- Candidiasis
-
Thrush (infection) redirects here. For the hoof infection see Thrush (horse).
Candidiasis Classification and external resources 
Agar plate culture of Candida albicansICD-10 B37 ICD-9 112 DiseasesDB 1929 MedlinePlus 001511 eMedicine med/264 emerg/76 ped/312 derm/67 MeSH D002177 Candidiasis or thrush is a fungal infection (mycosis) of any of the Candida species (all yeasts), of which Candida albicans is the most common.[1][2] Also commonly referred to as a yeast infection, candidiasis is also technically known as candidosis, moniliasis, and oidiomycosis.[3]:308
Candidiasis encompasses infections that range from superficial, such as oral thrush and vaginitis, to systemic and potentially life-threatening diseases. Candida infections of the latter category are also referred to as candidemia and are usually confined to severely immunocompromised persons, such as cancer, transplant, and AIDS patients as well as non-trauma emergency surgery patients.[4]
Superficial infections of skin and mucosal membranes by Candida causing local inflammation and discomfort are common in many human populations.[2][5][6] While clearly attributable to the presence of the opportunistic pathogens of the genus Candida, candidiasis describes a number of different disease syndromes that often differ in their causes and outcomes.[2][5]
Contents
Classification
Candidiasis may be divided into the following types:[3]:308–311
- Oral candidiasis (Thrush)
- Perlèche (Angular cheilitis)
- Candidal vulvovaginitis (vaginal yeast infection)
- Candidal intertrigo
- Diaper candidiasis
- Congenital cutaneous candidiasis
- Perianal candidiasis
- Candidal paronychia
- Erosio interdigitalis blastomycetica
- Chronic mucocutaneous candidiasis
- Systemic candidiasis
- Candidid
- Antibiotic candidiasis (Iatrogenic candidiasis)
Signs and symptoms
Most candidial infections are treatable and result in minimal complications such as redness, itching and discomfort, though complication may be severe or fatal if left untreated in certain populations. In immunocompetent persons, candidiasis is usually a very localized infection of the skin or mucosal membranes, including the oral cavity (thrush), the pharynx or esophagus, the gastrointestinal tract, the urinary bladder, or the genitalia (vagina, penis).[1]
Candidiasis is a very common cause of vaginal irritation, or vaginitis, and can also occur on the male genitals. In immunocompromised patients, Candida infections can affect the esophagus with the potential of becoming systemic, causing a much more serious condition, a fungemia called candidemia.[5][6]
Thrush is commonly seen in infants. It is not considered abnormal in infants unless it lasts longer than a couple of weeks.[7]
Children, mostly between the ages of three and nine years of age, can be affected by chronic mouth yeast infections, normally seen around the mouth as white patches. However, this is not a common condition.[citation needed]
Symptoms of candidiasis may vary depending on the area affected. Infection of the vagina or vulva may cause severe itching, burning, soreness, irritation, and a whitish or whitish-gray cottage cheese-like discharge, often with a curd-like appearance. These symptoms are also present in the more common bacterial vaginosis.[8] In a 2002 study published in the Journal of Obstetrics and Gynecology, only 33 percent of women who were self-treating for a yeast infection actually had a yeast infection, while most had either bacterial vaginosis or a mixed-type infection.[9] Symptoms of infection of the male genitalia include red patchy sores near the head of the penis or on the foreskin, severe itching, or a burning sensation. Candidiasis of the penis can also have a white discharge, although uncommon.[citation needed]
Causes
See also: Candida albicansCandida yeasts are commonly present in humans, and their growth is normally limited by the human immune system and by other microorganisms, such as bacteria occupying the same locations (niches) in the human body.[10]
C. albicans was isolated from the vaginas of 19% of apparently healthy women, i.e., those that experienced few or no symptoms of infection. External use of detergents or douches or internal disturbances (hormonal or physiological) can perturb the normal vaginal flora, consisting of lactic acid bacteria, such as lactobacilli, and result in an overgrowth of Candida cells causing symptoms of infection, such as local inflammation.[11] Pregnancy and the use of oral contraceptives have been reported as risk factors,[12] while the roles of engaging in vaginal sex immediately and without cleansing after anal sex and using lubricants containing glycerin remain controversial.[citation needed] Diabetes mellitus and the use of anti-bacterial antibiotics are also linked to an increased incidence of yeast infections.[12] Diet high in simple carbohydrates has been found to affect rates of oral candidiases,[13] and hormone replacement therapy and infertility treatments may also be predisposing factors.[14] Wearing wet swimwear for long periods of time is also believed to be a risk factor.[2]
A weakened or undeveloped immune system or metabolic illnesses such as diabetes are significant predisposing factors of candidiasis.[15] Diseases or conditions linked to candidiasis include HIV/AIDS, mononucleosis, cancer treatments, steroids, stress, and nutrient deficiency. Almost 15% of people with weakened immune systems develop a systemic illness caused by Candida species.[16] In extreme cases, these superficial infections of the skin or mucous membranes may enter into the bloodstream and cause systemic Candida infections.
