PMID 9617977.
- ^ Gartlehner G, Hansen RA, Thieda P, DeVeaugh-Geiss AM, Gaynes BN, Krebs EE, Lux LJ, Morgan LC, Shumate JA, Monroe LG, Lohr KN. (2007). Comparative Effectiveness of Second-Generation Antidepressants in the Pharmacologic Treatment of Adult Depression. PMID 20704050.
- ^ Levenson M, Holland C. "Antidepressants and Suicidality in Adults: Statistical Evaluation. (Presentation at Psychopharmacologic Drugs Advisory Committee; December 13, 2006)". http://www.fda.gov/ohrms/dockets/ac/06/slides/2006-4272s1-04-FDA.ppt. Retrieved 2007-05-13.
- ^ a b Stone MB, Jones ML (2006-11-17). "Clinical Review: Relationship Between Antidepressant Drugs and Suicidality in Adults" (PDF). Overview for December 13 Meeting of Psychopharmacologic Drugs Advisory Committee (PDAC). FDA. pp. 11–74. http://www.fda.gov/ohrms/dockets/ac/06/briefing/2006-4272b1-01-FDA.pdf. Retrieved 2007-09-22.
- ^ a b Levenson M, Holland C (2006-11-17). "Statistical Evaluation of Suicidality in Adults Treated with Antidepressants" (PDF). Overview for December 13 Meeting of Psychopharmacologic Drugs Advisory Committee (PDAC). FDA. pp. 75–140. http://www.fda.gov/ohrms/dockets/ac/06/briefing/2006-4272b1-01-FDA.pdf. Retrieved 2007-09-22.
- ^ Klein DF (2006). "The flawed basis for FDA post-marketing safety decisions: the example of anti-depressants and children". Neuropsychopharmacology 31 (4): 689–699. doi:10.1038/sj.npp.1300996. PMID 16395296.
- ^ Mann JJ, Ellis SP, Waternaux CM, Liu X, Oquendo MA, Malone KM, Brodsky BS, Haas GL, Currier D (2008). "Classification Trees Distinguish Suicide Attempters in Major Psychiatric Disorders: A Model of Clinical Decision Making". J Clin Psychiatry: e1–e9. PMID 18190232.
- ^ Tarek A. Hammad (2004-09-13). "Results of the Analysis of Suicidality in Pediatric Trials of Newer Antidepressants" (PDF). Presentation at the Meeting of Psychopharmacologic Drugs Advisory Committee and the Pediatric Advisory Committee on September 13, 2004. FDA. pp. 25, 28. http://www.fda.gov/ohrms/dockets/ac/04/slides/2004-4065S1_08_FDA-Hammad.ppt. Retrieved 2008-01-06.
- ^ Committee on Safety of Medicines Expert Working Group (December 2004). "Report on The Safety of Selective Serotonin Reuptake Inhibitor Antidepressants" (PDF). MHRA. http://www.mhra.gov.uk/home/groups/pl-p/documents/drugsafetymessage/con019472.pdf. Retrieved 2007-09-25.
- ^ Gunnell D, Saperia J, Ashby D (2005). "Selective serotonin reuptake inhibitors (SSRIs) and suicide in adults: meta-analysis of drug company data from placebo controlled, randomised controlled trials submitted to the MHRA's safety review". BMJ 330 (7488): 385–0. doi:10.1136/bmj.330.7488.385. PMC 549105. PMID 15718537. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=549105.
- ^ a b Sandson NB, Armstrong SC, Cozza KL (2005). "An overview of psychotropic drug-drug interactions". Psychosomatics 46 (5): 464–494. doi:10.1176/appi.psy.46.5.464. PMID 16145193.
- ^ An extensive list of possible interactions is available in Lexi-Comp (September 2008). "Fluoxetine". The Merck Manual Professional. http://www.merck.com/mmpe/lexicomp/fluoxetine.html. Retrieved on December 28, 2008.
- ^ Munoz-Bellido JL, Munoz-Criado S, Garcìa-Rodrìguez JA Int J Antimicrob Agents. 2000 Apr;14(3):177-80. Antimicrobial activity of psychotropic drugs: selective serotonin reuptake inhibitors. http://www.ncbi.nlm.nih.gov/pubmed/10773485
- ^ Mandrioli R, Forti GC, Raggi MA (February 2006). "Fluoxetine metabolism and pharmacological interactions: the role of cytochrome p450". Current Drug Metabolism 7 (2): 127–133. doi:10.2174/138920006775541561. PMID 16472103. http://www.bentham-direct.org/pages/content.php?CDM/2006/00000007/00000002/0002F.SGM.
- ^ Hiemke C, Härtter S (January 2000). "Pharmacokinetics of selective serotonin reuptake inhibitors". Pharmacology & Therapeutics 85 (1): 11–28. doi:10.1016/S0163-7258(99)00048-0. PMID 10674711. http://linkinghub.elsevier.com/retrieve/pii/S0163-7258(99)00048-0.
