- Herpes zoster
-
"Zoster" redirects here. For the ancient Greek article of dress, see Zoster (costume)."Shingles" redirects here. For other uses, see Shingle (disambiguation).
Herpes zoster Classification and external resources 
Herpes zoster blisters on the neck and shoulderICD-10 B02 ICD-9 053 DiseasesDB 29119 MedlinePlus 000858 eMedicine med/1007 derm/180 emerg/823 oph/257 ped/996 Herpes zoster (or simply zoster), commonly known as shingles and also known as zona, is a viral disease characterized by a painful skin rash with blisters in a limited area on one side of the body, often in a stripe. The initial infection with varicella zoster virus (VZV) causes the acute (short-lived) illness chickenpox which generally occurs in children and young people. Once an episode of chickenpox has resolved, the virus is not eliminated from the body but can go on to cause shingles—an illness with very different symptoms—often many years after the initial infection. Herpes zoster is not the same disease as herpes simplex despite the name similarity (both the varicella zoster virus and herpes simplex virus belong to the same viral subfamily Alphaherpesvirinae).
Varicella zoster virus can become latent in the nerve cell bodies and less frequently in non-neuronal satellite cells of dorsal root, cranial nerve or autonomic ganglion,[1] without causing any symptoms.[2] Years or decades after a chickenpox infection, the virus may break out of nerve cell bodies and travel down nerve axons to cause viral infection of the skin in the region of the nerve. The virus may spread from one or more ganglia along nerves of an affected segment and infect the corresponding dermatome (an area of skin supplied by one spinal nerve) causing a painful rash.[3][4] Although the rash usually heals within two to four weeks, some sufferers experience residual nerve pain for months or years, a condition called postherpetic neuralgia. Exactly how the virus remains latent in the body, and subsequently re-activates is not understood.[1]
Throughout the world the incidence rate of herpes zoster every year ranges from 1.2 to 3.4 cases per 1,000 healthy individuals, increasing to 3.9–11.8 per year per 1,000 individuals among those older than 65 years.[5][6][7] Antiviral drug treatment can reduce the severity and duration of herpes zoster if a seven-to-ten day course of these drugs is started within 72 hours of the appearance of the characteristic rash.[5][8]
Contents
Signs and symptoms
 A case of shingles that demonstrates the typical dermatomal distribution, in this case C8/T1
A case of shingles that demonstrates the typical dermatomal distribution, in this case C8/T1
The earliest symptoms of herpes zoster, which include headache, fever, and malaise, are nonspecific, and may result in an incorrect diagnosis.[5][9] These symptoms are commonly followed by sensations of burning pain, itching, hyperesthesia (oversensitivity), or paresthesia ("pins and needles": tingling, pricking, or numbness).[10] The pain may be mild to extreme in the affected dermatome, with sensations that are often described as stinging, tingling, aching, numbing or throbbing, and can be interspersed with quick stabs of agonizing pain.[11]
Herpes zoster in children is often painless, but older people are more likely to get zoster as they age, and the disease tends to be more severe.[12]
In most cases after 1–2 days, but sometimes as long as 3 weeks, the initial phase is followed by the appearance of the characteristic skin rash. The pain and rash most commonly occurs on the torso, but can appear on the face, eyes or other parts of the body. At first the rash appears similar to the first appearance of hives; however, unlike hives, herpes zoster causes skin changes limited to a dermatome, normally resulting in a stripe or belt-like pattern that is limited to one side of the body and does not cross the midline.[10] Zoster sine herpete ("zoster without herpes") describes a patient who has all of the symptoms of herpes zoster except this characteristic rash.[13]
Later the rash becomes vesicular, forming small blisters filled with a serous exudate, as the fever and general malaise continue. The painful vesicles eventually become cloudy or darkened as they fill with blood, crust over within seven to ten days; usually the crusts fall off and the skin heals, but sometimes, after severe blistering, scarring and discolored skin remain.[10]
Development of the shingles rash Day 1 Day 2 Day 5 Day 6 



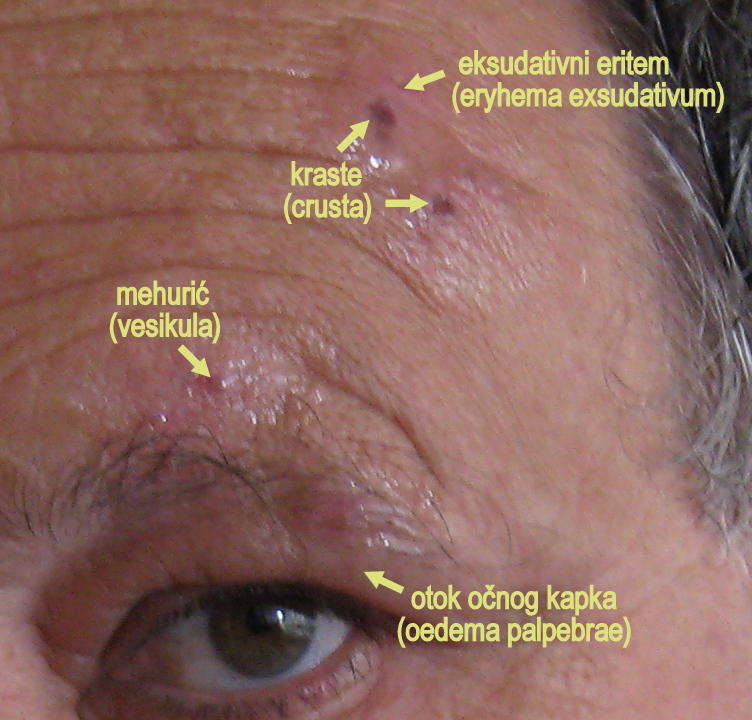
