- Substituted amphetamine
-
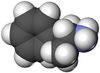
- Optical isomers of amphetamine
-

L-amphetamine
-
-
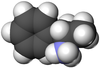
Substituted amphetamines are a chemical class of stimulants, entactogens, hallucinogens, and other drugs. They feature a phenethylamine core with a methyl group attached to the alpha carbon resulting in amphetamine, along with additional substitutions. Examples of amphetamines are amphetamine (itself), methamphetamine, ephedrine, cathinone, MDMA ("Ecstasy"), and DOM ("STP").
Amphetamine derivatives occur in nature, for example in the leaves of Ephedra and khat plants. These have been used since antiquity for their pharmacological effects. Amphetamines were first produced synthetically at the end of the 19th century. By the 1930s such synthetic amphetamines found use as decongestants in the symptomatic treatment of colds and also occasionally as psychoactive agents. Their effects on the central nervous system are diverse, but can be summarized by three overlapping types of activity: psychoanaleptic, hallucinogenic and empathogenic. Various amphetamines may cause these actions either separately or in combination. Improper consumption of amphetamine derivatives may result in addiction and aggressiveness, as well as in rapid deterioration of basic body functions and death. Therefore, production and distribution of most related drugs are controlled by the authorities both nationally and internationally.
Contents
History
Although the basic compound of the class, amphetamine, was synthesized earlier, Ephedra was used 5000 years ago in China as a medicinal plant; its active ingredients are alkaloids ephedrine, pseudoephedrine, norephedrine (phenylpropanolamine) and norpseudoephedrine (cathine). Natives of Yemen and Ethiopia have a long tradition of chewing khat leaves to achieve a stimulating effect. The active substances of khat are cathinone and to a lesser extent cathine.[1]
Amphetamine was first synthesized in 1887 by Romanian chemist Lazăr Edeleanu and did not attract special attention.[2] MDMA was produced in 1912 (according to other sources in 1914[3]) as an intermediate product. However, this synthesis also went largely unnoticed.[4] In the 1920s, both methamphetamine and an optical isomer of amphetamine dextroamphetamine (D-amphetamines) were synthesized. This synthesis was a by-product of a search for ephedrine, a bronchodialator used to treat asthma extracted exclusively from natural sources. Over-the-counter use of amphetamines was initiated in early 1930s by the pharmaceutical company Smith, Kline & French (now part of GlaxoSmithKline), as a medicine (Benzedrine) for colds and nasal congestion. Subsequently, amphetamine was used in the treatment of narcolepsy, obesity, hay fever, orthostatic hypotension, epilepsy, Parkinson's disease, alcoholism and migraine.[2][5] The "reinforcing" effects of amphetamines were quickly discovered, and the misuse of amphetamines had been noted as far back as 1936.[5]
During World War II, amphetamines were used by the German military to keep their tank crews awake for long periods, and treat depression. It was noticed that extended rest was required after such artificially induced activity.[2]
The widespread use of amphetamines began in the postwar Japan and quickly spread to other countries. Modified ("designer"), amphetamines gained popularity since 1960s, such as MDA and PMA.[5] MDMA was rediscovered and popularized by the American chemist Alexander Shulgin in 1965, after which it was used for some time in psychotherapy sessions.[4] In 1970, the United States adopted "the Controlled Substances Act" that limited non-medical use of amphetamines.[5] Street use of PMA was noted in 1972,[6] and in 1985, MDMA was banned by the US authorities in an emergency scheduling initiated by the US Drug Enforcement Agency.[7]
Since the mid 1990s, MDMA ("ecstasy") became a popular entactogenic drug among the youth and quite often non-MDMA substances were sold as "ecstasy".[8] In the first legally sanctioned trials in the USA in over twenty years, the safety profile of MDMA has been demonstrated, and it has been shown to be a successful adjunct to psychotherapy in the management of treatment-resistant Post-Traumatic Stress Disorder (PTSD) in victims of sexual abuse and sufferers of other conditions.[9]
Structure
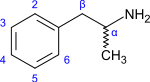 Structural formula of amphetamine
Structural formula of amphetamine
Amphetamines are a subgroup of the substituted phenethylamine class of compounds. Substitution of hydrogen atoms results in a large class of compounds. Typical reaction is substitution by methyl and sometimes ethyl groups at the amine and phenyl sites:[10][11][12]
Substance Substitutes Structure N α β phenyl group 2 3 4 5 Amphetamine (α-methylphenylethylamine) -CH3 
Methamphetamine (N-methylamphetamine) -CH3 -CH3 
Ephedrine pseudoephedrine -CH3 -CH3 -OH 
Cathinone -CH3 =O 
Methcathinone (ephedrone) -CH3 -CH3 =O 
MDA (3,4-methylenedioxyamphetamine) -CH3 -O-CH2-O- 
MDMA (3,4-methylenedioxymethamphetamine) -CH3 -CH3 -O-CH2-O- 
MDEA (3,4-methylenedioxy-N-ethylamphetamine) -CH2-CH3 -CH3 -O-CH2-O- 
EDMA (3,4-ethylenedioxy-N-methylamphetamine) -CH3 -CH3 -O-CH2-CH2-O- 
MBDB (N-methyl-1-(3,4-methylenedioxyphenyl)-2-aminobutane) -CH3 -CH2-CH3 -O-CH2-O- 
PMA (para-metoxyamphetamine) -CH3 -O-CH3 
PMMA (para-metoxymetamphetamine) -CH3 -CH3 -O-CH3 
4-MTA (4-methylthioamphetamine) -CH3 -S-CH3 
3,4-DMA (3,4-dimetoxyamphetamine) -CH3 -O-CH3 -O-CH3 
3,4,5-TMA (3,4,5-trimetoxyamphetamine, α-methylmescaline) -CH3 -O-CH3 -O-CH3 -O-CH3 
DOM (2,5-dimethoxy-4-methylamphetamine) -CH3 -O-CH3 -CH3 -O-CH3 
DOB (2,5-dimethoxy-4-bromoamphetamine) -CH3 -O-CH3 -Br -O-CH3 
Physiological action
Classification of central effects
Effects of amphetamines on the central nervous system are diverse and can be attributed to the three main classes:
- Psychoanaleptic
- Hallucinogenic
- Empathogenic – creating a sense of well-being, openness and empathy to others.
Studies on animals have shown that these classes of effects are independent. Various amphetamines may cause these actions, either separately or in combination; for example, amphetamine adds hallucination effect at high doses (amphetamine psychosis), however this is quite different than the 'hallucinongenic' phenomena that are typically associated with what are often commonly referred to as the psychedelic amphetamines.[13][14][15] The stimulating effect of amphetamine is similar to that of cocaine, but lasts longer.[16]
Mechanisms
The stimulating effect of amphetamines is mainly associated with an increased emissions of catecholamines norepinephrine and dopamine. In the normal operation, synaptic release of catecholamines is carried out by exocytosis of a vesicle which contain a neurotransmitter. Then, the neurotransmitter is reabsorbed from the synaptic cleft into the cytoplasm of the neuron. From the cytoplasm, the neurotransmitter penetrates back into the vesicles via the action of the vesicular monoamine transporter (VMAT).[17]
Presence of amphetamine and its derivative inverts the direction of the transport: neurotransmitter moves from vesicles to the cytoplasm and then to the synaptic cleft. As a result, vesicles are emptied, vesicular release of neurotransmitter is reduced, and the concentration of neurotransmitter in the synaptic cleft increases. In this three mechanisms are utilized:[17][18]
 Mechanism of amphetamine action. Left: normal operation of dopaminergic terminal. Right: dopaminergic terminal in presence of amphetamines. Note the reversal of action of the dopamine transporter (DAT) and the vesicular monoamine transporter (VMAT) and the decrease of the standard vesicular neurotransmitter efflux.
Mechanism of amphetamine action. Left: normal operation of dopaminergic terminal. Right: dopaminergic terminal in presence of amphetamines. Note the reversal of action of the dopamine transporter (DAT) and the vesicular monoamine transporter (VMAT) and the decrease of the standard vesicular neurotransmitter efflux.Inhibitors of reuptake of monoamines, such as cocaine, reduce the emission of monoamines, caused by amphetamine-type stimulants.[19] Effects of hallucinogenic amphetamines is similar to other classical hallucinogens and is related to their agonism to serotonin receptor of the type 5-HT2A.[20] Also, lesser-known mechanisms possibly associated with hallucinogenic effects (in traditional plain stimulant and non-hallucinogen class amphetamines) may potentially include agonism of the trace amine-associated receptors (TAARs) and other functions of the amphetamine molecular skeleton in the CNS.
Structure-Activity Relationships
There is a relationship between the chemical structure of the amphetamine compound and its effects. Substitutions of the amino group enhance the stimulating effect of the substance, but may reduce other actions. Examples include methamphetamine and N-hydroxyamphetamine, which are more powerful stimulants than amphetamine.[12]
Replacing methyl group in the position α to ethyl group reduces the stimulating and hallucinogenic actions, but does not affect the empathogenic action (as in MBDB) and suppression of appetite (as in phentermine).[8][13] Removing the methyl group in position α usually decreases the effectiveness of substance; thus, phenethylamine poorly penetrates the blood-brain barrier and is rapidly metabolized.[21] Substitutions in the phenyl group decrease the stimulating action, but may induce other effects.[22] Substitution in position 4 is usually associated with serotonergic action.[8]
Right-handed (dextrorotatory) enantiomers of amphetamines, such as dextroamphetamine, are usually 4–10 times more potent than left-handed, with the exception for MDMA and a few related substances whose efficiency does not depend on the isomerism.[8]
Peripheral effect
The effect of amphetamines on the autonomic nervous system is mainly due to emissions of norepinephrine. This enhances stimulation of α-and β-adrenoreceptors that can lead to tachycardia (increased heart rate), elevated blood pressure, mydriasis (dilated pupils), sweating and hyperthermia (elevated body temperature).[16][18]
Toxicity
Acute toxicity of amphetamines is primarily related with their impact on the central and peripheral adrenergic receptors. Regarding central nervous system, it can manifest itself as psychosis, visual and tactile hallucination and anxiety. The effects on cardiovascular system are expressed as tachycardia and increased blood pressure. The immediate causes of death from the use of amphetamines are usually hyperthermia, heart arrhythmia or stroke.[16]
Unlike many other drugs, amphetamine and especially methamphetamine are neurotoxic and can irreversibly damage dopaminergic and serotonergic neurons. It is believed that the toxic effect of amphetamines on dopaminergic neurons is associated with the formation of free radicals and peroxynitrite, which is a strong oxidizer. MDMA, moreover, reduces concentration of antioxidants glutathione and vitamin E in the brain, and is therefore neurotoxic in high doses. Whether or not MDMA is neurotoxic as a result of prolonged use in normal doses is being debated.[18][23][24]
Dependence
After prolonged use, amphetamines, except for classical hallucinogens,[25] can induce strong addiction that can last up to several weeks. Some energy drinks contain small levels of amphetamines depending on size and quantity; which can be mistaken in few drug test, depending on time, and amount of consumption.[26] It is believed that psychological dependence on amphetamines, as well as on other drugs, is associated with stimulation by the drug of dopaminergic neurons in the ventral tegmental area. Those neurons are responsible for feelings of reward that affect the processes of learning and adaptation.[27]
Physical dependence on amphetamine-type stimulants is controversial. Interruption after their prolonged use results in fatigue, depression, sleepiness and feeling of hunger. These symptoms may be regarded as components of withdrawal syndrome or just as normal response of the body to the lack of sleep and food that accompanies systematic use of amphetamine-type stimulants.[28]
Classic hallucinogens (such as DOM) do not cause addiction.[25] Laboratory animals which were taught to use stimulants did not use hallucinogens on their own initiative.[21]
Production, distribution and use
Free bases of amphetamines are liquids with limited resistance. Therefore, amphetamines are distributed as salts (sulfates, phosphates and chlorides). Amphetamine is usually sold as tablets and sometimes as capsules or syrup. Methamphetamine is usually available as a powder for inhalation or preparing a solution for intravenous injection, and less often as tablets or capsules. Also common is crystalline methamphetamine hydrochloride intended for smoking.[29] Methylenedioxyamphetamines (MDMA, MDEA) are usually tablets.[30]
Amphetamines have good bioavailability upon oral or intranasal administration.[31] Because of their lipophilicity, amphetamines easily penetrate the blood-brain barrier.[16] A typical oral dose is 5–20 mg for amphetamine and methamphetamine.,[32] 80–150 mg for MDA and MDMA,[33][34] 3–10 mg for DOM[35] and 1–3 mg for DOB.[36] Biological half-life is 8–30 h for amphetamine, 12–34 h for methamphetamine and 5–10 h for MDMA.[16]
The action of amphetamines usually lasts 4–6 hours,[37] but in some cases up to 24 hours.[16]
-

Capsules of amphetamine sulfate
-

Crystals of methamphetamine hydrochloride
-
Ecstasy pills
Treatment of amphetamine poisoning and addiction
One of the most dangerous manifestations of overdose with amphetamine-type stimulants are hyperthermia and hyperactivity which can cause various types of damage in skeletal muscles. Therefore, first aid in such overdose cases includes the physical immobilization of the patient, to prevent possible harm to the patient or others, and sedation by intravenous injection. Hyperthermia is reduced with external cooling and some measures might be taken to increase urination, in order to excrete the poison.[38]
Treatment of addiction to amphetamine and its derivatives are similar to those for other stimulants such as cocaine. Because of the weak physical effect of amphetamine addiction, the use of amphetamines is interrupted abruptly instead of gradually reducing the drug dose.[39][40]
The major symptoms of psychological addiction are depression, feeling of boredom and nostalgia for the pleasure associated with the drug. The treatment is usually based on individual work with the patient and the patient's desire to quit drug use.[41] Despite ongoing intensive search, by 2008, efficient medical treatment has not been available.[42] Although the tests are far from complete,[43] some positive results were achieved with the following drugs:[44]
- Dextroamphetamine, methylphenidate and modafinil (stimulants);
- Bupropion (an antidepressant);
- Risperidone (antipsychotic);
- Rivastigmine (an inhibitor of acetylcholinesterase);[42]
- Lobeline (an inhibitor of dopamine reuptake).[42]
Synthesis
Most amphetamines are synthetic compounds.[18] Exceptions include cathinone which is present in khat leaves and ephedrine and pseudoephedrine, the active components of Ephedra. These natural alkaloids have a much weaker effect than the amphetamine.[45][46]
From ephedrine and its derivatives
Methamphetamine can be obtained through one of the following redox reactions of ephedrine.[47] Ephedrine itself can be extracted from Ephedra.
