- Myocardial infarction complications
-
Main article: Myocardial infarction
Myocardial infarction complications may occur immediately following a heart attack (in the acute phase), or may need time to develop (a chronic problem). After an infarction, an obvious complication is a second infarction, which may occur in the domain of another atherosclerotic coronary artery, or in the same zone if there are any live cells left in the infarct.
Contents
Congestive heart failure
Main article: Congestive heart failureA myocardial infarction may compromise the function of the heart as a pump for the circulation, a state called heart failure. There are different types of heart failure; left- or right-sided (or bilateral) heart failure may occur depending on the affected part of the heart, and it is a low-output type of failure. If one of the heart valves is affected, this may cause dysfunction, such as mitral regurgitation in the case of left-sided coronary occlusion that disrupts the blood supply of the papillary muscles. The incidence of heart failure is particularly high in patients with diabetes and requires special management strategies.[1]
Myocardial rupture
Main article: Myocardial ruptureMyocardial rupture is most common three to five days after myocardial infarction, commonly of small degree, but may occur one day to three weeks later. In the modern era of early revascularization and intensive pharmacotherapy as treatment for MI, the incidence of myocardial rupture is about 1% of all MIs.[2] This may occur in the free walls of the ventricles, the septum between them, the papillary muscles, or less commonly the atria. Rupture occurs because of increased pressure against the weakened walls of the heart chambers due to heart muscle that cannot pump blood out effectively. The weakness may also lead to ventricular aneurysm, a localized dilation or ballooning of the heart chamber.
Risk factors for myocardial rupture include completion of infarction (no revascularization performed), female sex, advanced age, and a lack of a previous history of myocardial infarction.[2] In addition, the risk of rupture is higher in individuals who are revascularized with a thrombolytic agent than with PCI.[3][4] The shear stress between the infarcted segment and the surrounding normal myocardium (which may be hypercontractile in the post-infarction period) makes it a nidus for rupture.[5]
Rupture is usually a catastrophic event that may result a life-threatening process known as cardiac tamponade, in which blood accumulates within the pericardium or heart sac, and compresses the heart to the point where it cannot pump effectively. Rupture of the intraventricular septum (the muscle separating the left and right ventricles) causes a ventricular septal defect with shunting of blood through the defect from the left side of the heart to the right side of the heart, which can lead to right ventricular failure as well as pulmonary overcirculation. Rupture of the papillary muscle may also lead to acute mitral regurgitation and subsequent pulmonary edema and possibly even cardiogenic shock.
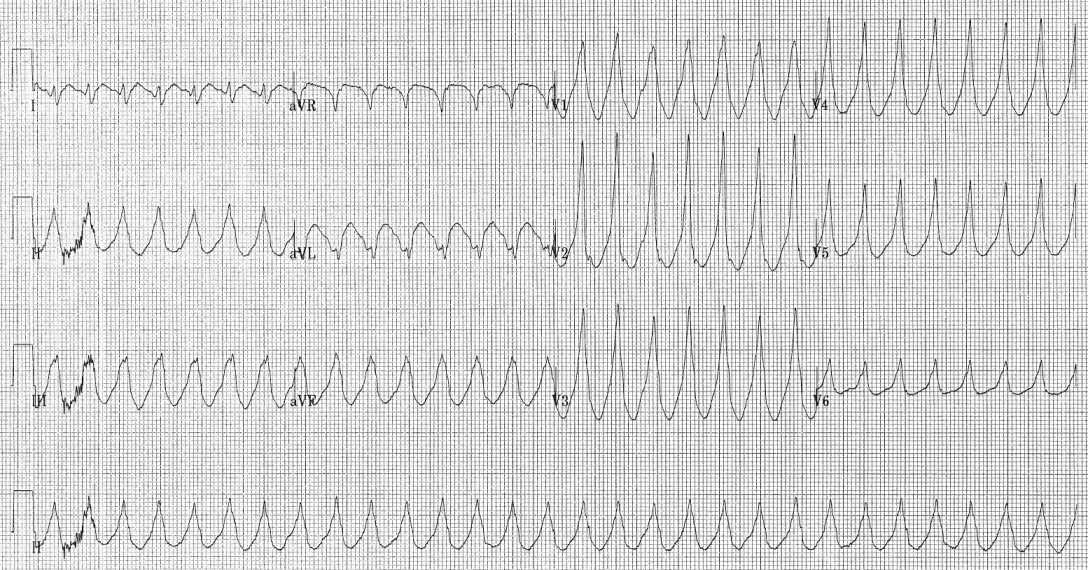
Arrhythmia
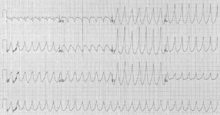
Since the electrical characteristics of the infarcted tissue change (see pathophysiology section), arrhythmias are a frequent complication.[6] The re-entry phenomenon may cause rapid heart rates (ventricular tachycardia and even ventricular fibrillation), and ischemia in the electrical conduction system of the heart may cause a complete heart block (when the impulse from the sinoatrial node, the normal cardiac pacemaker, does not reach the heart chambers).[7][8]
Pericarditis
Main article: PericarditisAs a reaction to the damage of the heart muscle, inflammatory cells are attracted. The inflammation may reach out and affect the heart sac. This is called pericarditis. In Dressler's syndrome, this occurs several weeks after the initial event.
