- Deep vein thrombosis
-
"DVT" redirects here. For other uses, see DVT (disambiguation).
Deep vein thrombosis Classification and external resources 
A deep vein thrombosis in the right leg. Note the swelling and redness.ICD-10 I80.2 ICD-9 453.40 DiseasesDB 3498 MedlinePlus 000156 eMedicine med/2785 MeSH D020246 Deep vein thrombosis (DVT) (also known as deep venous thrombosis or economy class syndrome) is the formation of a blood clot ("thrombus") in a deep vein. Deep vein thrombosis commonly affects the leg veins (such as the femoral vein or the popliteal vein) or the deep veins of the pelvis. Occasionally the veins of the arm are affected (such as in Paget-Schrötter disease). A DVT can occur without symptoms, but in many cases the affected extremity will be painful, swollen, red, and warm, and the superficial veins may be engorged. The most serious complication of a DVT is that the clot could dislodge and travel to the lungs, which is called a pulmonary embolism (PE). DVT is a medical emergency, so, all limb swellings, however trivial, should be regarded as a DVT until proven otherwise. Untreated lower extremity DVT has a 3% PE-related mortality rate. Deaths associated with upper extremity DVT are extremely rare.[1] A late complication of DVT is the post-thrombotic syndrome, which can manifest itself as edema, pain or discomfort and skin problems.
According to Virchow's triad, venous thrombosis occurs via three mechanisms: decreased flow rate of the blood, damage to the blood vessel wall and an increased tendency of the blood to clot (hypercoagulability). Several medical conditions can lead to DVT, such as compression of the veins, physical trauma, cancer, infections, certain inflammatory diseases and specific conditions such as stroke, heart failure or nephrotic syndrome. There are several factors which can increase a person's risk for DVT, including surgery, hospitalization, immobilization (such as when orthopedic casts are used, or during long-haul flights, leading to traveller's thrombosis), smoking, obesity, age, certain drugs (such as estrogen, or erythropoietin) and inborn tendencies to form clots known as thrombophilia (for example, in carriers of factor V Leiden). Women have an increased risk during pregnancy, if they are on oral contraceptives, and in the postnatal period, due to increased estrogen levels.
The most commonly used tests for the diagnosis of DVT are a blood test called D-dimers and doppler ultrasound of the affected veins. Sometimes, further testing is required to find the cause of the DVT. In specific cases, an attempt can be made to break down the clot (using thrombolytic agents). To prevent further accrual and formation of new clots with a risk of pulmonary embolism, anticoagulation (blood thinners) is advised (if not possible, an inferior vena cava filter may be used). Prevention of DVT is advised in many medical and surgical inpatients using anticoagulants, graduated compression stockings (also known as thromboembolic deterrent stockings) or intermittent pneumatic compression (IPC) devices.
Contents
Signs and symptoms
There may be no symptoms referable to the location of the DVT, but the classical symptoms of DVT include pain, swelling and redness of the leg and dilation of the surface veins. In up to 25% of all hospitalized patients, there may be some form of DVT, which often remains clinically inapparent (unless pulmonary embolism develops).
There are several techniques during physical examination to increase the detection of DVT, such as measuring the circumference of the affected and the contralateral limb at a fixed point (to objectivate edema), and palpating the venous tract, which is often tender. Physical examination is unreliable for excluding the diagnosis of deep vein thrombosis.
In phlegmasia alba dolens, the leg is pale and cool with a diminished arterial pulse caused by spasm. It usually results from acute occlusion of the iliac and femoral veins because of DVT.
In phlegmasia cerulea dolens, there is an acute and nearly total venous occlusion of the entire extremity outflow, including the iliac and femoral veins. The leg is usually painful, cyanosed (blue from lack of oxygen) and edematous (filled with fluid). Venous gangrene may supervene.
It is vital that the possibility of pulmonary embolism be included in the history, as this may warrant further investigation (see pulmonary embolism).
A careful history has to be taken considering risk factors (see below), including the use of estrogen-containing methods of hormonal contraception, recent long-haul flying, intravenous drug use and a history of miscarriage (which is a feature of several disorders that can also cause thrombosis). In the case of long-haul flying, recent studies have shown that risk of DVT is higher in travellers who smoke, are obese, or are currently taking contraceptive pills.[2] A family history can reveal a hereditary factor in the development of DVT. Approximately 35 percent of DVT patients have at least one hereditary thrombophilia, including deficiencies in the anticoagulation factors protein C, protein S, antithrombin, or mutations in the factor V and prothrombin genes.[3]
Cause
The most common risk factors are recent surgery or hospitalization.[4][5] 40% of these patients did not receive heparin prophylaxis. Other risk factors include advanced age, obesity, infection, immobilization, use of combined (estrogen-containing) forms of hormonal contraception, tobacco usage and air travel ("economy class syndrome", a combination of immobility and relative dehydration).[5][6] Thrombophilia (tendency to develop thrombosis) often expresses itself with recurrent thromboses.
Traveller's thrombosis
Traveller's thrombosis is the occurrence of deep vein thrombosis in travellers.[7][8] The term economy class syndrome has also been used to describe this.[9] Traveller's Thrombosis is most commonly reported in people who have travelled long distances by aircraft and who are already at an increased risk of thrombosis. A deep venous thrombosis can lead to the fatal complication of pulmonary embolism. Although all these diseases had been recognised for a long time,[10][11] the possibility of litigation against airline companies brought them into the limelight when this syndrome was reported.