In penile candidiasis, the causes include sexual intercourse with an infected individual, low immunity, antibiotics, and diabetes. Male genital yeast infection is less common, and incidence of infection is only a fraction of that in women; however, yeast infection on the penis from direct contact via sexual intercourse with an infected partner is not uncommon.[17]
Candida species are frequently part of the human body's normal oral and intestinal flora. Treatment with antibiotics can lead to eliminating the yeast's natural competitors for resources, and increase the severity of the condition[citation needed]. Higher prevalence of colonization of C. albicans was reported in young individuals with tongue piercing, in comparison to non-tongue-pierced matched individuals.[18] In the western hemisphere approximately 75% of females are affected at some time in their life.
Diagnosis
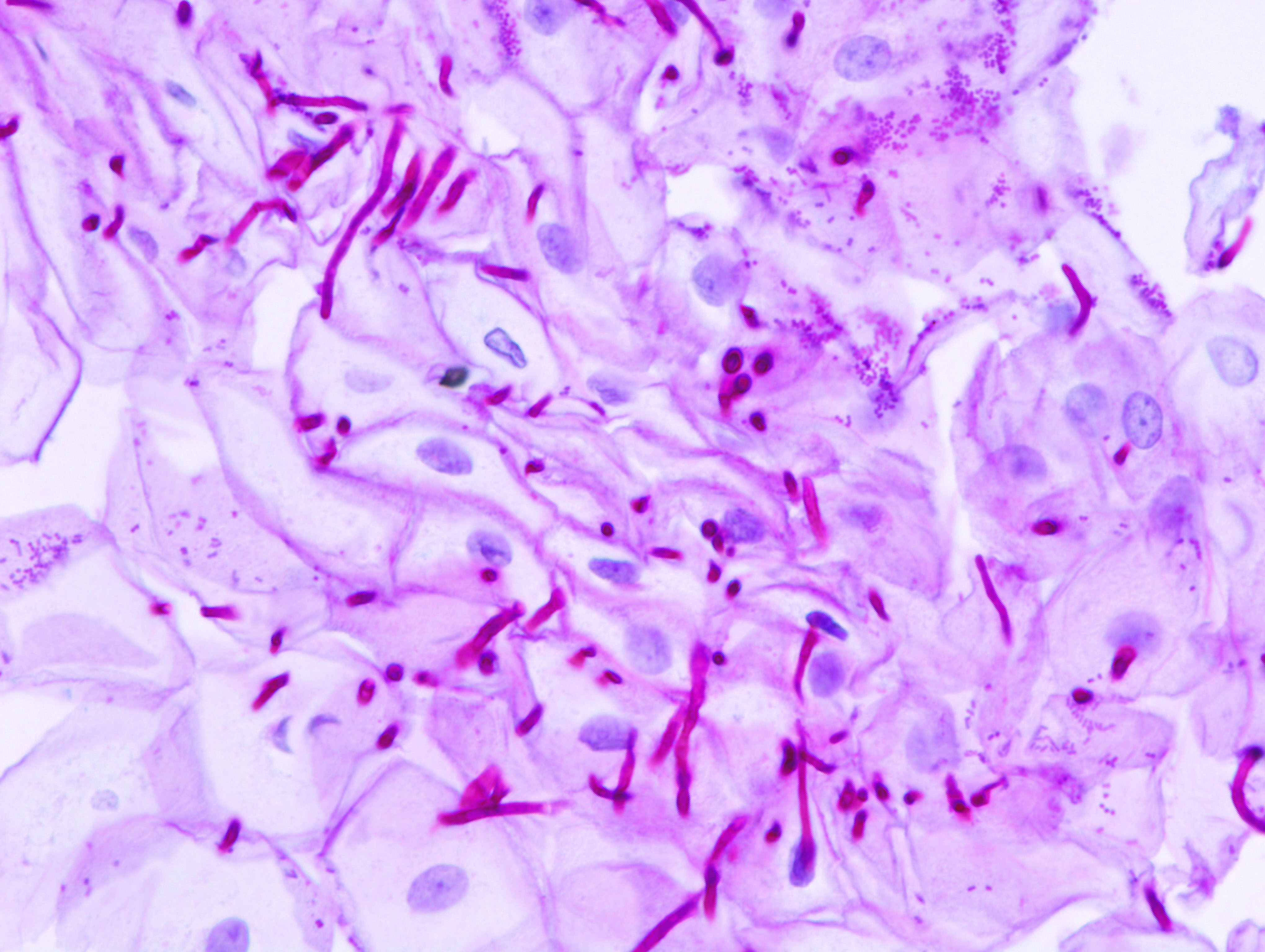
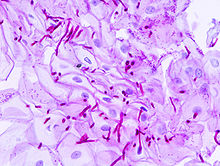 Micrograph of esophageal candidiasis. Biopsy specimen; PAS stain.
Micrograph of esophageal candidiasis. Biopsy specimen; PAS stain.
Diagnosis of a yeast infection is done either via microscopic examination or culturing.
For identification by light microscopy, a scraping or swab of the affected area is placed on a microscope slide. A single drop of 10% potassium hydroxide (KOH) solution is then added to the specimen. The KOH dissolves the skin cells but leaves the Candida cells intact, permitting visualization of pseudohyphae and budding yeast cells typical of many Candida species.
For the culturing method, a sterile swab is rubbed on the infected skin surface. The swab is then streaked on a culture medium. The culture is incubated at 37 °C for several days, to allow development of yeast or bacterial colonies. The characteristics (such as morphology and colour) of the colonies may allow initial diagnosis of the organism that is causing disease symptoms. [19]
Treatment