- ^ a b Burke WJ, Hendricks SE, McArthur-Miller D, Jacques D, Bessette D, McKillup T, Stull T, Wilson J (2000). "Weekly dosing of fluoxetine for the continuation phase of treatment of major depression: results of a placebo-controlled, randomized clinical trial". J Clin Psychopharmacol 20 (4): 423–427. doi:10.1097/00004714-200008000-00006. PMID 10917403.
- ^ "Drug Treatments in Psychiatry: Antidepressants". Newcastle University School of Neurology, Neurobiology and Psychiatry. 2005. http://www.ncl.ac.uk/nnp/teaching/management/drugrx/antdep.html. Retrieved 2007-04-14.
- ^ a b Pérez V, Puiigdemont D, Gilaberte I, Alvarez E, Artigas F (2001). "Augmentation of fluoxetine's antidepressant action by pindolol: analysis of clinical, pharmacokinetic, and methodologic factors". J Clin Psychopharmacol 21 (1): 36–45. doi:10.1097/00004714-200102000-00008. PMID 11199945.
- ^ Brunswick DJ, Amsterdam JD, Fawcett J, Quitkin FM, Reimherr FW, Rosenbaum JF, Beasley CM (2002). "Fluoxetine and norfluoxetine plasma concentrations during relapse-prevention treatment". J Affect Disord 68 (2–3): 243–249. doi:10.1016/S0165-0327(00)00333-5. PMID 12063152.
- ^ a b c Henry ME, Schmidt ME, Hennen J, Villafuerte RA, Butman ML, Tran P, Kerner LT, Cohen B, Renshaw PF (2005). "A comparison of brain and serum pharmacokinetics of R-fluoxetine and racemic fluoxetine: A 19-F MRS study". Neuropsychopharmacology 30 (8): 1576–1583. doi:10.1038/sj.npp.1300749. PMID 15886723.
- ^ Kinnunen LH, Moltz H, Metz J, Cooper M (2004). "Differential brain activation in exclusively homosexual and heterosexual men produced by the selective serotonin reuptake inhibitor, fluoxetine". Brain Res. 1024 (1–2): 251–254. doi:10.1016/j.brainres.2004.07.070. PMID 15451388.
- ^ Perry KW, Fuller RW (1997). "Fluoxetine increases norepinephrine release in rat hypothalamus as measured by tissue levels of MHPG-SO4 and microdialysis in conscious rats". J Neural Transm 104 (8–9): 953–966. doi:10.1007/BF01285563. PMID 9451727.
- ^ Bymaster FP, Zhang W, Carter PA et al. (April 2002). "Fluoxetine, but not other selective serotonin uptake inhibitors, increases norepinephrine and dopamine extracellular levels in prefrontal cortex". Psychopharmacology (Berl.) 160 (4): 353–361. doi:10.1007/s00213-001-0986-x. PMID 11919662.
- ^ a b Koch S, Perry KW, Nelson DL, Conway RG, Threlkeld PG, Bymaster FP (December 2002). "R-fluoxetine increases extracellular DA, NE, as well as 5-HT in rat prefrontal cortex and hypothalamus: an in vivo microdialysis and receptor binding study". Neuropsychopharmacology 27 (6): 949–959. doi:10.1016/S0893-133X(02)00377-9. PMID 12464452.
- ^ According, FP; Bymaster, FP; Zhang, W; Carter, PA; Chernet, E; Phebus, L; Wong, DT; Perry, KW (2002). "et al. (April 2002). "Fluoxetine, but not other selective serotonin uptake inhibitors, increases norepinephrine and dopamine extracellular levels in prefrontal cortex"". Psychopharmacology (Berl.) 160 (4): 353–361. doi:10.1007/s00213-001-0986-x. PMID 11919662. only injections of 10 and 20 mg/kg fluoxetine resulted in the increase of all three neurotransmitters. 3 mg/kg increased only serotonin and did not increase dopamine and norepinephrine. The injection with 0.7 mg/kg fluoxetine corresponds to the standard therapeutic dose of luoxetine, see Wyneken U, Sandoval M, Sandoval S et al. (November 2006). "Clinically relevant doses of fluoxetine and reboxetine induce changes in the TrkB content of central excitatory synapses". Neuropsychopharmacology 31 (11): 2415–2423. doi:10.1038/sj.npp.1301052. PMID 16554746.
- ^ Miguelez C, Fernandez-Aedo I, Torrecilla M, Grandoso L, Ugedo L (2009). "alpha(2)-Adrenoceptors mediate the acute inhibitory effect of fluoxetine on locus coeruleus noradrenergic neurons". Neuropharmacology 56 (6–7): 1068–1073. doi:10.1016/j.neuropharm.2009.03.004. PMID 19298831.
- ^ De-Spinning In Vitro Data.
- ^ de Gandarias JM, Echevarría E, Acebes I, Abecia LC, Casis O, Casis L (January 1999). "Effects of fluoxetine administration on mu-opoid receptor immunostaining in the rat forebrain". Brain Res. 817 (1–2): 236–240. doi:10.1016/S0006-8993(98)01256-6. PMID 9889376.
- ^ Lemberger L, Bergstrom RF, Wolen RL, Farid NA, Enas GG, Aronoff GR. Fluoxetine: clinical pharmacology and physiologic disposition. J. Clin. Psychiatry 46: 14-19, 1985.
