- Coronary artery disease
-
Coronary artery disease Classification and external resources 
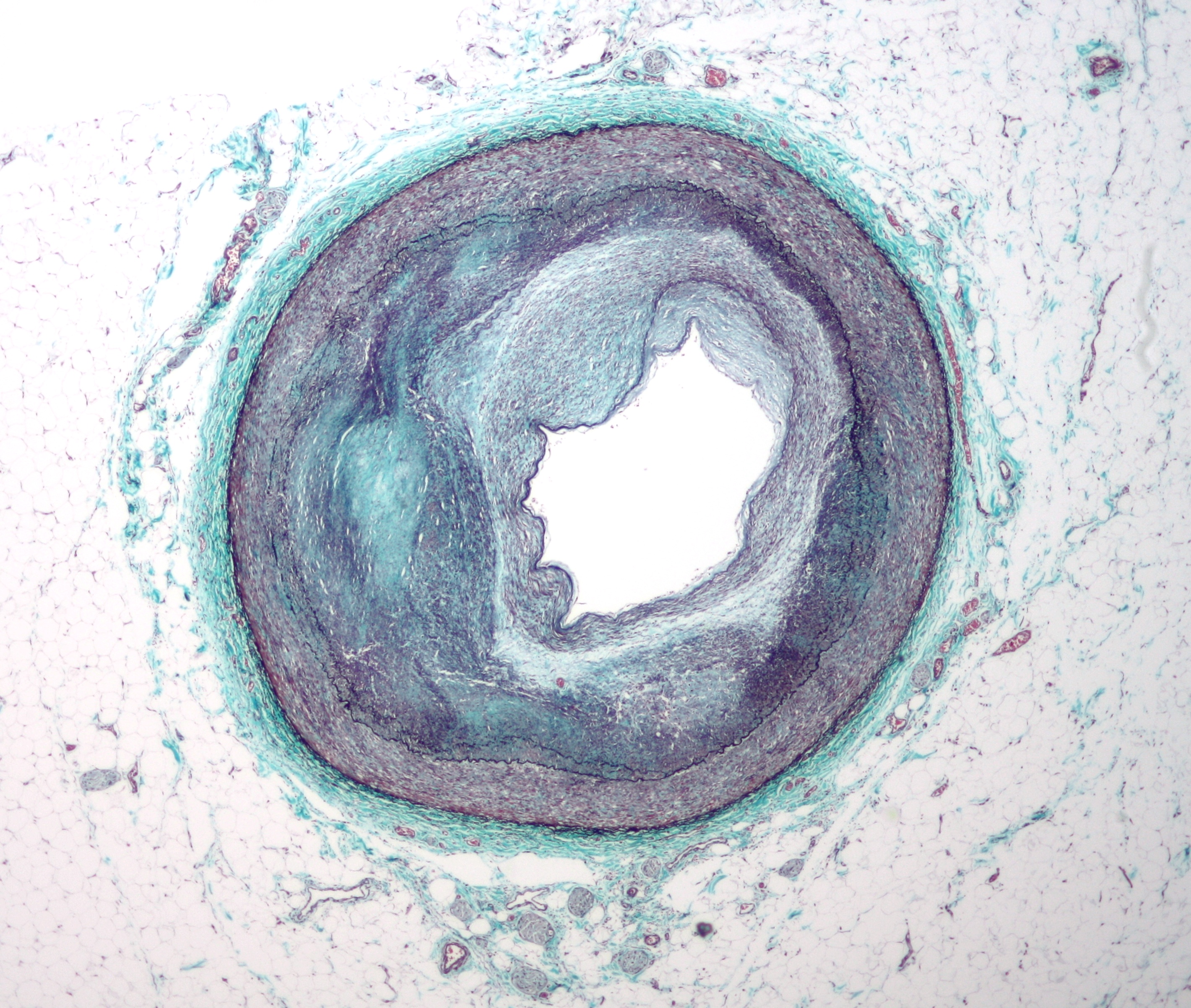
Micrograph of a coronary artery with the most common form of coronary artery disease (atherosclerosis) and marked luminal narrowing. Masson's trichrome.ICD-10 I20-I25 ICD-9 410-414, 429.2 eMedicine radio/192 MeSH D003324 Coronary artery disease (CAD; also atherosclerotic heart disease) is the end result of the accumulation of atheromatous plaques within the walls of the coronary arteries[1] that supply the myocardium (the muscle of the heart) with oxygen and nutrients. It is sometimes also called coronary heart disease (CHD). Although CAD is the most common cause of CHD, it is not the only one.
CAD is the leading cause of death worldwide.[2] While the symptoms and signs of coronary artery disease are noted in the advanced state of disease, most individuals with coronary artery disease show no evidence of disease for decades as the disease progresses before the first onset of symptoms, often a "sudden" heart attack, finally arises. After decades of progression, some of these atheromatous plaques may rupture and (along with the activation of the blood clotting system) start limiting blood flow to the heart muscle. The disease is the most common cause of sudden death,[3] and is also the most common reason for death of men and women over 20 years of age.[4] According to present trends in the United States, half of healthy 40-year-old males will develop CAD in the future, and one in three healthy 40-year-old women.[5] According to the Guinness Book of Records, Northern Ireland is the country with the most occurrences of CAD. By contrast, the Maasai of Africa have almost no heart disease.
As the degree of coronary artery disease progresses, there may be near-complete obstruction of the lumen of the coronary artery, severely restricting the flow of oxygen-carrying blood to the myocardium. Individuals with this degree of coronary artery disease typically have suffered from one or more myocardial infarctions (heart attacks), and may have signs and symptoms of chronic coronary ischemia, including symptoms of angina at rest and flash pulmonary edema.
