- Cardiac stress test
-
Not to be confused with Cardiac arrest.
Cardiac stress test Intervention 
A male patient walks on a stress test treadmill to have his heart's function checkedICD-9-CM 89.4 MeSH D025401 Cardiac stress test (or Cardiac diagnostic test) is a test used in medicine and cardiology to measure the heart's ability to respond to external stress in a controlled clinical environment.
The stress response is induced by exercise or drug stimulation. Cardiac stress tests compare the coronary circulation while the patient is at rest with the same patient's circulation observed during maximum physical exertion, showing any abnormal blood flow to the heart's muscle tissue (the myocardium). The results can be interpreted as a reflection on the general physical condition of the test patient. This test can be used to diagnose ischemic heart disease, and for patient prognosis after a heart attack (myocardial infarction).
Contents
Cardiac stress test
Not to be confused with Cardiac cycle.The cardiac stress test is done with heart stimulation, either by exercise on a treadmill, pedalling a stationary exercise bicycle ergometer[1] or with intravenous pharmacological stimulation, with the patient connected to an electrocardiogram (or ECG).
People who cannot use their legs may exercise with a bicycle-like crank that you can turn with your arms.[2]
The level of mechanical stress is progressively increased by adjusting the difficulty (steepness of the slope) and speed. The test administrator or attending physician examines the symptoms and blood pressure response. With use of ECG, the test is most commonly called a cardiac stress test, but is known by other names, such as exercise testing, stress testing treadmills, exercise tolerance test, stress test or stress test ECG.
Stress echocardiography
A stress test may be accompanied by echocardiography.[1] The echocardiography is performed both before and after the exercise so that structural differences can be compared.
Nuclear stress test
Typically, a radiotracer (Tc-99 sestamibi or Tl-201) may be injected during the test. After a suitable waiting period to ensure proper distribution of the radiotracer, photos are taken with a gamma camera to capture images of the blood flow. Photos taken before and after exercise are examined to assess the state of the coronary arteries of the patient.
Showing the relative amounts of radioisotope within the heart muscle, the nuclear stress tests more accurately identify regional areas of reduced blood flow.
Stress and potential cardiac damage from exercise during the test is a problem in patients with ECG abnormalities at rest or in patients with severe motor disability. Pharmacological stimulation from vasodilators such as dipyridamole or adenosine, or positive chronotropic agents such as dobutamine can be used. Testing personnel can include a cardiac radiologist, a nuclear medicine physician, a cardiologist, and/or a nurse.
Function
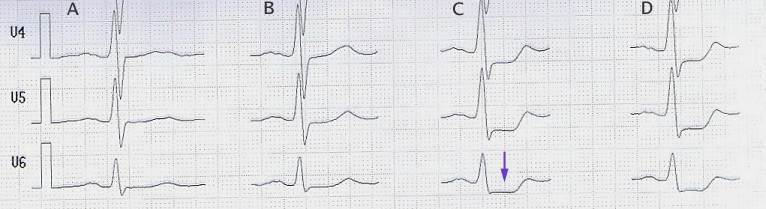
 Stress-ECG of a patient with coronary heart disease: ST-segment depression (arrow) at 100 Watt. A in rest, B at 75 Watt, C at 100 Watt, D at 125 Watt.
Stress-ECG of a patient with coronary heart disease: ST-segment depression (arrow) at 100 Watt. A in rest, B at 75 Watt, C at 100 Watt, D at 125 Watt.
The American Heart Association recommends ECG treadmill testing as the first choice for patients with medium risk of coronary heart disease according to risk factors of smoking, family history of coronary artery stenosis, hypertension, diabetes and high cholesterol.
- Perfusion stress test (or sestamibi) is appropriate for select patients, especially those with an abnormal resting electrocardiogram.
- Intracoronary ultrasound or angiogram can provide more information at the risk of complications associated with cardiac catheterization.
Diagnostic value
The common approach for stress testing by American College of Cardiology and American Heart Association indicates the following: [2]
- Treadmill test: sensitivity 67%, specificity 70%
- Nuclear test: sensitivity 81%, specificity 85-95%
(Sensitivity is the percentage of sick people who are correctly identified as having the condition. Specificity indicates the percentage of healthy people who are correctly identified as not having the condition.)