The mechanism for thrombosis in travellers is probably due to a combination of immobilisation, dehydration and underlying risk factors. Additional environmental factors during air travel may also play a role.[12][13] Although the problem has been specifically related to air travel, it would appear that the problem is linked to immobility and that all travellers, including travellers by bus, train and car, are equally at risk.[14]
Patients with diseases that predispose them to thrombosis, such as antiphospholipid syndrome or cancer, are at a much greater risk. The highest risk groups include the elderly, those suffering serious medical conditions such as cancer, those with recent orthopedic surgery (legs or knees) and pregnant women.[15] Some researchers believe that endurance-type athletes are a high risk group.[16]
The WRIGHT (World Health Organisation Research Into Global Hazards of Travel) project has investigated the association between travel and venous thromboembolism (VTE), a term which covers deep vein thrombosis and/or pulmonary embolism (PE).[17] This has reported that the risk of VTE approximately doubles after a long–haul flight (>4 hours) and also with other forms of travel where travellers are exposed to prolonged seated immobility. Risk increases with the duration of the travel and also in passengers having other known risk factors of VTE.
An International Consensus Statement on Traveller's Thrombosis was published in 2008.[18]
Pathophysiology
Virchow's triad is a group of three factors known to affect clot formation: rate of flow (stasis), the consistency of the blood (high viscosity), and quality of the vessel wall (epithelial dysfunction). Virchow noted that more deep venous thrombosis occurred in the left leg than in the right and proposed compression of the left common iliac vein by the overlying right common iliac artery as the underlying cause (see May-Thurner syndrome).[19]
It is recognized that thrombi usually develop first in the calf veins, "growing" in the direction of flow of the vein. DVTs are distinguished as being above or below the popliteal vein. Very extensive DVTs can extend into the iliac veins or the inferior vena cava. The risk of pulmonary embolism is higher in the presence of more extensive clots.
Diagnosis
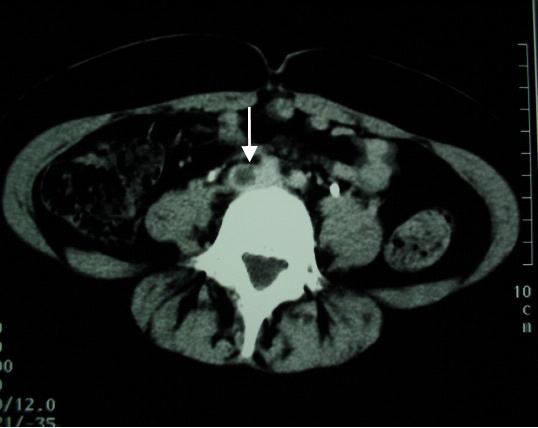
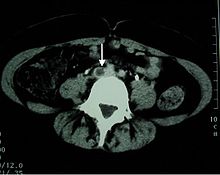 Abdominal computed tomographic scan showing a common iliac vein thrombosis. The arrow indicates the filling defect in the vein visualised using radiocontrast.
Abdominal computed tomographic scan showing a common iliac vein thrombosis. The arrow indicates the filling defect in the vein visualised using radiocontrast.
The gold standard is intravenous venography, which involves injecting a peripheral vein of the affected limb with a contrast agent and taking X-rays, to reveal whether the venous supply has been obstructed. Because of its invasiveness, this test is rarely performed.
Physical examination
Homans sign: Dorsiflexion of foot elicits pain in posterior calf. Pratt's sign: Squeezing of posterior calf elicits pain. However, these medical signs do not perform well and are not included in clinical prediction rules that combine best findings in order to diagnose DVT.[20]
Probability scoring
In 2006, Scarvelis and Wells overviewed a set of clinical prediction rules for DVT,[21] on the heels of a widely adopted set of clinical criteria for pulmonary embolism.[22][23]
Wells score or criteria: (Possible score -2 to 9)
- Active cancer (treatment within last 6 months or palliative) +1 point
- Calf swelling >3 cm compared to other calf (measured 10 cm below tibial tuberosity) +1 point
- Collateral superficial veins (non-varicose) +1 point
- Pitting edema (confined to symptomatic leg) +1 point
- Previous documented DVT +1 point.
- Swelling of entire leg +1 point
- Localized pain along distribution of deep venous system +1 point
- Paralysis, paresis, or recent cast immobilization of lower extremities +1 point
- Recently bedridden > 3 days, or major surgery requiring regional or general anesthetic in past 4 weeks +1 point
- Alternative diagnosis at least as likely -2 points
Interpretation:
- Score of 2 or higher — deep vein thrombosis is likely. Consider imaging the leg veins.
- Score of less than 2 — deep vein thrombosis is unlikely. Consider blood test such as d-dimer test to further rule out deep vein thrombosis.