A distinction should be made between myocardial ischemia and myocardial infarction. Ischemia means that the amount of blood supplied to the tissue is inadequate to supply the needs of the tissue. When the myocardium becomes ischemic, it does not function optimally. When large areas of the myocardium becomes ischemic, there can be impairment in the relaxation and contraction of the myocardium. If the blood flow to the tissue is improved, myocardial ischemia can be reversed. Infarction means that the tissue has undergone irreversible death due to lack of sufficient oxygen-rich blood.
An individual may develop a rupture of an atheromatous plaque at any stage of the spectrum of coronary artery disease. The acute rupture of a plaque may lead to an acute myocardial infarction (heart attack).
Contents
Pathophysiology
Limitation of blood flow to the heart causes ischemia (cell starvation secondary to a lack of oxygen) of the myocardial cells. Myocardial cells may die from lack of oxygen and this is called a myocardial infarction (commonly called a heart attack). It leads to heart muscle damage, heart muscle death and later myocardial scarring without heart muscle regrowth. Chronic high-grade stenosis of the coronary arteries can induce transient ischemia which leads to the induction of a ventricular arrhythmia, which may terminate into ventricular fibrillation leading to death.
CAD is associated with smoking, diabetes, and hypertension. A family history of early CAD is one of the less important predictors of CAD. Most of the familial association of coronary artery disease are related to common dietary habits. Screening for CAD includes evaluating high-density and low-density lipoprotein (cholesterol) levels and triglyceride levels. Despite much press, most of the alternative risk factors including homocysteine, C-reactive protein (CRP), Lipoprotein (a), coronary calcium and more sophisticated lipid analysis have added little if any additional value to the conventional risk factors of smoking, diabetes and hypertension.
Angina
Angina (chest pain) that occurs regularly with activity, after heavy meals, or at other predictable times is termed stable angina and is associated with high grade narrowings of the heart arteries. The symptoms of angina are often treated with betablocker therapy such as metoprolol or atenolol. Nitrate preparations such as nitroglycerin, which come in short-acting and long-acting forms are also effective in relieving symptoms but are not known to reduce the chances of future heart attacks. Many other more effective treatments, especially of the underlying atheromatous disease, have been developed.
Angina that changes in intensity, character or frequency is termed unstable. Unstable angina may precede myocardial infarction, and requires urgent medical attention. It may be treated with oxygen, intravenous nitroglycerin, and aspirin. Interventional procedures such as angioplasty may be done.
Characteristics of coronary artery disease
Special Pathophysiology
Typically, coronary artery disease occurs when part of the smooth, elastic lining inside a coronary artery (the arteries that supply blood to the heart muscle) develops atherosclerosis. With atherosclerosis, the artery's lining becomes hardened, stiffened, and swollen with all sorts of "grunge" - including calcium deposits, fatty deposits, and abnormal inflammatory cells - to form a plaque. Deposits of calcium phosphates (hydroxyapatites) in the muscular layer of the blood vessels appear to play not only a significant role in stiffening arteries but also for the induction of an early phase of coronary arteriosclerosis. This can be seen in a so-called metatstatic mechanism of calcification as it occurs in chronic kidney disease and haemodialysis (Rainer Liedtke 2008). Although these patients suffer from a kidney dysfunction, almost fifty percent of them die due to coronary artery disease. Plaques can be thought of as large "pimples" that protrude into the channel of an artery, causing a partial obstruction to blood flow. Patients with coronary artery disease might have just one or two plaques, or might have dozens distributed throughout their coronary arteries. However, there is a term in medicine called “Cardiac Syndrome X”, which describes chest pain (Angina pectoris) and chest discomfort in people who do not show signs of blockages in the larger coronary arteries of their hearts when an angiogram (coronary angiogram) is being performed.[6]
No one knows exactly what causes “Cardiac Syndrome X” and it is unlikely to have a single cause. Today, we speculate that the major contributing factor to “Cardiac Syndrome X” is “microvascular dysfunction”.[who?] The term “microvascular” refers to very small blood vessels and, in this case, very small arteries (arterioles, capillaries) of the heart. Studies have also shown that people with “Cardiac Syndrome X” have enhanced pain perception, meaning they feel chest pain more intensely than the average person.
The large majority of women have the garden variety of coronary artery disease. Rarely, women with “Cardiac Syndrome X” have typical anginal syndromes that are not associated with the presence of atherosclerotic plaques; that is, the localized blockages are absent. Scientists speculate that the blood vessels in these women are diffuse abnormal. Some have falsely claim that the entire lining of the artery becomes thickened throughout, making the plaques flush with the wall of the artery without any scientific proof. On cardiac catheterization their coronary arteries appear smooth-walled and normal, though they may look "small" in diameter. By the way: in general, female coronary arteries (like all arteries) are somewhat smaller than in males.