- ^ Pato MT, Murphy DL, DeVane CL. Sustained plasma concentrations of fluoxetine and/or norfluoxetine four and eight weeks after fluoxetine discontinuation. J. Clin. Psychopharmacol. 11: 224-225, 1991.
- ^ R. Baselt, Disposition of Toxic Drugs and Chemicals in Man, 8th edition, Biomedical Publications, Foster City, CA, 2008, pp. 645-648.
- ^ http://www.ncbi.nlm.nih.gov/pubmed/8831113
- ^ http://www.ncbi.nlm.nih.gov/pubmed/20021354
- ^ Wong, DT; Perry KW, Bymaster FP (September 2005). "The Discovery of Fluoxetine Hydrochloride (Prozac)". Nature Reviews Drug Discovery (Nature) 4 (9): 950–950. doi:10.1038/nrd1821. PMID 16121130.
- ^ a b c Wong, DT, Bymaster FP, Engleman EA (1995). "Prozac (fluoxetine, Lilly 110140), the first selective serotonin uptake inhibitor and an antidepressant drug: twenty years since its first publication". Life Sci 57 (5): 411–441. doi:10.1016/0024-3205(95)00209-O. PMID 7623609.
- ^ Wong D, Horng J, Bymaster F, Hauser K, Molloy B (1974). "A selective inhibitor of serotonin uptake: Lilly 110140, 3-(p-trifluoromethylphenoxy)-N-methyl-3-phenylpropylamine". Life Sci 15 (3): 471–479. doi:10.1016/0024-3205(74)90345-2. PMID 4549929.
- ^ Breggin, Peter R.; Ginger Ross Breggin (1995). Talking back to Prozac. Macmillan Publishers. pp. 1–2. ISBN 9780312956066.
- ^ Carlsson A, Wong DT (1997). "A note on the discovery of selective serotonin reuptake inhibitors". Life Sci 61 (12): 1203. doi:10.1016/S0024-3205(97)00662-0. PMID 9315511.
- ^ Swiatek, Jeff (August 2, 2001). "Prozac's profitable run coming to an end for Lilly". The Indianapolis Star. http://www2.indystar.com/library/factfiles/business/companies/lilly/stories/2001_0802.html.
- ^ "Electronic Orange Book". Food and Drug Administration. April 2007. http://www.accessdata.fda.gov/scripts/cder/ob/docs/obdetail.cfm?Appl_No=018936&TABLE1=OB_Rx. Retrieved May 24, 2007.
- ^ "Patent Expiration Dates for Common Brand-Name Drugs". http://www.express-scripts.com/pharmacist/notifications/docs/genericdrugs.htm. Retrieved 2007-07-20.
- ^ Class, Selena (December 2, 2002). "Pharma Overview". http://pubs.acs.org/cen/coverstory/8048/8048pharmaceutical.html. Retrieved 2009-06-15.
- ^ Healy D (2004) Let them eat Prozac. New York: New York University Press. pp 124–148.
- ^ Antidepressants and Violence: Problems at the Interface of Medicine and Law, David Healy, Andrew Herxheimer, and David B. Menkes, PLoS Med 3(9): e372 doi:10.1371/journal.pmed.0030372, 2006
- ^ Breggin, Peter R.; Ginger Ross Breggin (1995). Talking back to Prozac. Macmillan Publishers. p. 154. ISBN 9780312956066.
- ^ http://www.mayoclinic.com/health/antidepressant-withdrawal/AN01425
- ^ Kirsch I, Deacon BJ, Huedo-Medina TB, Scoboria A, Moore TJ, Johnson BT (February 2008). "Initial Severity and Antidepressant Benefits: A Meta-Analysis of Data Submitted to the Food and Drug Administration". PLoS Medicine. http://medicine.plosjournals.org/perlserv/?request=get-document&doi=10.1371/journal.pmed.0050045. Retrieved 2008-02-26.
- ^ "The creation of the Prozac myth". London: The Guardian. February 27, 2008. http://www.guardian.co.uk/society/2008/feb/27/mentalhealth.health1. Retrieved 2008-03-01.
- ^ Day, Michael (2008-02-26). "Prozac does not work in majority of depressed patients". New Scientist. http://www.newscientist.com/article/dn13375-prozac-does-not-work-in-most-depressed-patients.html. Retrieved 2008-03-01.
- ^ Blue, Laura (February 26, 2008). "Antidepressants Hardly Help". Time. http://www.time.com/time/health/article/0,8599,1717306,00.html. Retrieved 2008-03-01.
- ^ Johnson BT; Kirsch I (June 2008). "Do antidepressants work? Statistical significance versus clinical benefits". Significance 5 (2): 54–58. doi:10.1111/j.1740-9713.2008.00286.x. http://www.ingentaconnect.com/content/bpl/sign/2008/00000005/00000002/art00002.
- ^ http://www.faa.gov/news/press_releases/news_story.cfm?newsId=11293.