Blood tests
D-dimer
In a low-probability situation, current practice is to commence investigations by testing for D-dimer levels. This cross-linked fibrin degradation product is an indication that thrombosis is occurring, and that the blood clot is being dissolved by plasmin. A low D-dimer level should prompt other possible diagnoses (such as a ruptured Baker's cyst, if the patient is at sufficiently low clinical probability of DVT).[24][25]
Other blood tests
Other blood tests usually performed at this point are[citation needed]:
- complete blood count
- Primary coagulation studies: PT, APTT, Fibrinogen
- liver enzymes
- renal function and electrolytes
Imaging
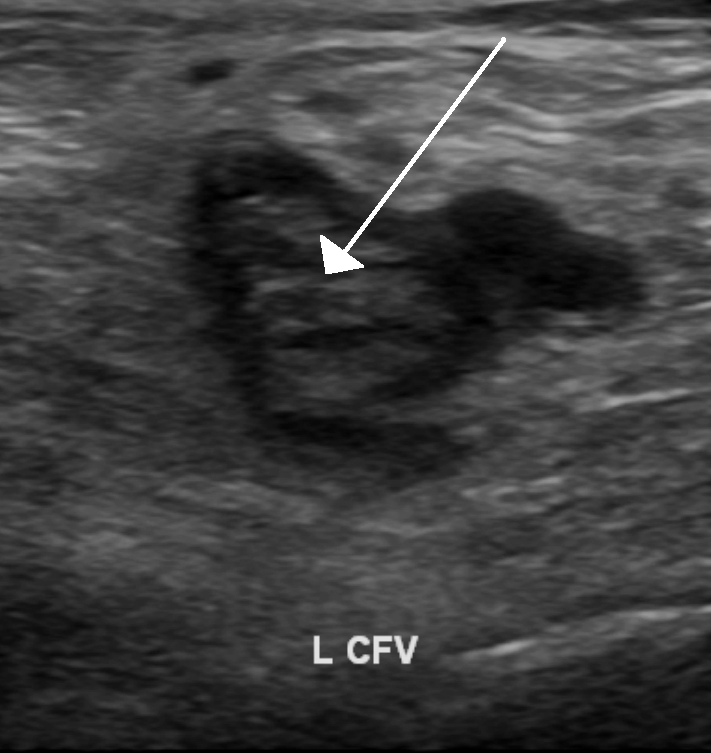
 An ultrasound image demonstrating a blood clot in the left common femoral vein.
An ultrasound image demonstrating a blood clot in the left common femoral vein.Impedance plethysmography, Doppler ultrasonography, compression ultrasound scanning of the leg veins, combined with duplex measurements (to determine blood flow), can reveal a blood clot and its extent (i.e. whether it is below or above the knee). Duplex Ultrasonography, due to its high sensitivity, specificity and reproducibility, has replaced venography as the most widely used test in the evaluation of the disease. This test involves both a B mode image and Doppler flow analysis. It is most sensitive and specific for detecting proximal thrombi (in the popliteal and femoral veins), but substantially less so for distal thrombi (in the calf veins).[26]
Prevention
Medical inpatients
Clinical practice guidelines state:
- American College of Physicians (ACP) in 2011:[27][28]
- "ACP recommends assessment of the risk for thromboembolism and bleeding in medical (including stroke) patients prior to initiation of prophylaxis of venous thromboembolism (Grade: strong recommendation, moderate-quality evidence)."
- "ACP recommends pharmacologic prophylaxis with heparin or a related drug for venous thromboembolism in medical (including stroke) patients unless the assessed risk for bleeding outweighs the likely benefits (Grade: strong recommendation, moderate-quality evidence)."
- "ACP recommends against the use of mechanical prophylaxis with graduated compression stockings for prevention of venous thromboembolism (Grade: strong recommendation, moderate-quality evidence)."
- "ACP does not support the application of performance measures in medical (including stroke) patients that promotes universal venous thromboembolism prophylaxis regardless of risk."
- American College of Chest Physicians (ACCP) in 2008:[15]
- "For acutely ill medical patients admitted to hospital with congestive heart failure or severe respiratory disease, or who are confined to bed and have one or more additional risk factors, including active cancer, previous VTE, sepsis, acute neurologic disease, or inflammatory bowel disease, we recommend thromboprophylaxis with LMWH (Grade 1A), LDUH (Grade 1A), or fondaparinux (Grade 1A)."
Enoxaparin or unfractionated heparin may be used.[29]
LMWH may be more effective than unfractionated heparin (UFH). If UFH is used, 5000 U 3 times daily may be more effective.[30]
Since publication of the ACCP guidelines, an additional randomized controlled trial[31] and meta-analysis[32] including the trial have been published. The meta-analysis concluded " Anticoagulant prophylaxis is effective in preventing symptomatic venous thromboembolism during anticoagulant prophylaxis in at-risk hospitalized medical patients. Additional research is needed to determine the risk for venous thromboembolism in these patients after prophylaxis has been stopped." With regards to which patients are at risk, most studies in the meta-analysis were of patients with New York Heart Association Functional Classification (NYHA) III-IV heart failure. Regarding patients at lesser risk of DVT, the trial above[31] and an earlier trial[33] are relevant yet inconclusive.
Since the ACCP guidelines, compression stockings have been studied for preventing clots in stroke patients.[34][35] In stroke patients, thigh-length stockings are more effective than knee stockings in the nonblinded CLOTS 2 randomized controlled trial[35] while thigh-length stockings were not better than no stockings in the CLOTS 1 nonblinded randomized controlled trial.[34] It is not clear why these two trials conflict.[36]
An effective preventative measure is early ambulation. [37]
Chronic renal dialysis patients may be at increased risk of thromboembolism,[38] but randomized controlled trials have not addressed the risk benefit of prophylaxis.
Surgery patients
In patients who have undergone surgery, low molecular weight heparins (LMWH) are routinely administered to prevent thrombosis. LMWH can only currently be administered subcutaneously by injection. Prophylaxis for pregnant women who have a history of thrombosis may be limited to LMWH injections or may not be necessary if their risk factors are mainly temporary.
Early and regular ambulation (walking) is a treatment that predates anticoagulants and is still recognized and used today. Walking activates the body's muscle pumps, increasing venous velocity and preventing stasis. IPC devices have proven protective in bed- or chair-ridden patients at very high risk or with contraindications to heparins. IPC machines use air bladders that are wrapped around the thigh and/or calf. The bladders alternately inflate and deflate, squeezing the muscles and increasing blood velocity by as much as 500%. IPC machines have been proven effective on knee and hip surgery patients (a population with a risk as high as 80% with no prophylactic treatment) of developing DVT and PE.