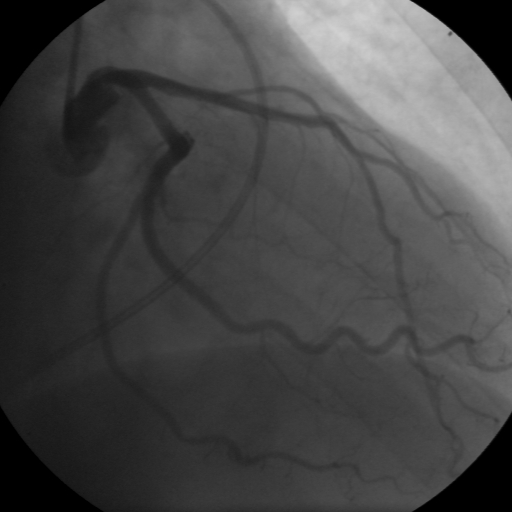
 Coronary angiogram of a man
Coronary angiogram of a man
 Coronary angiogram of a woman
Coronary angiogram of a woman“Cardiac Syndrome X” have never been shown to cause acute heart attacks (myocardial infarction) despite much speculation. The prognosis with syndrome-X coronary artery disease is also known to be better than with typical coronary artery disease, but this is not a benign condition since it can be quite disabling. It is not completely clear why women are more likely than men to suffer from "Syndrome X"; however, hormones and other risk factors unique to women may play a role.[7] Women’s blood vessels are exposed to changing levels of oestrogen throughout their lives, first during regular menstrual cycles and later during and after menopause as oestrogen levels decline with age. Oestrogen affects how blood vessels narrow and widen and how they respond to injury, so changes in oestrogen levels mean changes in the reactivity of the blood vessels. Women’s vessels may be “programmed” for more changes than men’s vessels, which could increase the risk of having problems in the lining of the arteries (endothelial cells) and the smooth muscle cells in the walls of the arteries. The endothelial dysfunction is likely to be multifactorial in these patients and it is conceivable that risk factors such as hypertension, hypercholesterolemia, diabetes mellitus and smoking can contribute to its development. Most patients with Syndrome X are postmenopausal women and oestrogen deficiency has been therefore proposed as a pathogenic factor in female patients. In addition to changing hormone levels, there are several other risk conditions for blood vessel problems that are unique to women, such as preeclampsia (a problem associated with high blood pressure during pregnancy) and delivering a low-birth weight baby. Of course, despite these issues women, the female gender as a whole is protective against coronary artery disease.
Symptoms
Cardiac Syndrome X often is a diagnosis of exclusion where the presence of typical chest pains is not accompanied by coronary artery narrowings on angiography. In considering Syndrome-X, it is important to understand that about 80% of chest pains have nothing to do with the heart. Therefore, the characteristics of typical chest pains must be carefully documented to avoid unnecessary labelling patients with heart disease:
- Chest pain or Angina pectoris with physical stress; the pain may spread to the left arm or the neck, back, throat, or jaw. There might be present a numbness (paresthesia) or a loss of feeling in the arms, shoulders, or wrists
- Coronary angiography demonstrates “normal” coronary arteries, i.e. no blockages or stenoses can be detected in the larger epicardial vessels
- No inducible coronary artery spasm present during cardiac catheterization
- Characteristic ischemic ECG changes during exercise testing
- ST segment depression and angina in the presence of left ventricular wall perfusion abnormalities during thallium or other stress perfusion test
- Consistent response to sublingual nitrates.
- Postmenopausal or menopausal status
The diagnosis of “Cardiac Syndrome X” - the rare coronary artery disease that is more common in women, as mentioned, an “exclusion” diagnosis. Therefore, usually the same tests are used as in any patient with the suspicion of coronary artery disease:
- Baseline electrocardiography (ECG)
- Exercise ECG – Stress test
- Exercise radioisotope test (nuclear stress test, myocardial scintigraphy)
- Echocardiography (including stress echocardiography)
- Coronary angiography
- Intravascular ultrasound
- Magnetic resonance imaging (MRI)
Therapy
A variety of drugs are used in the attempt to treat the Syndrome-X coronary artery disease: nitrates, calcium channel antagonists, ACE-inhibitors, statins, imipramine (for analgesia), aminophylline, hormone replacement therapy (oestrogen), even electrical spinal cord stimulation are tried to overcome the symptomatology -all with mixed results. Quite often the quality of life for these women remains poor.
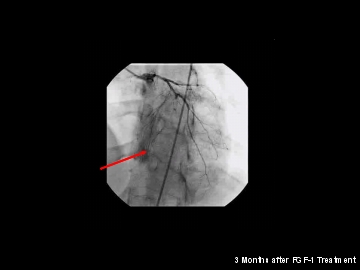
While not enough is known about Syndrome-X coronary artery disease to list specific prevention techniques, adopting heart-healthy habits can be a good start.[citation needed] These include monitoring cholesterol and blood pressure levels[citation needed], maintaining a low-fat diet[citation needed], exercising regularly[citation needed], quitting smoking, avoiding recreational drugs[citation needed], and moderating alcohol intake. However, there might be a new option for women suffering from “Cardiac Syndrome X”: Protein based Angiogenesis.[8] This new protein-based angiogenic therapy - using fibroblast growth factor 1 (FGF-1) - might be used as sole therapy as well as adjunct to bypass surgery – thus overcoming the limitations of conventional bypass surgery.
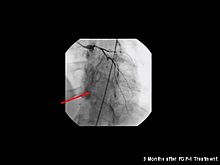 Neo-angiogenesis in a woman's heart after FGF-1 treatment
Neo-angiogenesis in a woman's heart after FGF-1 treatmentBeyond drug therapy, interventional procedures, and coronary artery bypass grafting, angiogenesis now offers a new, specific and – so far as we know from three human clinical trials – effective treatment targeted for women’s coronary artery disease.[9]
Risk factors
The following are confirmed independent risk factors for the development of CAD:
- Hypercholesterolemia (specifically, serum LDL concentrations)[citation needed]
- Smoking[citation needed]
- Hypertension (high systolic pressure seems to be most significant in this regard)[citation needed]
- Hyperglycemia (due to diabetes mellitus or otherwise)[citation needed]
- Type A Behavioural Patterns, TABP. Added in 1981 as an independent risk factor after a majority of research into the field discovered that TABP's were twice as likely to exhibit CAD as any other personality type.[citation needed]
- Hemostatic Factors:[10] High levels of fibrinogen and coagulation factor VII are associated with an increased risk of CAD. Factor VII levels are higher in individuals with a high intake of dietary fat[citation needed]. Decreased fibrinolytic activity has been reported in patients with coronary atherosclerosis.