Herpes zoster may have additional symptoms, depending on the dermatome involved. Herpes zoster ophthalmicus involves the orbit of the eye and occurs in approximately 10–25% of cases. It is caused by the virus reactivating in the ophthalmic division of the trigeminal nerve. In a few patients, symptoms may include conjunctivitis, keratitis, uveitis, and optic nerve palsies that can sometimes cause chronic ocular inflammation, loss of vision, and debilitating pain.[14] Herpes zoster oticus, also known as Ramsay Hunt syndrome type II, involves the ear. It is thought to result from the virus spreading from the facial nerve to the vestibulocochlear nerve. Symptoms include hearing loss and vertigo (rotational dizziness).[1]
Pathophysiology
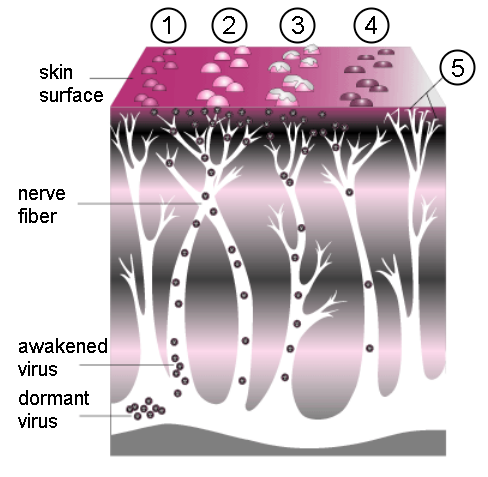
 Progression of herpes zoster. A cluster of small bumps (1) turns into blisters (2). The blisters fill with lymph, break open (3), crust over (4), and finally disappear. Postherpetic neuralgia can sometimes occur due to nerve damage (5),
Progression of herpes zoster. A cluster of small bumps (1) turns into blisters (2). The blisters fill with lymph, break open (3), crust over (4), and finally disappear. Postherpetic neuralgia can sometimes occur due to nerve damage (5),The causative agent for herpes zoster is varicella zoster virus (VZV), a double-stranded DNA virus related to the Herpes simplex virus group. Most people are infected with this virus as children, and suffer from an episode of chickenpox. The immune system eventually eliminates the virus from most locations, but it remains dormant (or latent) in the ganglia adjacent to the spinal cord (called the dorsal root ganglion) or the ganglion semilunare (ganglion Gasseri) in the base of the skull.[15] Repeated attacks of herpes zoster are rare,[10] and it is extremely rare for patients to suffer more than three recurrences.[15]
Herpes zoster occurs only in people who have been previously infected with VZV; although it can occur at any age, approximately half of the cases in the USA occur in those aged 50 years or older.[16] The disease results from the virus reactivating in a single sensory ganglion.[4] In contrast to Herpes simplex virus, the latency of VZV is poorly understood. The virus has not been recovered from human nerve cells by cell culture and the location and structure of the viral DNA is not known. Virus-specific proteins continue to be made by the infected cells during the latent period, so true latency, as opposed to a chronic low-level infection, has not been proven.[2][17] Although VZV has been detected in autopsies of nervous tissue,[18] there are no methods to find dormant virus in the ganglia in living people.
Unless the immune system is compromised, it suppresses reactivation of the virus and prevents herpes zoster. Why this suppression sometimes fails is poorly understood,[6] but herpes zoster is more likely to occur in people whose immune system is impaired due to aging, immunosuppressive therapy, psychological stress, or other factors.[19] Upon reactivation, the virus replicates in the nerve cells, and virions are shed from the cells and carried down the axons to the area of skin served by that ganglion. In the skin, the virus causes local inflammation and blisters. The short- and long-term pain caused by herpes zoster comes from the widespread growth of the virus in the infected nerves, which causes inflammation.[20]
As with chickenpox and/or other forms of herpes, direct contact with an active rash can spread VZV to a person who has no immunity to the virus. This newly infected individual may then develop chickenpox, but will not immediately develop shingles. Until the rash has developed crusts, a person is extremely contagious. A person is also not infectious before blisters appear, or during postherpetic neuralgia (pain after the rash is gone).[10]
Diagnosis
 Herpes zoster on the chest
Herpes zoster on the chestIf the rash has appeared, identifying this disease (making a differential diagnosis) requires only a visual examination, since very few diseases produce a rash in a dermatomal pattern (see map). However, herpes simplex virus (HSV) can occasionally produce a rash in such a pattern. The Tsanck smear is helpful for diagnosing acute infection with a herpes virus, but does not distinguish between HSV and VZV.[21]
When the rash is absent (early or late in the disease, or in the case of zoster sine herpete), herpes zoster can be difficult to diagnose.[22] Apart from the rash, most symptoms can occur also in other conditions.