- ^ http://www.alphapharm.com.au/media/39940/zactin%20cmi.pdf
- ^ http://www.alphapharm.com.au/media/39670/lovan%20cmi.pdf
- ^ http://en.wikipedia.org/wiki/List_of_drugs:_Fl#fluo
- ^ http://www.mydr.com.au/cmis/PDFs/CMI6561.pdf
- ^ http://www.abdiibrahim.com.tr/english/urunler.asp?bolum=9
- ^ http://drugs-about.com/drugs-f/floxet.html
External links
- Biography of Dr. David T. Wong, one of the inventors of Prozac
- Biography of Dr. Bryan B. Molloy, one of the inventors of Prozac
- Trouble in Prozac – Fortune Magazine
- U.S. National Library of Medicine: Drug Information Portal – Fluoxetine
Antidepressants (N06A) Specific reuptake inhibitors (RIs), enhancers (REs), and releasing agents (RAs) Alaproclate • Citalopram • Escitalopram • Femoxetine • Fluoxetine# • Fluvoxamine • Indalpine • Ifoxetine • Litoxetine • Lubazodone • Panuramine • Paroxetine • Pirandamine • Seproxetine • Sertraline# • Vilazodone • Zimelidine‡Bicifadine • Clovoxamine • Desvenlafaxine • Duloxetine • Levomilnacipran • Eclanamine • Milnacipran • Sibutramine • VenlafaxineSerotonin–norepinephrine–dopamine reuptake inhibitors (SNDRIs)Brasofensine • BTS-74,398 • Cocaine • Diclofensine • DOV-21,947 • DOV-102,677 • DOV-216,303 • EXP-561 • Fezolamine • JNJ-7925476 • NS-2359 • PRC200-SS • Pridefine • SEP-225,289 • SEP-227,162 • TesofensineAmedalin • Atomoxetine/Tomoxetine • Binedaline • Ciclazindol • Daledalin • Esreboxetine • Lortalamine • Mazindol • Nisoxetine • Reboxetine • Talopram • Talsupram • Tandamine • ViloxazineDopamine reuptake inhibitors (DRIs)Amineptine • Bupropion/Amfebutamone# • Cilobamine • Manifaxine • Methylphenidate • Nomifensine • Radafaxine • TametralineNorepinephrine-dopamine releasing agents (NDRAs)Serotonin-norepinephrine-dopamine releasing agents (SNDRAs)4-Methyl-αMT • αET/Etryptamine • αMT/MetryptamineOthersIndeloxazine • Teniloxazine • Tramadol • ViqualineReceptor antagonists and/or reuptake inhibitors Serotonin antagonists and reuptake inhibitors (SARIs)Serotonin modulators and stimulators (SMSs)VortioxetineTricyclic and tetracyclic antidepressants (TCAs/TeCAs) TricyclicsAmezepine • Amineptine • Amitriptyline# • Amitriptylinoxide • Azepindole • Butriptyline • Cianopramine • Clomipramine • Cotriptyline • Cyanodothiepin • Demexiptiline • Depramine/Balipramine • Desipramine • Dibenzepin • Dimetacrine • Dosulepin/Dothiepin • Doxepin • Enprazepine • Fluotracen • Hepzidine • Homopipramol • Imipramine • Imipraminoxide • Intriptyline • Iprindole • Ketipramine • Litracen • Lofepramine • Losindole • Mariptiline • Melitracen • Metapramine • Mezepine • Naranol • Nitroxazepine • Nortriptyline • Noxiptiline • Octriptyline • Opipramol • Pipofezine • Propizepine • Protriptyline • Quinupramine • Tampramine • Tianeptine • Tienopramine • Trimipramine;7-OH-Amoxapine • Amoxapine • Aptazapine • Azipramine • Ciclazindol • Ciclopramine • Esmirtazapine • Loxapine • Maprotiline • Mazindol • Mianserin • Mirtazapine • Oxaprotiline • Setiptiline/TeciptilineMonoamine oxidase inhibitors (MAOIs) NonselectiveIrreversible: Benmoxin • Echinopsidine • Iproclozide • Iproniazid • Isocarboxazid • Mebanazine • Metfendrazine • Nialamide • Octamoxin • Phenelzine • Pheniprazine • Phenoxypropazine • Pivalylbenzhydrazine • Safrazine • Tranylcypromine; Reversible: Caroxazone • Paraxazone;MAOA-SelectiveIrreversible: Clorgiline; Reversible: Amiflamine • Bazinaprine • Befloxatone • Befol • Brofaromine • Cimoxatone • Esuperone • Harmala Alkaloids (Harmine, Harmaline, Tetrahydroharmine, Harman, Norharman, etc) • Methylene Blue • Metralindole • Minaprine • Moclobemide • Pirlindole • Sercloremine • Tetrindole • Toloxatone • Tyrima;MAOB-SelectiveIrreversible: Ladostigil • Mofegiline • Pargyline • Rasagiline • Selegiline; Reversible: Lazabemide • MilacemideAzapirones and other 5-HT1A receptor agonists Alnespirone • Aripiprazole • Befiradol • Buspirone • Eptapirone • Flesinoxan • Flibanserin • Gepirone • Ipsapirone • Oxaflozane • Tandospirone • Vilazodone • ZalospironeSerotonergics 5-HT1 receptor ligands Agonists: Azapirones: Alnespirone • Binospirone • Buspirone • Enilospirone • Eptapirone • Gepirone • Ipsapirone • Perospirone • Revospirone • Tandospirone • Tiospirone • Umespirone • Zalospirone; Antidepressants: Etoperidone • Nefazodone • Trazodone • Vortioxetine; Antipsychotics: Aripiprazole • Asenapine • Clozapine • Quetiapine • Ziprasidone; Ergolines: Dihydroergotamine • Ergotamine • Lisuride • Methysergide • LSD; Tryptamines: 5-CT • 5-MeO-DMT • 5-MT • Bufotenin • DMT • Indorenate • Psilocin • Psilocybin; Others: 8-OH-DPAT • Adatanserin • Befiradol • BMY-14802 • Cannabidiol • Dimemebfe • Ebalzotan • Eltoprazine • F-11,461 • F-12,826 • F-13,714 • F-14,679 • F-15,063 • F-15,599 • Flesinoxan • Flibanserin • Lesopitron • LY-293,284 • LY-301,317 • MKC-242 • NBUMP • Osemozotan • Oxaflozane • Pardoprunox • Piclozotan • Rauwolscine • Repinotan • Roxindole • RU-24,969 • S 14,506 • S-14,671 • S-15,535 • Sarizotan • SSR-181,507 • Sunepitron • U-92,016-A • Urapidil • Vilazodone • Xaliproden • Yohimbine
Antagonists: Antipsychotics: Iloperidone • Risperidone • Sertindole; Beta blockers: Alprenolol • Cyanopindolol • Iodocyanopindolol • Oxprenolol • Pindobind • Pindolol • Propranolol • Tertatolol; Others: AV965 • BMY-7,378 • CSP-2503 • Dotarizine • Flopropione • GR-46611 • Isamoltane • Lecozotan • Mefway • Metitepine/Methiothepin • MPPF • NAN-190 • PRX-00023 • Robalzotan • S-15535 • SB-649,915 • SDZ 216-525 • Spiperone • Spiramide • Spiroxatrine • UH-301 • WAY-100,135 • WAY-100,635 • XylamidineAgonists: Lysergamides: Dihydroergotamine • Ergotamine • Methysergide; Piperazines: Eltoprazine • TFMPP; Triptans: Avitriptan • Eletriptan • Sumatriptan • Zolmitriptan; Tryptamines: 5-CT • 5-MT; Others: CGS-12066A • CP-93,129 • CP-94,253 • CP-135,807 • RU-24,969 • Vortioxetine
Antagonists: Lysergamides: Metergoline; Others: AR-A000002 • Elzasonan • GR-127,935 • Isamoltane • Metitepine/Methiothepin • SB-216,641 • SB-224,289 • SB-236,057 • YohimbineAgonists: Lysergamides: Dihydroergotamine • Methysergide; Triptans: Almotriptan • Avitriptan • Eletriptan • Frovatriptan • Naratriptan • Rizatriptan • Sumatriptan • Zolmitriptan; Tryptamines: 5-CT • 5-Ethyl-DMT • 5-MT • 5-(Nonyloxy)tryptamine; Others: CP-135,807 • CP-286,601 • GR-46611 • L-694,247 • L-772,405 • PNU-109,291 • PNU-142,633
Antagonists: Lysergamides: Metergoline; Others: Alniditan • BRL-15,572 • Elzasonan • GR-127,935 • Ketanserin • LY-310,762 • LY-367,642 • LY-456,219 • LY-456,220 • Metitepine/Methiothepin • Ritanserin • Yohimbine • ZiprasidoneAgonists: Lysergamides: Methysergide; Triptans: Eletriptan; Tryptamines: BRL-54443 • Tryptamine
Antagonists: Metitepine/MethiothepinAgonists: Triptans: Eletriptan • Naratriptan • Sumatriptan; Tryptamines: 5-MT; Others: BRL-54443 • Lasmiditan • LY-334,370
Antagonists: Metitepine/Methiothepin5-HT2 receptor ligands Agonists: Lysergamides: ALD-52 • Ergometrine • Lisuride • LA-SS-Az • LSD • LSD-Pip • Lysergic acid 2-butyl amide • Lysergic acid 3-pentyl amide • Methysergide; Phenethylamines: 25I-NBF • 25I-NBMD • 25I-NBOH • 25I-NBOMe • 2C-B • 2C-B-FLY • 2CB-Ind • 2C-C-NBOMe • 2C-E • 2C-I • 2C-TFM-NBOMe • 2C-T-2 • 2C-T-7 • 2C-T-21 • 2CBCB-NBOMe • 2CBFly-NBOMe • Bromo-DragonFLY • DOB • DOC • DOI • DOM • MDA • MDMA • Mescaline • TCB-2 • TFMFly; Piperazines: BZP • Quipazine • TFMPP; Tryptamines: 5-CT • 5-MeO-α-ET • 5-MeO-α-MT • 5-MeO-DET • 5-MeO-DiPT • 5-MeO-DMT • 5-MeO-DPT • 5-MT • α-ET • α-Methyl-5-HT • α-MT • Bufotenin • DET • DiPT • DMT • DPT • Psilocin • Psilocybin; Others: AL-34662 • AL-37350A • Dimemebfe • Medifoxamine • Oxaflozane • PNU-22394 • RH-34