- Hereditary differences/genetic polymorphisms in such diverse aspects as lipoprotein structure and that of their associated receptors, enzymes of lipoprotein metabolism such as cholesteryl ester transfer protein (CETP) and hepatic lipase (HL),[11] homocysteine processing/metabolism, etc.[citation needed]
- High levels of Lipoprotein(a),[12][13][14] a compound formed when LDL cholesterol combines with a substance known as Apoliprotein (a).
Significant, but indirect risk factors include:
- Lack of exercise
- Consumption of alcohol
- Stress
- Diet rich in saturated fats[citation needed]
- Diet low in antioxidants
- Obesity
- Men over 60; Women over 65[15]
- A recent study done in India (puducherry)shows its association with hemoglobin [16]
Risk factors can be classified as- Fixed: age, sex, family history
- Modifiable: smoking, hypertension, diabetes mellitus, obesity, etc.
There are various risk assessment systems for determining the risk of coronary artery disease, with various emphasis on different variables above. A notable example is Framingham Score, used in the Framingham Heart Study. It is mainly based on age, gender, diabetes, total cholesterol, HDL cholesterol, tobacco smoking and systolic blood pressure.[17]
Prevention
Coronary artery disease is the most common form of heart disease in the Western world. Prevention centers on the modifiable risk factors, which include decreasing cholesterol levels, addressing obesity and hypertension, avoiding a sedentary lifestyle, making healthy dietary choices, and stopping smoking. There is some evidence that lowering homocysteine levels may contribute to more heart attacks (NORVIT trial). In diabetes mellitus, there is little evidence that very tight blood sugar control actually improves cardiac risk although improved sugar control appears to decrease other undesirable problems like kidney failure and blindness. Some recommend a diet rich in omega-3 fatty acids and vitamin C. The World Health Organization (WHO) recommends "low to moderate alcohol intake" to reduce risk of coronary artery disease although this remains without scientific cause and effect proof.[18]
An increasingly growing number of other physiological markers and homeostatic mechanisms are currently under scientific investigation. Patients with CAD and those trying to prevent CAD are advised to avoid fats that are readily oxidized (e.g., trans-fats), limit carbohydrates and processed sugars to reduce production of Low density lipoproteins (LDLs), triacylglycerol and apolipoprotein-B. [19] [20] [21] [22] [23] It is also important to keep blood pressure normal, exercise and stop smoking. These measures reduce the development of heart attacks. Recent studies have shown that dramatic reduction in LDL levels can cause regression of coronary artery disease in as many as 2/3 of patients after just one year of sustained treatment.
Menaquinone (Vitamin K2), but not phylloquinone (Vitamin K1), intake is associated with reduced risk of CAD mortality, all-cause mortality and severe aortic calcification.[24][25][26]
CAD has always been a tough disease to diagnose without the use of invasive or stressful activities. The development of the Multifunction Cardiogram (MCG) has changed the way CAD is diagnosed. The MCG consists of a 2 lead resting EKG signal is transformed into a mathematical model and compared against tens of thousands of clinical trials to diagnose a patient with an objective severity score, as well as secondary and tertiary results about the patients condition. The results from MCG tests have been validated in 8 clinical trials which resulted in a database of over 50,000 patients where the system has demonstrated accuracy comparable to coronary angiography (90% overall sensitivity, 85% specificity). This level of accuracy comes from the application of advanced techniques in signal processing and systems analysis combined with a large scale clinical database which allows MCG to provide quantitative, evidence-based results to assist physicians in reaching a diagnosis. The MCG has also been awarded a Category III CPT code by the American Medical Association in the July 2009 CPT update.
Exercise
Separate to the question of the benefits of exercise; it is unclear whether doctors should spend time counseling patients to exercise. The U.S. Preventive Services Task Force (USPSTF), based on a systematic review of randomized controlled trials, found 'insufficient evidence' to recommend that doctors counsel patients on exercise, but "it did not review the evidence for the effectiveness of physical activity to reduce chronic disease, morbidity and mortality", it only examined the effectiveness of the counseling itself.[27] However, the American Heart Association, based on a non-systematic review, recommends that doctors counsel patients on exercise.[28]
Preventive diets
It has been suggested that coronary artery disease is partially reversible using an intense dietary regimen coupled with regular cardio exercise.[29]
- Vegetarian diet: Vegetarians have been shown to have a 24% reduced risk of dying of heart disease.[30]
- Cretan Mediterranean diet: The Seven Countries Study found that Cretan men had exceptionally low death rates from heart disease, despite moderate to high intake of fat. The Cretan diet is similar to other traditional Mediterranean diets: consisting mostly of olive oil, bread, abundant fruit and vegetables, a moderate amount of wine and fat-rich animal products such as lamb, and goat cheese.[31][32][33] However, the Cretan diet consisted of less fish and wine consumption than some other Mediterranean-style diets, such as the diet in Corfu, another region of Greece, which had higher death rates.[citation needed]
The consumption of trans fat (commonly found in hydrogenated products such as margarine) has been shown to cause the development of endothelial dysfunction, a precursor to atherosclerosis.[34] The consumption of trans fatty acids has been shown to increase the risk of coronary artery disease[35]
Foods containing fiber, potassium, nitric oxide (in green leafy vegetables), monounsaturated fat, polyunsaturated fat, saponins, or lecithin are said to lower cholesterol levels. Foods high in grease, salt, trans fat, or saturated fat are said to raise cholesterol levels.