- Conversion of ephedrine to chloroephedrine using thionyl chloride (SOCl2), followed by catalytic hydrogenation. The most catalysts for this reaction are palladium or platinum);[48]

- Reduction of ephedrine using hydroiodic acid in the presence of red phosphorus.

Similarly, from norephedrine (phenylpropanolamine) can be obtained from amphetamine.[49] Methcathinone (the n-methyl homologue of cathinone) can be obtained by oxidation of ephedrine with potassium permanganate in the presence of acetic acid.[50] Cathinone can be produced by a similar oxidation of phenylpropanolamine (norephedrine).[46]
From safrole
Safrole – the main component of the Sassafras oil – is used for the synthesis of MDA, MDMA and other amphetamines containing methylenedioxyphenyl group as follows:[51]
- Reaction of Safrole with hexamine in the presence of sodium iodide results in MDA;
- Reaction with methanol solution of ammonia at high temperature and pressure also yields MDA; similar reactions with methylamine and ethylamine result, respectively, in MDMA and MDEA.

From phenyl-2-propanone (P2P) and its derivatives
Methamphetamine can be produced by reacting phenyl-2-propanone and (P2P) with methylamine in the presence of aluminium amalgam.[52]

P2P itself is usually obtained from phenylacetic acid and acetic anhydride.[53]
Similarly, MDA or MDMA can be produced from 3,4-methylenedioxyphenyl-2-propanone (MDP2P),[54] and the MDP2P can be obtained from piperonal.[55]
From benzaldehyde and its derivatives
Amphetamines can be synthesized by condensation of benzaldehyde with nitroethane using amine as a catalyst, followed by reduction using, e.g. lithium aluminum hydride.[56][57] Derivatives of benzaldehyde are used in reactions occurring via substitution of the phenyl group of benzaldehyde. For example, piperonal is used for preparing MDA,[33] and it can in turn be extracted as alkaloid piperine present in black pepper.[58]

Market
 Adderall – a drug used in treating ADHD and narcolepsy, which includes levoamphetamine and dextroamphetamine
Adderall – a drug used in treating ADHD and narcolepsy, which includes levoamphetamine and dextroamphetamine
Currently, the application of amphetamines and their derivatives in medicine is very limited. Amphetamine, dextroamphetamine, methamphetamine and methylphenidate (Ritalin) are used in the treatment of narcolepsy and attention-deficit hyperactivity disorder.[5] Bupropion, a substituted cathinone with very weak psychostimulant properties relative to most chemicals of this class, is widely used as an atypical antidepressant and smoking cessation aid, under the brand names Wellbutrin and Zyban, and is also used off-label to treat attention-deficit hyperactive disorder.
According to UN Office on Drugs and Crime (UNODC), the world's illegal production in 2007 was 230 to 640 tons of amphetamine-type stimulants (amphetamine, methamphetamine, methcathinone and derivatives) and 72 to 137 tons of methylenedioxyamphetamine (MDA, MDMA, MDEA).[59] The global market for amphetamine-type stimulants is estimated at $65 billion.[60] Production of amphetamines is mainly concentrated near the markets. The trade is mainly concentrated within a country in order to avoid customs control.[61] North America (mainly the states California and Oregon) is the leader in the production of methamphetamine,[8] whereas Europe dominates the production of amphetamine and methylenedioxyamphetamine (MDA, MDMA, MDEA).[62]
UNODC estimates that between 15 and 50 million people used amphetamines at least once during the year of 2007, that constitutes 0.4–1.2% of the total population aged 15 to 64.[63] In Russia, amphetamines are the third most popular type of drug after marijuana and opiates.[64]
Legal status
Because of potential abuse, distribution of amphetamines and their analogues are controlled by the authorities. Those substances are categorized into schedules I-V. Schedule I substances may be used only for scientific or very limited medical purposes with a special license; those substances may not be sold to individuals, even with a prescription. Turnover of substances from Schedule II is allowed under strict control.[65]
Agents Legal status by 2009.[66][67][68][69] UN Convention on Psychotropic Substances of 1971[65] US Russia D, L-amphetamine (racemic) Schedule II Schedule II Schedule II Dextroamphetamine (D-amphetamine) Schedule II Schedule II Schedule I Levamphetamine (L-amphetamine) Schedule II Schedule II Schedule III Methamphetamine Schedule II Schedule II Schedule I Cathinone Methcathinone Schedule I Schedule I Schedule I MDA, MDMA, MDEA Schedule I Schedule I Schedule I PMA Schedule I Schedule I Schedule I DOB, DOM, 3,4,5-TMA Schedule I Schedule I Schedule I Methylphenidate Schedule II Schedule II Schedule I Chemical derivatives of substituted amphetamine
Standard Name Chemical Name # of Subs Amphetamine α-Methyl-2-phenylethylamine 0 Methamphetamine N-Methylamphetamine, (1R,2S)- 1 Ethylamphetamine N-Ethylamphetamine 1 Propylamphetamine N-Propylamphetamine 1 Isopropylamphetamine N-iso-Propylamphetamine 1 Phentermine α-Methylamphetamine 1 Phenylpropanolamine (PPA) β-Hydroxyamphetamine, (1R,2S)- 1 Cathine β-Hydroxyamphetamine, (1S,2S)- 1 Cathinone β-Ketoamphetamine 1 Ortetamine 2-Methylamphetamine 1 2-Fluoroamphetamine (2-FA) 2-Fluoroamphetamine 1 3-Methylamphetamine (3-MA) 3-Methylamphetamine 1 3-Fluoroamphetamine (3-FA) 3-Fluoroamphetamine 1 Norfenfluramine 3-Trifluoromethylamphetamine 1 4-Methylamphetamine (4-MA) 4-Methylamphetamine 1 para-Methoxyamphetamine (PMA) 4-Methoxyamphetamine 1 para-Ethoxyamphetamine 4-Ethoxyamphetamine 1 4-Methylthioamphetamine (4-MTA) 4-Methylthioamphetamine 1 Norpholedrine (α-Me-TRA) 4-Hydroxyamphetamine 1 para-Bromoamphetamine (PBA, 4-BA) 4-Bromoamphetamine 1 para-Chloroamphetamine (PCA, 4-CA) 4-Chloroamphetamine 1 para-Fluoroamphetamine (PFA, 4-FA, 4-FMP) 4-Fluoroamphetamine 1 para-Iodoamphetamine (PIA, 4-IA) 4-Iodoamphetamine 1 Dimethylamphetamine N,N-Dimethylamphetamine 2 Benzphetamine N-Benzyl-N-methylamphetamine 2 Selegiline N-Methyl-N-propargylamphetamine, (R)- 2 Mephentermine N-Methyl-α-methylamphetamine 2 Phenpentermine α,β-Dimethylamphetamine 2 Ephedrine (EPH) β-Hydroxy-N-methylamphetamine, (1R,2S)- 2 Pseudoephedrine (PSE) β-Hydroxy-N-methylamphetamine, (1S,2S)- 2 Methcathinone β-Keto-N-methylamphetamine 2 Ethcathinone β-Keto-N-ethylamphetamine 2 Clortermine 2-Chloro-α-methylamphetamine 2 Methoxymethylamphetamine (MMA) 3-Methoxy-4-methylamphetamine 2 Fenfluramine 3-Trifluoromethyl-N-ethylamphetamine 2 Dexfenfluramine 3-Trifluoromethyl-N-ethylamphetamine, (S)- 2 4-Methylmethamphetamine (4-MMA) 4-Methyl-N-methylamphetamine 2 Para-methoxymethamphetamine (PMMA) 4-Methoxy-N-methylamphetamine 2 para-Methoxyethylamphetamine (PMEA) 4-Methoxy-N-ethylamphetamine 2 Pholedrine 4-Hydroxy-N-methylamphetamine 2 Chlorphentermine 4-Chloro-α-methylamphetamine 2 para-Fluoromethamphetamine (PFMA, 4-FMA) 4-Fluoro-N-methylamphetamine 2 Xylopropamine 3,4-Dimethylamphetamine 2 α-Methyldopamine (α-Me-DA) 3,4-Dihydroxyamphetamine 2 Methylenedioxyamphetamine (MDA) 3,4-Methylenedioxyamphetamine 2 Dimethoxyamphetamine (DMA) X,X-Dimethoxyamphetamine 2 Nordefrin (α-Me-NE) β,3,4-Trihydroxyamphetamine, (R)- 3 Oxilofrine β,4-Dihydroxy-N-methylamphetamine 3 Aleph 2,5-dimethoxy-4-methylthioamphetamine 3 Dimethoxybromoamphetamine (DOB) 2,5-Dimethoxy-4-bromoamphetamine 3 Dimethoxychloroamphetamine (DOC) 2,5-Dimethoxy-4-chloroamphetamine 3 Dimethoxyfluoroethylamphetamine (DOEF) 2,5-Dimethoxy-4-fluoroethylamphetamine 3 Dimethoxyethylamphetamine (DOET) 2,5-Dimethoxy-4-ethylamphetamine 3 Dimethoxyfluoroamphetamine (DOF) 2,5-Dimethoxy-4-fluoroamphetamine 3 Dimethoxyiodoamphetamine (DOI) 2,5-Dimethoxy-4-iodoamphetamine 3 Dimethoxymethylamphetamine (DOM) 2,5-Dimethoxy-4-methylamphetamine 3 Dimethoxynitroamphetamine (DON) 2,5-Dimethoxy-4-nitroamphetamine 3 Dimethoxypropylamphetamine (DOPR) 2,5-Dimethoxy-4-propylamphetamine 3 Dimethoxytrifluoromethylamphetamine (DOTFM) 2,5-Dimethoxy-4-trifluoromethylamphetamine 3 Methylenedioxymethamphetamine (MDMA) 3,4-Methylenedioxy-N-methylamphetamine 3 Methylenedioxyethylamphetamine (MDEA) 3,4-Methylenedioxy-N-ethylamphetamine 3 Methylenedioxyhydroxyamphetamine (MDOH) 3,4-Methylenedioxy-N-hydroxyamphetamine 3 2-Methyl-MDA 3,4-Methylenedioxy-2-methylamphetamine 3 5-Methyl-MDA 4,5-Methylenedioxy-3-methylamphetamine 3 Methoxymethylenedioxyamphetamine (MMDA) 3-Methoxy-4,5-methylenedioxyamphetamine 3 Trimethoxyamphetamine (TMA) X,X,X-Trimethoxyamphetamine 3 Dimethylcathinone β-Keto-N,N-dimethylamphetamine 3 Diethylcathinone β-Keto-N,N-diethylamphetamine 3 Bupropion β-Keto-3-chloro-N-tert-butylamphetamine 3 Mephedrone (4-MMC) β-Keto-4-methyl-N-methylamphetamine 3 Methedrone (PMMC) β-Keto-4-methoxy-N-methylamphetamine 3 Brephedrone (4-BMC) β-Keto-4-bromo-N-methylamphetamine 3 Flephedrone (4-FMC) β-Keto-4-fluoro-N-methylamphetamine 3 Ganesha 2,5-Dimethoxy-3,4-dimethylamphetamine 4 Dimethoxymethylenedioxyamphetamine (DMMDA) 2,5-Dimethoxy-3,4-methylenedioxyamphetamine 4 FLEA (MDMHA) 3,4-Methylenedioxy-N-methyl-N-hydroxyamphetamine 4 Methoxymethylenedioxymethamphetamine (MMDMA) 3-Methoxy-4,5-methylenedioxy-N-methylamphetamine 4 EDMA (MDMC) 3,4-Ethylenedioxy-N-methylamphetamine 4 Ethylone (MDEC, bk-MDEA) β-Keto-3,4-methylenedioxy-N-ethylamphetamine 4 See also
References
- ^ Paul M Dewick (2002). Medicinal Natural Products. A Biosynthetic Approach. Second Edition. Wiley. pp. 383–384. ISBN 0471496405. http://books.google.com/?id=A4zptjOJfKQC&pg=PP1.