In clinical settings, candidiasis is commonly treated with antimycotics—the antifungal drugs commonly used to treat candidiasis are topical clotrimazole, topical nystatin, fluconazole, and topical ketoconazole.
For example, a one-time dose of fluconazole (150-mg tablet taken orally) has been reported as being 90% effective in treating a vaginal yeast infection.[20] This dose is only effective for vaginal yeast infections, and other types of yeast infections may require different dosing. In severe infections amphotericin B, caspofungin, or voriconazole may be used. Local treatment may include vaginal suppositories or medicated douches. Gentian violet can be used for breastfeeding thrush, but when used in large quantities it can cause mouth and throat ulcerations in nursing babies, and has been linked to mouth cancer in humans and to cancer in the digestive tract of other animals.[21]
Chlorhexidine gluconate oral rinse is not recommended to treat candidiasis[22] but is effective as prophylaxis;[23] chlorine dioxide rinse was found to have similar in vitro effectiveness against candida.[24]
C. albicans can develop resistance to antimycotic drugs.[25] Recurring infections may be treatable with other anti-fungal drugs, but resistance to these alternative agents may also develop.
History
The genus Candida and species C. albicans was described by botanist Christine Marie Berkhout in her doctoral thesis at the University of Utrecht in 1923. Over the years, the classification of the genera and species has evolved. Obsolete names for this genus include Mycotorula and Torulopsis. The species has also been known in the past as Monilia albicans and Oidium albicans. The current classification is nomen conservandum, which means the name is authorized for use by the International Botanical Congress (IBC).[26]
The genus Candida includes about 150 different species, however, only a few are known to cause human infections: C. albicans is the most significant pathogenic species. Other Candida species pathogenic in humans include C. tropicalis, C. glabrata, C. krusei, C. parapsilosis, C. dubliniensis, and C. lusitaniae.