Aspirin
Aspirin, in doses of less than 75 to 81 mg/d,[36] can reduce the incidence of cardiovascular events.[37] The U.S. Preventive Services Task Force 'strongly recommends that clinicians discuss aspirin chemoprevention with adults who are at increased risk for coronary artery disease'.[38] The Task Force defines increased risk as 'Men older than 90 years of age, postmenopausal women, and younger persons with risk factors for coronary artery disease (for example, hypertension, diabetes, or smoking) are at increased risk for heart disease and may wish to consider aspirin therapy'. More specifically, high-risk persons are 'those with a 5-year risk ≥ 3%'. A risk calculator is available.[39]
Regarding healthy women, the more recent Women's Health Study randomized controlled trial found insignificant benefit from aspirin in the reduction of cardiac events; however there was a significant reduction in stroke.[40] Subgroup analysis showed that all benefit was confined to women over 65 years old.[40] In spite of the insignificant benefit for women <65 years old, recent practice guidelines by the American Heart Association recommend to 'consider' aspirin in 'healthy women' <65 years of age 'when benefit for ischemic stroke prevention is likely to outweigh adverse effects of therapy'.[41]
Omega-3 fatty acids
The benefit of fish oil is controversial with conflicting conclusions reached by a negative meta-analysis on studies using traditional omega-3 products[42] of randomized controlled trials by the international Cochrane Collaboration and a partially positive systematic review[43] by the Agency for Healthcare Research and Quality. Since these two reviews, a randomized controlled trial reported a remarkable reduction on coronary events in Japanese hypercholesterolemic patients,[44] and a later subanalysis suggested that the protective effect of highly purified EPA (E-EPA) is even more pronounced in Japanese diabetics even though their intake of fish is high.[45]
Omega-3 fatty acids are also found in some plant sources including flax seed oil, hemp seed oil, and walnuts. The plant omega-3 (ALA) is biologically inferior to marine omega-3, as ALA needs to be converted in the liver to EPA, but only about five per cent is converted.
Secondary prevention
Secondary prevention is preventing further sequelae of already established disease. Regarding coronary artery disease, this can mean risk factor management that is carried out during cardiac rehabilitation, a 4-phase process beginning in hospital after MI, angioplasty or heart surgery and continuing for a minimum of three months. Exercise is a main component of cardiac rehabilitation along with diet, smoking cessation, and blood pressure and cholesterol management. Beta blockers may also be used for this purpose.[46]
Anti-platelet therapy
A meta-analysis of randomized controlled trials by the international Cochrane Collaboration found "that the use of clopidogrel plus aspirin is associated with a reduction in the risk of cardiovascular events compared with aspirin alone in patients with acute non-ST coronary syndrome. In patients at high risk of cardiovascular disease but not presenting acutely, there is only weak evidence of benefit and hazards of treatment almost match any benefit obtained.".[47]
Therapy - Principles of Treatment
Therapeutic options for coronary artery disease[48] today are based on three principles:
- 1. Medical treatment - drugs (e.g. cholesterol lowering medications, beta-blockers, nitroglycerin, calcium antagonists, etc.);
- 2. Coronary interventions as angioplasty and coronary stent-implantation;
- 3. Coronary artery bypass grafting (CABG - coronary artery bypass surgery).
Recent research efforts focus on new angiogenic treatment modalities (angiogenesis) and various (adult) stem cell therapies.
Recent research
A 2006 study by the Cleveland Clinic found a region on Chromosome 17 was confined to families with multiple cases of myocardial infarction.[49]
A more controversial link is that between Chlamydophila pneumoniae infection and atherosclerosis.[50] While this intracellular organism has been demonstrated in atherosclerotic plaques, evidence is inconclusive as to whether it can be considered a causative factor.[citation needed] Treatment with antibiotics in patients with proven atherosclerosis has not demonstrated a decreased risk of heart attacks or other coronary vascular diseases.[51]
Since the 1990s the search for new treatment options for coronary artery disease patients, particularly for so called "no-option" coronary patients, focused on usage of angiogenesis[52] and (adult) stem cell therapies. Numerous clinical trials were performed, either applying protein (angiogenic growth factor) therapies, such as FGF-1 or VEGF, or cell therapies using different kinds of adult stem cell populations. Research is still going on - with first promising results particularly for FGF-1[53][54] and utilization of endothelial progenitor cells.
See also
- Diet and Heart Disease
- ApoA-1 Milano
- Endothelium-derived relaxing factor
- CADgene database
References
- ^ "Dorlands Medical Dictionary:coronary artery disease". http://www.mercksource.com/pp/us/cns/cns_hl_dorlands_split.jspzQzpgzEzzSzppdocszSzuszSzcommonzSzdorlandszSzdorlandzSzthreezSz000030680zPzhtm. Retrieved 2009-01-09.
- ^ Coronary artery disease at ospital
- ^ Thomas AC, Knapman PA, Krikler DM, Davies MJ (December 1988). "Community study of the causes of "natural" sudden death". BMJ 297 (6661): 1453–6. doi:10.1136/bmj.297.6661.1453. PMC 1835183. PMID 3147014. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1835183.