- ^ a b c Snow, p. 1
- ^ A. Richard Green et al. (2003). "The Pharmacology and Clinical Pharmacology of 3,4-Methylenedioxymethamphetamine (MDMA, "Ecstasy")". Pharmacological Reviews 55 (3): 463–508. doi:10.1124/pr.55.3.3. PMID 12869661.
- ^ a b Goldfrank, p. 1125
- ^ a b c d e Goldfrank, p. 1119
- ^ Liang Han Ling et al. (2001). "Poisoning with the recreational drug paramethoxyamphetamine ("death" )". The Medical Journal of Australia 174 (9): 453–5. PMID 11386590. http://www.mja.com.au/public/issues/174_09_070501/ling/ling.html.
- ^ Snow, p.71
- ^ a b c d e Goldfrank, p. 1121
- ^ Mithoefer M. et al. (2011). "The safety and efficacy of 3,4-methylenedioxymethamphetamine assisted psychotherapy in subjects with chronic, treatment-resistant posttraumatic stress disorder: the first randomized controlled pilot study". Journal of Psychopharmacology 25 (4): 439–52. doi:10.1177/0269881110378371. PMC 3122379. PMID 20643699. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=3122379.
- ^ Goldfrank, pp. 1125–1127
- ^ Glennon, pp. 184–187
- ^ a b Schatzberg, p.843
- ^ a b Glennon, p. 186
- ^ Glennon, pp. 181–189
- ^ Goldfrank, p. 1120
- ^ a b c d e f Goldfrank, p. 1122
- ^ a b Goldfrank, pp.215, 1121
- ^ a b c d Katzung, p.565
- ^ S. D. Robertson, H.J. Matthies and A. Galli (2009). "A closer look at amphetamine induced reverse transport and trafficking of the dopamine and norepinephrine transporters". Mol. Neurobiol. 2 (2): 73–80. doi:10.1007/s12035-009-8053-4. PMC 2729543. PMID 19199083. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2729543.
- ^ Glennon, p. 183
- ^ a b Glennon, p. 185
- ^ Schatzberg, p.844
- ^ Schatzberg, p.847
- ^ Maria S. Quinton and Bryan K. Yamamoto (2006). "Causes and Consequences of Methamphetamine and MDMA Toxicity". AAPS Journal 8 (2): E337–47. doi:10.1208/aapsj080238. PMID 16796384.
- ^ a b Katzung, p.559
- ^ Ghodse, p. 115
- ^ Katzung, p.556
- ^ Ghodse, pp. 114–115
- ^ Veselovskaya, p.53
- ^ Veselovskaya, p. 164
- ^ Veselovskaya, pp.59–60
- ^ Veselovskaya, p.60
- ^ a b A. Shulgin (1991). "PiHKaL: MDA". http://www.erowid.org/library/books_online/pihkal/pihkal100.shtml. Retrieved 2009-11-15.
- ^ A. Shulgin (1991). "PiHKaL: MDMA". http://www.erowid.org/library/books_online/pihkal/pihkal109.shtml. Retrieved 2009-11-15.
- ^ A. Shulgin (1991). "PiHKaL: DOM". http://www.erowid.org/library/books_online/pihkal/pihkal068.shtml. Retrieved 2009-11-21.
- ^ A. Shulgin (1991). "PiHKaL: DOB". http://www.erowid.org/library/books_online/pihkal/pihkal062.shtml. Retrieved 2009-11-21.
- ^ Finkel, Richard; Clark, Michelle A.; Cubeddu, Luigi X (2009). Lippincott's Illustrated Reviews: Pharmacology, 4th Edition. Lippincott Williams & Wilkins. p. 560. ISBN 0781771552. http://books.google.com/?id=Q4hG2gRhy7oC.
- ^ Goldfrank, pp. 1124–1125
- ^ Ghodes, pp.275–276
- ^ Richard K. Ries, Shannon Miller, David A Fiellin, Richard Saitz (2009-04-01). Principles of Addiction Medicine. Lippincott Williams & Wilkins. p. 712. ISBN 0781774772. http://books.google.com/?id=j6GGBud8DXcC&lpg=PA1&pg=PT741.
- ^ Malcolm Bruce (2000). "Managing amphetamine dependence". Advances in Psychiatric Treatment 6 (1): 33–40. doi:10.1192/apt.6.1.33. http://apt.rcpsych.org/cgi/reprint/6/1/33.pdf.
- ^ a b c Iván D. Montoya and Frank Vocci (2008). "Novel Medications to Treat Addictive Disorders". Curr Psychiatry Rep 10 (5): 392–8. doi:10.1007/s11920-008-0063-9. PMC 2610431. PMID 18803912. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2610431.
- ^ Ahmed Elkashef et al. (2008). "Pharmacotherapy of Methamphetamine Addiction: An Update". Subst Abuse 29 (3): 31–49. doi:10.1080/08897070802218554. PMC 2597382. PMID 19042205. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2597382.
- ^ Richard K. Ries, Shannon Miller, David A Fiellin, Richard Saitz (2009-04-01). Principles of Addiction Medicine. Lippincott Williams & Wilkins. pp. 712–713. ISBN 0781774772. http://books.google.com/?id=j6GGBud8DXcC&lpg=PA1&pg=PT741.
- ^ Goldfrank, pp. 1126–1127
- ^ a b AI Bragin (2002). "Acute intoxication with stimulant containing cathinone (based on transcultural studies)" (in ru). http://www.psychiatry.ua/articles/paper156.htm. Retrieved 2009-11-15.
- ^ TS Cantrell et al. (1988). "A Study of Impurities Found in Methamphetamine Synthesized From Ephedrine". Forensic Science International 39: 39–53. doi:10.1016/0379-0738(88)90116-8. http://www.erowid.org/archive/rhodium/chemistry/meth.impurities.html.
- ^ Andrew Allen and Thomas S. Cantrell (1989). "Synthetic Reductions in Clandestine Amphetamine and Methamphetamine Laboratories". Forensic Science International 42 (3): 183–199. doi:10.1016/0379-0738(89)90086-8. http://www.erowid.org/archive/rhodium/chemistry/amphetamine.reduction.html.
- ^ UNODC, p. 118
- ^ Ledgard, pp. 157–158
- ^ Ledgard, pp. 113, 125, 140, 146
- ^ Snow, p. 90
- ^ Snow, p. 127
- ^ Ledgard, pp. 131, 137
- ^ Ledgard, p. 124
- ^ CB Gairaud and G.R. Lappin (1953). "The Synthesis of beta-Nitrostyrenes". J. Org. Chem. 18: 1–3. doi:10.1021/jo01129a001. http://www.erowid.org/archive/rhodium/chemistry/nitrostyrenes.gairaud-lappin.html.
- ^ Gordon A. Alles (1932). "dl-beta-Phenylisopropylamines". J. Am. Chem. Soc. 54: 271–274. doi:10.1021/ja01340a040. http://www.erowid.org/archive/rhodium/chemistry/meth.alles.html.
- ^ Ledgard, pp. 122–123
- ^ UNODC, p. 115
- ^ "UN warns of growing synthetic drug abuse in Asia, Middle East". http://www.topnews.in/law/un-warns-growing-synthetic-drug-abuse-asia-middle-east. Retrieved 2009-11-17.
- ^ UNODC, p. 126
- ^ UNODC, pp. 116–117
- ^ UNODC, p. 146
- ^ UNODC, pp. 59, 112, 154
- ^ a b "Convention on Psychotropic Substances, 1971". http://www.incb.org/pdf/e/conv/convention_1971_en.pdf. Retrieved 2009-11-17.
- ^ "Список psychotropic substances under international control" (in ru). http://www.incb.org/pdf/e/list/green_ru.pdf. Retrieved 2009-11-17.
- ^ "DEA Drug Scheduling". http://www.justice.gov/dea/pubs/scheduling.html. Retrieved 2009-11-17.
- ^ "Resolution of RF Government of 30 June 1998 N 681 "On approval of list of drugs psychotropic substances and their precursors subject to control in the Russian Federation"" (in ru). http://base.garant.ru/12112176.htm. Retrieved 2009-11-15.
- ^ "US Controlled Substances Act (CSA) · Schedule II · Section (d) to (e): Stimulants to Depressants". http://isomerdesign.com/Cdsa/scheduleUS.php?schedule=2§ion=4&structure=C. Retrieved 2009-11-28.
Bibliography
- Hamid Ghodse (2002). Drugs and Addictive Behaviour. A Guide to Treatment. 3rd Edition. Cambridge University Press. pp. 501. ISBN 0511058446. http://books.google.com/?id=3WF79shLxB4C&lpg=PP1&pg=PP1.
- Richard A. Glennon (2008). The American Psychiatric Publishing textbook of substance abuse treatment. American Psychiatric Publishing. ISBN 978-1-58562-276-4. http://books.google.com/?id=6wdJgejlQzYC&lpg=PA181&pg=PA181.