Pregnancy
See also: Hypercoagulability in pregnancyThe risk of deep vein thrombosis is increased in pregnancy because of a physiologically adaptive mechanism of increased hypercoagulability to prevent postpartum hemorrhage.[39] However, when combined with an additional underlying hypercoagulable states, the risk of thrombosis or embolism may become substantial.[39]
While the general consensus among physicians is that the safety of the mother supersedes the safety of the developing fetus, changes in the anticoagulation regimen during pregnancy can be performed to minimize the risks to the developing fetus while maintaining therapeutic levels of anticoagulation in the mother.
The main issue with anticoagulation in pregnancy is that warfarin, the most commonly used anticoagulant in chronic administration, is known to have teratogenic effects on the fetus if administered in early pregnancy.[40][41]
Travellers
A Cochrane review in 2006 concluded that passengers can expect a substantial reduction in the incidence of symptomless DVT and leg oedema if they wear compression stockings.[42] A randomised study in 2001 compared two sets of long haul airline passengers over the age of 50; one set wore MediUK mediven travel compression hosiery, while the other did not. The passengers were all scanned and blood tested to check for the incidence of DVT. The results showed that asymptomatic DVT occurred in 10% of the passengers who did not wear compression socks, whilst the group wearing compression had no DVTs. The authors concluded that wearing elastic compression hosiery reduces the incidence of DVT in long haul airline passengers. However it is worth noting that an asymptomatic DVT incidence of 10% is much higher than the expected symptomatic rate (alternatively estimated at less than 0.25%[43]) and wearing compression stockings was also associated with symptomatic superficial thrombophlebitis in 4%.[44]
Plane travellers who travel on the window seat have double risk of DVT.[45]
Prevention consists of adequate hydration (drinking, abstaining from alcoholic beverages and caffeine), moving around and calf muscle exercises.[8] Any traveller with significant risk factors should seek medical advice and be considered for prophylaxis. Aspirin alone is not recommended.[15] Severe risk for thrombosis can prompt a physician to prescribe injections with low molecular weight heparin (LMWH), a form of prophylaxis already in common use in hospital patients.[15]
Management
Anticoagulation
Anticoagulation is the usual treatment for DVT. In general, patients are initiated on a brief course (i.e., less than a week) of heparin treatment while they start on a 3- to 6-month course of warfarin (or related vitamin K inhibitors). Low molecular weight heparin (LMWH) is preferred,[46] though unfractionated heparin is given in patients who have a contraindication to LMWH (e.g., renal failure or imminent need for invasive procedure). In patients who have had recurrent DVTs (two or more), anticoagulation is generally "life-long." The Cochrane Collaboration has meta-analyzed the risk and benefits of prolonged anti-coagulation.[47] Once the thrombosis is treated with RBC-thinning agents, the affected area has a fair chance of returning to its normal proportions. However, thinning agents do not lessen the chance of embolism to the pulmonary or coronary arteries. Thus, while the area affected with deep venous thrombosis (i.e. the legs) may cease coagulation, pulmonary embolism is still as possible. In a 2008 Cochrane review, it was found that anticoagulation used in combination with leg compression is a more effective therapy than anticoagulation alone.[48]
An abnormal D-dimer level at the end of treatment might signal the need for continued treatment among patients with a first unprovoked proximal deep-vein thrombosis.[49]
Despite the fact that no one disputes this, based on a meta analysis done by the Cochrane Collaboration where they found only one randomized trial of anti coagulation vs placebo in the treatment of VTE in which there was no significant difference between the two.[50]
Current recommendations for initial treatment of acute DVT include initiation of a vitamin K antagonist (VKA) together with LMWH or UFH on the first treatment day.[51] Heparin may be discontinued when the international normalized ratio (INR) is stable and greater than 2.0. For the duration and intensity of treatment for acute DVT of the leg, the recommendations include the following:
- for patients with a first episode of DVT secondary to a transient (reversible) risk factor, long-term treatment with a VKA for 3 months.
- for patients with a first episode of idiopathic DVT, treatment with a VKA for at least 6 to 12 months. The dose of VKA is adjusted to maintain INR in the range of 2.0 to 3.0.
- for the prevention of the post-thrombotic syndrome, the use of an elastic compression stocking is recommended.
Thrombolysis
Thrombolysis is generally reserved for extensive clot, e.g. an iliofemoral thrombosis. Although a meta-analysis of randomized controlled trials by the Cochrane Collaboration shows improved outcomes with thrombolysis,[52] there may be an increase in serious bleeding complications. In July 2008, the American College of Chest Physicians (ACCP) published new evidence-based clinical guidelines for the treatment of venous thromboembolic (VTE) disease which for the first time suggested the use of pharmacomechanical thrombolysis in the treatment of certain cases of acute DVT. Complete 2008 ACCP VTE guidelines can be downloaded at no charge at: TheNewGuidelines.org
Thrombectomy
Thrombus can be removed with a mechanical thrombectomy device. Combination therapy that uses mechanical thrombectomy to deliver localized thrombolytics has recently received considerable attention as a treatment for DVT.