Laboratory tests are available to diagnose herpes zoster. The most popular test detects VZV-specific IgM antibody in blood; this appears only during chickenpox or herpes zoster and not while the virus is dormant.[23] In larger laboratories, lymph collected from a blister is tested by polymerase chain reaction for VZV DNA, or examined with an electron microscope for virus particles.[24]
In a recent study, samples of lesions on the skin, eyes, and lung from 182 patients with presumed herpes simplex or herpes zoster were tested with real-time PCR or with viral culture. In this comparison, viral culture detected VZV with only a 14.3% sensitivity, although the test was highly specific (specificity=100%). By comparison, real-time PCR resulted in 100% sensitivity and specificity. Overall testing for herpes simplex and herpes zoster using PCR showed a 60.4% improvement over viral culture.[25]
Prevention
A live vaccine for VZV exists, marketed as Zostavax.[26] In a 2005 study of 38,000 older adults it prevented half the cases of herpes zoster and reduced the number of cases of postherpetic neuralgia by two-thirds.[27] A 2007 study found that the zoster vaccine is likely to be cost-effective in the U.S., projecting an annual savings of $82 to $103 million in healthcare costs with cost-effectiveness ratios ranging from $16,229 to $27,609 per quality-adjusted life year gained.[28] In October 2007 the vaccine was officially recommended in the U.S. for healthy adults aged 60 and over.[26][29] Adults also receive an immune boost from contact with children infected with varicella (chicken pox), a boosting method that prevents about a quarter of herpes zoster cases among unvaccinated adults, but that is becoming less common in the U.S. now that children are routinely vaccinated against varicella.[8][30] The shingles vaccination can cut the risk of the severe disease by 55 percent.[31] The Centers for Disease Control and Prevention recommends shingle vaccine for use in people 60 years old and older to prevent shingles, but it is not recommended to treat active shingles or post-herpetic neuralgia (pain after the rash is gone) once it develops.[32]
In the United Kingdom and other parts of Europe, population-based varicella immunization is not practised. The rationale is that until the entire population could be immunized, adults who have previously contracted VZV would instead derive benefit from occasional exposure to VZV (from children), which serves as a booster to their immunity to the virus, and may reduce the risk of shingles later on in life.[33] The UK Health Protection Agency states that, while the vaccine is licensed in the UK, there are no plans to introduce it into the routine childhood immunization scheme, although it may be offered to healthcare workers who have no immunity to VZV.[34]
A 2006 study of 243 cases and 483 matched controls found that fresh fruit is associated with a reduced risk of developing shingles–people who consumed less than one serving of fruit a day had a risk three times as great as those who consumed more than three servings, after adjusting for other factors such as total energy intake. For those aged 60 or more, vitamins and vegetable intake had a similar association.[35]
Treatment
The aims of treatment are to limit the severity and duration of pain, shorten the duration of a shingles episode, and reduce complications. Symptomatic treatment is often needed for the complication of postherpetic neuralgia.[36] However, a study on untreated herpes zoster shows that, once the rash has cleared, postherpetic neuralgia is very rare in people under 50 and wears off in time; in older people the pain wore off more slowly, but even in people over 70, 85% were pain free one year after their shingles outbreak.[37]
Analgesics
People with mild to moderate pain can be treated with over-the-counter analgesics. Topical lotions containing calamine can be used on the rash or blisters and may be soothing. Occasionally, severe pain may require an opioid medication, such as morphine. Once the lesions have crusted over, capsaicin cream (Zostrix) can be used. Topical lidocaine and nerve blocks may also reduce pain.[38] Administering gabapentin along with antivirals may offer relief of postherpetic neuralgia.[36]
Antivirals
Antiviral drugs inhibit VZV replication and reduce the severity and duration of herpes zoster with minimal side effects, but do not reliably prevent postherpetic neuralgia. Of these drugs, acyclovir has been the standard treatment, but the new drugs valaciclovir and famciclovir demonstrate similar or superior efficacy and good safety and tolerability.[36] The drugs are used both as prophylaxis (for example in AIDS patients) and as therapy during the acute phase. Antiviral treatment is recommended for all immunocompetent individuals with herpes zoster over 50 years old, preferably given within 72 hours of the appearance of the rash.[39] Complications in immunocompromised individuals with herpes zoster may be reduced with intravenous acyclovir. In people who are at a high risk for repeated attacks of shingles, five daily oral doses of acyclovir are usually effective.[1]
Steroids
Orally administered corticosteroids are frequently used in treatment of the infection, despite clinical trials of this treatment being unconvincing. Nevertheless, one trial studying immunocompetent patients older than 50 years of age with localized herpes zoster, suggested that administration of prednisone with aciclovir improved healing time and quality of life.[40] Upon one-month evaluation, aciclovir with prednisone increased the likelihood of crusting and healing of lesions by about twofold, when compared to placebo. This trial also evaluated the effects of this drug combination on quality of life at one month, showing that patients had less pain, and were more likely to stop the use of analgesic agents, return to usual activities and have uninterrupted sleep. However, when comparing cessation of herpes zoster-associated pain or post herpetic neuralgia, there was no difference between aciclovir plus prednisone and simply aciclovir alone. Because of the risks of corticosteroid treatment, it is recommended that this combination of drugs only be used in people more than 50 years of age, due to their greater risk of postherpetic neuralgia.[40]
Herpes zoster ophthalmicus
 Herpes zoster ophthalmicus
Herpes zoster ophthalmicus Trigeminal herpes zoster with uveitis and keratitis
Trigeminal herpes zoster with uveitis and keratitisTreatment for herpes zoster ophthalmicus is similar to standard treatment for herpes zoster at other sites. A recent trial comparing aciclovir with its prodrug, valaciclovir, demonstrated similar efficacies in treating this form of the disease.[41] The significant advantage of valciclovir over aciclovir is its dosing of only 3 times/day (compared with aciclovir's 5 times/day dosing), which could make it more convenient for patients and improve adherence with therapy.[42]
Prognosis
The rash and pain usually subside within three to five weeks, but about one in five patients develops a painful condition called postherpetic neuralgia, which is often difficult to manage. In some patients, herpes zoster can reactivate presenting as zoster sine herpete: pain radiating along the path of a single spinal nerve (a dermatomal distribution), but without an accompanying rash. This condition may involve complications that affect several levels of the nervous system and cause multiple cranial neuropathies, polyneuritis, myelitis, or aseptic meningitis. Other serious effects that may occur in some cases include partial facial paralysis (usually temporary), ear damage, or encephalitis.[1] During pregnancy, first infections with VZV, causing chickenpox, may lead to infection of the fetus and complications in the newborn, but chronic infection or reactivation in shingles are not associated with fetal infection.[43][44]
There is a slightly increased risk of developing cancer after a herpes zoster infection. However, the mechanism is unclear and mortality from cancer did not appear to increase as a direct result of the presence of the virus.[45] Instead, the increased risk may result from the immune suppression that allows the reactivation of the virus.[46]
Although herpes zoster typically resolves within 2 weeks, certain complications may arise:
- Secondary bacterial infection
- Motor involvement - incl. weakness especially in "motor herpes zoster"
- Eye involvement - trigeminal nerve involvement (as seen in herpes ophthalmicus) should be treated early and aggressively as it may lead to blindness. Involvement of the tip of the nose in the zoster rash is a strong predictor of herpes ophthalmicus.[47]
- Postherpetic neuralgia - a condition of chronic pain following herpes zoster
Epidemiology
 See also: Chickenpox epidemiology
See also: Chickenpox epidemiologyVaricella zoster virus (VZV) has a high level of infectivity and has a worldwide prevalence.[48] Herpes zoster is a re-activation of latent VZV infection: this means that zoster can only occur in someone who has previously had chickenpox (varicella).