- Lewis R. Goldfrank, Neal Flomenbaum (2006). Goldfrank's Toxicologic Emergencies, 8th Edition. McGraw Hill. ISBN 0071479147. http://books.google.com/?id=cvJuLqBxGUcC&lpg=PP1&pg=PP1.
- Bertram G. Katzung (2009). Basic & clinical pharmacology. 11th edition. McGraw-Hill Medical. ISBN 0071604057. http://books.google.com/?id=srRLpM5miGYC&lpg=PP1&pg=PP1.
- Jared Ledgard (2007). A Laboratory History of Narcotics. Volume 1. Amphetamines and Derivatives. Jared Ledgard. pp. 268. ISBN 0615156940.
- Alan F. Schatzberg, Charles B. Nemeroff (2009). The American Psychiatric Publishing Textbook of Psychopharmacology. The American Psychiatric Publishing. ISBN 9781585623099. http://books.google.com/?id=Xx7iNGdV25IC&pg=PP1.
- Otto Snow (2002). Amphetamine syntheses. Thoth Press. ISBN 096631283X.
- UNODC (2009). WDR_2009/WDR2009_eng_web.pdf World Drug Report 2009. United Nations. pp. 306. ISBN 9789211482409. http://www.unodc.org/documents/wdr/ WDR_2009/WDR2009_eng_web.pdf.
- Veselovskaya NV, Kovalenko AE (2000). Drugs. Properties, effects, pharmacokinetics, metabolism. MA: Triada-X. ISBN 9785944970299.
Stimulants (N06B) Adamantanes Adaphenoxate • Adapromine • Amantadine • Bromantane • Chlodantane • Gludantane • Memantine • Midantane
Adenosine antagonists 8-Chlorotheophylline • 8-Cyclopentyltheophylline • 8-Phenyltheophylline • Aminophylline • Caffeine • CGS-15943 • Dimethazan • Paraxanthine • SCH-58261 • Theobromine • TheophyllineAlkylamines Arylcyclohexylamines Benocyclidine • Dieticyclidine • Esketamine • Eticyclidine • Gacyclidine • Ketamine • Phencyclamine • Phencyclidine • Rolicyclidine • Tenocyclidine • Tiletamine
Benzazepines 6-Br-APB • SKF-77434 • SKF-81297 • SKF-82958
Cholinergics A-84543 • A-366,833 • ABT-202 • ABT-418 • AR-R17779 • Altinicline • Anabasine • Arecoline • Cotinine • Cytisine • Dianicline • Epibatidine • Epiboxidine • GTS-21 • Ispronicline • Nicotine • PHA-543,613 • PNU-120,596 • PNU-282,987 • Pozanicline • Rivanicline • Sazetidine A • SIB-1553A • SSR-180,711 • TC-1698 • TC-1827 • TC-2216 • TC-5619 • Tebanicline • UB-165 • Varenicline • WAY-317,538
Convulsants Anatoxin-a • Bicuculline • DMCM • Flurothyl • Gabazine • Pentetrazol • Picrotoxin • Strychnine • Thujone
Eugeroics Adrafinil • Armodafinil • CRL-40941 • Modafinil
Oxazolines 4-Methylaminorex • Aminorex • Clominorex • Cyclazodone • Fenozolone • Fluminorex • Pemoline • Thozalinone
Phenethylamines 1-(4-Methylphenyl)-2-aminobutane • 1-Phenyl-2-(piperidin-1-yl)pentan-3-one • 1-Methylamino-1-(3,4-methylenedioxyphenyl)propane • 2-Fluoroamphetamine • 2-Fluoromethamphetamine • 2-OH-PEA • 2-Phenyl-3-aminobutane • 2-Phenyl-3-methylaminobutane • 2,3-MDA • 3-Fluoroamphetamine • 3-Fluoroethamphetamine • 3-Fluoromethcathinone • 3-Methoxyamphetamine • 3-Methylamphetamine • 3,4-DMMC • 4-BMC • 4-Ethylamphetamine • 4-FA • 4-FMA • 4-MA • 4-MMA • 4-MTA • 6-FNE • Alfetamine • α-Ethylphenethylamine • Amfecloral • Amfepentorex • Amfepramone • Amidephrine • Amphetamine (Dextroamphetamine, Levoamphetamine) • Amphetaminil • Arbutamine • β-Methylphenethylamine • β-Phenylmethamphetamine • Benfluorex • Benzedrone • Benzphetamine • BDB (J) • BOH (Hydroxy-J) • BPAP • Buphedrone • Bupropion (Amfebutamone) • Butylone • Cathine • Cathinone • Chlorphentermine • Cinnamedrine • Clenbuterol • Clobenzorex • Cloforex • Clortermine • D-Deprenyl • Denopamine • Dimethoxyamphetamine • Dimethylamphetamine • Dimethylcathinone (Dimethylpropion, Metamfepramone) • Dobutamine • DOPA (Dextrodopa, Levodopa) • Dopamine • Dopexamine • Droxidopa • EBDB (Ethyl-J) • Ephedrine • Epinephrine (Adrenaline) • Epinine (Deoxyepinephrine) • Etafedrine • Ethcathinone (Ethylpropion) • Ethylamphetamine (Etilamfetamine) • Ethylnorepinephrine (Butanefrine) • Ethylone • Etilefrine • Famprofazone • Fenbutrazate • Fencamine • Fenethylline • Fenfluramine (Dexfenfluramine) • Fenmetramide • Fenproporex • Flephedrone • Fludorex • Furfenorex • Gepefrine • HMMA • Hordenine • Ibopamine • IMP • Indanylamphetamine • Isoetarine • Isoethcathinone • Isoprenaline (Isoproterenol) • L-Deprenyl (Selegiline) • Lefetamine • Lisdexamfetamine • Lophophine (Homomyristicylamine) • Manifaxine • MBDB (Methyl-J; "Eden") • MDA (Tenamfetamine) • MDBU • MDEA ("Eve") • MDMA ("Ecstasy", "Adam") • MDMPEA (Homarylamine) • MDOH • MDPR • MDPEA (Homopiperonylamine) • Mefenorex • Mephedrone • Mephentermine • Metanephrine • Metaraminol • Methamphetamine (Desoxyephedrine, Methedrine; Dextromethamphetamine, Levomethamphetamine) • Methoxamine • Methoxyphenamine • MMA • Methcathinone (Methylpropion) • Methedrone • Methoxyphenamine • Methylone • MMDA • MMDMA • MMMA • Morazone • N-Benzyl-1-phenethylamine • N,N-Dimethylphenethylamine • Naphthylamphetamine • Nisoxetine • Norepinephrine (Noradrenaline) • Norfenefrine • Norfenfluramine • Normetanephrine • Octopamine • Orciprenaline • Ortetamine • Oxilofrine • Paredrine (Norpholedrine, Oxamphetamine, Mycadrine) • PBA • PCA • PHA • Pargyline • Pentorex (Phenpentermine) • Pentylone • Phendimetrazine • Phenmetrazine • Phenpromethamine • Phentermine • Phenylalanine • Phenylephrine (Neosynephrine) • Phenylpropanolamine • Pholedrine • PIA • PMA • PMEA • PMMA • PPAP • Prenylamine • Propylamphetamine • Pseudoephedrine • Radafaxine • Ropinirole • Salbutamol (Albuterol; Levosalbutamol) • Sibutramine • Synephrine (Oxedrine) • Theodrenaline • Tiflorex (Flutiorex) • Tranylcypromine • Tyramine • Tyrosine • Xamoterol • Xylopropamine • Zylofuramine
Piperazines Piperidines 1-Benzyl-4-(2-(diphenylmethoxy)ethyl)piperidine • 1-(3,4-Dichlorophenyl)-1-(piperidin-2-yl)butane • 2-Benzylpiperidine • 2-Methyl-3-phenylpiperidine • 3,4-Dichloromethylphenidate • 4-Benzylpiperidine • 4-Methylmethylphenidate • Desoxypipradrol • Difemetorex • Diphenylpyraline • Ethylphenidate • Methylnaphthidate • Methylphenidate (Dexmethylphenidate) • N-Methyl-3β-propyl-4β-(4-chlorophenyl)piperidine • Nocaine • Phacetoperane • Pipradrol • SCH-5472
Pyrrolidines 2-Diphenylmethylpyrrolidine • α-PPP • α-PBP • α-PVP • Diphenylprolinol • MDPPP • MDPBP • MDPV • MPBP • MPHP • MPPP • MOPPP • Naphyrone • PEP • Prolintane • Pyrovalerone
Tropanes 3-CPMT • 3'-Chloro-3α-(diphenylmethoxy)tropane • 3-Pseudotropyl-4-fluorobenzoate • 4'-Fluorococaine • AHN-1055 • Altropane (IACFT) • Brasofensine • CFT (WIN 35,428) • β-CIT (RTI-55) • Cocaethylene • Cocaine • Dichloropane (RTI-111) • Difluoropine • FE-β-CPPIT • FP-β-CPPIT • Ioflupane (123I) • Norcocaine • PIT • PTT • RTI-31 • RTI-32 • RTI-51 • RTI-105 • RTI-112 • RTI-113 • RTI-117 • RTI-120 • RTI-121 (IPCIT) • RTI-126 • RTI-150 • RTI-154 • RTI-171 • RTI-177 • RTI-183 • RTI-193 • RTI-194 • RTI-199 • RTI-202 • RTI-204 • RTI-229 • RTI-241 • RTI-336 • RTI-354 • RTI-371 • RTI-386 • Salicylmethylecgonine • Tesofensine • Troparil (β-CPT, WIN 35,065-2) • Tropoxane • WF-23 • WF-33 • WF-60
Others 1-(Thiophen-2-yl)-2-aminopropane • 2-Amino-1,2-dihydronaphthalene • 2-Aminoindane • 2-Aminotetralin • 2-MDP • 2-Phenylcyclohexylamine • 2-Phenyl-3,6-dimethylmorpholine • 3-Benzhydrylmorpholine • 3,3-Diphenylcyclobutanamine • 5-(2-Aminopropyl)indole • 5-Iodo-2-aminoindane • AL-1095 • Amfonelic acid • Amineptine • Amiphenazole • Atipamezole • Atomoxetine (Tomoxetine) • Bemegride • Benzydamine • BTQ • BTS 74,398 • Carphedon • Ciclazindol • Cilobamine • Clofenciclan • Cropropamide • Crotetamide • Cypenamine • D-161 • Diclofensine • Dimethocaine • Efaroxan • Etamivan • EXP-561 • Fencamfamine • Fenpentadiol • Feprosidnine • G-130 • Gamfexine • Gilutensin • GSK1360707F • GYKI-52895 • Hexacyclonate • Idazoxan • Indanorex • Indatraline • JNJ-7925476 • JZ-IV-10 • Lazabemide • Leptacline • Levopropylhexedrine • Lomevactone • LR-5182 • Mazindol • Meclofenoxate • Medifoxamine • Mefexamide • Mesocarb • Methastyridone • Methiopropamine • N-Methyl-3-phenylnorbornan-2-amine • Nefopam • Nikethamide • Nomifensine • O-2172 • Oxaprotiline • Phthalimidopropiophenone • PNU-99,194 • Propylhexedrine • PRC200-SS • Rasagiline • Rauwolscine • Rubidium chloride • Setazindol • Tametraline • Tandamine • Trazium • UH-232 • Yohimbine
See also Sympathomimetic aminesEntactogens Aminoindanes Aminotetralins 6-CATPhenethylamines
(and amphetamines,