Compression stockings
Elastic compression stockings should be routinely applied "beginning within 1 month of diagnosis of proximal DVT and continuing for a minimum of 1 year after diagnosis".[46] Starting within one week may be more effective.[53] They reduce the risk of postthrombotic syndrome.[54] The stockings in almost all trials were stronger than routine anti-embolism stockings and created either 20–30 mm Hg or 30–40 mm Hg. Most trials used knee-high stockings. A meta-analysis of randomized controlled trials by the Cochrane Collaboration showed reduced incidence of post-thrombotic syndrome.[55] The number needed to treat is relatively high, at 4 to 5 patients needing to have been treated to prevent one case of post-thrombotic syndrome.[56]
Compression Systems
Intermittent pneumatic compression (IPC) can be of benefit to patients deemed to be at risk of deep vein thrombosis. IPC is an accepted treatment method for preventing blood clots or deep venous thromboses (DVTs) and complications of venous stasis in persons after trauma, orthopaedic surgery, neurosurgery, or in disabled persons who are unable to walk or mobilise effectively.
Intermittent pneumatic compression (IPC) uses an air pump to inflate and deflate an airtight bag wrapped around the leg. This technique is also used to stop blood clots developing during surgery. However, the review of trials found conflicting evidence about whether or not IPC is better than compression bandages and hosiery. Intermittent pneumatic compression (IPC) is better for healing leg ulcers than no compression but it is uncertain if it improves healing when bandages or hosiery are already used [57]
Inferior vena cava filter
Inferior vena cava filter reduces pulmonary embolism[58] and is an option for patients with an absolute contraindiciation to anticoagulant treatment (e.g., cerebral hemorrhage) or those rare patients who have objectively documented recurrent PEs while on anticoagulation, an inferior vena cava filter (also referred to as a Greenfield filter) may prevent pulmonary embolisation of the leg clot. However these filters are themselves potential of thrombosis,[59] IVC filters are viewed as a temporizing measure for preventing life-threatening pulmonary embolism.[60]
Hospitalization
Treatment at home is an option according to a meta-analysis by the Cochrane Collaboration.[61] Hospitalization should be considered in patients with more than two of the following risk factors as these patients may have more risk of complications during treatment[62]:
- bilateral DVT
- renal insufficiency
- low body weight (<70 kg/154 lbs)
- recent immobility
- chronic heart failure
- cancer
Prognosis
Main article: Post-thrombotic syndromeIn the one to two year period after the initial development of symptoms of deep vein thrombosis (DVT), post-thrombotic syndrome occurs in between as little as a fifth, and as much as half of cases. A "severe" post-thrombotic syndrome likewise varies in frequency between a twentieth and a tenth of individuals diagnosed with DVT. This malady is sometimes characterized by varicose ulceration.[63]
Epidemiology
DVTs occur in about 1 per 1000 persons per year. It is estimated that approximately 350,000 to 600,000 Americans each year suffer from DVT and pulmonary embolism and at least 100,000 deaths may be directly or indirectly related to these diseases.[64]
DVT is much less common in the pediatric population. About 1 in 100,000 people under the age of 18 experiences deep vein thrombosis, possibly due to a child's high rate of heartbeats per minute, relatively active lifestyle when compared with adults, and fewer comorbidities (e.g. malignancy).
In pregnant women, it has an incidence of 0.5 to 7 per 1,000 pregnancies, and is the second most common cause of maternal death in developed countries after bleeding.[65]
References
- ^ . Turpie AGG (March 2008). "Deep Venous Thrombosis". The Merck's Manuals Online Medical Library. http://www.merck.com/mmpe/sec07/ch081/ch081b.html?qt=dvt&alt=sh#sec07-ch081-ch081b-1775.
- ^ Firkin F, Nandurkar H (2009). "Flying and thromboembolism". Australian Prescriber 32 (6): 148–50. http://www.australianprescriber.com/magazine/32/6/148/50/.
- ^ Rosendall FR. (2005). "Venous Thrombosis: the role of genes, environment, and behavior.". Hematology Am Soc Hematol Educ Program 2005: 1–12. doi:10.1182/asheducation-2005.1.1. PMID 16304352.
- ^ Spencer FA, Lessard D, Emery C, Reed G, Goldberg RJ (2007). "Venous thromboembolism in the outpatient setting". Arch. Intern. Med. 167 (14): 1471–5. doi:10.1001/archinte.167.14.1471. PMC 2762787. PMID 17646600. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2762787.
- ^ a b Bulger CM, Jacobs C, Patel NH (June 2004). "Epidemiology of acute deep vein thrombosis". Tech Vasc Interv Radiol 7 (2): 50–4. PMID 15252760.
- ^ Tsai A, Cushman M, Rosamond W, Heckbert S, Polak J, Folsom A (2002). "Cardiovascular risk factors and venous thromboembolism incidence: the longitudinal investigation of thromboembolism etiology". Arch Intern Med 162 (10): 1182–9. doi:10.1001/archinte.162.10.1182. PMID 12020191.
- ^ Bagshaw M (2001). "Traveller's thrombosis: a review of deep vein thrombosis associated with travel. The Air Transport Medicine Committee, Aerospace Medical Association.". Aviation, space, and environmental medicine 72 (9): 848–851. PMID 11565823.
- ^ a b Philbrick JT, Shumate R, Siadaty MS, Becker DM (2007). "Air travel and venous thromboembolism: a systematic review". Journal of general internal medicine : official journal of the Society for Research and Education in Primary Care Internal Medicine 22 (1): 107–14. doi:10.1007/s11606-006-0016-0. PMC 1824715. PMID 17351849. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1824715.
- ^ Cruickshank JM, Gorlin R, Jennett B (August 1988). "Air travel and thrombotic episodes: the economy class syndrome.". Lancet 2 (8609): 497–8. PMID 2900413.