Herpes zoster has no relationship to season and does not occur in epidemics. There is, however, a strong relationship with increasing age.[12][19] The incidence rate of herpes zoster ranges from 1.2 to 3.4 per 1,000 person-years among healthy individuals, increasing to 3.9–11.8 per 1,000 person‐years among those older than 65 years,[5][12] and incidence rates worldwide are similar.[5][7] This relationship with age has been demonstrated in many different countries,[5][7][49][50][51][52] and is attributed to the fact that cellular immunity declines as people grow older.
Another important risk factor is immunocompromise: HIV is an important example of immune compromise[53][54]). Other risk factors include psychological stress.[11][55][56] Blacks are at lower risk of shingles than white caucasians.[57][58] It is unclear whether the risk is increased in females. Other potential risk factors include mechanical trauma, and exposure to immunotoxins.[19][56]
There is not strong evidence for a genetic link or a link to family history. A 2008 study showed that people with close relatives who have had shingles are twice as likely to develop it themselves,[59] but a study performed in Italy was not able to prove that family history is not a risk factor or evidence for a link to genetic factors.[56]
Adults with latent VZV infection who are exposed intermittently to children with chickenpox receive an immune boost.[12][56] This periodic boost to the immune system helps to prevent shingles in older adults. When routine chickenpox vaccination was introduced in the US, the concern was that because older adults would no longer receive this natural, periodic boost, this would result in an increase in the incidence of shingles in the US.
Multiple studies and surveillance data, at least when viewed superficially, demonstrate no consistent trends in incidence in the U.S. since the chickenpox vaccination program began in 1995.[60] However, upon closer inspection, the two studies that showed no increase in shingles incidence were conducted among populations where varicella vaccination was not as yet widespread in the community.[61][62] A recent study by Patel et al. concluded that since the introduction of the chickenpox vaccine, hospitalization costs for complications of shingles have increased by more than $700 million annually for those over 60 years.[63] Another study by Yih et al. reported that as varicella vaccine coverage in children increased, the incidence of varicella decreased and the occurrence of shingles among adults increased 90%.[64] The results of a further study by Yawn et al. showed a 28% increase in shingles incidence from 1996 to 2001.[65] It is likely that incidence rate will change in the future, due to the aging of the population, changes in therapy for malignant and autoimmune diseases, and changes in chickenpox vaccination rates; a wide adoption of zoster vaccination could dramatically reduce the incidence rate.[5]
In one study, it was estimated that 26% of patients who contract herpes zoster eventually present with complications. Postherpetic neuralgia arises in approximately 20% of patients.[66] A study of 1994 California data found hospitalization rates of 2.1 per 100,000 person-years, rising to 9.3 per 100,000 person-years for ages 60 and up.[67] An earlier Connecticut study found a higher hospitalization rate; the difference may be due to the prevalence of HIV in the earlier study, or to the introduction of antivirals in California before 1994.[68]
History
Herpes zoster has a long recorded history, although historical accounts fail to distinguish the blistering caused by VZV and those caused by smallpox,[16] ergotism, and erysipelas. It was only in the late eighteenth century that William Heberden established a way to differentiate between herpes zoster and smallpox,[69] and only in the late nineteenth century that herpes zoster was differentiated from erysipelas. In 1831, Richard Bright hypothesized that the disease arose from the dorsal root ganglion, and this was confirmed in an 1861 paper by Felix von Bärunsprung.[70]
The first indications that chickenpox and herpes zoster were caused by the same virus were noticed at the beginning of the 20th century. Physicians began to report that cases of herpes zoster were often followed by chickenpox in the younger people who lived with the shingles patients. The idea of an association between the two diseases gained strength when it was shown that lymph from a sufferer of herpes zoster could induce chickenpox in young volunteers. This was finally proved by the first isolation of the virus in cell cultures, by the Nobel laureate Thomas Huckle Weller, in 1953.[71]
Until the 1940s, the disease was considered benign, and serious complications were thought to be very rare.[72] However, by 1942, it was recognized that herpes zoster was a more serious disease in adults than in children, and that it increased in frequency with advancing age. Further studies during the 1950s on immunosuppressed individuals showed that the disease was not as benign as once thought, and the search for various therapeutic and preventive measures began.[73] By the mid-1960s, several studies identified the gradual reduction in cellular immunity in old age, observing that in a cohort of 1,000 people who lived to the age of 85, approximately 500 (i.e., 50%) would have at least one attack of herpes zoster, and 10 (i.e., 1%) would have at least two attacks.[74]
In historical shingles studies, shingles incidence generally increased with age. However, in his 1965 paper, Dr. Hope-Simpson was first to suggest, “The peculiar age distribution of zoster may in part reflect the frequency with which the different age groups encounter cases of varicella and because of the ensuing boost to their antibody protection have their attacks of zoster postponed.”[12] Lending support to this hypothesis that contact with children with chickenpox boosts adult cell-mediated immunity to help postpone or suppress shingles, is the study by Thomas et al., which reported that adults in households with children had lower rates of shingles than households without children.[75] Also, the study by Terada et al. indicated that pediatricians reflected incidence rates from 1/2 to 1/8 that of the general population their age.[76]
Etymology
The family name of all the herpesviridae is derived from the Greek word herpein ("to creep"),[77] referring to the latent, recurring infections typical of this group of viruses. Zoster comes from Greek zōstēr, meaning "belt" or "girdle", after the characteristic belt-like dermatomal rash.[78] The common name for the disease, shingles, derives from the Latin cingulus, a variant of Latin cingulum meaning "girdle".[79]
See also
- Disseminated herpes zoster
- Inflammatory skin lesions following zoster infection
References
- ^ a b c d e Johnson, RW & Dworkin, RH (2003). "Clinical review: Treatment of herpes zoster and postherpetic neuralgia". BMJ 326 (7392): 748. doi:10.1136/bmj.326.7392.748. PMC 1125653. PMID 12676845. http://www.bmj.com/cgi/content/full/326/7392/748.