cathinones, etc)4-CAB • 4-FA • 4-FMA • 4-MTA • 4-FPP • 5-APDB • 6-APDB • Ariadne • BDB • Brephedrone • Eutylone • Flephedrone • IAP • IMP • Metaescaline • Mephedrone • Methedrone • MMA • NAP • Norfenfluramine • Pentylone • PMA • PMEA • PMMA • TAPMDxx 2-Methyl-MDA • 5-Methyl-MDA • 6-Methyl-MDA • bk-MBDB (butylone) • bk-MDEA (ethylone) • bk-MDMA (methylone) • DMMDA • DMMDA-2 • EBDB • EBDP • EDMA • MDAI • MDMAI • MMAI • MDAT • MDMAT • MDA • MDDM • MDEA • MDIP • MDMA • MDMOH • MDMP • MDMPEA • MDOH • MDPEA • MDPH • MDPR • MMDPEA (Lophophine) • MBDB • MBDP • MMDA • MMDA-2 • MMDMATryptamines Adrenergics Receptor ligands Agonists: 5-FNE • 6-FNE • Amidephrine • Anisodamine • Anisodine • Cirazoline • Dipivefrine • Dopamine • Ephedrine • Epinephrine (Adrenaline) • Etilefrine • Ethylnorepinephrine • Indanidine • Levonordefrin • Metaraminol • Methoxamine • Methyldopa • Midodrine • Naphazoline • Norepinephrine (Noradrenaline) • Octopamine • Oxymetazoline • Phenylephrine • Phenylpropanolamine • Pseudoephedrine • Synephrine • Tetrahydrozoline
Antagonists: Abanoquil • Adimolol • Ajmalicine • Alfuzosin • Amosulalol • Arotinolol • Atiprosin • Benoxathian • Buflomedil • Bunazosin • Carvedilol • CI-926 • Corynanthine • Dapiprazole • DL-017 • Domesticine • Doxazosin • Eugenodilol • Fenspiride • GYKI-12,743 • GYKI-16,084 • Indoramin • Ketanserin • L-765,314 • Labetalol • Mephendioxan • Metazosin • Monatepil • Moxisylyte (Thymoxamine) • Naftopidil • Nantenine • Neldazosin • Nicergoline • Niguldipine • Pelanserin • Phendioxan • Phenoxybenzamine • Phentolamine • Piperoxan • Prazosin • Quinazosin • Ritanserin • RS-97,078 • SGB-1,534 • Silodosin • SL-89.0591 • Spiperone • Talipexole • Tamsulosin • Terazosin • Tibalosin • Tiodazosin • Tipentosin • Tolazoline • Trimazosin • Upidosin • Urapidil • Zolertine
* Note that many TCAs, TeCAs, antipsychotics, ergolines, and some piperazines like buspirone, trazodone, nefazodone, etoperidone, and mepiprazole all antagonize α1-adrenergic receptors as well, which contributes to their side effects such as orthostatic hypotension.Agonists: (R)-3-Nitrobiphenyline • 4-NEMD • 6-FNE • Amitraz • Apraclonidine • Brimonidine • Cannabivarin • Clonidine • Detomidine • Dexmedetomidine • Dihydroergotamine • Dipivefrine • Dopamine • Ephedrine • Ergotamine • Epinephrine (Adrenaline) • Esproquin • Etilefrine • Ethylnorepinephrine • Guanabenz • Guanfacine • Guanoxabenz • Levonordefrin • Lofexidine • Medetomidine • Methyldopa • Mivazerol • Naphazoline • Norepinephrine (Noradrenaline) • Phenylpropanolamine • Piperoxan • Pseudoephedrine • Rilmenidine • Romifidine • Talipexole • Tetrahydrozoline • Tizanidine • Tolonidine • Urapidil • Xylazine • Xylometazoline
Antagonists: 1-PP • Adimolol • Aptazapine • Atipamezole • BRL-44408 • Buflomedil • Cirazoline • Efaroxan • Esmirtazapine • Fenmetozole • Fluparoxan • GYKI-12,743 • GYKI-16,084 • Idazoxan • Mianserin • Mirtazapine • MK-912 • NAN-190 • Olanzapine • Phentolamine • Phenoxybenzamine • Piperoxan • Piribedil • Rauwolscine • Rotigotine • SB-269,970 • Setiptiline • Spiroxatrine • Sunepitron • Tolazoline • Yohimbine
* Note that many atypical antipsychotics and azapirones like buspirone and gepirone (via metabolite 1-PP) antagonize α2-adrenergic receptors as well.βAgonists: 2-FNE • 5-FNE • Amibegron • Arbutamine • Arformoterol • Arotinolol • BAAM • Bambuterol • Befunolol • Bitolterol • Broxaterol • Buphenine • Carbuterol • Cimaterol • Clenbuterol • Denopamine • Deterenol • Dipivefrine • Dobutamine • Dopamine • Dopexamine • Ephedrine • Epinephrine (Adrenaline) • Etafedrine • Etilefrine • Ethylnorepinephrine • Fenoterol • Formoterol • Hexoprenaline • Higenamine • Indacaterol • Isoetarine • Isoprenaline (Isoproterenol) • Isoxsuprine • Labetalol • Levonordefrin • Levosalbutamol • Mabuterol • Methoxyphenamine • Methyldopa • Norepinephrine (Noradrenaline) • Orciprenaline • Oxyfedrine • Phenylpropanolamine • Pirbuterol • Prenalterol • Ractopamine • Procaterol • Pseudoephedrine • Reproterol • Rimiterol • Ritodrine • Salbutamol (Albuterol) • Salmeterol • Solabegron • Terbutaline • Tretoquinol • Tulobuterol • Xamoterol • Zilpaterol • Zinterol
Antagonists: Acebutolol • Adaprolol • Adimolol • Afurolol • Alprenolol • Alprenoxime • Amosulalol • Ancarolol • Arnolol • Arotinolol • Atenolol • Befunolol • Betaxolol • Bevantolol • Bisoprolol • Bopindolol • Bormetolol • Bornaprolol • Brefonalol • Bucindolol • Bucumolol • Bufetolol • Buftiralol • Bufuralol • Bunitrolol • Bunolol • Bupranolol • Burocrolol • Butaxamine • Butidrine • Butofilolol • Capsinolol • Carazolol • Carpindolol • Carteolol • Carvedilol • Celiprolol • Cetamolol • Cicloprolol • Cinamolol • Cloranolol • Cyanopindolol • Dalbraminol • Dexpropranolol • Diacetolol • Dichloroisoprenaline • Dihydroalprenolol • Dilevalol • Diprafenone • Draquinolol • Dropranolol • Ecastolol • Epanolol • Ericolol • Ersentilide • Esatenolol • Esmolol • Esprolol • Eugenodilol • Exaprolol • Falintolol • Flestolol • Flusoxolol • Hydroxycarteolol • Hydroxytertatolol • ICI-118,551 • Idropranolol • Indenolol • Indopanolol • Iodocyanopindolol • Iprocrolol • Isoxaprolol • Isamoltane • Labetalol • Landiolol • Levobetaxolol • Levobunolol • Levocicloprolol • Levomoprolol • Medroxalol • Mepindolol • Metalol • Metipranolol • Metoprolol • Moprolol • Nadolol • Nadoxolol • Nafetolol • Nebivolol • Neraminol • Nifenalol • Nipradilol • Oberadilol • Oxprenolol • Pacrinolol • Pafenolol • Pamatolol • Pargolol • Parodilol • Penbutolol • Penirolol • PhQA-33 • Pindolol • Pirepolol • Practolol • Primidolol • Procinolol • Pronethalol • Propafenone • Propranolol • Ridazolol • Ronactolol • Soquinolol • Sotalol • Spirendolol • SR 59230A • Sulfinalol • TA-2005 • Talinolol • Tazolol • Teoprolol • Tertatolol • Terthianolol • Tienoxolol • Tilisolol • Timolol • Tiprenolol • Tolamolol • Toliprolol • Tribendilol • Trigevolol • Xibenolol • XipranololReuptake inhibitors Selective norepinephrine reuptake inhibitors: Amedalin • Atomoxetine (Tomoxetine) • Ciclazindol • Daledalin • Esreboxetine • Lortalamine • Mazindol • Nisoxetine • Reboxetine • Talopram • Talsupram • Tandamine • Viloxazine; Norepinephrine-dopamine reuptake inhibitors: Amineptine • Bupropion (Amfebutamone) • Fencamine • Fencamfamine • Lefetamine • Levophacetoperane • LR-5182 • Manifaxine • Methylphenidate • Nomifensine • O-2172 • Radafaxine; Serotonin-norepinephrine reuptake inhibitors: Bicifadine • Desvenlafaxine • Duloxetine • Eclanamine • Levomilnacipran • Milnacipran • Sibutramine • Venlafaxine; Serotonin-norepinephrine-dopamine reuptake inhibitors: Brasofensine • Diclofensine • DOV-102,677 • DOV-21,947 • DOV-216,303 • JNJ-7925476 • JZ-IV-10 • Methylnaphthidate • Naphyrone • NS-2359 • PRC200-SS • SEP-225,289 • SEP-227,162 • Tesofensine; Tricyclic antidepressants: Amitriptyline • Butriptyline • Cianopramine • Clomipramine • Desipramine • Dosulepin • Doxepin • Imipramine • Lofepramine • melitracen • Nortriptyline • Protriptyline • Trimipramine; Tetracyclic antidepressants: Amoxapine • Maprotiline • Mianserin • Oxaprotiline • Setiptiline; Others: Cocaine • CP-39,332 • EXP-561 • Fezolamine • Ginkgo biloba • Indeloxazine • Nefazodone • Nefopam • Pridefrine • Tapentadol • Teniloxazine • Tramadol • ZiprasidoneReleasing agents Morpholines: Fenbutrazate • Morazone • Phendimetrazine • Phenmetrazine; Oxazolines: 4-Methylaminorex • Aminorex • Clominorex • Cyclazodone • Fenozolone • Fluminorex • Pemoline • Thozalinone; Phenethylamines (also amphetamines, cathinones, phentermines, etc): 2-OH-PEA • 4-CAB • 4-FA • 4-FMA • 4-MA • 4-MMA • Alfetamine • Amfecloral • Amfepentorex • Amfepramone • Amphetamine (Dextroamphetamine, Levoamphetamine) • Amphetaminil • β-Me-PEA • BDB • Benzphetamine • BOH • Buphedrone • Butylone • Cathine • Cathinone • Clobenzorex • Clortermine • D-Deprenyl • Dimethylamphetamine • Dimethylcathinone (Dimethylpropion, metamfepramone) • DMA • DMMA • EBDB • Ephedrine • Ethcathinone • Ethylamphetamine • Ethylone • Famprofazone • Fenethylline • Fenproporex • Flephedrone • Fludorex • Furfenorex • Hordenine • IAP • IMP • L-Deprenyl (Selegiline) • Lisdexamfetamine • Lophophine • MBDB • MDA (Tenamfetamine) • MDEA • MDMA • MDMPEA • MDOH • MDPEA • Mefenorex • Mephedrone • Mephentermine • Methamphetamine (Dextromethamphetamine, Levomethamphetamine) • Methcathinone • Methedrone • Methylone • NAP • Ortetamine • Paredrine • pBA • pCA • Pentorex (Phenpentermine) • Phenethylamine • Pholedrine • Phenpromethamine • Phentermine • Phenylpropanolamine • pIA • Prenylamine • Propylamphetamine • Pseudoephedrine • Tiflorex • Tyramine • Xylopropamine • Zylofuramine; Piperazines: 2C-B-BZP • BZP • MBZP • mCPP • MDBZP • MeOPP • pFPP; Others: 2-Amino-1,2-dihydronaphthalene • 2-Aminoindane • 2-Aminotetralin • 2-Benzylpiperidine • 4-Benzylpiperidine • 5-IAI • Clofenciclan • Cyclopentamine • Cypenamine • Cyprodenate • Feprosidnine • Gilutensin • Heptaminol • Hexacyclonate • Indanorex • Isometheptene • Methylhexanamine • Octodrine • Phthalimidopropiophenone • Propylhexedrine (Levopropylhexedrine) • TuaminoheptaneEnzyme inhibitors 3,4-DihydroxystyreneDBHCGS-19281A • SKF-64139 • SKF-7698Nonselective: Benmoxin • Caroxazone • Echinopsidine • Furazolidone • Hydralazine • Indantadol • Iproclozide • Iproniazid • Isocarboxazid • Isoniazid • Linezolid • Mebanazine • Metfendrazine • Nialamide • Octamoxin • Paraxazone • Phenelzine • Pheniprazine • Phenoxypropazine • Pivalylbenzhydrazine • Procarbazine • Safrazine • Tranylcypromine; MAO-A selective: Amiflamine • Bazinaprine • Befloxatone • Befol • Brofaromine • Cimoxatone • Clorgiline • Esuprone • Harmala alkaloids (Harmine, Harmaline, Tetrahydroharmine, Harman, Norharman, etc) • Methylene Blue • Metralindole • Minaprine • Moclobemide • Pirlindole • Sercloremine • Tetrindole • Toloxatone • Tyrima; MAO-B selective: D-Deprenyl • Selegiline (L-Deprenyl) • Ladostigil • Lazabemide • Milacemide • Mofegiline • Pargyline • Rasagiline • Safinamide