- ^ Homans J (1954). "Thrombosis of the deep leg veins due to prolonged sitting". N Engl J Med 250 (4): 148–149. doi:10.1056/NEJM195401282500404. PMID 13119864.
- ^ Symington IS, Stack BH (1977). "Pulmonary thromboembolism after travel". Br J Dis Chest 71 (2): 138–140. doi:10.1016/0007-0971(77)90097-3. PMID 861157.
- ^ Bendz B, Rostrup M, Sevre K, Andersen TO, Sandset PM (2000). "Association between acute hypobaric hypoxia and activation of coagulation in human beings". Lancet 356 (9242): 1657–8. doi:10.1016/S0140-6736(00)03165-2. PMID 11089830.
- ^ [1]
- ^ Ferrari E, Chevallier T, Chapelier A, Baudouy M (1999). "Travel as a risk factor for venous thromboembolic disease: a case-control study". Chest 115 (2): 440–4. doi:10.1378/chest.115.2.440. PMID 10027445.
- ^ a b c d Geerts WH, Bergqvist D, Pineo GF, Heit JA, Samama CM, Lassen MR, Colwell CW; American College of Chest Physicians (2008). "Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition)". Chest 133 (6 Suppl): 381S–453S. doi:10.1378/chest.08-0656. PMID 18574271.
- ^ Meyering C, Howard T (2004). "Hypercoagulability in athletes". Curr Sports Med Rep 3 (2): 77–83. PMID 14980135.
- ^ World health organization (2007). WHO Research Into Global Hazards of Travel (WRIGHT) Project : final report of phase I.
- ^ Schobersberger W, Toff WD, Eklöf B, Fraedrich G, Gunga HC, Haas S, Landgraf H, Lapostolle F, Partsch H, Perschler F, Schnapka J, Schobersberger B, Scurr JH, Watzke H; Hall consensus development group. (2008). "Traveller's thrombosis: international consensus statement". VASA 37 (4): 311–7. doi:10.1024/0301-1526.37.4.311. PMID 19003740.
- ^ Virchow R (1851). "Ueber die Erweiterung kleinerer Gefäfse". Arch Pathol Anat Physiol Klin Med 3 (3): 427–62. doi:10.1007/BF01960918.
- ^ Wells PS, Owen C, Doucette S, Fergusson D, Tran H (2006). "Does this patient have deep vein thrombosis?". JAMA 295 (2): 199–207. doi:10.1001/jama.295.2.199. PMID 16403932.
- ^ Scarvelis D, Wells P (2006). "Diagnosis and treatment of deep-vein thrombosis". CMAJ 175 (9): 1087–92. doi:10.1503/cmaj.060366. PMC 1609160. PMID 17060659. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1609160.
- ^ Neff MJ; ACEP (August 2003). "ACEP releases clinical policy on evaluation and management of pulmonary embolism". Am Fam Physician 68 (4): 759–60. PMID 12952389. http://www.aafp.org/afp/20030815/practice.html.
- ^ Wells P, Anderson D, Rodger M, Ginsberg J, Kearon C, Gent M, Turpie A, Bormanis J, Weitz J, Chamberlain M, Bowie D, Barnes D, Hirsh J (2000). "Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: increasing the models utility with the SimpliRED D-dimer". Thromb Haemost 83 (3): 416–20. PMID 10744147.
- ^ Wells PS, Anderson DR, Rodger M, et al. (2003). "Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis". N. Engl. J. Med. 349 (13): 1227–35. doi:10.1056/NEJMoa023153. PMID 14507948.
- ^ Bates SM, Kearon C, Crowther M, et al. (2003). "A diagnostic strategy involving a quantitative latex D-dimer assay reliably excludes deep venous thrombosis". Ann. Intern. Med. 138 (10): 787–94. PMID 12755550.
- ^ Elizabeth D Agabegi; Agabegi, Steven S. (2008). Step-Up to Medicine (Step-Up Series). Hagerstwon, MD: Lippincott Williams & Wilkins. ISBN 0-7817-7153-6.
- ^ Qaseem, Amir; Roger Chou, Linda L. Humphrey, Melissa Starkey, Paul Shekelle (2011-11-01). "Venous Thromboembolism Prophylaxis in Hospitalized Patients: A Clinical Practice Guideline From the American College of Physicians". Annals of Internal Medicine 155 (9): 625–632. doi:10.1059/0003-4819-155-9-201111010-00011. http://www.annals.org/content/155/9/625.abstract. Retrieved 2011-11-01.
- ^ Lederle, Frank A.; Dylan Zylla, Roderick MacDonald, Timothy J. Wilt (2011-11-01). "Venous Thromboembolism Prophylaxis in Hospitalized Medical Patients and Those With Stroke: A Background Review for an American College of Physicians Clinical Practice Guideline". Annals of Internal Medicine 155 (9): 602–615. doi:10.1059/0003-4819-155-9-201111010-00008. http://www.annals.org/content/155/9/602.abstract. Retrieved 2011-11-01.
- ^ King CS, Holley AB, Jackson JL, Shorr AF, Moores LK (2007). "Twice vs three times daily heparin dosing for thromboembolism prophylaxis in the general medical population: A metaanalysis". Chest 131 (2): 507–16. doi:10.1378/chest.06-1861. PMID 17296655.
- ^ Wein L, Wein S, Haas SJ, Shaw J, Krum H (2007). "Pharmacological Venous Thromboembolism Prophylaxis in Hospitalized Medical Patients: A Meta-analysis of Randomized Controlled Trials". Archives of Internal Medicine 167 (14): 1476–1486. doi:10.1001/archinte.167.14.1476. PMID 17646601.