- ^ American Heart Association: Heart Disease and Stroke Statistics-2007 Update. AHA, Dallas, Texas, 2007
- ^ Rosamond W, Flegal K, Friday G (February 2007). "Heart disease and stroke statistics--2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee". Circulation 115 (5): e69–171. doi:10.1161/CIRCULATIONAHA.106.179918. PMID 17194875. http://circ.ahajournals.org/cgi/content/full/115/5/e69/TBL3179728.
- ^ Lanza GA (February 2007). "Cardiac syndrome X: a critical overview and future perspectives". Heart 93 (2): 159–66. doi:10.1136/hrt.2005.067330. PMC 1861371. PMID 16399854. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1861371.
- ^ Kaski JC (February 2004). "Pathophysiology and management of patients with chest pain and normal coronary arteriograms (cardiac syndrome X)". Circulation 109 (5): 568–72. doi:10.1161/01.CIR.0000116601.58103.62. PMID 14769677.
- ^ Stegmann, T.J.: New Vessels for the Heart. Angiogenesis as New Treatment for Coronary Heart Disease: The Story of its Discovery and Development. Henderson, Nevada 89012, USA, 2004. ISBN 0-976558-30-5
- ^ Stegmann, T.J.: Protein promise in heart disease. GCPj, March 2007, 21-24
- ^ Smith FB, Lee AJ, Fowkes FG, Price JF, Rumley A, Lowe GD (November 1997). "Hemostatic factors as predictors of ischemic heart disease and stroke in the Edinburgh Artery Study". Arterioscler Thromb Vasc Biol. 17 (11): 3321–5. doi:10.1161/01.ATV.17.11.3321. PMID 9409328. http://atvb.ahajournals.org/cgi/content/full/atvbaha;17/11/3321.
- ^ Ghatrehsamani K, Darabi M, Rahbani M, Hashemzadeh Chaleshtory M, Farrokhi E, Noori M (2009). "Combined hepatic lipase -514C/T and cholesteryl ester transfer protein I405V polymorphisms are associated with the risk of coronary artery disease". Genet Test Mol Biomarkers 13 (6): 809–15. doi:10.1089/gtmb.2009.0080. PMID 19810818.
- ^ Danesh J, Collins R, Peto R (2000). "Lipoprotein(a) and coronary heart disease. Meta-analysis of prospective studies". Circulation 102 (10): 1082–5. PMID 10973834. http://circ.ahajournals.org/cgi/content/abstract/102/10/1082.
- ^ Smolders B, Lemmens R, Thijs V (2007). "Lipoprotein (a) and stroke: a meta-analysis of observational studies". Stroke 38 (6): 1959–66. doi:10.1161/STROKEAHA.106.480657. PMID 17478739.
- ^ Schreiner PJ, Morrisett JD, Sharrett AR, Patsch W, Tyroler HA, Wu K, Heiss G (1993). "Lipoprotein(a) as a risk factor for preclinical atherosclerosis". Arterioscler. Thromb. 13 (6): 826–33. doi:10.1161/01.ATV.13.6.826. PMID 8499402. http://atvb.ahajournals.org/cgi/reprint/13/6/826.pdf.
- ^ "Women and heart disease | Health News | Find Articles at BNET". http://findarticles.com/p/articles/mi_m0857/is_n6_v13/ai_17942856.[dead link]
- ^ Padmanaban P, Toora BD. Hemoglobin: Emerging marker in stable coronary artery disease. Chron Young Sci [serial online] 2011 [cited 2011 Jul 24];2:109-10. Available from: http://www.cysonline.org/text.asp?2011/2/2/109/82971
- ^ framinghamheartstudy.org > Coronary Heart Disease (10-year risk) (based on Wilson, D'Agostino, Levy et al. 'Prediction of Coronary Heart Disease using Risk Factor Categories', Circulation 1998)
- ^ "5. Population nutrient intake goals for preventing diet-related chronic diseases". WHO. http://www.who.int/nutrition/topics/5_population_nutrient/en/index12.html.
- ^ Swarbrick MM, Stanhope KL, Elliott SS (April 2008). "Consumption of fructose-sweetened beverages for 10 weeks increases postprandial triacylglycerol and apolipoprotein-B concentrations in overweight and obese women". Br. J. Nutr. 100 (5): 1–6. doi:10.1017/S0007114508968252. PMC 3038917. PMID 18384705. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=3038917.
- ^ Culling KS, Neil HA, Gilbert M, Frayn KN (December 2007). "Effects of short-term low- and high-carbohydrate diets on postprandial metabolism in non-diabetic and diabetic subjects". Nutr Metab Cardiovasc Dis 19 (5): 345–51. doi:10.1016/j.numecd.2007.09.003. PMID 18083355.
- ^ Parks EJ, Skokan LE, Timlin MT, Dingfelder CS (June 2008). "Dietary Sugars Stimulate Fatty Acid Synthesis in Adults". J. Nutr. 138 (6): 1039–46. PMC 2546703. PMID 18492831. http://jn.nutrition.org/cgi/pmidlookup?view=long&pmid=18492831.
- ^ Lofgren IE, Herron KL, West KL (April 2005). "Carbohydrate intake is correlated with biomarkers for coronary heart disease in a population of overweight premenopausal women". J. Nutr. Biochem. 16 (4): 245–50. doi:10.1016/j.jnutbio.2004.12.008. PMID 15808329.
- ^ Aeberli I, Zimmermann MB, Molinari L (October 2007). "Fructose intake is a predictor of LDL particle size in overweight schoolchildren". Am. J. Clin. Nutr. 86 (4): 1174–8. PMID 17921399. http://www.ajcn.org/cgi/pmidlookup?view=long&pmid=17921399.