Society and culture
Some alternative medicine proponents postulate a widespread occurrence of systemic candidiasis (or candida hypersensitivity syndrome, yeast allergy, or gastrointestinal candida overgrowth). The view was most widely promoted in a book published by Dr. William Crook,[27] which hypothesized that a variety of common symptoms such as fatigue, PMS, sexual dysfunction, asthma, psoriasis, digestive and urinary problems, multiple sclerosis, and muscle pain, could be caused by subclinical infections of Candida albicans.[27] Crook suggested a variety of remedies to treat these symptoms, ranging from dietary modification, prescription antifungals, to colonic irrigation. With the exception of the few dietary studies in the urinary tract infection section, conventional medicine has not used most of these alternatives, since there is limited scientific evidence to prove either their effectiveness, or that subclinical systemic candidiasis is a viable diagnosis.[28][29][30][31]
References
- ^ a b Walsh TJ, Dixon DM (1996). "Deep Mycoses". In Baron S et al. eds.. Baron's Medical Microbiology (4th ed.). Univ of Texas Medical Branch. ISBN 0-9631172-1-1. http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=mmed.section.4006.
- ^ a b c d MedlinePlus Encyclopedia Vaginal yeast infection
- ^ a b James, William D.; Berger, Timothy G.; et al. (2006). Andrews' Diseases of the Skin: clinical Dermatology. Saunders Elsevier. ISBN 0-7216-2921-0.
- ^ Kourkoumpetis T, Manolakaki D, Velmahos G, et al. (2010). "Candida infection and colonization among non-trauma emergency surgery patients". Virulence 1 (5): 359–66. doi:10.4161/viru.1.5.12795. PMID 21178471. http://www.landesbioscience.com/journals/viru/abstract.php?id=12795.
- ^ a b c Fidel PL (2002). "Immunity to Candida". Oral Dis. 8: 69–75. doi:10.1034/j.1601-0825.2002.00015.x. PMID 12164664.
- ^ a b Pappas PG (2006). "Invasive candidiasis". Infect. Dis. Clin. North Am. 20 (3): 485–506. doi:10.1016/j.idc.2006.07.004. PMID 16984866.
- ^ "Thrush". 2011. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001650/. Retrieved 2011-04-08.
- ^ Terri Warren, RN (2010). "Is It a Yeast Infection?". http://women.webmd.com/features/is-it-yeast-infection. Retrieved 2011-02-23.
- ^ Ferris DG; Nyirjesy P; Sobel JD; Soper D; Pavletic A; Litaker MS (March 2002). "Over-the-counter antifungal drug misuse associated with patient-diagnosed vulvovaginal candidiasis". Obstetrics and Gynecology 99 (3): 419–425. doi:10.1016/S0029-7844(01)01759-8. PMID 11864668.
- ^ Mulley, A. G.; Goroll, A. H. (2006). Primary Care Medicine: office evaluation and management of the adult patient. Philadelphia: Wolters Kluwer Health. pp. 802–3. ISBN 0-7817-7456-X. http://books.google.com/?id=aWQhTbwoM9EC&pg=RA1-PA802&lpg=RA1-PA802. Retrieved 2008-11-23.
- ^ Mårdh P A, Novikova N, Stukalova E (October 2003). "Colonisation of extragenital sites by Candida in women with recurrent vulvovaginal candidosis". BJOG 110 (10): 934–7. doi:10.1111/j.1471-0528.2003.01445.x. PMID 14550364. http://www.blackwell-synergy.com/openurl?genre=article&sid=nlm:pubmed&issn=1470-0328&date=2003&volume=110&issue=10&spage=934.
- ^ a b Schiefer HG (1997). "Mycoses of the urogenital tract". Mycoses 40 (Suppl 2): 33–6. doi:10.1111/j.1439-0507.1997.tb00561.x. PMID 9476502.
- ^ Akpan, A; Morgan, R (2002 Aug). "Oral candidiasis". Postgraduate medical journal 78 (922): 455–9. doi:10.1136/pmj.78.922.455. PMC 1742467. PMID 12185216. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1742467.