Cardiogenic shock
A complication that may occur in the acute setting soon after a myocardial infarction or in the weeks following it is cardiogenic shock. Cardiogenic shock is defined as a hemodynamic state in which the heart cannot produce enough of a cardiac output to supply an adequate amount of oxygenated blood to the tissues of the body.
While the data on performing interventions on individuals with cardiogenic shock is sparse, trial data suggests a long-term mortality benefit in undergoing revascularization if the individual is less than 75 years old and if the onset of the acute myocardial infarction is less than 36 hours and the onset of cardiogenic shock is less than 18 hours.[9] If the patient with cardiogenic shock is not going to be revascularized, aggressive hemodynamic support is warranted, with insertion of an intra-aortic balloon pump if not contraindicated.[9] If diagnostic coronary angiography does not reveal a culprit blockage that is the cause of the cardiogenic shock, the prognosis is poor.[9]
References
- ^ Canto JG, Shlipak MG, Rogers WJ, Malmgren JA, Frederick PD, Lambrew CT, Ornato JP, Barron HV, Kiefe CI. (2000). "Prevalence, clinical characteristics, and mortality among patients with myocardial infarction presenting without chest pain". JAMA 283 (24): 3223–9. doi:10.1001/jama.283.24.3223. PMID 10866870.
- ^ a b Yip HK, Wu CJ, Chang HW, Wang CP, Cheng CI, Chua S, Chen MC. (2003). "Cardiac rupture complicating acute myocardial infarction in the direct percutaneous coronary intervention reperfusion era" (PDF). Chest 124 (2): 565–71. doi:10.1378/chest.124.2.565. PMID 12907544. http://www.chestjournal.org/cgi/reprint/124/2/565.pdf.
- ^ Becker RC, Gore JM, Lambrew C, Weaver WD, Rubison RM, French WJ, Tiefenbrunn AJ, Bowlby LJ, Rogers WJ. (1996). "A composite view of cardiac rupture in the United States National Registry of Myocardial Infarction". J Am Coll Cardiol 27 (6): 1321–6. doi:10.1016/0735-1097(96)00008-3. PMID 8626938.
- ^ Moreno R, Lopez-Sendon J, Garcia E, Perez de Isla L, Lopez de Sa E, Ortega A, Moreno M, Rubio R, Soriano J, Abeytua M, Garcia-Fernandez MA. (2002). "Primary angioplasty reduces the risk of left ventricular free wall rupture compared with thrombolysis in patients with acute myocardial infarction". J Am Coll Cardiol 39 (4): 598–603. doi:10.1016/S0735-1097(01)01796-X. PMID 11849857.
- ^ Shin P, Sakurai M, Minamino T, Onishi S, Kitamura H. (1983). "Postinfarction cardiac rupture. A pathogenetic consideration in eight cases". Acta Pathol Jpn 33 (5): 881–93. PMID 6650169.
- ^ Podrid, Philip J.; Peter R. Kowey (2001). Cardiac Arrhythmia: Mechanisms, Diagnosis, and Management. Lippincott Williams & Wilkins. ISBN 0781724864.
- ^ Sung, Ruey J.; Michael R. Lauer (2000). Fundamental Approaches to the Management of Cardiac Arrhythmias. Springer. ISBN 0792365593.
- ^ Josephson, Mark E. (2002). Clinical Cardiac Electrophysiology: Techniques and Interpretations. Lippincott Williams & Wilkins. ISBN 0683306936.
- ^ a b c Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD, Buller CE, Jacobs AK, Slater JN, Col J, McKinlay SM, LeJemtel TH. (1999). "Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock". N Engl J Med 341 (9): 625–34. doi:10.1056/NEJM199908263410901. PMID 10460813.
Categories:- Aging-associated diseases
- Causes of death
- Ischemic heart diseases
- Medical emergencies
Wikimedia Foundation. 2010.