The value of stress tests has always been recognized as limited in assessing heart disease such as atherosclerosis, a condition which mainly produces wall thickening and enlargement of the arteries. This is because the stress test compares the patient's coronary flow status before and after exercise and is suitable to detecting specific areas of ischemia and lumen narrowing, not a generalized arterial thickening.
According to American Heart Association data[citation needed], about 65% of men and 47% of women have as their first symptom of cardiovascular disease a heart attack or sudden cardiac arrest. Stress tests, carried out shortly before these events, are not relevant to the prediction of infarction in the majority of individuals tested.[dubious ] Over the past two decades, better methods[citation needed] have been developed to identify atherosclerotic disease before it becomes symptomatic.
These detection methods have included either anatomical or physiological.
- Examples of anatomical methods include
- CT coronary calcium score
- Intima-media thickness (IMT)
- Intravascular ultrasound (IVUS)
- Examples of physiological methods include
- Lipoprotein analysis
- HbA1c
- Hs-CRP
- Homocysteine
The anatomic methods directly measure some aspects of the actual process of atherosclerosis itself and therefore offer the possibility of early diagnosis, but are often more expensive and may be invasive (in the case of IVUS, for example). The physiological methods are often less expensive and more secure, but are not able to quantify the current status of the disease or directly track progression.[citation needed]
Absolute contraindications
Absolute contraindications to cardiac stress test include:
- Acute myocardial infarction within 48 hours
- Unstable angina not yet stabilized with medical therapy
- Uncontrolled cardiac arrhythmia, which may have significant hemodynamic responses (e.g. ventricular tachycardia)
- Severe symptomatic aortic stenosis, aortic dissection, pulmonary embolism, and pericarditis
- Multivessel coronary artery diseases that have a high risk of producing an acute myocardial infarction
Adverse effects
Side effects from cardiac stress testing may include
- Palpitations, chest pain, MI, shortness of breath, headache, nausea or fatigue.
- Adenosine and dipyridamole can cause mild hypotension.
- As the tracers used for this test are carcinogenic, frequent use of these tests carries a small risk of cancer.
Pharmacological agents
The choice of pharmacologic stress agents used in the test depends on factors such as potential drug interactions with other treatments and concomitant diseases.
Pharmacologic agents such as Adenosine, Lexiscan (Regadenoson), or dipyridamole is generally used when a patient cannot achieve adequate work level with treadmill exercise, or has poorly controlled hypertension or left bundle branch block. However, a exercise stress test may provide more information about exercise tolerance than a pharmacologic stress test.[3]
Commonly used agents include:
- Vasodilators acting as adenosine receptor agonists, such as Adenosine itself, and Dipyridamole (brand name "Persantine"),[4] which acts indirectly at the receptor.
- Regadenoson (brand name "Lexiscan"), which acts specifically at the Adenosine A2A receptor, thus affecting the heart more than the lung.
- Dobutamine. The effects of beta-agonists such as dobutamine can be reversed by administering beta-blockers such as propranolol.
Lexiscan (Regadenoson) or Dobutamine is often used in patients with severe reactive airway disease (Asthma or COPD) as adenosine and dipyridamole can cause acute exacerbation of these conditions. If the patient's Asthma is treated with an inhaler then it should be used as a pre-treatment prior to the injection of the pharmacologic stress agent. In addition, if the patient is actively wheezing then the physician should determine the benefits versus the risk to the patient of performing a stress test especially outside of a hospital setting.
Aminophylline may be used to attenuate severe and/or persistent adverse reactions to Adenosine and Lexiscan.
Limitations
The stress test does not detect:
- Atheroma
- Vulnerable plaques
The test has relatively high rates of false positives and false negatives compared with other clinical tests.
Results
Once the stress test is completed, the patient generally is advised to not suddenly stop activity, but to slowly decrease the intensity of the exercise over the course of several minutes.
- Increased spatial resolution allows a more sensitive detection of ischemia.
- Stress testing, even if made in time, is not able to guarantee the prevention of symptoms, fainting, or death. Stress testing, although more effective than a resting ECG at detecting heart function, is only able to detect certain cardiac properties.
- The detection of high-grade coronary artery stenosis by a cardiac stress test was the key to recognizing people who have heart attacks since 1980. From 1960 to 1990, despite the success of stress testing to identify many who were at high risk of heart attack, the inability of this test correctly identify many others is discussed in medical circles but unexplained.
- High degrees of coronary artery stenosis, which are detected by stress testing methods are often, though not always, responsible for recurrent symptoms of angina.