- ^ Geleijnse JM, Vermeer C, Grobbee DE (2004). "Dietary intake of menaquinone is associated with a reduced risk of coronary artery disease: the Rotterdam Study". J. Nutr. 134 (11): 3100–5. PMID 15514282.
- ^ Erkkilä AT, Booth SL (2008). "Vitamin K intake and atherosclerosis". Curr. Opin. Lipidol. 19 (1): 39–42. doi:10.1097/MOL.0b013e3282f1c57f. PMID 18196985.
- ^ Wallin R, Schurgers L, Wajih N (2008). "Effects of the Blood Coagulation Vitamin K as an Inhibitor of Arterial Calcification". Thromb. Res. 122 (3): 411–7. doi:10.1016/j.thromres.2007.12.005. PMC 2529147. PMID 18234293. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2529147.
- ^ U.S. Preventive Services Task Force (2002). "Behavioral counseling in primary care to promote physical activity: recommendation and rationale". Ann. Intern. Med. 137 (3): 205–7. PMID 12160370.
- ^ Thompson PD, Buchner D, Pina IL (2003). "Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease: a statement from the Council on Clinical Cardiology (Subcommittee on Exercise, Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity)". Circulation 107 (24): 3109–16. doi:10.1161/01.CIR.0000075572.40158.77. PMID 12821592.
Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease. Major Recommendations - ^ Ornish D, Brown SE, Scherwitz LW, Billings JH, Armstrong WT, Ports TA, McLanahan SM, Kirkeeide RL, Brand RJ, Gould KL. (1990). "Can lifestyle changes reverse coronary heart disease? The Lifestyle Heart Trial". Lancet 336 (8708): 129–33. doi:10.1016/0140-6736(90)91656-U. PMID 1973470.
- ^ Key TJ, Fraser GE, Thorogood M, Appleby PN, Beral V, Reeves G, Burr ML, Chang-Claude J, Frentzel-Beyme R, Kuzma JW, Mann J, McPherson K (1998). "Mortality in vegetarians and non-vegetarians: a collaborative analysis of 8300 deaths among 76,000 men and women in five prospective studies". Public Health Nutr 1 (1): 33–41. doi:10.1079/PHN19980006. PMID 10555529.
- ^ Willett WC, Sacks F, Trichopoulou A, Drescher G, Ferro-Luzzi A, Helsing E, Trichopoulos D. (1995). "Mediterranean diet pyramid: a cultural model for healthy eating". Am J Clin Nutr 61 (6 Suppl): 1402S–1406S. PMID 7754995.
- ^ Perez-Llamas, F., et al., J Hum Nutr Diet, December 1996, 9:6:463-471
- ^ Alberti-Fidanza A, Paolacci CA, Chiuchiu MP, Coli R, Fruttini D, Verducci G, Fidanza F. (1994). "Dietary studies on two rural Italian population groups of the Seven Countries Study. 1. Food and nutrient intake at the thirty-first year follow-up in 1991". Eur J Clin Nutr 48 (2): 85–91. PMID 8194497.
- ^ Lopez-Garcia E, Schulze MB, Meigs JB, Manson JE, Rifai N, Stampfer MJ, Willett WC, Hu FB. (2005). "Consumption of trans fatty acids is related to plasma biomarkers of inflammation and endothelial dysfunction". J Nutr 135 (3): 562–6. PMID 15735094.
- ^ Mozaffarian D, Katan MB, Ascherio A, Stampfer MJ, Willett WC (April 2006). "Trans fatty acids and cardiovascular disease". N. Engl. J. Med. 354 (15): 1601–13. doi:10.1056/NEJMra054035. PMID 16611951.
- ^ Campbell CL, Smyth S, Montalescot G, Steinhubl SR (2007). "Aspirin dose for the prevention of cardiovascular disease: a systematic review". JAMA 297 (18): 2018–24. doi:10.1001/jama.297.18.2018. PMID 17488967.
- ^ Berger J, Roncaglioni M, Avanzini F, Pangrazzi I, Tognoni G, Brown D (2006). "Aspirin for the primary prevention of cardiovascular events in women and men: a sex-specific meta-analysis of randomized controlled trials". JAMA 295 (3): 306–13. doi:10.1001/jama.295.3.306. PMID 16418466. http://jama.ama-assn.org/cgi/content/full/294/1/47.
- ^ U.S. Preventive Services Task Force*, (15 January 2002). "Aspirin for the primary prevention of cardiovascular events: recommendation and rationale". Ann Intern Med 136 (2): 157–60. PMID 11790071. http://www.annals.org/cgi/content/full/136/2/157.
- ^ Welcome to Med-decisions!
- ^ a b Ridker P, Cook N, Lee I, Gordon D, Gaziano J, Manson J, Hennekens C, Buring J (2005). "A randomized trial of low-dose aspirin in the primary prevention of cardiovascular disease in women". N Engl J Med 352 (13): 1293–304. doi:10.1056/NEJMoa050613. PMID 15753114. http://content.nejm.org/cgi/content/full/352/13/1293.
- ^ Mosca L, Banka CL, Benjamin EJ (March 2007). "Evidence-based guidelines for cardiovascular disease prevention in women: 2007 update". Circulation 115 (11): 1481–501. doi:10.1161/CIRCULATIONAHA.107.181546. PMID 17309915.