Antagonists: Atypical antipsychotics: Amperozide • Aripiprazole • Carpipramine • Clocapramine • Clozapine • Gevotroline • Iloperidone • Melperone • Mosapramine • Olanzapine • Paliperidone • Pimozide • Quetiapine • Risperidone • Sertindole • Ziprasidone • Zotepine; Typical antipsychotics: Loxapine • Pipamperone; Antidepressants: Amitriptyline • Amoxapine • Aptazapine • Etoperidone • Mianserin • Mirtazapine • Nefazodone • Teniloxazine • Trazodone; Others: 5-I-R91150 • AC-90179 • Adatanserin • Altanserin • AMDA • APD-215 • Blonanserin • Cinanserin • CSP-2503 • Cyproheptadine • Deramciclane • Dotarizine • Eplivanserin • Esmirtazapine • Fananserin • Flibanserin • Ketanserin • KML-010 • Lubazodone • Mepiprazole • Metitepine/Methiothepin • Nantenine • Pimavanserin • Pizotifen • Pruvanserin • Rauwolscine • Ritanserin • S-14,671 • Sarpogrelate • Setoperone • Spiperone • Spiramide • SR-46349B • Volinanserin • Xylamidine • YohimbineAgonists: Oxazolines: 4-Methylaminorex • Aminorex; Phenethylamines: Chlorphentermine • Cloforex • DOB • DOC • DOI • DOM • Fenfluramine • MDA • MDMA • Norfenfluramine; Tryptamines: 5-CT • 5-MT • α-Methyl-5-HT; Others: BW-723C86 • Cabergoline • mCPP • Pergolide • PNU-22394 • Ro60-0175
Antagonists: Agomelatine • Asenapine • EGIS-7625 • Ketanserin • Lisuride • LY-272,015 • Metitepine/Methiothepin • PRX-08066 • Rauwolscine • Ritanserin • RS-127,445 • Sarpogrelate • SB-200,646 • SB-204,741 • SB-206,553 • SB-215,505 • SB-221,284 • SB-228,357 • SDZ SER-082 • Tegaserod • YohimbineAgonists: Phenethylamines: 2C-B • 2C-E • 2C-I • 2C-T-2 • 2C-T-7 • 2C-T-21 • DOB • DOC • DOI • DOM • MDA • MDMA • Mescaline; Piperazines: Aripiprazole • mCPP • TFMPP; Tryptamines: 5-CT • 5-MeO-α-ET • 5-MeO-α-MT • 5-MeO-DET • 5-MeO-DiPT • 5-MeO-DMT • 5-MeO-DPT • 5-MT • α-ET • α-Methyl-5-HT • α-MT • Bufotenin • DET • DiPT • DMT • DPT • Psilocin • Psilocybin; Others: A-372,159 • AL-38022A • CP-809,101 • Dimemebfe • Lorcaserin• Medifoxamine • MK-212 • Org 12,962 • ORG-37,684 • Oxaflozane • PNU-22394 • Ro60-0175 • Ro60-0213 • Vabicaserin • WAY-629 • WAY-161,503 • YM-348
Antagonists: Atypical antipsychotics: Clozapine • Iloperidone • Melperone • Olanzapine • Paliperidone • Pimozide • Quetiapine • Risperidone • Sertindole • Ziprasidone • Zotepine; Typical antipsychotics: Chlorpromazine • Loxapine • Pipamperone; Antidepressants: Agomelatine • Amitriptyline • Amoxapine • Aptazapine • Etoperidone • Fluoxetine • Mianserin • Mirtazapine • Nefazodone • Nortriptyline • Tedatioxetine • Trazodone; Others: Adatanserin • Cinanserin • Cyproheptadine • Deramciclane • Dotarizine • Eltoprazine • Esmirtazapine • FR-260,010 • Ketanserin • Ketotifen • Latrepirdine • Metitepine/Methiothepin • Methysergide • Pizotifen • Ritanserin • RS-102,221 • S-14,671 • SB-200,646 • SB-206,553 • SB-221,284 • SB-228,357 • SB-242,084 • SB-243,213 • SDZ SER-082 • Xylamidine5-HT3, 5-HT4, 5-HT5, 5-HT6, 5-HT7 ligands Agonists: Piperazines: BZP • Quipazine; Tryptamines: 2-Methyl-5-HT • 5-CT; Others: Chlorophenylbiguanide • Butanol • Ethanol • Halothane • Isoflurane • RS-56812 • SR-57,227 • SR-57,227-A • Toluene • Trichloroethane • Trichloroethanol • Trichloroethylene • YM-31636