- Unstable atheroma produces "vulnerable plaques" hidden within the walls of coronary arteries which go undetected by this test.
- Limitation in blood flow to the left ventricle can lead to recurrent angina pectoris.
See also
Cardiac
Cardiac arrest
Harvard Step Test
Metabolic equivalent
Robert A. BruceReferences
- ^ Rimmerman, Curtis (2009-05-05). The Cleveland Clinic Guide to Heart Attacks. Kaplan Publishing. pp. 113–. ISBN 9781427799685. http://books.google.com/books?id=o3k3fLOjUNEC&pg=PA113. Retrieved 25 September 2011.
- ^ Gibbons, R., Balady, G.; Timothybricker, J., Chaitman, B., Fletcher, G., Froelicher, V., Mark, D., McCallister, B. et al. (2002). "ACC / AHA 2002 guideline update for exercise testing: summary articleA report of the American College of Cardiology / American Heart Association Task Force on Practice Guidelines,Journal of the American College of Cardiology
- ^ Weissman, Neil J.; Adelmann, Gabriel A. (2004). Cardiac imaging secrets. Elsevier Health Sciences. pp. 126–. ISBN 9781560535157. http://books.google.com/books?id=TTWdpgTFU9cC&pg=PA126. Retrieved 25 September 2011.
- ^ Nicholls, Stephen J.; Worthley, Stephen (2011-01). Cardiovascular Imaging for Clinical Practice. Jones & Bartlett Learning. pp. 198–. ISBN 9780763756222. http://books.google.com/books?id=JUDJp7DFpxUC&pg=PA198. Retrieved 25 September 2011.
Further reading
- Sabatine, Marc (February 15, 2000). Pocket Medicine. Lippincott Williams & Wilkins. pp. 256 pages.
- Master AM, Oppenheimer ET (1929). "A simple exercise tolerance test for circulatory efficiency with standard tables for normal individuals". Am J Med Sci . . Retrieved , retrieved on 6 August 2010.
- Gibbons, R.; Balady, G.; Timothybricker, J.; Chaitman, B.; Fletcher, G.; Froelicher, V.; Mark, D.; McCallister, B. et al. (2002). "ACC/AHA 2002 guideline update for exercise testing: summary articleA report of the American college of cardiology/American heart association task force on practice guidelines ". Journal of the American College of Cardiology , - retrieved on 6 August 2010
- E. Boden, William; Robert A. O'Rourke, Koon K. Teo, Pamela M. Hartigan, David J. Maron, M.D., William J. Kostuk, M.D., Merril Knudtson, M.D. et al. (2007). "Optimal Medical Therapy with or without PCI for Stable Coronary Disease: the COURAGE trial". New England Journal of Medicine - consulted in 12th of april 2010.
- Medline Plus ,Exercise Stress Test - Retrieved on 26 January 2010
- Harvard Health Publications,Preparation for an Exercise Stress - Retrieved on 26 January 2010
- Exercise Stress ,Cool down properly - Retrieved on 2010-01-26
- Cardiac Stress,Expect after the test - Retrieved on 2010-01-26
- Circulation, Fletcher et al. AHA Exercise Standards for Testing.
- National Guideline Clearinghouse. Cardiac Stress Test Supplement. ,2003,
- Michael Jerosch-Herold; Seethamraju, RT; Swingen, CM; Wilke, NM; Stillman, AE (2004). "Analysis of myocardial perfusion MRI". Journal of MRI.
- Thomson LE; Kim, RJ; Judd, RM ,2004, "Magnetic resonance imaging for the assessment of myocardial viability". Journal of MRI.
- A. de González (2004). "Risk of cancer from diagnostic X-rays: estimates for the UK and 14 other countries". The Lancet
- Morin; Gerber, TC; McCollough, CH ,2003, "Radiation Dose in Computed Tomography of the Heart".Circulation.
External links
- medline plus
- Harvard Health Publication
- medicine.net
- cardiacstress.net
- American journal of medical sciences
- New england journal of medicine
- Stress Test Info from the American Heart Association
- Nuclear stress test at NIH MedLine
- Stress test FAQ's
- Adenosine Nuclear Stress Test
- Dobutamine Nuclear Stress Test
Categories:- Cardiac procedures
- Radiology
- Nuclear medicine
- Medical tests

Wikimedia Foundation. 2010.