- ^ a b Kennedy PG (2002). "Varicella-zoster virus latency in human ganglia". Rev. Med. Virol. 12 (5): 327–34. doi:10.1002/rmv.362. PMID 12211045.
- ^ Peterslund NA (1991). "Herpesvirus infection: an overview of the clinical manifestations". Scand J Infect Dis Suppl 80: 15–20. PMID 1666443.
- ^ a b Gilden DH, Cohrs RJ, Mahalingam R (2003). "Clinical and molecular pathogenesis of varicella virus infection". Viral Immunol 16 (3): 243–58. doi:10.1089/088282403322396073. PMID 14583142.
- ^ a b c d e f g Dworkin RH, Johnson RW, Breuer J et al. (2007). "Recommendations for the management of herpes zoster". Clin. Infect. Dis 44 Suppl 1: S1–26. doi:10.1086/510206. PMID 17143845. http://www.journals.uchicago.edu/doi/full/10.1086/510206.
- ^ a b Donahue JG, Choo PW, Manson JE, Platt R (1995). "The incidence of herpes zoster". Arch. Intern. Med 155 (15): 1605–9. doi:10.1001/archinte.155.15.1605. PMID 7618983.
- ^ a b c Araújo LQ, Macintyre CR, Vujacich C (2007). "Epidemiology and burden of herpes zoster and post-herpetic neuralgia in Australia, Asia and South America" (PDF). Herpes 14 (Suppl 2): 40A–4A. PMID 17939895. http://www.ihmf.org/journal/download/5%20-%20Herpes%2014.2%20suppl%20Araujo.pdf.
- ^ a b Cunningham AL, Breuer J, Dwyer DE, Gronow DW, Helme RD, Litt JC, Levin MJ, Macintyre CR (2008). "The prevention and management of herpes zoster". Med. J. Aust. 188 (3): 171–6. PMID 18241179.
- ^ Zamula E (May–June 2001). [permanent.access.gpo.gov/lps1609/www.fda.gov/fdac/features/2001/301_pox.html "Shingles: an unwelcome encore"]. FDA Consumer 35 (3): 21–5. PMID 11458545. permanent.access.gpo.gov/lps1609/www.fda.gov/fdac/features/2001/301_pox.html. Retrieved 2010-01-05. Revised June 2005.
- ^ a b c d e Stankus SJ, Dlugopolski M, Packer D (2000). "Management of herpes zoster (shingles) and postherpetic neuralgia". Am Fam Physician 61 (8): 2437–44, 2447–8. PMID 10794584. http://www.aafp.org/afp/20000415/2437.html.
- ^ a b Katz J, Cooper EM, Walther RR, Sweeney EW, Dworkin RH (2004). "Acute pain in herpes zoster and its impact on health-related quality of life". Clin. Infect. Dis 39 (3): 342–8. doi:10.1086/421942. PMID 15307000. http://www.journals.uchicago.edu/doi/full/10.1086/421942.
- ^ a b c d e Hope-Simpson RE (1965). "The nature of herpes zoster: a long-term study and a new hypothesis". Proc R Soc Med 58: 9–20. PMC 1898279. PMID 14267505. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1898279.
- ^ Furuta Y, Ohtani F, Mesuda Y, Fukuda S, Inuyama Y (2000). "Early diagnosis of zoster sine herpete and antiviral therapy for the treatment of facial palsy". Neurology 55 (5): 708–10. PMID 10980741.
- ^ Shaikh S, Ta CN (2002). "Evaluation and management of herpes zoster ophthalmicus". Am Fam Physician 66 (9): 1723–1730. PMID 12449270. http://www.aafp.org/afp/20021101/1723.html.
- ^ a b Steiner I, Kennedy PG, Pachner AR (2007). "The neurotropic herpes viruses: herpes simplex and varicella-zoster". Lancet Neurol 6 (11): 1015–28. doi:10.1016/S1474-4422(07)70267-3. PMID 17945155.
- ^ a b Weinberg JM (2007). "Herpes zoster: epidemiology, natural history, and common complications". J Am Acad Dermatol 57 (6 Suppl): S130–5. doi:10.1016/j.jaad.2007.08.046. PMID 18021864.
- ^ Kennedy PG (2002). "Key issues in varicella-zoster virus latency". J. Neurovirol 8 Suppl 2 (2): 80–4. doi:10.1080/13550280290101058. PMID 12491156.
- ^ Mitchell BM, Bloom DC, Cohrs RJ, Gilden DH, Kennedy PG (2003). "Herpes simplex virus-1 and varicella-zoster virus latency in ganglia" (PDF). J. Neurovirol 9 (2): 194–204. doi:10.1080/713831492. PMID 12707850. http://www.jneurovirol.com/o_pdf/9(2)/194-204.pdf.
- ^ a b c Thomas SL, Hall AJ (2004). "What does epidemiology tell us about risk factors for herpes zoster?". Lancet Infect Dis 4 (1): 26–33. doi:10.1016/S1473-3099(03)00857-0. PMID 14720565.
- ^ Schmader K (2007). "Herpes zoster and postherpetic neuralgia in older adults". Clin. Geriatr. Med. 23 (3): 615–32, vii–viii. doi:10.1016/j.cger.2007.03.003. PMID 17631237. http://linkinghub.elsevier.com/retrieve/pii/S0749-0690(07)00021-3.
- ^ Oranje AP, Folkers E (1988). "The Tzanck smear: old, but still of inestimable value". Pediatr Dermatol 5 (2): 127–9. doi:10.1111/j.1525-1470.1988.tb01154.x. PMID 2842739.
- ^ Chan J, Bergstrom RT, Lanza DC, Oas JG (2004). "Lateral sinus thrombosis associated with zoster sine herpete". Am J Otolaryngol 25 (5): 357–60. doi:10.1016/j.amjoto.2004.03.007. PMID 15334402.