* Note that MAO-B inhibitors also influence norepinephrine/epinephrine levels since they inhibit the breakdown of their precursor dopamine.COMTOthers Ferrous Iron (Fe2+) • S-Adenosyl-L-Methionine • Vitamin B3 (Niacin, Nicotinamide → NADPH) • Vitamin B6 (Pyridoxine, Pyridoxamine, Pyridoxal → Pyridoxal Phosphate) • Vitamin B9 (Folic acid → Tetrahydrofolic acid) • Vitamin C (Ascorbic acid) • Zinc (Zn2+)OthersActivity enhancers: BPAP • PPAP; Release blockers: Bethanidine • Bretylium • Guanadrel • Guanazodine • Guanclofine • Guanethidine • Guanoxan; Toxins: Oxidopamine (6-Hydroxydopamine)List of adrenergic drugsDopaminergics Receptor ligands AgonistsAdamantanes: Amantadine • Memantine • Rimantadine; Aminotetralins: 7-OH-DPAT • 8-OH-PBZI • Rotigotine • UH-232; Benzazepines: 6-Br-APB • Fenoldopam • SKF-38,393 • SKF-77,434 • SKF-81,297 • SKF-82,958 • SKF-83,959; Ergolines: Bromocriptine • Cabergoline • Dihydroergocryptine • Lisuride • LSD • Pergolide; Dihydrexidine derivatives: 2-OH-NPA • A-86,929 • Ciladopa • Dihydrexidine • Dinapsoline • Dinoxyline • Doxanthrine; Others: A-68,930 • A-77,636 • A-412,997 • ABT-670 • ABT-724 • Aplindore • Apomorphine • Aripiprazole • Bifeprunox • BP-897 • CY-208,243 • Dizocilpine • Etilevodopa • Flibanserin • Ketamine • Melevodopa • Modafinil • Pardoprunox • Phencyclidine • PD-128,907 • PD-168,077 • PF-219,061 • Piribedil • Pramipexole • Propylnorapomorphine • Pukateine • Quinagolide • Quinelorane • Quinpirole • RDS-127 • Ro10-5824 • Ropinirole • Rotigotine • Roxindole • Salvinorin A • SKF-89,145 • Sumanirole • Terguride • Umespirone • WAY-100,635AntagonistsTypical antipsychotics: Acepromazine • Azaperone • Benperidol • Bromperidol • Clopenthixol • Chlorpromazine • Chlorprothixene • Droperidol • Flupentixol • Fluphenazine • Fluspirilene • Haloperidol • Loxapine • Mesoridazine • Methotrimeprazine • Nemonapride • Penfluridol • Perazine • Periciazine • Perphenazine • Pimozide • Prochlorperazine • Promazine • Sulforidazine • Sulpiride • Sultopride • Thioridazine • Thiothixene • Trifluoperazine • Triflupromazine • Trifluperidol • Zuclopenthixol; Atypical antipsychotics: Amisulpride • Asenapine • Blonanserin • Cariprazine • Carpipramine • Clocapramine • Clozapine • Gevotroline • Iloperidone • Lurasidone • Melperone • Molindone • Mosapramine • Olanzapine • Paliperidone • Perospirone • Piquindone • Quetiapine • Remoxipride • Risperidone • Sertindole • Tiospirone • Ziprasidone • Zotepine; Antiemetics: AS-8112 • Alizapride • Bromopride • Clebopride • Domperidone • Metoclopramide • Thiethylperazine; Others: Amoxapine • Buspirone • Butaclamol • Ecopipam • EEDQ • Eticlopride • Fananserin • L-745,870 • Nafadotride • Nuciferine • PNU-99,194 • Raclopride • Sarizotan • SB-277,011-A • SCH-23,390 • SKF-83,959 • Sonepiprazole • Spiperone • Spiroxatrine • Stepholidine • Tetrahydropalmatine • Tiapride • UH-232 • YohimbineReuptake inhibitors PlasmalemmalDAT inhibitorsPiperazines: DBL-583 • GBR-12,935 • Nefazodone • Vanoxerine; Piperidines: BTCP • Desoxypipradrol • Dextromethylphenidate • Difemetorex • Ethylphenidate • Methylnaphthidate • Methylphenidate • Phencyclidine • Pipradrol; Pyrrolidines: Diphenylprolinol • Methylenedioxypyrovalerone (MDPV) • Naphyrone • Prolintane • Pyrovalerone; Tropanes: β-CPPIT • Altropane • Brasofensine • CFT • Cocaine • Dichloropane • Difluoropine • FE-β-CPPIT • FP-β-CPPIT • Ioflupane (123I) • Iometopane • RTI-112 • RTI-113 • RTI-121 • RTI-126 • RTI-150 • RTI-177 • RTI-229 • RTI-336 • Tenocyclidine • Tesofensine • Troparil • Tropoxane • WF-11 • WF-23 • WF-31 • WF-33; Others: Adrafinil • Armodafinil • Amfonelic acid • Amineptine • Benzatropine (Benztropine) • Bromantane • BTQ • BTS-74,398 • Bupropion (Amfebutamone) • Ciclazindol • Diclofensine • Dimethocaine • Diphenylpyraline • Dizocilpine • DOV-102,677 • DOV-21,947 • DOV-216,303 • Etybenzatropine (Ethylbenztropine) • EXP-561 • Fencamine • Fencamfamine • Fezolamine • GYKI-52,895 • Indatraline • Ketamine • Lefetamine • Levophacetoperane • LR-5182 • Manifaxine • Mazindol • Medifoxamine • Mesocarb • Modafinil • Nefopam • Nomifensine • NS-2359 • O-2172 • Pridefrine • Propylamphetamine • Radafaxine • SEP-225,289 • SEP-227,162 • Sertraline • Sibutramine • Tametraline • TripelennamineVMAT inhibitorsReleasing agents Morpholines: Fenbutrazate • Morazone • Phendimetrazine • Phenmetrazine; Oxazolines: 4-Methylaminorex (4-MAR, 4-MAX) • Aminorex • Clominorex • Cyclazodone • Fenozolone • Fluminorex • Pemoline • Thozalinone; Phenethylamines (also amphetamines, cathinones, phentermines, etc): 2-Hydroxyphenethylamine (2-OH-PEA) • 4-CAB • 4-Methylamphetamine (4-MA) • 4-Methylmethamphetamine (4-MMA) • Alfetamine • Amfecloral • Amfepentorex • Amfepramone • Amphetamine (Dextroamphetamine, Levoamphetamine) • Amphetaminil • β-Methylphenethylamine (β-Me-PEA) • Benzodioxolylbutanamine (BDB) • Benzodioxolylhydroxybutanamine (BOH) • Benzphetamine • Buphedrone • Butylone • Cathine • Cathinone • Clobenzorex • Clortermine • D-Deprenyl • Dimethoxyamphetamine (DMA) • Dimethoxymethamphetamine (DMMA) • Dimethylamphetamine • Dimethylcathinone (Dimethylpropion, metamfepramone) • Ethcathinone (Ethylpropion) • Ethylamphetamine • Ethylbenzodioxolylbutanamine (EBDB) • Ethylone • Famprofazone • Fenethylline • Fenproporex • Flephedrone • Fludorex • Furfenorex • Hordenine • Lophophine (Homomyristicylamine) • Mefenorex • Mephedrone • Methamphetamine (Desoxyephedrine, Methedrine; Dextromethamphetamine, Levomethamphetamine) • Methcathinone (Methylpropion) • Methedrone • Methoxymethylenedioxyamphetamine (MMDA) • Methoxymethylenedioxymethamphetamine (MMDMA) • Methylbenzodioxolylbutanamine (MBDB) • Methylenedioxyamphetamine (MDA, tenamfetamine) • Methylenedioxyethylamphetamine (MDEA) • Methylenedioxyhydroxyamphetamine (MDOH) • Methylenedioxymethamphetamine (MDMA) • Methylenedioxymethylphenethylamine (MDMPEA, homarylamine) • Methylenedioxyphenethylamine (MDPEA, homopiperonylamine) • Methylone • Ortetamine • Parabromoamphetamine (PBA) • Parachloroamphetamine (PCA) • Parafluoroamphetamine (PFA) • Parafluoromethamphetamine (PFMA) • Parahydroxyamphetamine (PHA) • Paraiodoamphetamine (PIA) • Paredrine (Norpholedrine, Oxamphetamine) • Phenethylamine (PEA) • Pholedrine • Phenpromethamine • Prenylamine • Propylamphetamine • Tiflorex (Flutiorex) • Tyramine (TRA) • Xylopropamine • Zylofuramine; Piperazines: 2,5-Dimethoxy-4-bromobenzylpiperazine (2C-B-BZP) • Benzylpiperazine (BZP) • Methoxyphenylpiperazine (MeOPP, paraperazine) • Methylbenzylpiperazine (MBZP) • Methylenedioxybenzylpiperazine (MDBZP, piperonylpiperazine); Others: 2-Amino-1,2-dihydronaphthalene (2-ADN) • 2-Aminoindane (2-AI) • 2-Aminotetralin (2-AT) • 4-Benzylpiperidine (4-BP) • 5-IAI • Clofenciclan • Cyclopentamine • Cypenamine • Cyprodenate • Feprosidnine • Gilutensin • Heptaminol • Hexacyclonate • Indanylaminopropane (IAP) • Indanorex • Isometheptene • Methylhexanamine • Naphthylaminopropane (NAP) • Octodrine • Phthalimidopropiophenone • Propylhexedrine (Levopropylhexedrine) • Tuaminoheptane (Tuamine)Enzyme inhibitors PAH inhibitors3,4-DihydroxystyreneTH inhibitorsNonselective: Benmoxin • Caroxazone • Echinopsidine • Furazolidone • Hydralazine • Indantadol • Iproclozide • Iproniazid • Isocarboxazid • Isoniazid • Linezolid • Mebanazine • Metfendrazine • Nialamide • Octamoxin • Paraxazone • Phenelzine • Pheniprazine • Phenoxypropazine • Pivalylbenzhydrazine • Procarbazine • Safrazine • Tranylcypromine; MAO-A selective: Amiflamine • Bazinaprine • Befloxatone • Befol • Brofaromine • Cimoxatone • Clorgiline • Esuprone • Harmala alkaloids • Methylene Blue • Metralindole • Minaprine • Moclobemide • Pirlindole • Sercloremine • Tetrindole • Toloxatone • Tyrima; MAO-B selective: D-Deprenyl • L-Deprenyl (Selegiline) • Ladostigil • Lazabemide • Milacemide • Pargyline • Rasagiline • SafinamideDBH inhibitorsOthers Ferrous iron (Fe2+) • Tetrahydrobiopterin • Vitamin B3 (Niacin, Nicotinamide → NADPH) • Vitamin B6 (Pyridoxine, Pyridoxamine, Pyridoxal → Pyridoxal phosphate) • Vitamin B9 (Folic acid → Tetrahydrofolic acid) • Vitamin C (Ascorbic acid) • Zinc (Zn2+)OthersActivity enhancers: Benzofuranylpropylaminopentane (BPAP) • Phenylpropylaminopentane (PPAP); Toxins: Oxidopamine (6-Hydroxydopamine)List of dopaminergic drugsSerotonergics 5-HT1 receptor ligands Agonists: Azapirones: Alnespirone • Binospirone • Buspirone • Enilospirone • Eptapirone • Gepirone • Ipsapirone • Perospirone • Revospirone • Tandospirone • Tiospirone • Umespirone • Zalospirone; Antidepressants: Etoperidone • Nefazodone • Trazodone • Vortioxetine; Antipsychotics: Aripiprazole • Asenapine • Clozapine • Quetiapine • Ziprasidone; Ergolines: Dihydroergotamine • Ergotamine • Lisuride • Methysergide • LSD; Tryptamines: 5-CT • 5-MeO-DMT • 5-MT • Bufotenin • DMT • Indorenate • Psilocin • Psilocybin; Others: 8-OH-DPAT • Adatanserin • Befiradol • BMY-14802 • Cannabidiol • Dimemebfe • Ebalzotan • Eltoprazine • F-11,461 • F-12,826 • F-13,714 • F-14,679 • F-15,063 • F-15,599 • Flesinoxan • Flibanserin • Lesopitron • LY-293,284 • LY-301,317 • MKC-242 • NBUMP • Osemozotan • Oxaflozane • Pardoprunox • Piclozotan • Rauwolscine • Repinotan • Roxindole • RU-24,969 • S 14,506 • S-14,671 • S-15,535 • Sarizotan • SSR-181,507 • Sunepitron • U-92,016-A • Urapidil • Vilazodone • Xaliproden • Yohimbine
Antagonists: Antipsychotics: Iloperidone • Risperidone • Sertindole; Beta blockers: Alprenolol • Cyanopindolol • Iodocyanopindolol • Oxprenolol • Pindobind • Pindolol • Propranolol • Tertatolol; Others: AV965 • BMY-7,378 • CSP-2503 • Dotarizine • Flopropione • GR-46611 • Isamoltane • Lecozotan • Mefway • Metitepine/Methiothepin • MPPF • NAN-190 • PRX-00023 • Robalzotan • S-15535 • SB-649,915 • SDZ 216-525 • Spiperone • Spiramide • Spiroxatrine • UH-301 • WAY-100,135 • WAY-100,635 • XylamidineAgonists: Lysergamides: Dihydroergotamine • Ergotamine • Methysergide; Piperazines: Eltoprazine • TFMPP; Triptans: Avitriptan • Eletriptan • Sumatriptan • Zolmitriptan; Tryptamines: 5-CT • 5-MT; Others: CGS-12066A • CP-93,129 • CP-94,253 • CP-135,807 • RU-24,969
Antagonists: Lysergamides: Metergoline; Others: AR-A000002 • Elzasonan • GR-127,935 • Isamoltane • Metitepine/Methiothepin • SB-216,641 • SB-224,289 • SB-236,057 • YohimbineAgonists: Lysergamides: Dihydroergotamine • Methysergide; Triptans: Almotriptan • Avitriptan • Eletriptan • Frovatriptan • Naratriptan • Rizatriptan • Sumatriptan • Zolmitriptan; Tryptamines: 5-CT • 5-Ethyl-DMT • 5-MT • 5-(Nonyloxy)tryptamine; Others: CP-135,807 • CP-286,601 • GR-46611 • L-694,247 • L-772,405 • PNU-109,291 • PNU-142,633
Antagonists: Lysergamides: Metergoline; Others: Alniditan • BRL-15,572 • Elzasonan • GR-127,935 • Ketanserin • LY-310,762 • LY-367,642 • LY-456,219 • LY-456,220 • Metitepine/Methiothepin • Ritanserin • Yohimbine • ZiprasidoneAgonists: Lysergamides: Methysergide; Triptans: Eletriptan; Tryptamines: BRL-54443 • Tryptamine
Antagonists: Metitepine/MethiothepinAgonists: Triptans: Eletriptan • Naratriptan • Sumatriptan; Tryptamines: 5-MT; Others: BRL-54443 • Lasmiditan • LY-334,370
Antagonists: Metitepine/Methiothepin5-HT2 receptor ligands Agonists: Lysergamides: ALD-52 • Ergometrine • Lisuride • LA-SS-Az • LSD • LSD-Pip • Lysergic acid 2-butyl amide • Lysergic acid 3-pentyl amide • Methysergide; Phenethylamines: 25I-NBF • 25I-NBMD • 25I-NBOH • 25I-NBOMe • 2C-B • 2C-B-FLY • 2CB-Ind • 2C-C-NBOMe • 2C-E • 2C-I • 2C-TFM-NBOMe • 2C-T-2 • 2C-T-7 • 2C-T-21 • 2CBCB-NBOMe • 2CBFly-NBOMe • Bromo-DragonFLY • DOB • DOC • DOI • DOM • MDA • MDMA • Mescaline • TCB-2 • TFMFly; Piperazines: BZP • Quipazine • TFMPP; Tryptamines: 5-CT • 5-MeO-α-ET • 5-MeO-α-MT • 5-MeO-DET • 5-MeO-DiPT • 5-MeO-DMT • 5-MeO-DPT • 5-MT • α-ET • α-Methyl-5-HT • α-MT • Bufotenin • DET • DiPT • DMT • DPT • Psilocin • Psilocybin; Others: AL-34662 • AL-37350A • Dimemebfe • Medifoxamine • Oxaflozane • PNU-22394 • RH-34
Antagonists: Atypical antipsychotics: Amperozide • Aripiprazole • Carpipramine • Clocapramine • Clozapine • Gevotroline • Iloperidone • Melperone • Mosapramine • Olanzapine • Paliperidone • Pimozide • Quetiapine • Risperidone • Sertindole • Ziprasidone • Zotepine; Typical antipsychotics: Loxapine • Pipamperone; Antidepressants: Amitriptyline • Amoxapine • Aptazapine • Etoperidone • Mianserin • Mirtazapine • Nefazodone • Teniloxazine • Trazodone; Others: 5-I-R91150 • AC-90179 • Adatanserin • Altanserin • AMDA • APD-215 • Blonanserin • Cinanserin • CSP-2503 • Cyproheptadine • Deramciclane • Dotarizine • Eplivanserin • Esmirtazapine • Fananserin • Flibanserin • Ketanserin • KML-010 • Lubazodone • Mepiprazole • Metitepine/Methiothepin • Nantenine • Pimavanserin • Pizotifen • Pruvanserin • Rauwolscine • Ritanserin • S-14,671 • Sarpogrelate • Setoperone • Spiperone • Spiramide • SR-46349B • Volinanserin • Xylamidine • YohimbineAgonists: Oxazolines: 4-Methylaminorex • Aminorex; Phenethylamines: Chlorphentermine • Cloforex • DOB • DOC • DOI • DOM • Fenfluramine • MDA • MDMA • Norfenfluramine; Tryptamines: 5-CT • 5-MT • α-Methyl-5-HT; Others: BW-723C86 • Cabergoline • mCPP • Pergolide • PNU-22394 • Ro60-0175
Antagonists: Agomelatine • Asenapine • EGIS-7625 • Ketanserin • Lisuride • LY-272,015 • Metitepine/Methiothepin • PRX-08066 • Rauwolscine • Ritanserin • RS-127,445 • Sarpogrelate • SB-200,646 • SB-204,741 • SB-206,553 • SB-215,505 • SB-221,284 • SB-228,357 • SDZ SER-082 • Tegaserod • YohimbineAgonists: Phenethylamines: 2C-B • 2C-E • 2C-I • 2C-T-2 • 2C-T-7 • 2C-T-21 • DOB • DOC • DOI • DOM • MDA • MDMA • Mescaline; Piperazines: Aripiprazole • mCPP • TFMPP; Tryptamines: 5-CT • 5-MeO-α-ET • 5-MeO-α-MT • 5-MeO-DET • 5-MeO-DiPT • 5-MeO-DMT • 5-MeO-DPT • 5-MT • α-ET • α-Methyl-5-HT • α-MT • Bufotenin • DET • DiPT • DMT • DPT • Psilocin • Psilocybin; Others: A-372,159 • AL-38022A • CP-809,101 • Dimemebfe • Lorcaserin• Medifoxamine • MK-212 • Org 12,962 • ORG-37,684 • Oxaflozane • PNU-22394 • Ro60-0175 • Ro60-0213 • Vabicaserin • WAY-629 • WAY-161,503 • YM-348
Antagonists: Atypical antipsychotics: Clozapine • Iloperidone • Melperone • Olanzapine • Paliperidone • Pimozide • Quetiapine • Risperidone • Sertindole • Ziprasidone • Zotepine; Typical antipsychotics: Chlorpromazine • Loxapine • Pipamperone; Antidepressants: Agomelatine • Amitriptyline • Amoxapine • Aptazapine • Etoperidone • Fluoxetine • Mianserin • Mirtazapine • Nefazodone • Nortriptyline • Tedatioxetine • Trazodone; Others: Adatanserin • Cinanserin • Cyproheptadine • Deramciclane • Dotarizine • Eltoprazine • Esmirtazapine • FR-260,010 • Ketanserin • Ketotifen • Latrepirdine • Metitepine/Methiothepin • Methysergide • Pizotifen • Ritanserin • RS-102,221 • S-14,671 • SB-200,646 • SB-206,553 • SB-221,284 • SB-228,357 • SB-242,084 • SB-243,213 • SDZ SER-082 • Xylamidine5-HT3, 5-HT4, 5-HT5, 5-HT6, 5-HT7 ligands Agonists: Piperazines: BZP • Quipazine; Tryptamines: 2-Methyl-5-HT • 5-CT; Others: Chlorophenylbiguanide • Butanol • Ethanol • Halothane • Isoflurane • RS-56812 • SR-57,227 • SR-57,227-A • Toluene • Trichloroethane • Trichloroethanol • Trichloroethylene • YM-31636
Antagonists: Antiemetics: AS-8112 • Alosetron • Azasetron • Batanopride • Bemesetron • Cilansetron • Dazopride • Dolasetron • Granisetron • Lerisetron • Ondansetron • Palonosetron • Ramosetron • Renzapride • Tropisetron • Zacopride • Zatosetron; Atypical antipsychotics: Clozapine • Olanzapine • Quetiapine; Tetracyclic antidepressants: Amoxapine • Mianserin • Mirtazapine; Others: CSP-2503 • ICS-205,930 • MDL-72,222 • Memantine • Nitrous Oxide • Ricasetron • Sevoflurane • Tedatioxetine • Thujone • Vortioxetine • XenonAgonists: Gastroprokinetic Agents: Cinitapride • Cisapride • Dazopride • Metoclopramide • Mosapride • Prucalopride • Renzapride • Tegaserod • Velusetrag • Zacopride; Others: 5-MT • BIMU8 • CJ-033,466 • PRX-03140 • RS-67333 • RS-67506 • SL65.0155 • Antagonists: GR-113,808 • GR-125,487 • L-Lysine • Piboserod • RS-39604 • RS-67532 • SB-203,186 • SB-204,070Agonists: Lysergamides: Ergotamine • LSD; Tryptamines: 5-CT; Others: Valerenic Acid
Antagonists: Asenapine • Latrepirdine • Metitepine/Methiothepin • Ritanserin • SB-699,551