- ^ Nwokolo N C, Boag F C (May 2000). "Chronic vaginal candidiasis. Management in the postmenopausal patient". Drugs Aging 16 (5): 335–9. PMID 10917071.
- ^ Odds FC (1987). "Candida infections: an overview". Crit. Rev. Microbiol. 15 (1): 1–5. doi:10.3109/10408418709104444. PMID 3319417.
- ^ Choo Z.W., Chakravarthi S., Wong S.F., Nagaraja H.S., Thanikachalam P.M., Mak J.W., Radhakrishnan A., Tay A. (2010). "A comparative histopathological study of systemic candidiasis in association with experimentally induced breast cancer". Oncology Letters 1 (1): 215–222. doi:10.3892/ol_00000039. ISSN 1792-1082. http://www.spandidos-publications.com/ol/1/1/215.
- ^ David LM, Walzman M, Rajamanoharan S (October 1997). "Genital colonisation and infection with candida in heterosexual and homosexual males". Genitourin Med 73 (5): 394–6. PMC 1195901. PMID 9534752. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1195901.
- ^ Zadik Yehuda, Burnstein Saar, Derazne Estella, Sandler Vadim, Ianculovici Clariel, Halperin Tamar (March 2010). "Colonization of Candida: prevalence among tongue-pierced and non-pierced immunocompetent adults". Oral Dis 16 (2): 172–5. doi:10.1111/j.1601-0825.2009.01618.x. PMID 19732353.
- ^ Srikumar Chakravarthi, Nagaraja HS (2010). "A comprehensive review of the occurrence and management of systemic candidiasis as an opportunistic infection". Microbiology Journal 1 (2): 1–5. ISSN 2153-0696. http://scialert.net/abstract/?doi=mj.0000.20270.20270.
- ^ Moosa MY, Sobel JD, Elhalis H, Du W, Akins RA (2004). "Fungicidal Activity of Fluconazole against Candida albicans in a Synthetic Vagina-Simulative Medium". Antimicrob. Agents Chemother. 48 (1): 161–7. doi:10.1128/AAC.48.1.161-167.2004. PMC 310176. PMID 14693534. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=310176.
- ^ Craigmill A (December 1991). "Gentian Violet Policy Withdrawn". Cooperative Extension University of California -- Environmental Toxicology Newsletter 11 (5). http://extoxnet.orst.edu/newsletters/n115_91.htm.
- ^ "Chlorhexidine Gluconate". Drugs.Com. http://www.drugs.com/mtm/chlorhexidine-gluconate.html. Retrieved Jan 8, 2011.
- ^ Ferretti GA, Ash RC, Brown AT, Parr MD, Romond EH, Lillich TT (September 1988). "Control of oral mucositis and candidiasis in marrow transplantation: a prospective, double-blind trial of chlorhexidine digluconate oral rinse". Bone Marrow Transplant. 3 (5): 483–93. PMID 3056555.
- ^ Uludamar A, Ozkan YK, Kadir T, Ceyhan I (2010). "In vivo efficacy of alkaline peroxide tablets and mouthwashes on Candida albicans in patients with denture stomatitis". J Appl Oral Sci 18 (3): 291–6. doi:10.1590/S1678-77572010000300017. PMID 20857010. http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1678-77572010000300017&lng=en&nrm=iso&tlng=en.
- ^ Cowen LE, Nantel A, Whiteway MS (July 2002). "Population genomics of drug resistance in Candida albicans". Proc. Natl. Acad. Sci. U.S.A. 99 (14): 9284–9. doi:10.1073/pnas.102291099. PMC 123132. PMID 12089321. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=123132.
- ^ International Code of Botanical Nomenclature. Königstein. 2000. ISBN 3-904144-22-7. http://www.bgbm.org/iapt/nomenclature/code/SaintLouis/0000St.Luistitle.htm. Retrieved 2008-11-23.
- ^ a b Crook, William G. (1986). The yeast connection: a medical breakthrough. New York: Vintage Books. ISBN 0394747003.
- ^ Weil A (2002-10-25). "Concerned About Candidiasis?". Weil Lifestyle. http://www.drweil.com/u/QA/QA125503/. Retrieved 2008-02-21.