- ^ Arvin AM (1996). "Varicella-zoster virus" (PDF). Clin. Microbiol. Rev 9 (3): 361–81. PMC 172899. PMID 8809466. http://cmr.asm.org/cgi/reprint/9/3/361.pdf.
- ^ Beards G, Graham C, Pillay D (1998). "Investigation of vesicular rashes for HSV and VZV by PCR". J. Med. Virol 54 (3): 155–7. doi:10.1002/(SICI)1096-9071(199803)54:3<155::AID-JMV1>3.0.CO;2-4. PMID 9515761.
- ^ Stránská R, Schuurman R, de Vos M, van Loon AM. (2003). "Routine use of a highly automated and internally controlled real-time PCR assay for the diagnosis of herpes simplex and varicella-zoster virus infections". J Clin Virol. 30 (1): 39–44. doi:10.1016/j.jcv.2003.08.006. PMID 15072752.
- ^ a b Harpaz R, Ortega-Sanchez IR, Seward JF (June 6, 2008). "Prevention of herpes zoster: recommendations of the Advisory Committee on Immunization Practices (ACIP)". MMWR Recomm Rep 57 (RR–5): 1–30; quiz CE2–4. PMID 18528318. http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5705a1.htm. Retrieved 2010-01-04.
- ^ Oxman MN, Levin MJ, Johnson GR, Schmader KE, Straus SE, Gelb LD et al. (2005). "A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults". N. Engl. J. Med. 253 (22): 2271–84. doi:10.1056/NEJMoa051016. PMID 15930418.
- ^ Pellissier JM, Brisson M, Levin MJ (2007). "Evaluation of the cost-effectiveness in the United States of a vaccine to prevent herpes zoster and postherpetic neuralgia in older adults". Vaccine 25 (49): 8326–37. doi:10.1016/j.vaccine.2007.09.066. PMID 17980938.
- ^ Advisory Committee on Immunization Practices (20 November 2007). "Recommended adult immunization schedule: United States, October 2007 – September 2008". Ann Intern Med 147 (10): 725–9. PMID 17947396. http://www.annals.org/cgi/content/full/147/10/725.
- ^ Brisson M, Gay N, Edmunds W, Andrews N (2002). "Exposure to varicella boosts immunity to herpes-zoster: implications for mass vaccination against chickenpox". Vaccine 20 (19–20): 2500–7. doi:10.1016/S0264-410X(02)00180-9. PMID 12057605.
- ^ Tseng HF, SmithN, Harpaz R, Bialek SR, Sy LS, Jacobsen SJ (2011). "Herpes Zoster Vaccine in Older Adults and the Risk of Subsequent Herpes Zoster Disease". JAMA 305 (2): 160–166. doi:10.1001/jama.2010.1983. PMID 21224457.
- ^ Gilden D (February 2011). "Efficacy of live zoster vaccine in preventing zoster and postherpetic neuralgia". J Intern Med 269 (5): 496–506. doi:10.1111/j.1365-2796.2011.02359.x. PMC 3083261. PMID 21294791. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=3083261. Retrieved 2011-03-13.
- ^ NHS Direct (2008-02-07). "Why isn’t the chickenpox vaccine available in the UK?". Archived from the original on 2008-04-23. http://web.archive.org/web/20080423095454/http://www.nhsdirect.nhs.uk/articles/article.aspx?articleId=1032. Retrieved 2008-03-22.
- ^ Health Protection Agency (2006-05-11). "Chickenpox / Varicella — General Information". http://www.hpa.org.uk/infections/topics_az/chickenpox/gen_info.htm. Retrieved 2008-03-22.
- ^ Thomas SL, Wheeler JG, Hall AJ (2006). "Micronutrient intake and the risk of herpes zoster: a case-control study". Int J Epidemiol 35 (2): 307–14. doi:10.1093/ije/dyi270. PMID 16330478. http://ije.oxfordjournals.org/cgi/content/full/35/2/307.
- ^ a b c Tyring SK (2007). "Management of herpes zoster and postherpetic neuralgia". J Am Acad Dermatol 57 (6 Suppl): S136–42. doi:10.1016/j.jaad.2007.09.016. PMID 18021865.
- ^ Sigurdur Helgason et al (2000). "Prevalence of postherpetic neuralgia after a single episode of herpes zoster: prospective study with long term follow up" (PDF). British Medical Journal 321 (7264): 794–6. doi:10.1136/bmj.321.7264.794. PMC 27491. PMID 11009518. http://www.bmj.com/cgi/content/full/321/7264/794.
- ^ Baron R (2004). "Post-herpetic neuralgia case study: optimizing pain control". Eur. J. Neurol 11 Suppl 1: 3–11. doi:10.1111/j.1471-0552.2004.00794.x. PMID 15061819.
- ^ Breuer J, Whitley R (2007). "Varicella zoster virus: natural history and current therapies of varicella and herpes zoster" (PDF). Herpes 14 (Suppl 2): 25–9. PMID 17939892. http://www.ihmf.org/journal/download/2%20-%20Herpes%2014.2%20suppl%20Breuer.pdf.
- ^ a b Whitley RJ, Weiss H, Gnann JW, Tyring S, Mertz GJ, Pappas PG, Schleupner CJ, Hayden F, Wolf J, Soong SJ (1996). "Acyclovir with and without prednisone for the treatment of herpes zoster. A randomized, placebo-controlled trial. The National Institute of Allergy and Infectious Diseases Collaborative Antiviral Study Group". Ann. Intern. Med. 125 (5): 376–83. PMID 8702088.
- ^ Colin J, Prisant O, Cochener B, Lescale O, Rolland B, Hoang-Xuan T (2000). "Comparison of the Efficacy and Safety of Valaciclovir and Acyclovir for the Treatment of Herpes zoster Ophthalmicus". Ophthalmology 107 (8): 1507–11. doi:10.1016/S0161-6420(00)00222-0. PMID 10919899.