* Note that the 5-HT5B receptor is not functional in humans.Agonists: Lysergamides: Dihydroergotamine • Ergotamine • Lisuride • LSD • Mesulergine • Metergoline • Methysergide; Tryptamines: 2-Methyl-5-HT • 5-BT • 5-CT • 5-MT • Bufotenin • E-6801 • E-6837 • EMD-386,088 • EMDT • LY-586,713 • Tryptamine; Others: WAY-181,187 • WAY-208,466
Antagonists: Antidepressants: Amitriptyline • Amoxapine • Clomipramine • Doxepin • Mianserin • Nortriptyline; Atypical antipsychotics: Aripiprazole • Asenapine • Clozapine • Fluperlapine • Iloperidone • Olanzapine • Tiospirone; Typical antipsychotics: Chlorpromazine • Loxapine; Others: BGC20-760 • BVT-5182 • BVT-74316 • Cerlapirdine • EGIS-12,233 • GW-742,457 • Ketanserin • Latrepirdine • Lu AE58054 • Metitepine/Methiothepin • MS-245 • PRX-07034 • Ritanserin • Ro04-6790 • Ro 63-0563 • SB-258,585 • SB-271,046 • SB-357,134 • SB-399,885 • SB-742,457Agonists: Lysergamides: LSD; Tryptamines: 5-CT • 5-MT • Bufotenin; Others: 8-OH-DPAT • AS-19 • Bifeprunox • E-55888 • LP-12 • LP-44 • RU-24,969 • Sarizotan
Antagonists: Lysergamides: 2-Bromo-LSD • Bromocriptine • Dihydroergotamine • Ergotamine • Mesulergine • Metergoline • Methysergide; Antidepressants: Amitriptyline • Amoxapine • Clomipramine • Imipramine • Maprotiline • Mianserin; Atypical antipsychotics: Amisulpride • Aripiprazole • Clozapine • Olanzapine • Risperidone • Sertindole • Tiospirone • Ziprasidone • Zotepine; Typical antipsychotics: Chlorpromazine • Loxapine; Others: Butaclamol • EGIS-12,233 • Ketanserin • LY-215,840 • Metitepine/Methiothepin • Pimozide • Ritanserin • SB-258,719 • SB-258,741 • SB-269,970 • SB-656,104 • SB-656,104-A • SB-691,673 • SLV-313 • SLV-314 • Spiperone • SSR-181,507Reuptake inhibitors Selective serotonin reuptake inhibitors (SSRIs): Alaproclate • Citalopram • Dapoxetine • Desmethylcitalopram • Desmethylsertraline • Escitalopram • Femoxetine • Fluoxetine • Fluvoxamine • Indalpine • Ifoxetine • Litoxetine • Lubazodone • Panuramine • Paroxetine • Pirandamine • RTI-353 • Seproxetine • Sertraline • Tedatioxetine • Vilazodone • Vortioxetine • Zimelidine; Serotonin-norepinephrine reuptake inhibitors (SNRIs): Bicifadine • Desvenlafaxine • Duloxetine • Eclanamine • Levomilnacipran • Milnacipran • Sibutramine • Venlafaxine; Serotonin-norepinephrine-dopamine reuptake inhibitors (SNDRIs): Brasofensine • Diclofensine • DOV-102,677 • DOV-21,947 • DOV-216,303 • NS-2359 • SEP-225289 • SEP-227,162 • Tesofensine; Tricyclic antidepressants (TCAs): Amitriptyline • Butriptyline • Cianopramine • Clomipramine • Desipramine • Dosulepin • Doxepin • Imipramine • Lofepramine • Nortriptyline • Pipofezine • Protriptyline • Trimipramine; Tetracyclic antidepressants (TeCAs): Amoxapine; Piperazines: Nefazodone • Trazodone; Antihistamines: Brompheniramine • Chlorphenamine • Diphenhydramine • Mepyramine/Pyrilamine • Pheniramine • Tripelennamine; Opioids: Pethidine • Methadone • Propoxyphene; Others: Cocaine • CP-39,332 • Cyclobenzaprine • Dextromethorphan • Dextrorphan • EXP-561 • Fezolamine • Mesembrine • Nefopam • PIM-35 • Pridefine • Roxindole • SB-649,915 • ZiprasidoneReleasing agents Aminoindanes: 5-IAI • AMMI • ETAI • MDAI • MDMAI • MMAI • TAI; Aminotetralins: 6-CAT • 8-OH-DPAT • MDAT • MDMAT; Oxazolines: 4-Methylaminorex • Aminorex • Clominorex • Fluminorex; Phenethylamines (also Amphetamines, Cathinones, Phentermines, etc): 2-Methyl-MDA • 4-CAB • 4-FA • 4-FMA • 4-HA • 4-MTA • 5-APDB • 5-Methyl-MDA • 6-APDB • 6-Methyl-MDA • AEMMA • Amiflamine • BDB • BOH • Brephedrone • Butylone • Chlorphentermine • Cloforex • Amfepramone • Metamfepramone • DFMDA • DMA • DMMA • EBDB • EDMA • Ethylone • Etolorex • Fenfluramine (Dexfenfluramine) • Flephedrone • IAP • IMP • Lophophine • MBDB • MDA • MDEA • MDHMA • MDMA • MDMPEA • MDOH • MDPEA • Mephedrone • Methedrone • Methylone • MMA • MMDA • MMDMA • MMMA • NAP • Norfenfluramine • 4-TFMA • pBA • pCA • pIA • PMA • PMEA • PMMA • TAP; Piperazines: 2C-B-BZP • 2-BZP • 3-MeOPP • BZP • DCPP • MBZP • mCPP • MDBZP • MeOPP • Mepiprazole • pCPP • pFPP • pTFMPP • TFMPP; Tryptamines: 4-Methyl-αET • 4-Methyl-αMT • 5-CT • 5-MeO-αET • 5-MeO-αMT • 5-MT • αET • αMT • DMT • Tryptamine (itself); Others: Indeloxazine • Tramadol • ViqualineEnzyme inhibitors Nonselective: Benmoxin • Caroxazone • Echinopsidine • Furazolidone • Hydralazine • Indantadol • Iproclozide • Iproniazid • Isocarboxazid • Isoniazid • Linezolid • Mebanazine • Metfendrazine • Nialamide • Octamoxin • Paraxazone • Phenelzine • Pheniprazine • Phenoxypropazine • Pivalylbenzhydrazine • Procarbazine • Safrazine • Tranylcypromine; MAO-A Selective: Amiflamine • Bazinaprine • Befloxatone • Befol • Brofaromine • Cimoxatone • Clorgiline • Esuprone • Harmala alkaloids (Harmine, Harmaline, Tetrahydroharmine, Harman, Norharman, etc) • Methylene Blue • Metralindole • Minaprine • Moclobemide • Pirlindole • Sercloremine • Tetrindole • Toloxatone • TyrimaOthers Ferrous iron (Fe2+) • Magnesium (Mg2+) • Tetrahydrobiopterin • Vitamin B3 (Niacin, Nicotinamide → NADPH) • Vitamin B6 (Pyridoxine, Pyridoxamine, Pyridoxal → Pyridoxal phosphate) • Vitamin B9 (Folic Acid → Tetrahydrofolic acid) • Vitamin C (Ascorbic acid) • Zinc (Zn2+)OthersPhenethylamines Phenethylamines Psychedelics: 2C-B • 2C-B-FLY • 2C-C • 2C-D • 2C-E • 2C-F • 2C-G • 2C-I • 2C-N • 2C-P • 2C-SE • 2C-T • 2C-T-2 • 2C-T-4 • 2C-T-7 • 2C-T-8 • 2C-T-9 • 2C-T-13 • 2C-T-15 • 2C-T-17 • 2C-T-21 • 2C-TFM • 2C-YN • Allylescaline • DESOXY • Escaline • Isoproscaline • Jimscaline • Macromerine • MEPEA • Mescaline • Metaescaline • Methallylescaline • Proscaline • Psi-2C-T-4 • TCB-2
Stimulants: 2-OH-PEA • β-Me-PEA • Hordenine • N-Me-PEA • Phenethylamine (PEA)
Entactogens: Lophophine • MDPEA • MDMPEA
Others: BOH • DMPEAAmphetamines
PhenylisopropylaminesPsychedelics: 3C-BZ • 3C-E • 3C-P • Aleph • Beatrice • Bromo-DragonFLY • D-Deprenyl • DMA • DMCPA • DMMDA • DOB • DOC • DOEF • DOET • DOI • DOM • DON • DOPR • DOTFM • Ganesha • MMDA • MMDA-2 • Psi-DOM • TMA • TeMA
Stimulants: 4-MA • 4-MMA • 4-MTA • 5-IT • Alfetamine • Amfecloral • Amfepentorex • Amphetamine (Dextroamphetamine, Levoamphetamine) • Amphetaminil • Benfluorex • Benzphetamine • Cathine • Clobenzorex • Dimethylamphetamine • Ephedrine (EPH) • Ethylamphetamine • Fencamfamine • Fencamine • Fenethylline • Fenfluramine (Dexfenfluramine) • Fenproporex • Fludorex • Furfenorex • Isopropylamphetamine • Lefetamine • Mefenorex • Methamphetamine (Dextromethamphetamine, Levomethamphetamine) • Methoxyphenamine • MMA • Norfenfluramine • Oxilofrine • Ortetamine • PBA • PCA • Phenpromethamine • PFA • PFMA • PIA • PMA • PMEA • PMMA • Phenylpropanolamine (PPA) • Prenylamine • Propylamphetamine • Pseudoephedrine (PSE) • Sibutramine • Tiflorex (Flutiorex) • Tranylcypromine • Xylopropamine • Zylofuramine
Entactogens: 5-APDB • 6-APB • 6-APDB • EDA • IAP • MDA • MDEA • MDHMA (FLEA) • MDMA ("Ecstasy") • MDOH • MMDMA • NAP • TAP
Others: Amiflamine • DFMDA • D-Deprenyl • L-Deprenyl (Selegiline)Phentermines Stimulants: Chlorphentermine • Cloforex • Clortermine • Etolorex • Mephentermine • Pentorex (Phenpentermine) • Phentermine
Entactogens: MDPH • MDMPHCathinones Stimulants: Amfepramone • Brephedrone • Buphedrone • Bupropion (Amfebutamone) • Cathinone (Propion) • Dimethylcathinone (Dimethylpropion, Metamfepramone) • Ethcathinone (Ethylpropion) • Flephedrone • Methcathinone (Methylpropion) • Mephedrone • Methedrone
Entactogens: Ethylone • MethylonePhenylisobutylamines Phenylalkylpyrrolidines Stimulants: α-PBP • α-PPP • α-PVP • MDPBP • MDPPP • MDPV • MOPPP • MPBP • MPHP • MPPP • Naphyrone • PEP • Prolintane • PyrovaleroneCatecholamines
(and relatives..)6-FNE • 6-OHDA • α-Me-DA • α-Me-TRA • Adrenochrome • Ciladopa • D-DOPA (Dextrodopa) • Dopamine • Epinephrine (Adrenaline) • Epinine • Fenclonine • Ibopamine • L-DOPA (Levodopa) • L-DOPS (Droxidopa) • L-Phenylalanine • L-Tyrosine • meta-Octopamine • meta-Tyramine • Metanephrine • Metirosine • Methyldopa • Nordefrin (Levonordefrin) • Norepinephrine (Noradrenaline) • Normetanephrine • para-Octopamine • para-TyramineMiscellaneous Amidephrine • Arbutamine • Cafedrine • Denopamine • Dobutamine • Dopexamine • Etafedrine • Ethylnorepinephrine • Etilefrine • Famprofazone • Gepefrine • Isoprenaline (Isoproterenol) • Isoetarine • Metaraminol • Metaterol • Methoxamine • Norfenefrine • Orciprenaline • Phenylephrine (Neosynephrine) • Phenoxybenzamine • Prenalterol • Pronethalol • Propranolol • Salbutamol (Albuterol; Levosalbutamol) • Synephrine (Oxedrine) • Theodrenaline • XamoterolCategories:- Amphetamines
















Wikimedia Foundation. 2010.