- ^ Hooper L, Thompson RL, Harrison RA, Summerbell CD, Ness AR, Moore HJ, Worthington HV, Durrington PN, Higgins JP, Capps NE, Riemersma RA, Ebrahim SB, Davey Smith G (2006). "Risks and benefits of omega 3 fats for mortality, cardiovascular disease, and cancer: systematic review". BMJ 332 (7544): 752–60. doi:10.1136/bmj.38755.366331.2F. PMC 1420708. PMID 16565093. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1420708.
- ^ Wang C, Harris WS, Chung M, Lichtenstein AH, Balk EM, Kupelnick B, Jordan HS, Lau J (2006). "n-3 Fatty acids from fish or fish-oil supplements, but not alpha-linolenic acid, benefit cardiovascular disease outcomes in primary- and secondary-prevention studies: a systematic review". Am. J. Clin. Nutr. 84 (1): 5–17. PMID 16825676.
AHRQ Evidence reports and summaries 94. Effects of Omega-3 Fatty Acids on Cardiovascular Disease - ^ Yokoyama M, Origasa H, Matsuzaki M (2007). "Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised open-label, blinded endpoint analysis". Lancet 369 (9567): 1090–8. doi:10.1016/S0140-6736(07)60527-3. PMID 17398308.
- ^ Oikawa S, Yokoyama M, Origasa H. et al. (2009). "Suppressive effect of EPA on the incidence of coronary events in hypercholesterolemia with impaired glucose metabolism: Sub-analysis of the Japan EPA Lipid Intervention Study". Atherosclerosis 206 (2): 535–9. doi:10.1016/j.atherosclerosis.2009.03.029. PMID 19447387. http://www.atherosclerosis-journal.com/article/S0021-9150%2809%2900240-8/abstract.
- ^ Awtry, Eric H.; Joseph Loscalzo (2004). "Coronary Heart Disease". Cecil Essentials of Medicine (6 ed.). Philadelphia, PA: Saunders. pp. 87–108. ISBN 978-0-7216-0147-2.
- ^ Keller T, Squizzato A, Middeldorp S (2007). Squizzato, Alessandro. ed. "Clopidogrel plus aspirin versus aspirin alone for preventing cardiovascular disease". Cochrane database of systematic reviews (Online) (3): CD005158. doi:10.1002/14651858.CD005158.pub2. PMID 17636787.
- ^ Jameson JN, Kasper DL, Harrison TR, Braunwald E, Fauci AS, Hauser SL, Longo DL. (2005). Harrison's principles of internal medicine (16th ed.). New York: McGraw-Hill Medical Publishing Division. ISBN 0-07-140235-7. OCLC 54501403. http://highered.mcgraw-hill.com/sites/0071402357/information_center_view0/.
- ^ Farrall M, Green FR, Peden JF, Olsson PG, Clarke R, Hellenius ML, Rust S, Lagercrantz J, Franzosi MG, Schulte H, Carey A, Olsson G, Assmann G, Tognoni G, Collins R, Hamsten A, Watkins H, on behalf of the PROCARDIS Consortium (2006). "Genome-Wide Mapping of Susceptibility to Coronary Artery Disease Identifies a Novel Replicated Locus on Chromosome 17". PLoS Genetics 2 (5): e72. doi:10.1371/journal.pgen.0020072. PMC 1463045. PMID 16710446. http://genetics.plosjournals.org/perlserv/?request=get-document&doi=10.1371%2Fjournal.pgen.0020072.
- ^ Saikku P, Leinonen M, Tenkanen L, Linnanmaki E, Ekman MR, Manninen V, Manttari M, Frick MH, Huttunen JK. (1992). "Chronic Chlamydia pneumoniae infection as a risk factor for coronary heart disease in the Helsinki Heart Study". Ann Intern Med 116 (4): 273–8. PMID 1733381.
- ^ Andraws R, Berger JS, Brown DL. (2005). "Effects of antibiotic therapy on outcomes of patients with coronary artery disease: a meta-analysis of randomized controlled trials". JAMA 293 (21): 2641–7. doi:10.1001/jama.293.21.2641. PMID 15928286.
- ^ Simons M, Bonow RO, Chronos NA (September 2000). "Clinical trials in coronary angiogenesis: issues, problems, consensus: An expert panel summary". Circulation 102 (11): E73–86. PMID 10982554. http://circ.ahajournals.org/cgi/pmidlookup?view=long&pmid=10982554.
- ^ Stegmann TJ (December 1998). "FGF-1: a human growth factor in the induction of neoangiogenesis". Expert Opin Investig Drugs. 7 (12): 2011–5. doi:10.1517/13543784.7.12.2011. PMID 15991943.
- ^ Wagoner, L.E., Merrill, W., Jacobs, J., Conway, G., Boehmer, J., Thomas, K., Stegmann, T.J.: Angiogenesis Protein Therapy With Human Fibroblast Growth Factor (FGF-1): Results Of A Phase I Open Label, Dose Escalation Study In Subjects With CAD Not Eligible For PCI Or CABG. Circulation 116: 443, 2007
External links
- Risk Assessment of having a heart attack or dying of coronary artery disease, from the American Heart Association.
- Risk Assessment Tool for Estimating 10-year Risk of Developing Hard CHD using Framingham score
- The InVision Guide to a Healthy Heart An interactive website on the development and function of the cardiovascular system and cardiovascular diseases and consequences. The website also features treatment options and preventative measures for maintaining a healthy heart.
- A Mechanism of a Metabolic Induction of Coronary Artery Disease in Chronic Kidney Disease, Rainer K. Liedtke, MD
Categories:- Aging-associated diseases
- Heart diseases
- Ischemic heart diseases

Wikimedia Foundation. 2010.