- ^ Osterberg L, Blaschke T (2005). "Adherence to medication". N. Engl. J. Med. 353 (5): 487–97. doi:10.1056/NEJMra050100. PMID 16079372.
- ^ Paryani SG, Arvin AM (1986). "Intrauterine infection with varicella-zoster virus after maternal varicella". N. Engl. J. Med. 314 (24): 1542–6. doi:10.1056/NEJM198606123142403. PMID 3012334.
- ^ Enders G, Miller E, Cradock-Watson J, Bolley I, Ridehalgh M (1994). "Consequences of varicella and herpes zoster in pregnancy: prospective study of 1739 cases". Lancet 343 (8912): 1548–51. doi:10.1016/S0140-6736(94)92943-2. PMID 7802767.
- ^ Sørensen HT, Olsen JH, Jepsen P, Johnsen SP, Schønheyder HC, Mellemkjaer L (2004). "The risk and prognosis of cancer after hospitalisation for herpes zoster: a population-based follow-up study". Br. J. Cancer 91 (7): 1275–9. doi:10.1038/sj.bjc.6602120. PMC 2409892. PMID 15328522. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2409892.
- ^ Ragozzino MW, Melton LJ, Kurland LT, Chu CP, Perry HO (1982). "Risk of cancer after herpes zoster: a population-based study". N. Engl. J. Med. 307 (7): 393–7. doi:10.1056/NEJM198208123070701. PMID 6979711.
- ^ "Herpes Zoster Ophthalmicus". Merck Manual (Merk.com). October 2008. http://www.merck.com/mmpe/sec09/ch102/ch102e.html. Retrieved June 2010.
- ^ Apisarnthanarak A, Kitphati R, Tawatsupha P, Thongphubeth K, Apisarnthanarak P, Mundy LM (2007). "Outbreak of varicella-zoster virus infection among Thai healthcare workers". Infect Control Hosp Epidemiol 28 (4): 430–4. doi:10.1086/512639. PMID 17385149.
- ^ Brisson M, Edmunds WJ, Law B, et al. (2001). "Epidemiology of varicella zoster virus infection in Canada and the United Kingdom". Epidemiol Infect 127 (2): 305–14. PMID 11693508.
- ^ Insinga RP, Itzler RF, Pellissier JM, Saddier P, Nikas AA (2005). "The incidence of herpes zoster in a United States administrative database". J Gen Intern Med 20 (8): 748–53. PMID 16050886.
- ^ Yawn BP, Saddier P, Wollan PC, St Sauver JL, Kurland MJ, Sy LS (2007). "A population-based study of the incidence and complication rates of herpes zoster before zoster vaccine introduction". Mayo Clin Proc 82 (11): 1341–9. doi:10.4065/82.11.1341. PMID 17976353.
- ^ de Melker H, Berbers G, Hahné S, et al. (2006). "The epidemiology of varicella and herpes zoster in The Netherlands: implications for varicella zoster virus vaccination.". Vaccine 24 (18): 3946–52. doi:10.1016/j.vaccine.2006.02.017. PMID 16564115.
- ^ Colebunders R, Mann JM, Francis H, et al.. "Herpes zoster in African patients: a clinical predictor of human immunodeficiency virus infection". J Infect Dis 157 (2): 314–318. doi:10.1093/infdis/157.2.314.
- ^ Buchbinder SP, Katz MH, Hessol NA, et al. (1992). "Herpes zoster and human immunodeficiency virus infection". J Infect Dis 166 (5): 1153–1156. doi:10.1093/infdis/166.5.1153.
- ^ Livengood JM (2000). "The role of stress in the development of herpes zoster and postherpetic neuralgia". Curr Rev Pain 4 (1): 7–11. PMID 10998709.
- ^ a b c d Gatti A, Pica F, Boccia MT, De Antoni F, Sabato AF, Volpi A. (2010). "No evidence of family history as a risk factor for herpes zoster in patients with post-herpetic neuralgia.". J Med Virol 82 (6): 1007–11. PMID 20419815.
- ^ Schmader K, George LK, Burchett BM, Pieper CF (1998). "Racial and psychosocial risk factors for herpes zoster in the elderly.". J Infect Dis 178 (Suppl 1): S67–70. PMID 9852978.
- ^ Schmader K, George LK, Burchett BM, Hamilton JD, Pieper CF (1998). "Race and stress in the incidence of herpes zoster in older adults.". J Am Geriatr Soc 46 (8): 973–7. PMID 9706885.
- ^ Hicks LD, Cook-Norris RH, Mendoza N, Madkan V, Arora A, Tyring SK (May 2008). "Family history as a risk factor for herpes zoster: a case-control study". Arch Dermatol 144 (5): 603–8. doi:10.1001/archderm.144.5.603. PMID 18490586.
- ^ Marin M, Güris D, Chaves SS, Schmid S, Seward JF (June 22, 2007). "Prevention of varicella: recommendations of the Advisory Committee on Immunization Practices (ACIP)". MMWR Recomm Rep 56 (RR–4): 1–40. PMID 17585291. http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5604a1.htm.
- ^ Jumaan AO, Yu O, Jackson LA, Bohlke K, Galil K, Seward JF (2005). "Incidence of herpes zoster, before and after varicella-vaccination-associated decreases in the incidence of varicella, 1992–2002". J Infect Dis. 191 (12): 2002–2007. doi:10.1086/430325. PMID 15897984.
- ^ Whitley RJ (2005). "Changing dynamics of varicella-zoster virus infections in the 21st century: the impact of vaccination". J Infect Dis. 191 (12): 1999–2001. doi:10.1086/430328. PMID 15897983.
- ^ Patel MS, Gebremariam A, Davis MM (2008). "Herpes zoster-related hospitalizations and expenditures before and after introduction of the varicella vaccine in the United States". Control Hosp Epidemiol 29 (12): 1157–1163. doi:10.1086/591975. PMID 18999945.