Antagonists: Antiemetics: AS-8112 • Alosetron • Azasetron • Batanopride • Bemesetron • Cilansetron • Dazopride • Dolasetron • Granisetron • Lerisetron • Ondansetron • Palonosetron • Ramosetron • Renzapride • Tropisetron • Zacopride • Zatosetron; Atypical antipsychotics: Clozapine • Olanzapine • Quetiapine; Tetracyclic antidepressants: Amoxapine • Mianserin • Mirtazapine; Others: CSP-2503 • ICS-205,930 • MDL-72,222 • Memantine • Nitrous Oxide • Ricasetron • Sevoflurane • Tedatioxetine • Thujone • Vortioxetine • XenonAgonists: Gastroprokinetic Agents: Cinitapride • Cisapride • Dazopride • Metoclopramide • Mosapride • Prucalopride • Renzapride • Tegaserod • Velusetrag • Zacopride; Others: 5-MT • BIMU8 • CJ-033,466 • PRX-03140 • RS-67333 • RS-67506 • SL65.0155 • Antagonists: GR-113,808 • GR-125,487 • L-Lysine • Piboserod • RS-39604 • RS-67532 • SB-203,186 • SB-204,070Agonists: Lysergamides: Ergotamine • LSD; Tryptamines: 5-CT; Others: Valerenic Acid
Antagonists: Asenapine • Latrepirdine • Metitepine/Methiothepin • Ritanserin • SB-699,551
* Note that the 5-HT5B receptor is not functional in humans.Agonists: Lysergamides: Dihydroergotamine • Ergotamine • Lisuride • LSD • Mesulergine • Metergoline • Methysergide; Tryptamines: 2-Methyl-5-HT • 5-BT • 5-CT • 5-MT • Bufotenin • E-6801 • E-6837 • EMD-386,088 • EMDT • LY-586,713 • Tryptamine; Others: WAY-181,187 • WAY-208,466
Antagonists: Antidepressants: Amitriptyline • Amoxapine • Clomipramine • Doxepin • Mianserin • Nortriptyline; Atypical antipsychotics: Aripiprazole • Asenapine • Clozapine • Fluperlapine • Iloperidone • Olanzapine • Tiospirone; Typical antipsychotics: Chlorpromazine • Loxapine; Others: BGC20-760 • BVT-5182 • BVT-74316 • Cerlapirdine • EGIS-12,233 • GW-742,457 • Ketanserin • Latrepirdine • Lu AE58054 • Metitepine/Methiothepin • MS-245 • PRX-07034 • Ritanserin • Ro04-6790 • Ro 63-0563 • SB-258,585 • SB-271,046 • SB-357,134 • SB-399,885 • SB-742,457Agonists: Lysergamides: LSD; Tryptamines: 5-CT • 5-MT • Bufotenin; Others: 8-OH-DPAT • AS-19 • Bifeprunox • E-55888 • LP-12 • LP-44 • RU-24,969 • Sarizotan
Antagonists: Lysergamides: 2-Bromo-LSD • Bromocriptine • Dihydroergotamine • Ergotamine • Mesulergine • Metergoline • Methysergide; Antidepressants: Amitriptyline • Amoxapine • Clomipramine • Imipramine • Maprotiline • Mianserin; Atypical antipsychotics: Amisulpride • Aripiprazole • Clozapine • Olanzapine • Risperidone • Sertindole • Tiospirone • Ziprasidone • Zotepine; Typical antipsychotics: Chlorpromazine • Loxapine; Others: Butaclamol • EGIS-12,233 • Ketanserin • LY-215,840 • Metitepine/Methiothepin • Pimozide • Ritanserin • SB-258,719 • SB-258,741 • SB-269,970 • SB-656,104 • SB-656,104-A • SB-691,673 • SLV-313 • SLV-314 • Spiperone • SSR-181,507 • VortioxetineReuptake inhibitors Selective serotonin reuptake inhibitors (SSRIs): Alaproclate • Citalopram • Dapoxetine • Desmethylcitalopram • Desmethylsertraline • Escitalopram • Femoxetine • Fluoxetine • Fluvoxamine • Indalpine • Ifoxetine • Litoxetine • Lubazodone • Panuramine • Paroxetine • Pirandamine • RTI-353 • Seproxetine • Sertraline • Tedatioxetine • Vilazodone • Vortioxetine • Zimelidine; Serotonin-norepinephrine reuptake inhibitors (SNRIs): Bicifadine • Desvenlafaxine • Duloxetine • Eclanamine • Levomilnacipran • Milnacipran • Sibutramine • Venlafaxine; Serotonin-norepinephrine-dopamine reuptake inhibitors (SNDRIs): Brasofensine • Diclofensine • DOV-102,677 • DOV-21,947 • DOV-216,303 • NS-2359 • SEP-225289 • SEP-227,162 • Tesofensine; Tricyclic antidepressants (TCAs): Amitriptyline • Butriptyline • Cianopramine • Clomipramine • Desipramine • Dosulepin • Doxepin • Imipramine • Lofepramine • Nortriptyline • Pipofezine • Protriptyline • Trimipramine; Tetracyclic antidepressants (TeCAs): Amoxapine; Piperazines: Nefazodone • Trazodone; Antihistamines: Brompheniramine • Chlorphenamine • Diphenhydramine • Mepyramine/Pyrilamine • Pheniramine • Tripelennamine; Opioids: Pethidine • Methadone • Propoxyphene; Others: Cocaine • CP-39,332 • Cyclobenzaprine • Dextromethorphan • Dextrorphan • EXP-561 • Fezolamine • Mesembrine • Nefopam • PIM-35 • Pridefine • Roxindole • SB-649,915 • ZiprasidoneReleasing agents Aminoindanes: 5-IAI • AMMI • ETAI • MDAI • MDMAI • MMAI • TAI; Aminotetralins: 6-CAT • 8-OH-DPAT • MDAT • MDMAT; Oxazolines: 4-Methylaminorex • Aminorex • Clominorex • Fluminorex; Phenethylamines (also Amphetamines, Cathinones, Phentermines, etc): 2-Methyl-MDA • 4-CAB • 4-FA • 4-FMA • 4-HA • 4-MTA • 5-APDB • 5-Methyl-MDA • 6-APDB • 6-Methyl-MDA • AEMMA • Amiflamine • BDB • BOH • Brephedrone • Butylone • Chlorphentermine • Cloforex • Amfepramone • Metamfepramone • DCA • DFMDA • DMA • DMMA • EBDB • EDMA • Ethylone • Etolorex • Fenfluramine (Dexfenfluramine) • Flephedrone • IAP • IMP • Lophophine • MBDB • MDA • MDEA • MDHMA • MDMA • MDMPEA • MDOH • MDPEA • Mephedrone • Methedrone • Methylone • MMA • MMDA • MMDMA • MMMA • NAP • Norfenfluramine • 4-TFMA • pBA • pCA • pIA • PMA • PMEA • PMMA • TAP; Piperazines: 2C-B-BZP • 2-BZP • 3-MeOPP • BZP • DCPP • MBZP • mCPP • MDBZP • MeOPP • Mepiprazole • pCPP • pFPP • pTFMPP • TFMPP; Tryptamines: 4-Methyl-αET • 4-Methyl-αMT • 5-CT • 5-MeO-αET • 5-MeO-αMT • 5-MT • αET • αMT • DMT • Tryptamine (itself); Others: Indeloxazine • Tramadol • ViqualineEnzyme inhibitors AGN-2979 • FenclonineNonselective: Benmoxin • Caroxazone • Echinopsidine • Furazolidone • Hydralazine • Indantadol • Iproclozide • Iproniazid • Isocarboxazid • Isoniazid • Linezolid • Mebanazine • Metfendrazine • Nialamide • Octamoxin • Paraxazone • Phenelzine • Pheniprazine • Phenoxypropazine • Pivalylbenzhydrazine • Procarbazine • Safrazine • Tranylcypromine; MAO-A Selective: Amiflamine • Bazinaprine • Befloxatone • Befol • Brofaromine • Cimoxatone • Clorgiline • Esuprone • Harmala alkaloids (Harmine, Harmaline, Tetrahydroharmine, Harman, Norharman, etc) • Methylene Blue • Metralindole • Minaprine • Moclobemide • Pirlindole • Sercloremine • Tetrindole • Toloxatone • TyrimaOthers Ferrous iron (Fe2+) • Magnesium (Mg2+) • Tetrahydrobiopterin • Vitamin B3 (Niacin, Nicotinamide → NADPH) • Vitamin B6 (Pyridoxine, Pyridoxamine, Pyridoxal → Pyridoxal phosphate) • Vitamin B9 (Folic Acid → Tetrahydrofolic acid) • Vitamin C (Ascorbic acid) • Zinc (Zn2+)OthersEli Lilly and Company Corporate directors John C. Lechleiter · Ralph Alvarez · Sir Winfried Bischoff · Michael L. Eskew · Martin S. Feldstein · J. Erik Fyrwald · Alfred G. Gilman · Karen N. Horn · Ellen R. Marram · Douglas R. Oberhelman · Franklyn G. Prendergast · Kathi P. SeifertProducts Alimta (pemetrexed) · Gemzar (gemcitabine hydrochloride) · ReoPro (abciximab) · Byetta · Glucagon · Humulin · Humalog · Cymbalta (duloxetine hydrochloride) · Cialis · Cymbalta · Humatrope · Prozac · Strattera · Symbyax · Zyprexa · Evista · Forteo · XigrisAnnual revenue: $20.4 billion USD ( -10.17% FY 2008) · Employees: 40,250 · Stock symbol: NYSE: LLY · Website: www.lilly.comCategories:
-10.17% FY 2008) · Employees: 40,250 · Stock symbol: NYSE: LLY · Website: www.lilly.comCategories:- Selective serotonin reuptake inhibitors
- Eli Lilly and Company
- World Health Organization essential medicines
- Phenol ethers
- Organofluorides
- InChI=1S/C17H18F3NO/c1-21-12-11-16(13-5-3-2-4-6-13)22-15-9-7-14(8-10-15)17(18,19)20/h2-10,16,21H,11-12H2,1H3




Wikimedia Foundation. 2010.