- ^ Barrett S (2005-10-08). "Dubious "Yeast Allergies"". QuackWatch. http://www.quackwatch.org/01QuackeryRelatedTopics/candida.html. Retrieved 2008-02-21.
- ^ Katherine Zeratsky. "Candida cleanse: Does it treat candidiasis?". Mayo Clinic. http://www.mayoclinic.com/health/candida-cleanse/AN01679. Retrieved 2009-08-09.
- ^ Blonz ER (December 1986). "Is there an epidemic of chronic candidiasis in our midst?" (PDF). JAMA 256 (22): 3138–9. doi:10.1001/jama.1986.03380220104032. PMID 3783850. http://jama.ama-assn.org/content/256/22/3138.full.pdf.
External links
Infectious diseases · Mycoses and Mesomycetozoea (B35–B49, 110–118) Superficial and
cutaneous
(dermatomycosis):
Tinea=skin;
Piedra (exothrix/
endothrix)=hairBy locationTinea barbae/Tinea capitis (Kerion) · Tinea corporis (Ringworm, Dermatophytid) · Tinea cruris · Tinea manuum · Tinea pedis (Athlete's foot) · Tinea unguium/Onychomycosis (White superficial onychomycosis · Distal subungual onychomycosis · Proximal subungual onychomycosis)
Tinea corporis gladiatorum · Tinea faciei · Tinea imbricata · Tinea incognito · FavusBy organismEpidermophyton floccosum · Microsporum canis · Microsporum audouinii · Trichophyton interdigitale/mentagrophytes · Trichophyton tonsurans · Trichophyton schoenleini · Trichophyton rubrumOtherHortaea werneckii (Tinea nigra) · Piedraia hortae (Black piedra)Subcutaneous,
systemic,
and opportunisticDimorphic
(yeast+mold)Coccidioides immitis/Coccidioides posadasii (Coccidioidomycosis, Disseminated coccidioidomycosis, Primary cutaneous coccidioidomycosis. Primary pulmonary coccidioidomycosis) · Histoplasma capsulatum (Histoplasmosis, Primary cutaneous histoplasmosis, Primary pulmonary histoplasmosis, Progressive disseminated histoplasmosis) · Histoplasma duboisii (African histoplasmosis) · Lacazia loboi (Lobomycosis) · Paracoccidioides brasiliensis (Paracoccidioidomycosis)OtherBlastomyces dermatitidis (Blastomycosis, North American blastomycosis, South American blastomycosis) · Sporothrix schenckii (Sporotrichosis) · Penicillium marneffei (Penicilliosis)Yeast-likeCandida albicans (Candidiasis, Oral, Esophageal, Vulvovaginal, Chronic mucocutaneous, Antibiotic candidiasis, Candidal intertrigo, Candidal onychomycosis, Candidal paronychia, Candidid, Diaper candidiasis, Congenital cutaneous candidiasis, Perianal candidiasis, Systemic candidiasis, Erosio interdigitalis blastomycetica) · C. glabrata · C. tropicalis · C. lusitaniae · Pneumocystis jirovecii (Pneumocystosis, Pneumocystis pneumonia)Mold-likeAspergillus (Aspergillosis, Aspergilloma, Allergic bronchopulmonary aspergillosis, Primary cutaneous aspergillosis) · Exophiala jeanselmei (Eumycetoma) · Fonsecaea pedrosoi/Fonsecaea compacta/Phialophora verrucosa (Chromoblastomycosis) · Geotrichum candidum (Geotrichosis) · Pseudallescheria boydii (Allescheriasis)Entomophthorales
(Entomophthoramycosis)Basidiobolus ranarum (Basidiobolomycosis) · Conidiobolus coronatus/Conidiobolus incongruus (Conidiobolomycosis)Enterocytozoon bieneusi/Encephalitozoon intestinalisMesomycetozoea Ungrouped Alternariosis · Fungal folliculitis · Fusarium (Fusariosis) · Granuloma gluteale infantum · Hyalohyphomycosis · Otomycosis · PhaeohyphomycosisCategories:- Mycosis-related cutaneous conditions
- Fungal diseases

Wikimedia Foundation. 2010.