- ^ Yih WK, Brooks DR, Lett SM, Jumaan AO, Zhang Z. Clements KM, Seward JF (2005). "The incidence of varicella and herpes zoster in Massachusetts as measured by the Behavioral Risk Factor Surveillance System (BRFSS) during a period of increasing varicella vaccine coverage, 1998–2003". BMC Public Health 5: 68–68. doi:10.1186/1471-2458-5-68. PMC 1177968. PMID 15960856. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1177968.
- ^ Yawn BP, Saddier P, Wollan PC, St Sauver JL, Kurland MJ, Sy LS (2007). "A population-based study of the incidence and complication rates of herpes zoster before zoster vaccine introduction". Mayo Clin Proc 82 (11): 1341–1349. doi:10.4065/82.11.1341. PMID 17976353.
- ^ Volpi A (2007). "Severe complications of herpes zoster" (PDF). Herpes 14 (Suppl 2): 35A–9A. PMID 17939894. http://www.ihmf.org/journal/download/4%20-%20Herpes%2014.2%20suppl%20Volpi.pdf.
- ^ Coplan P, Black S, Rojas C (2001). "Incidence and hospitalization rates of varicella and herpes zoster before varicella vaccine introduction: a baseline assessment of the shifting epidemiology of varicella disease". Pediatr Infect Dis J 20 (7): 641–5. doi:10.1097/00006454-200107000-00002. PMID 11465834.
- ^ Weaver BA (1 March 2007). "The burden of herpes zoster and postherpetic neuralgia in the United States". J Am Osteopath Assoc 107 (3 Suppl): S2–7. PMID 17488884. http://www.jaoa.org/cgi/content/full/107/suppl_1/S2.
- ^ Weller TH (2000). "Chapter 1. Historical perspective". In Arvin AM, Gershon AA. Varicella-Zoster Virus: Virology and Clinical Management. Cambridge University Press. ISBN 0521660246.
- ^ Oaklander AL (October 1999). "The pathology of shingles: Head and Campbell's 1900 monograph". Arch. Neurol. 56 (10): 1292–4. doi:10.1001/archneur.56.10.1292. PMID 10520948.
- ^ Weller TH (1953). "Serial propagation in vitro of agents producing inclusion bodies derived from varicella and herpes zoster". Proc. Soc. Exp. Biol. Med. 83 (2): 340–6. PMID 13064265.
- ^ Holt LE, McIntosh R (1936). Holt's Diseases of Infancy and Childhood. D Appleton Century Company. pp. 931–3.
- ^ Weller TH (1997). "Varicella-herpes zoster virus". In Evans AS, Kaslow RA. Viral Infections of Humans: Epidemiology and Control. Plenum Press. pp. 865–92. ISBN 978-0306448553.
- ^ Hope-Simpson RE (1965). "The nature of herpes zoster; a long-term study and a new hypothesis". Proc R Soc Med 58: 9–20. PMC 1898279. PMID 14267505. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1898279.
- ^ Thomas SL, Wheeler JG, Hall AJ (2002). "Contacts with varicella or with children and protection against herpes zoster in adults: a case-control study". Lancet 360 (9334): 678–682. doi:10.1016/S0140-6736(02)09837-9. PMID 12241874.
- ^ Terada K, Hiraga Y, Kawano S, Kataoka N (1995). "Incidence of herpes zoster in pediatricians and history of reexposure to varicella-zoster virus in patients with herpes zoster". Kansenshogaku Zasshi 69 (8): 908–912. PMID 7594784.
- ^ "Herpes | Define Herpes at Dictionary.com". http://dictionary.reference.com/browse/herpes. Retrieved 2011-03-14.
- ^ "Online Etymology Dictionary". http://www.etymonline.com/index.php?search=Zoster. Retrieved 2011-03-14.
- ^ "Online Etymology Dictionary". http://www.etymonline.com/index.php?search=shingles&searchmode=none. Retrieved 2011-03-14.
External links
- NINDS Shingles Information Page, National Institute of Neurological Disorders and Stroke
- Herpes zoster at the Open Directory Project
- Links to pictures of Shingles (Hardin MD) University of Iowa
- Facts About The Cornea and Corneal Disease: Herpes Zoster (Shingles), National Eye Institute
Infectious skin disease: Viral cutaneous conditions, including viral exanthema (B00–B09, 050–059) HSV (Herpes simplex, Herpetic whitlow, Herpes gladiatorum, Herpetic keratoconjunctivitis, Herpetic sycosis, Neonatal herpes simplex, Herpes genitalis, Herpes labialis, Eczema herpeticum, Herpetiform esophagitis) · Herpes B virus (B virus infection)VZV (Chickenpox, Herpes zoster, Herpes zoster oticus, Ophthalmic zoster, Disseminated herpes zoster, Zoster-associated pain, Inflammatory skin lesions following zoster infection, Modified varicella-like syndrome)Human herpesvirus 6/Roseolovirus (Exanthema subitum, Roseola vaccinia)SealpoxOtherYatapoxvirus: Tanapox · Yaba monkey tumor virusPapillomaviridaeHPV (Wart/Plantar wart, Heck's disease, Genital wart (giant), Laryngeal papillomatosis, Butcher's wart, Bowenoid papulosis, Epidermodysplasia verruciformis, Verruca plana, Pigmented wart, Verrucae palmares et plantares )
BPV (Equine sarcoid)Parvovirus B19 (Erythema infectiosum, Reticulocytopenia, Papular purpuric gloves and socks syndrome)CAV (Hand, foot and mouth disease, Herpangina) · FMDV (Foot-and-mouth disease) · Boston exanthem diseaseUngrouped unknown/multiple: Asymmetric periflexural exanthem of childhood · Post-vaccination follicular eruption · Lipschütz ulcer · Eruptive pseudoangiomatosis · Viral-associated trichodysplasia · Gianotti–Crosti syndromeVaricella zoster Infections Other Categories:- Chickenpox
- Viral diseases
- Herpesviruses
- Virus-related cutaneous conditions








Wikimedia Foundation. 2010.