- ^ a b Lederle FA, Sacks JM, Fiore L, et al. (January 2006). "The prophylaxis of medical patients for thromboembolism pilot study". Am. J. Med. 119 (1): 54–9. doi:10.1016/j.amjmed.2005.03.049. PMID 16431185.
- ^ Dentali F, Douketis JD, Gianni M, Lim W, Crowther MA (February 2007). "Meta-analysis: anticoagulant prophylaxis to prevent symptomatic venous thromboembolism in hospitalized medical patients". Ann. Intern. Med. 146 (4): 278–88. PMID 17310052. http://annals.org/cgi/content/full/146/4/278.
- ^ Gärdlund B; Gårdlund, B. (May 1996). "Randomised, controlled trial of low-dose heparin for prevention of fatal pulmonary embolism in patients with infectious diseases. The Heparin Prophylaxis Study Group". Lancet 347 (9012): 1357–61. doi:10.1016/S0140-6736(96)91009-0. PMID 8637340.
- ^ a b "Effectiveness of thigh-length graduated compression stockings to reduce the risk of deep vein thrombosis after stroke (CLOTS trial 1): a multicentre, randomised controlled trial". The Lancet 373: 1958–1965. 2009. doi:10.1016/S0140-6736(09)60941-7.
- ^ a b The CLOTS (Clots in Legs Or sTockings after Stroke) Trial Collaboration (2010). "Thigh-Length Versus Below-Knee Stockings for Deep Venous Thrombosis Prophylaxis After Stroke: A Randomized Trial". Annals of internal medicine 153 (9): 553–562. doi:10.1059/0003-4819-153-9-201011020-00280. PMID 20855784.
- ^ Kearon C, O'Donnell M (November 2010). "Should patients with stroke wear compression stockings to prevent venous thromboembolism?". Ann Intern Med 153 (9): 610–1. doi:10.1059/0003-4819-153-9-201011020-00285. PMID 20855785.
- ^ Perry, Anne Griffen (2010). Clinical Nursing Skills and Techniques. 1180 Westline Industrial Drive St. Louis, Missouri 63146: Mosby, Inc.. pp. 243. ISBN 978-0-323-05289-4.
- ^ Tveit DP, Hypolite IO, Hshieh P, et al. (2002). "Chronic dialysis patients have high risk for pulmonary embolism". Am. J. Kidney Dis. 39 (5): 1011–7. doi:10.1053/ajkd.2002.32774. PMID 11979344.
- ^ a b Page 264 in: Gresele, Paolo (2008). Platelets in hematologic and cardiovascular disorders: a clinical handbook. Cambridge UK: Cambridge University Press. ISBN 0-521-88115-3.
- ^ Sathienkijkanchai A, Wasant P. (2005). "Fetal warfarin syndrome". J Med Assoc Thai 88 (Suppl 8): S246–50. PMID 16856447.
- ^ Schaefer C, Hannemann D, Meister R, Eléfant E, Paulus W, Vial T, Reuvers M, Robert-Gnansia E, Arnon J, De Santis M, Clementi M, Rodriguez-Pinilla E, Dolivo A, Merlob P. (2006). "Vitamin K antagonists and pregnancy outcome. A multi-centre prospective study". Thromb Haemost 95 (6): 949–57. doi:10.1160/TH06-02-0108. PMID 16732373.
- ^ Clarke MJ, Hopewell S, Juszczak E, Eisinga A, Kjeldstrøm M (2006). "Compression stockings for preventing deep vein thrombosis in airline passengers". Cochrane Database Syst Rev (2): CD004002. doi:10.1002/14651858.CD004002.pub2. PMID 16625594.
- ^ Hirsh J, O'Donnell MJ (2001). "Venous thromboembolism after long flights: are airlines to blame?". Lancet 357 (9267): 1461–2. doi:10.1016/S0140-6736(00)04669-9. PMID 11377591.
- ^ Scurr JH, Machin SJ, Bailey-King S, Mackie IJ, McDonald S, Smith PD (2001). "Frequency and prevention of symptomless deep-vein thrombosis in long-haul flights: a randomised trial". Lancet 357 (9267): 1485–9. doi:10.1016/S0140-6736(00)04645-6. PMID 11377600.
- ^ Schreijer, Anja J. M.; Suzanne C. Cannegieter, Carine J. M. Doggen, Frits R. Rosendaal (Nov 25 2008). "The effect of flight-related behaviour on the risk of venous thrombosis after air travel". British Journal of Haematology 144 (3): 425–429. doi:10.1111/j.1365-2141.2008.07489.x. PMID 19036084.
- ^ a b Snow V, Qaseem A, Barry P, et al. (2007). "Management of venous thromboembolism: a clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians". Ann. Intern. Med. 146 (3): 204–10. PMID 17261857. http://www.annals.org/cgi/content/full/146/3/204.
- ^ Hutten BA, Prins MH (2006). Prins, Martin H. ed. "Duration of treatment with vitamin K antagonists in symptomatic venous thromboembolism". Cochrane Database Syst Rev (1): CD001367. doi:10.1002/14651858.CD001367.pub2. PMID 16437432.
- ^ Kakkos SK, Caprini JA, Geroulakos G, Nicolaides AN, Stansby GP, Reddy DJ (2008). Kakkos, Stavros K. ed. "Combined intermittent pneumatic leg compression and pharmacological prophylaxis for prevention of venous thromboembolism in high-risk patients". Cochrane Database Syst Rev (4): CD005258. doi:10.1002/14651858.CD005258.pub2. PMID 18843686. http://onlinelibrary.wiley.com/o/cochrane/clsysrev/articles/CD005258/frame.html.
- ^ Palareti G, Cosmi B, Legnani C, et al. (2006). "D-dimer testing to determine the duration of anticoagulation therapy". N. Engl. J. Med. 355 (17): 1780–9. doi:10.1056/NEJMoa054444. PMID 17065639.
- ^ Cundiff DK, Manyemba J, Pezzullo JC (2006). Cundiff, David K. ed. "Anticoagulants versus non-steroidal anti-inflammatories or placebo for treatment of venous thromboembolism". Cochrane Database Syst Rev (1): CD003746. doi:10.1002/14651858.CD003746.pub2. PMID 16437461.
- ^ Harry R. Büller, Giancarlo Agnelli, Russel D. Hull, Thomas M. Hyers, Martin H. Prins, and Gary E. Raskob (September 2004). "Antithrombotic Therapy for Venous Thromboembolic Disease: The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy". Chest 126 (3): 401S–428S. doi:10.1378/chest.126.3_suppl.401S. PMID 15383479. http://chestjournal.chestpubs.org/content/126/3_suppl/401S.full. Retrieved 12 August 2010.
- ^ Watson L, Armon M (2004). Watson, Lorna. ed. "Thrombolysis for acute deep vein thrombosis". Cochrane Database Syst Rev (4): CD002783. doi:10.1002/14651858.CD002783.pub2. PMID 15495034.
- ^ Prandoni P, Lensing AW, Prins MH, et al. (2004). "Below-knee elastic compression stockings to prevent the post-thrombotic syndrome: a randomized, controlled trial". Ann. Intern. Med. 141 (4): 249–56. PMID 15313740.
- ^ Musani MH, Matta F, Yaekoub AY, Liang J, Hull RD, Stein PD (August 2010). "Venous compression for prevention of postthrombotic syndrome: a meta-analysis". Am. J. Med. 123 (8): 735–40. doi:10.1016/j.amjmed.2010.01.027. PMID 20670728.
- ^ Kolbach D, Sandbrink M, Hamulyak K, Neumann H, Prins M (2003). Kolbach, Dinanda N. ed. "Non-pharmaceutical measures for prevention of post-thrombotic syndrome". Cochrane Database Syst Rev (1): CD004174. doi:10.1002/14651858.CD004174.pub2. PMID 14974060.
- ^ Kakkos S, Daskalopoulou S, Daskalopoulos M, Nicolaides A, Geroulakos G (2006). "Review on the value of graduated elastic compression stockings after deep vein thrombosis". Thromb Haemost 96 (4): 441–5. PMID 17003920.
- ^ http://www2.cochrane.org/reviews/en/ab001899.html
- ^ Decousus H, Leizorovicz A, Parent F, Page Y, Tardy B, Girard P, Laporte S, Faivre R, Charbonnier B, Barral F, Huet Y, Simonneau G (1998). "A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. Prévention du Risque d'Embolie Pulmonaire par Interruption Cave Study Group". N Engl J Med 338 (7): 409–15. doi:10.1056/NEJM199802123380701. PMID 9459643.
- ^ Prepic Study, Group (2005). "Eight-year follow-up of patients with permanent vena cava filters in the prevention of pulmonary embolism: the PREPIC (Prevention du Risque d'Embolie Pulmonaire par Interruption Cave) randomized study". Circulation 112 (3): 416–22. doi:10.1161/CIRCULATIONAHA.104.512834. PMID 16009794.
- ^ Young T, Aukes J, Hughes R, Tang H (2007). Young, Tim. ed. "Vena caval filters for the prevention of pulmonary embolism". Cochrane Database Syst Rev (3): CD006212. doi:10.1002/14651858.CD006212.pub2. PMID 17636834.
- ^ Othieno R, Abu Affan M, Okpo E (2007). Othieno, Richard. ed. "Home versus in-patient treatment for deep vein thrombosis". Cochrane Database Syst Rev (3): CD003076. doi:10.1002/14651858.CD003076.pub2. PMID 17636714.
- ^ Trujillo-Santos J, Herrera S, Page MA, et al. (2006). "Predicting adverse outcome in outpatients with acute deep vein thrombosis. findings from the RIETE Registry". J. Vasc. Surg. 44 (4): 789–93. doi:10.1016/j.jvs.2006.06.032. PMID 16926081.
- ^ The post-thrombotic syndrome: current knowledge, controversies, and directions for future research
- ^ "The Surgeon General's Call to Action to Prevent Deep Vein Thrombosis and Pulmonary Embolism 2008" (PDF). http://www.surgeongeneral.gov/topics/deepvein/calltoaction/call-to-action-on-dvt-2008.pdf. Retrieved 2008-10-13.
- ^ Venös tromboembolism (VTE) — Guidelines for treatment in C counties. Bengt Wahlström, Emergency department, Uppsala Academic Hospital. January 2008
External links
- North American Thrombosis Forum
- "Antithrombotic and Thrombolytic Therapy, 8th Ed: ACCP Guidelines". Chest (American College of Chest Physicians) 133 (6 suppl b–C). June 2008. http://chestjournal.chestpubs.org/content/133/6_suppl.
- International Society on Thrombosis and Haemostasis
- DVT patient information
Categories:- Coagulopathies
- Diseases of veins, lymphatic vessels and lymph nodes

Wikimedia Foundation. 2010.